
Abstract
Purpose
There is no consensus on the type of surgical treatment of congenital pseudarthrosis of the clavicle due to its rarity. The purpose of this study is to provide evidence in favor of a surgical technique and to explore factors correlated with bone consolidation.
Methods
Systematic review of the literature and an analysis of the data for each subject, including all available subjects from the published series and clinical cases since 1990. Fisher’s exact tests or T-tests were used to evaluate the effect of independent variables (age at surgery and type of treatment) on bone healing.
Results
The literature search provides 305 articles; 30 were selected, reporting 191 patients and 194 clavicles. One hundred and fifty-one clavicles were operated on at a mean age of nine years and four months (from 8 months to 21 years). Thirteen clavicles (8, 6%) had not consolidated at the last follow-up. Concerning the type of fixation, the rate of healing was similar for plates and pins (p = 0.27). The rate of consolidation was higher with autograft than with allograft, xenograft, or no graft (p = 0.00001), and was 100% for vascularized graft. The mean age at surgery was higher for patients who healed at the last follow-up (118 vs. 61 months, p = 0.001).
Conclusion
In the event of surgical indication for congenital pseudarthrosis of the clavicle, it is recommended to perform autograft and stable fixation (level 4) after seven years old (level 4).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Congenital pseudarthrosis of the clavicle (CPC) is a very rare condition.
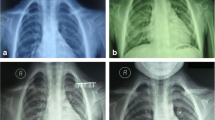
In a newborn or young child, diagnosis usually faces a non-painful tumefaction of the middle part of the clavicle. Sometimes, it is detected fortuitously on imaging assessments for another reason [1]. A plain X-ray shows an interruption of the clavicle with rounded bone extremities and no callus (Figs. 1, 2, and 3). The gap between the extremities may be of various widths. CPC is a diagnosis of exclusion: low age, no history of previous fracture, painless lesion with an increasing size following the growth [2].

Example of congenital pseudarthrosis of clavicle (personal case) before surgery

The same patient immediately after the fixation of the plate

The same patient 21 months after plate fixation
During physical examination, special attention must be paid to signs of neurofibromatosis type 1 (café-au-lait spots, family history, etc.) or cleidocranial dysplasia (abnormal fontanelle and dental anomalies).
Histologically, both bone extremities are covered with growth cartilage [2]. Such an anomaly seems to result from the failed coalescence of the two primary ossification centres of the clavicle [3]. However, the true mechanism of the pseudarthrosis is still unknown, and multiple familial cases might suggest a possible genetic transmission [2].
The high position of the right subclavian arteries would be a factor of compression or interposition between the two fragments and could explain the very strong predominance on the right side. However, bilateral forms are possible; therefore, a bilateral X-ray is always required.
No clear consensus is established about the indications of the surgery, age at surgery, type of fixation, or bone graft [1,2,3].
This study aims to perform a systematic review of the literature on the results of various surgical treatments, including statistical analysis, based on individual patient data to explore the factors correlated with healing.
Materials and methods
This review has been submitted and registered to the PROSPERO website https://www.crd.york.ac.uk/PROSPERO/ with the number CRD42018106025.
This report has been prepared according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, as suggested by the Enhancing the Quality and Transparency Of health Research (EQUATOR) network [4].
As this is a literature review, ethics committee approval is not required.
Eligibility criteria
The aim of this study was to analyze all case series and case reports of congenital pseudarthrosis of the clavicle.
Articles were screened for interventions. They were included if they clearly reported the type of treatment (or lack of treatment) and the outcome at the last follow-up (healing, yes/no). Articles that reported only conservative treatment were excluded. All other types of documents were not retained, i.e., surgical techniques, letters to the editor, or instructional pieces.
Search strategy
The electronic databases, EMBASE, MEDLINE/PubMed, Science Direct, Scopus, and Web of Knowledge, were searched from 1990 to December 31, 2020, for keywords, “congenital” + “clavicle” + “pseudarthrosis” or “pseudoarthrosis.”
To be comprehensive, bibliographies of relevant reviews and selected studies were examined. Reviews, historical, and major articles were manually added.
Study selection was performed in two stages by paired reviewers (first and last author), screening independently and in duplicate. Titles and abstracts were screened in the first stage, followed by a full-text screening on potentially eligible citations.
Data collection process
The same paired reviewers extracted the data independently and in duplicate using electronic data extraction forms. Disagreements were resolved by consensus or through discussion with a third investigator (2nd author). The selection of the articles is summarized in the PRISMA diagram (Fig. 4).

PRISMA flow chart
Statistical analysis
A “meta-type” analysis of patients’ individual data (characteristics of each case retrieved) was performed to increase evidence of factors that could influence healing. Therefore, the statistical analysis using PredictMed was based on individual patient data to mimic a case–control study [5]. Fisher’s exact tests or T-tests were used to compare data between patients with and without healing at the last follow-up [5].
Results
Database query yielded 305 articles (Fig. 4); after deleting duplicates, we retained 295 articles.
Two hundred fifty five abstracts did not meet the inclusion criteria, so 40 titles were selected for a complete reading. After a thorough reading, eight others were excluded. In total, the literature search found 32 articles between 1990 and 2020. Three articles were not found in the international databases: one in an Indian journal, a second in a Russian journal, and the third from an Italian journal. Unfortunately, we failed to contact the authors to obtain a copy.
An article of 1988 was added manually. The analysis, therefore, covers 30 papers, allowing us to collect a total of 191 patients and 194 clavicles.
In all, 12 patients had associated anomalies: three patients had genetic syndromes (a Lemli syndrome, a Prader-Willi syndrome, and a rare chromosomal deletion), five had various coastal anomalies, three had hypertrophy of the C7 transverse process, and one presented a bifurcation of the clavicle.
Surgical data and healing
Overall, on average, 151 clavicles were operated upon at nine years old and four months (range: 8 months to 21 years); 138 had healed at the last follow-up (91%).
The mean age at surgery was higher for patients who healed at the last follow-up (118 vs. 61 months, p = 0.001).
The average time of healing, as reported for 82 clavicles, was 111 days (range 45 to 252). The average delay between surgery and implant removal was nine months and ten days (range 2 to 24 months).
At the last follow-up, 13 patients (8.6%) experienced a failure at the end of treatment, i.e., persistent pseudarthrosis. Of these 13 failures, four had presented a post-operative complication: two cases of post-operative infection and two cases of protuberance of the pins under the skin. Eleven of these patients, however, had a correct function despite the failure, and we have no information on the function of the other two.
A total of 22 complications were found (15%): infections (5 cases), pseudarthrosis after a first surgery (10 cases), implant fracture (3 cases: 2 plates and one pin), implant protrusion (3 cases: 2 pins and one plate), and one clavicle fracture at D 10 after plate removal.
Type of fixation (Table 1)
The choice of the type of fixation varied before 2004; since 2004, however, there has been a prevalent use of plates (Figs. 2 and 3). Overall, we collected 82 fixations by plate and screws (70 healed after a first surgery, eight needed a surgical revision, and four did not heal), 35 by pins or wires (28 healed after a first surgery and one after surgical revision), nine bone sutures (6 healed), and four others (all healed). In 21 cases, we have no precision about the type of fixation. Whatever the type of fixation (p = 0.27), the bone healing rate was similar.
Bone graft
It is noted that since 2007, the autograft has been constant, and since 2015, there have been uses of vascularized grafts, i.e., induced membrane and vascularized fibula.
Overall, 111 autografts (mostly from the iliac crest), eight allografts, two xenografts, two induced membranes with autografts, and one vascularized fibula were found; in four cases, the types of the graft were not specified, and in 23 cases, there was no bone graft. The rate of healing was higher for autograft than for allograft, xenograft, or no graft (p = 0.00001).
Discussion
This update confirms that congenital pseudarthrosis of the clavicle is rare and that few associated anomalies can be highlighted. Contrary to the literature [6], we found no case of associated neurofibromatosis.
About three-fourths of the reported cases underwent surgery. This ratio is probably overestimated, as conservative treatments are less reported than surgical options.
The question of the need for surgery is not answered in this review. However, two attitudes are described: either systematic intervention [7] or waiting for functional issues or weakness [2, 8, 9]. In favor of systematic intervention, the general attitude facing a malformation is repairing “ad integrum” in order to allow normal functioning. Experience from adults shows that nonunion after midshaft clavicle fracture can lead to weakness and pain, in addition to social issues. Rigid internal fixation with autogenous bone graft (mainly iliac crest) has been shown to reach more than 80% of union rate in adults [10]. However, there is no consensus on the restoration of the clavicular length. If acute fractures with more than 20-mm shortening provide worse results and altered shoulder kinematic after non-operative treatment [11], length restoration after nonunion does not seem to be efficient on clinical results [12].
In favour of conservative treatment until functional issues, subjective evaluation of upper extremity function with the Constant-Murley score is often similar to the unaffected shoulder [9]. This is a common finding in congenital bone anomalies due to early adaptation of function.
As already reported, CPC healing may be long and require multiple procedures. The overall healing ratio is found to be about 90%, which is consistent with previous reports. Patients and parents must be clearly informed before carrying any surgical indication that complications are described in 15% of cases.
Surprisingly, the early age at surgery was associated with a lower healing ratio, while some authors [1, 13, 14] indicate early surgery between four and six years, arguing that the healing potential would be higher earlier in life. In our opinion, the higher rate of healing for older patients may be more related to the quality and stability of the fixation as bone segments are of higher dimensions.
Concerning the bone graft, the autologous iliac crest has provided better results than synthetic, heterologous, or no graft.
Vascularized transplants have been recently reported in 3 successful cases. However, they require either a two time procedure (induced membrane) or a complex procedure with microsurgery (vascularized fibula). From these preliminary results and experience with other sites of congenital pseudarthrosis, such techniques can be useful in case of revision surgery or large bone defect [5, 15].
Regarding bone fixation, this analysis has not allowed us to highlight the superiority of the pins or plates. However, recent literature reports mostly plates, which is probably related to the availability of locking plates. Therefore, we cannot provide evidence-based recommendations but a simple expert opinion in favour of locking plates.
Data availability
No availability of data and materials.
References
Persiani P, Molayem I, Villani C et al (2008) Surgical treatment of congenital pseudarthrosis of the clavicle : a report on 17 cases. Acta Orthop Belg 74:161–166
Cadilhac C, Odent T, Finidori G, et al (2021) Pseudarthrose congénitale de la clavicule [Internet]. In: Orthopédie pédiatrique. Elsevier; [cité 2021 févr 20]. page 57‑60.Available from: https://linkinghub.elsevier.com/retrieve/pii/B9782294701764500074
Alldred AJ (1963) Congenital pseudarthrosis of the clavicle. J Bone Joint Surg Br 45-B:312‑9.
Solla F, Bertoncelli CM, Rampal V (2020) Does the PROSPERO registration prevent double review on the same topic? BMJ Evid-Based Med bmjebm-2020–111361.
Solla F, Lemoine J, Musoff C et al (2019) Surgical treatment of congenital pseudarthrosis of the forearm: review and quantitative analysis of individual patient data. Hand Surg Rehabil 38:233–241
Ullot Font R, Cepero Campà S, Gargantilla Vázquez A et al (2006) Seudoartrosis congénita de clavícula. An Pediatría 2006(64):273–276
Kohler R, Chappuis JP, Daudet M (1980) Congenital pseudarthrosis of the clavicle. Apropos of 7 cases. Chir Pediatr 21:201–7
Galanopoulos I, Ashwood N, Garlapati AK, et al (2012) Congenital pseudarthrosis of clavicle: illustrated operative technique and histological findings. Case Rep 2012;2012:bcr2012006908‑bcr2012006908.
Kołodziej L, Bohatyrewicz A, Kotrych D (2008) Congenital pseudoarthrosis of the clavicle: is operative treatment necessary? A report of four cases and literature review. Chir Narzadow Ruchu Ortop Pol 73:277‑80, 252‑6.
Faraud A, Bonnevialle N, Allavena C et al (2014) Outcomes from surgical treatment of middle-third clavicle fractures nonunion in adults: a series of 21 cases. Orthop Traumatol Surg Res 100:175–180
Lazarides S, Zafiropoulos G (2006) Conservative treatment of fractures at the middle third of the clavicle: the relevance of shortening and clinical outcome. J Shoulder Elbow Surg 15:191–194
Hollo D, Kolling C, Audigé L et al (2020) Plating and cortical bone grafting of clavicular nonunions: clinical outcome and its relation to clavicular length restoration. JSES Int 4:508–514
Ettl V, Wild A, Krauspe R et al (2005) Surgical treatment of congenital pseudarthrosis of the clavicle: a report of three cases and review of the literature. Eur J Pediatr Surg 15:56–60
Studer K, Baker MP, Krieg AH (2017) Operative treatment of congenital pseudarthrosis of the clavicle: a single-centre experience. J Pediatr Orthop B 26:245–249
Kohler R, Solla F, Pinson S et al (2005) Pseudarthrose congénitale de l’avant-bras associée à la neurofibromatose. Rev Chir Orthopédique Réparatrice Appar Mot 91:773–781
Stephen B. Schnall, John D. King et al (1988) Congenital pseudarthrosis of clavicle: a review of litterature and surgical result of six cases. J Pediatr Orthop 316‑21.
LeGaye J, Noel H, Lokietek W (1991) Congenital pseudarthrosis of the clavicle. Apropos of a case report and literature review. Acta Orthop Belg 57:209–12
Schoenecker PL, Johnson GE, Howard B et al (1992) Congenital pseudarthrosis. Orthop Rev 1992(21):855–860
Köster G, Kunze E, von Knoch M (2008) (2008) Die operative Behandlung der kongenitalen Klavikulapseudarthrose. Z Für Orthop Ihre Grenzgeb 137:414–418
Malawski S, Zasacki W (1999) (1999) Congenital pseudoarthrosis of the clavicle: review of literature and a case report. Chir Narzadow Ruchu Ortop Pol 64:341–345
Cadilhac C, Fenoll B, Peretti A (2020) Etude de 25 cas chez l’enfant 2020;6.
Lorente Molto FJ, Bonete Lluch DJ, Garrido IM (2001) (2001) Congenital pseudarthrosis of the clavicle: a proposal for early surgical treatment. J Pediatr Orthop 21:689–693
Dzupa V, Bartonicek J, Zidka M (2007) Fracture of the clavicle after surgical treatment for congenital pseudarthrosis. Med Sci Monit 4.
Güneş T, Erdem M (2005) Sen C (2005) A case of congenital pseudarthrosis of the clavicle. Acta Orthop Traumatol Turc 39:266–269
Lelei L (2005) Congenital pseudoarthrosis of the clavicle: case report. East Afr. Med. J. [Internet] 2005 [cité 2021 févr 21]; 82. Available from: http://www.ajol.info/index.php/eamj/article/view/9319
Jeon I-H, Wilson I, Angus WW (2006) Reconstruction of congenital pseudarthrosis of the clavicle in an adult. J Orthop Sci 11:229–231
Beslikas T, Dadoukis D, Gigis I et al (2007) Congenital pseudarthrosis of the clavicle: a case report. J Orthop Surg 15:87–90
Sponer P, Neumann D, Karpas K (2008) Congenital pseudoarthrosis of the clavicle in a boy with Prader-Willi’s syndrome. Acta Chir Orthop Traumatol Cech 75:134–136
Glotzbecker MP, Shin EK, Chen NC et al (2009) Salvage reconstruction of congenital pseudarthrosis of the clavicle with vascularized fibular graft after failed operative treatment: a case report. J Pediatr Orthop 29:411–415
Currarino G, Herring JA (2009) Congenital pseudarthrosis of the clavicle. Pediatr Radiol 39:1343–1349
Chandran P, George H, James LA (2011) Congenital clavicular pseudarthrosis: comparison of two treatment methods. J Child Orthop 5:1–4
Elliot RR, Richards RH (2011) Failed operative treatment in two cases of pseudarthrosis of the clavicle using internal fixation and bovine cancellous xenograft (Tutobone). J Pediatr Orthop B 20:349–353
Singla R, Devgan A, Gogna P et al (2014) Congenital pseudoarthrosis of the clavicle with bifurcation. Indian J Orthop 48:435
Salman Ghaffari, Masoud Shayesteh Azar, Mohammad Hossein (2015) Congenital pseudoarthrosis of the clavicle; a rare case. Int. Arch. Med. [Internet] 2015 [cité 2021 févr 21]; Available from: http://imed.pub/ojs/index.php/iam/article/view/967
Abdellaoui H, Atarraf K, Chater L, et al (2017) Congenital pseudarthrosis of the clavicle treated by Masquelet technique. BMJ Case Rep bcr-2017–221557.
Di Gennaro GL, Cravino M, Martinelli A et al (2017) Congenital pseudarthrosis of the clavicle: a report on 27 cases. J Shoulder Elbow Surg 26:e65-70
Dung T, Le K, Van B, Son T et al (2017) Congenital pseudarthrosis of the clavicle in a 7-year-old girl: a case report treated with smooth elastic intramedullary pinning without bone grafting and literature review. Open J Orthop Rheumatol 2:023–024
Giwnewer U, Rubin G, Dohovni E et al (2018) Congenital pseudoarthrosis of the clavicle: should we reconsider timing and fixation method? J Orthop Surg 26:230949901879953
Haddad B, Zribi S, Haraux E et al (2019) Induced membrane technique for clavicle reconstruction in paediatric patients: report of four cases. Orthop Traumatol Surg Res 105:733–737
Kim AE, Vuillermin CB, Bae DS et al (2020) Congenital pseudarthrosis of the clavicle: surgical decision making and outcomes. J Shoulder Elbow Surg 29:302–307
Author information
Authors and Affiliations
Contributions
All the authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Federico Solla and Carlo Bertoncelli. The first draft of the manuscript was written by Cédric Assouto and Federico Solla, and all the authors commented on previous versions of the manuscript. All the authors read and approved the final manuscript.
Cédric Assouto performed the study and wrote the article.
Marc-Olivier Gauci supervised the study, wrote, and revised the article.
Sikha Bagui supervised the study, wrote, and revised the article.
Marco Monticone supervised the study, wrote, and revised the article.
Carlo Mario Bertoncelli supervised the study and revised the text.
Virginie Rampal supervised the study and revised the text.
Federico Solla conceived and supervised the study, wrote, and revised the text.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study did not require ethics approval.
Informed consent was obtained from all individual participants included in the study.
The authors affirm that human research participants provided informed consent for publication of the images in Fig. 1, 2, 3 and 4.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Assouto, C., Bertoncelli, C.M., Gauci, MO. et al. Congenital pseudarthrosis of the clavicle: a systematic review. International Orthopaedics (SICOT) 46, 2577–2583 (2022). https://doi.org/10.1007/s00264-022-05470-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-022-05470-6