
Abstract
Osteonecrosis of the femoral head (ONFH) is a devastating condition affecting relatively young patients whereby the femoral head is necrotic, resulting in significant pain, articular surface collapse, and eventual osteoarthritis. This condition has been highly associated with chronic steroid use, alcoholism, and hip trauma, as well as other less common conditions. Without intervention, this condition has a high likelihood of progressing and developing into end-stage osteoarthritis. Unfortunately, ONFH is difficult to diagnose on plain radiographs in the early stages of the disease, and often requires more advanced imaging modalities such as MRI in order to fully assess for early degeneration. Providers, therefore, must have a high index of suspicion when a younger patient presents with hip pain and negative X-rays. Unfortunately, in patients whose femoral heads have already collapsed, joint-preserving procedures are not effective, and total hip arthroplasty remains the most reliable long-term treatment. Multiple treatments have been pursued to address osteonecrosis in patients whose femoral head have not yet collapsed, but the results of these treatments are mixed. The most promising of these interventions to date is core decompression with the use of concentrated bone marrow aspirate to improve the healing potential of the femoral head. Further studies including randomized clinical trials are necessary in order to assess the effectiveness of this therapy, the best possible source of cells and the best method of implantation in order to further improve results in those with pre-collapse ONFH.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteonecrosis of the femoral head (ONFH) is an unfortunate condition that may lead to debilitating hip pain and severe arthritis in relatively young individuals. In the USA alone, it has an incidence estimated at 15,000–20,000 new cases per year [1, 2]. It is seen commonly in the post-traumatic patient who has previously sustained a proximal femur fracture—especially in subcapital femoral neck fractures—or dislocations of the hip [1]. It can also be seen, however, in patients with chronic glucocorticoid steroids use, alcohol abuse, sickle cell disease, HIV, and Lupus [3, 4]. These pathologies lead to ischaemic changes to the femoral head, which overtime causes significant weakening of the trabecular bone. With repetitive weight bearing and stress, the weakened femoral head will eventually fail and collapse, if not addressed [5, 6]. Very few osteonecrotic femoral heads will spontaneously resolve, and approximately 67% of asymptomatic patients and 85% of symptomatic patients will progress to femoral head collapse [7]. ONFH that has progressed to femoral head collapse is most effectively managed with total hip arthroplasty (THA), and osteonecrosis accounts for approximately 10% of the roughly 250,000 THAs performed annually in the USA [1, 7]. Arthroplasty, however, is not the optimal treatment in this patient population, as the average age of those affected by ONFH is between 20 and 40 years, and the expected longevity of THA implants falls well short of the longevity of these patients [4]. Consequently, young patients treated with arthroplasty will almost certainly require at least one revision during their lifespan. As a result, joint-preserving treatments are preferred when dealing with ONFH [1]. These treatments are most effective in patients whose conditions are being addressed prior to the onset of irreversible femoral head collapse. Therefore, the clinician must have a high level of suspicion when dealing with hip and groin pain in patients who have risk factors for ONFH, as early diagnosis prior to the onset of femoral head collapse is associated with less overall morbidity.
Diagnosis
Early diagnosis of ONFH is of upmost importance. An accurate history and physical exam are crucial, and the physician must have a low threshold for further studies in patients who have risk factors for the disease and endorse hip or groin pain that is exacerbated by weight bearing and relieved with rest [1, 8]. On physical exam, there may be limitations in range of motion, and passive internal rotation of the affected lower extremity may be particularly painful [1]. Unfortunately, the early stages of ONFH may be asymptomatic, as no structural change has taken place to cause pain [1]. Plain radiographs are generally the first imaging modality used. While X-ray is not particularly sensitive at identifying early-stage osteonecrosis, it can be useful, and frog-leg lateral views should always be obtained [1, 8, 9]. In the later stages of the disease, one will see subchondral cysts, sclerosis, and eventually femoral head collapse and flattening on X-ray [8]. If no abnormalities are seen on plain radiographs and ONFH is still suspected, an advance imaging study may be done; the gold standard imaging modality for the pre-collapse stages of ONFH is MRI [1, 9]. An early osteonecrotic lesion will have a single-density line on the T1 images, typically in the anterosuperior aspect of the femoral head. On the T2 images, one may see a “double line sign”, which represents high signal intensity in the subchondral bone bordering the lesion [1, 8]. In a patient found to have ONFH, the contralateral hip should be investigated, as this disease is present bilaterally in 70–75% of patients [1, 4, 8].
Classification
There are numerous grading systems available for evaluating the severity of ONFH. The Ficat system was one of the first to be proposed, and is based on plain X-ray. Ficat I is a normal radiograph. In Ficat II, subchondral cysts are present as well as sclerosis, but the joint space is maintained and there is no femoral head collapse. In Ficat III, the femoral head has flattened and there is subchondral fracture (crescent sign); however, the joint space is maintained. In Ficat IV disease, there is joint space narrowing with osteophyte formation, consistent with typical osteoarthritis [1, 8].
The Association Research Circulation Osseous (ARCO) classification system was established in 1991 and has been updated several times; it relies on multiple imaging modalities to further grade the severity of osteonecrosis, and it is broken down into five stages (0–4). Stage 0 does not show any changes on X-ray, CT, scintigraphy, or MRI. In this initial stage, osteonecrosis can only be defined histologically. In stage 1 disease, both X-ray and CT are negative, but either MRI or scintigraphy is abnormal. Stage 2 is characterized by early changes in X-ray appearance such as sclerosis; however, there is no crescent sign present and the integrity of the subchondral bone has not yet been compromised. In stage 3 disease, there is radiographic evidence of early fracture (crescent sign) and flattening of the femoral head. Lastly, stage 4 is defined by the presence of joint space narrowing and destruction, indicating the onset or presence of osteoarthritis [8, 10].
Most recently, the Nijmegen modification (Table 1) has been proposed in order to better subclassify the third stage of the ARCO system. This modification sought to subdivide stage 3 ONFH into an early and late phase. The inspiration for this change was the observation that some of those patients with early femoral head collapse who were grouped into stage 3 disease did not progress to more advanced stages of disease and were found to be more likely to respond favorably to joint-preserving procedures [10].
Treatment
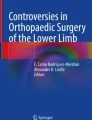
The optimal treatment of pre-collapse (ARCO stage 1 and 2) ONFH is controversial, as there is a paucity of studies with high-level evidence and much of the literature is plagued by small patient cohorts over a short follow-up period [1]. Core decompression (CD) is currently the most commonly performed procedure for treating pre-collapse ONFH [2, 3]. Increased intramedullary pressure is consistently seen in ONFH, and this increased pressure is thought to potentially tamponade off the blood supply to the head of the femur [2, 11]. CD works by drilling one or multiple tracts from the greater trochanter, through the femoral neck, and into the subchondral bone of the femoral head (Fig. 1 a, b) [7]. These tracts relieve the increased pressure and can potentially help to restore adequate blood flow to the femoral head, thereby allowing for healing and preservation of the joint [12, 13]. Studies have found, however, that the mesenchymal stem cells (MSCs) present in the femoral head of a patient with ONFH—the same cells responsible for its repair—may be deficient in both quantity and quality, thereby leading to deficient angiogenesis and bone remodeling following CD [11, 14].

a, b AP and lateral fluoroscopic radiographs taken during a core decompression procedure. A guide pin is first placed in the osteonecrotic lesion, and it is over drilled with a cannulated reamer (8–10 mm depending on lesion size)
The injection of concentrated bone marrow aspirates, containing autologous bone marrow mononuclear cells (BMMCs), through the CD tracts was first proposed by Hernigou et al. in 1993 in order to address this issue [4]. By injecting autologous BMMCs directly into the femoral head, one may hypothetically increase the population of active stem cells present for osteogenesis [15]. Once injected into the femoral head defect, these cells have been found to survive and proliferate for up to 12 weeks [16]. BMMC injection into areas of necrosis has been a controversial topic that has shown conflicting, but overall positive outcomes.
In a prospective, randomized clinical trial by Tabatabee et al., 28 hips classified as either ARCO stage I, II, or III in 18 patients were treated with either core decompression alone or in conjunction with injection of BMMCs over a two year follow-up time [13]. While this study was limited by a small patient group and short follow-up time, it produced some impressive results. The patients who had BMMCs injected had significantly decreased VAS and WOMAC scores. At the end of the follow-up period, three patients who underwent BMMC injection had improvement as measured by MRI and none had undergone THA. In the 14 hips who had received CD without BMMC injection, however, none of the patients had an improvement in MRI and three ultimately underwent THA within the study period [13].
Three more randomized clinical trials [17,18,19] reported favourable results of the of BMMC instillation. On the other hand, Lim et al. assessed multiple drilling and BMMC implantation to treat the early stages ONFH in 128 patients (190 hips). There were no significant differences in the clinical and radiographic results between the two groups [20].
Mesenchymal stem cells (MSC) residing in BMMCs are multipotent cells that have the ability to differentiate into a wide array of specialized cells such as bone, cartilage, adipose, and muscle [6]. These cells can be derived from various sources such as bone marrow, adipose, and dental pulp [3]. MSCs’ capacity for multipotent differentiation is dependent upon the local milieu where the cell is placed and the various cytokines and growth factors with which it comes into contact [6]. MSCs are particularly desirable for the treatment of ONFH, as they provide a source of osteoblasts to the site of interest, and these cells may participate in osteogenesis and repair the necrotic defect [4, 6, 11, 16]. Not only do MSCs provide the precursor cells for repair but they also secrete growth factors and pro-angiogenic factors such as BMP-2 and VEGF that serve to stimulate the local repair processes that prevent further femoral head degeneration in ONFH [21, 22]. In a recent meta-analysis by Xu et al. comparing core decompression alone and in conjunction with MSC implantation, MSCs were found to improve Harris Hip Score (HHS), decrease the necrotic burden of the femoral head, and delay disease progression, and decrease the incidence of total hip arthroplasty in these patients [11].
While the majority of current studies investigating MSCs use cells derived from bone marrow—specifically from the iliac crest—these cells may also be harvested from adipose tissue. This procedure involves first procuring the tissue through liposuction, then digesting that product with collagenase, which serves to break down the adipose matrix. This product is then centrifuged in order to isolate the MSCs [23]. This method of acquiring MSCs is not only cheaper but also less invasive and painful than that used for bone marrow harvesting [24]. In his in vitro study, Wyles et al. found that adipose-derived MSCs (aMSCs) have a higher potential for not only proliferation but also osteogenic differentiation, making them very appealing for ONFH treatment [25]. Unfortunately, the few studies investigating in vivo use of this subset of MSCs have been somewhat underpowered, only looking at a small number of patients. While the results of these studies have been promising, there is a lack of randomized clinical trials. Further investigations using larger patient populations will need to take place before the use of aMSCs can be made commonplace in the treatment of ONFH [23]. Although there is a paucity of studies looking at the use of adipose-derived MSCs for ONFH, they may play a large role in the future treatment of this condition. Houdek et al. found that both the quantity and quality (with respect to osteogenic differentiation ability) of bone marrow-derived MSCs are decreased in patients with ONFH when compared to that of patients without the disease [14]. Therefore, other types of stem cells should be investigated thoroughly in order to determine the optimal source for patients with potentially deficient bone marrow MSCs.
While the results of studies have unfortunately been inconsistent, this may be due to the finding that not all ONFH patients are optimal candidates for autologous MSC transplantation. Patients with ONFH secondary to corticosteroid use and alcoholism not only have MSCs with decreased activity but they have also been observed to be less likely to differentiate into bone and have a proclivity toward adipose cell differentiation [8, 14, 15, 26, 27]. Consequently, these cells are less likely to differentiate into osteoblasts, making them much less able to adequately address the root cause of ONFH and participate in femoral head salvage. As a result, patients who have ONFH as a result of these conditions may be less likely to reap the benefits of MSC transplantation and are, therefore, more likely to progress to femoral head collapse [7]. The equivocal results of several studies that compare the efficacy of MSC use in CD to traditional CD may be due to the use of this poorly predisposed patient population. Future studies should further investigate the response to autologous MSC transplantation in patients who have osteonecrosis as a result of steroid and alcohol use and those who developed it due to another cause. These studies should also investigate if a difference exists in this patient population’s response to bone marrow and adipose-derived mesenchymal stem cells.
Conclusion
Osteonecrosis of the femoral head is an unfortunate and oftentimes devastating disease of young- to middle-aged people in which the femoral head may collapse, leading to early-onset osteoarthritis. Depending on the severity of the disease, these patients may require a total hip arthroplasty at a particularly young age and are, therefore, likely to require revision total hip surgery, as they will likely outlive the longevity of their implant. Early diagnosis and refining of joint-preserving procedures are especially important in order to avoid the need for joint replacement in this patient population. BMMCs are particularly appealing in the treatment of ONFH because they provide not only a source of cells used for the potential repair of the femoral head but they also provide cytokines and growth factors that may encourage the cells already present within the femoral head to initiate the healing process. Further studies utilizing large patient groups are necessary in order to elucidate not only the true effect of BMMC implantation but also the optimal source of mesenchymal stem cells.
References
Moya-Angeler J, Gianakos A, Villa J, Ni A, Lane J (2015) Current concepts on osteonecrosis of the femoral head. World J Orthop 6:590–601
Papakostidis C, Tosounidis T, Jones E, Giannoudis P (2016) The role of “cell therapy” in osteonecrosis of the femoral head: a systematic review of the literature and meta-analysis of 7 studies. Acta Orthop 87:71–78
Lau R, Perruccio A, Evan H, Mahomed S, Mahomed N, Gandhi R (2014) Stem cell therapy for the treatment of early stage avascular necrosis of the femoral head: a systematic review. BMC Musculoskelet Disord 15:1–10
Hernigou P, Trousselier M, Roubineau F, Bouthors C, Chevallier N, Rouard H, Flouzat-Lachaniette C (2016) Stem cell therapy for the treatment of hip osteonecrosis: a 30-year review of progress. Clin Orthop Surg 8:1–8
Looney A, Dighe A, Novicoff W, Cui Q (2016) Stem cell therapy for early stage osteonecrosis: challenges and future research direction. Formosan J Musculoskelet Disord 7:119–126. https://doi.org/10.6492/RJMD.20151130
Wang C, Wand Y, Meng HY, Yuan XL, Xu XL, Wang AI, Guo QY, Peng J, Lu SB (2015) Application of bone marrow mesenchymal stem cells to the treatment of osteonecrosis of the femoral head. Int J Clin Exp Med 8:3127–3135
Pepke W, Kasten P, Beckmann N, Janicki P, Egermann M (2016) Core decompression and autologous bone marrow concentrate for treatment of femoral head osteonecrosis: a randomized prospective study. Orthop Rev 8:5–9
Kaushik A, Das A, Cui Q (2012) Osteonecrosis of the femoral head: an update in the year 2012. World J Orthop 3:49–56
Mont M, Cherian J, Sierra R, Jones L, Lieberman J (2015) Nontraumatic osteonecrosis of the femoral head: where do we stand today? J Bone Joint Surg Am 97:1604–1627
Gardeniers J, Gosling-Gardeniers A, Rijnen W (2014) The ARCO staging system: generation and evolution since 1991. In: Koo KH, Mont M, Jones L (eds) Osteonecrosis. Springer, New York, pp 215–218
Xu S, Zhang L, Jin H, Shan L, Zhou L, Xiao L, Tong P (2017) Autologous stem cells combined core decompression for treatment of avascular necrosis of the femoral head: a systematic meta-analysis. Biomed Res Int 2017:1–11
Wang BL, Sun W, Shi ZC, Yue DB, Guo WS, Xu SQ, Lou JN, Li ZR (2010) Treatment of nontraumatic osteonecrosis of the femoral head with the implantation of core decompression and concentrated autologous bone marrow containing mononuclear cells. Arch Orthop Trauma Surg 130:859–865
Tabatabaee R, Saberi S, Parvizi J, Mortazavi S, Farzan M (2015) Combining concentrated autologous bone marrow stem cells injection with core decompression improves outcome for patients with early-stage osteonecrosis of the femoral head: a comparative study. J Arthroplast 30(Suppl 1):11–15
Houdek M, Wyles C, Packard B, Terzic A, Behfar A, Sierra R (2016) Decreased osteogenic activity of mesenchymal stem cells in patients with corticosteroid-induced osteonecrosis of the femoral head. J Arthroplast 31:893–898
Hernigou P, Poignard A, Manicom O, Mathieu G, Rouard H (2005) The use of percutaneous autologous bone marrow transplantation in nonunion and avascular necrosis of bone. J Bone Joint Surg (Br) 87:896–902
Yan Z, Hang D, Guo C, Chen Z (2009) Fate of mesenchymal stem cells transplanted to osteonecrosis of femoral head. J Orthop Res 27:442–446
Ma Y, Wang T, Liao J, Gu H, Lin X, Jiang Q, Bulsara MK, Zheng M, Zheng Q (2014) Efficacy of autologous bone marrow buffy coat grafting combined with core decompression in patients with avascular necrosis of femoral head: a prospective, double-blinded, randomized, controlled study. Stem Cell Res Ther 5:115
Zhao D, Cui D, Wang B, Tian F, Guo L, Yang L, Liu B, Yu X (2012) Treatment of early stage osteonecrosis of the femoral head with autologous implantation of bone marrow-derived and cultured mesenchymal stem cells. Bone 50:325–330
Sen RK, Tripathy SK, Aggarwal S, Marwaha N, Sharma RR, Khandelwal N (2012) Early results of core decompression and autologous bone marrow mononuclear cells instillation in femoral head osteonecrosis: a randomized control study. J Arthroplast 27:679–686
Lim YW, Kim YS, Lee JW, Kwon SY (2013) Stem cell implantation for osteonecrosis of the femoral head. Exp Mol Med 45:e61. https://doi.org/10.1038/emm.128
Song H, Tao L, Wang F, Wand W, Wei Y, Shen W, Zhou F (2015) Effect of bone mesenchymal stem cells transplantation on the micro-environment of early osteonecrosis of the femoral head. Int J Clin Exp Pathol 8:14528–14534
Yuan HF, Zhang J, Guo CG, Yan ZQ (2016) Clinical outcomes of osteonecrosis of the femoral head after autologous bone marrow stem cell implantation: a meta-analysis of seven case-control studies. Clinics 71:110–113
Pak J, Lee J, Park K, Park M, Kang LW, Lee S (2017) Current use of autologous adipose tissue-derived stromal vascular fraction cells for orthopedic applications. J Biomed Sci 24:1–12
Baer PC, Geiger H (2012) Adipose-derived mesenchymal stromal/stem cells: tissue localization, characterization, and heterogeneity. Stem Cells Int 2012:1–11
Wyles C, Houdek M, Crespo-Diaz R, Norambuena G, Stalboerger P, Terzic A, Behfar A, Sierra R (2015) Adipose-derived mesenchymal stem cells are phenotypically superior for regeneration in the setting of osteonecrosis of the femoral head. Clin Orthop Relat Res 473:3080–3090
Hernigou P, Beaujean F (1997) Abnormalities in the bone marrow of the iliac crest in patients who have osteonecrosis secondary to corticosteroid therapy or alcohol abuse. J Bone Joint Surg Am 79:1047–1053
Cui Q, Wang GJ, Balian G (1997) Steroid-induced adipogenesis in a pluripotential cell line from bone marrow. J Bone Joint Surg Am 79:1054–1063
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Cui or an immediate family member serves as a paid consultant to Exactech has received research or institutional support from the National Institute of Health, Department of Defense and Exactech; serves as a board member, owner, officer, or committee member of the Virginia Orthopaedic Society, Journal of Arthroplasty, World Journal of Orthopaedics and Journal of Orthopaedic Research; and received royalties from Elsevier. None of the following authors or any immediate family member has received anything of value from or has stock or stock options held in a commercial company or institution related directly or indirectly to the subject of this article: Dr. Larson, Dr. Goodman, Dr. Jones, and Dr. Koo.
Rights and permissions
About this article

Cite this article
Larson, E., Jones, L.C., Goodman, S.B. et al. Early-stage osteonecrosis of the femoral head: where are we and where are we going in year 2018?. International Orthopaedics (SICOT) 42, 1723–1728 (2018). https://doi.org/10.1007/s00264-018-3917-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-018-3917-8