
Abstract
Purpose
Arthroscopy of the hip joint is considered a demanding procedure with long learning curve. There are only a few studies that concentrate on this topic. This prospective clinical study evaluates the learning curve of the hip arthroscopy based on clinical outcomes, surgical time, and complication rate.
Materials
In this study, we first evaluated 150 hip arthroscopy procedures performed by a single surgeon. The patient group consisted of 86 females and 64 males with mean age 37 years (range 16–69). Study cohorts were divided into groups of 50 patients. Surgical time, complication rate and clinical results based on NAHS score were recorded for each group. Statistical analysis of differences between groups was performed using the ANOVA method and paired t-test.
Results
We found a statistically significant decrease of complication rate with more procedures performed. There were significantly better clinical outcomes after at least 100 procedures. No difference in surgical time was found, but towards the end of the learning curve, more complex procedures were performed. The only statistical difference was the portal setup time. The learning curves were constructed based on these results.
Conclusions
Hip arthroscopy provides very good clinical outcomes if precisely indicated and performed. It is, however, a demanding procedure with many possible pitfalls and complications. According to our study, at least 100 procedures are needed to gain basic technical and indication skills. The presence of a more skilled surgeon in the beginning of the learning curve is advised to reduce the complication rate.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hip arthroscopy is currently considered a rapidly evolving treatment method for various hip pathologies. The main indication for hip artrhoscopy is the treatment of labral and cartilage defects associated with femoro-acetabular impingement syndrome (FAI) [1]. The number of patients has increased rapidly over the past decade and many surgeons are now performing hip arthroscopy as a routine procedure. However, hip arthroscopy is known to be a demanding procedure with a steep and long learning curve [2]. Surgeons’ skills and experience are crucial to achieve good clinical results and a low complication rate [3]. However, there is no clear evidence in literature about the number of procedures needed to obtain basic hip arthroscopy skills [4, 5]. In our department, hip arthroscopy has been established as one of the standard techniques to address hip pathology in patients under the age of 50.
We assume that the learning curve for hip arthroscopy is much steeper compared to learning curves for knee [6] and shoulder arthroscopy [7], as the hip arthroscopy has several aspects that make the procedure more technically demanding. In most studies, surgical time and complication rates are used to evaluate the learning curve [2]. Apart from the learning curve to achieve appropriate technical skills, we also decided to evaluate clinical outcomes at least 24 months after the surgery, as well as the type of procedures performed during the arthroscopy after a certain amount of experience. We prospectively evaluated the first 150 hip arthroscopy procedures performed in our department by a single surgeon. Surgical time, complication rates, types of procedures and subjective patient outcomes based on non-arthritic hip score (NAHS) [8] were evaluated in this prospective study. Based on this analysis, we aim to estimate a learning curve for hip arthroscopy. This study may help to focus on the basic pitfalls in the training of novice surgeons in hip arthroscopy.
Material and methods
In this study, the first 150 hip arthroscopic procedures performed by a single surgeon in the years 2010–2015 were prospectively evaluated. The mean age of patients was 37 years (16–67). In the patient cohort, 86 females and 64 males were evaluated. The main diagnosis was FAI and its associated pathology. Surgical indications are summarised in Table 1. Patients included in this study had no signs of severe osteoarthritis on a pre-operative X-ray. The joint line narrowing to under 4 mm on AP standing radiographs was considered to be a contraindication for hip arthroscopy. All patients had plain MRIs (no contrast) prior to surgery to confirm the diagnosis and to exclude patients with possible avascular necrosis (AVN) of the femoral head. We used standard T1 and T2 weigthed coronal, transversal and radial scans to evaluate basic chondrolabral pathology as the contrast MRI arthrograms were not available for all patients at the time of the study.
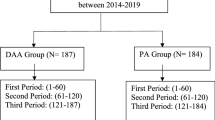
Patients were divided into three groups of 50 patients according to the surgeon’s experience, measured by the total number of procedures performed. The first patient group consisted of cases 1–50, the second group with cases 51–100 and the third group with cases 101–150.
The surgical team consisted of the main surgeon and the assisting surgeon, both of whom were experienced in knee and shoulder arthroscopy. Prior to starting to perform hip arthroscopies, the individually evaluated surgeon had performed more than 300 arthroscopic knee and shoulder procedures and underwent both the basic and the advanced level cadaveric hip arthroscopy courses. The evaluated surgeon was also familiar with hip preserving surgery using standard approaches for surgical hip dislocation (SHD) and anterior minimally invasive approach (AMIS) as well as being trained in X-ray and MRI evaluation of FAI syndrome and proper clinical examination.
Surgical technique
All patients were treated using a standardised arthroscopic technique with the patient in supine position on a traction table. The arthroscopy started with central compartment evaluation. Traction was applied and guide wire inserted into the joint through an anterolateral portal using puncture needle and X-ray control. The portal was dilated and a 70° scope was inserted through the portal. An anterior portal was established under direct visualisation outside-in. After the portal setup, the basic diagnostic evaluation was performed. The hip labrum, articular cartilage, femoral head, acetabular fossa and joint capsule were inspected. After diagnosing the pathology, a shaver was used to thin down the joint capsule; no capsular excision was made. After this preparation, rim trimming and labral reconstruction was performed using the mid anterior portal to insert the suture anchors. We used tying suture anchors designed for hip labral repair. At the end of the central compartment treatment we repaired articular cartilage; we mainly used microfracturing of the subchondral bone and loose end trimming using a shaver. After the central compartment was treated, we cancelled the traction and inspected the peripheral compartment. Synovectomy and capsular reduction were performed if needed, femoral head/neck junction was inspected for CAM deformity and it was reduced under X-ray control. When the femoral head osteoplasty was finished, dynamic impingement evaluation was performed and any residual impingement repaired. The arthroscopic procedure was ended by drain insertion and portal suture.
Post-operative management
All patients underwent standardised post-operative protocol. Patients were allowed partial weight bearing ambulation using crutches from the day of the surgery. The drain was removed the second day before the patient was discharged from the hospital care. The first check-up was at ten days post-operatively to remove the stitches and to evaluate the wound. Patients were limited to 90° flexion in the hip joint, and rotations were allowed according to subjective pain for the first four weeks post-operatively. After four weeks, full range of motion was allowed with individual limitation according to subjective pain. Weight bearing with limitation of up to 2/3 of the body weight was proposed for six weeks post-operatively. After six weeks from the surgery, gradual weight-bearing without support was allowed according to clinical status. Patients with large cartilage defects (over 2 cm2) were recommended to use crutches for six to eight weeks. Exercising in swimming pool and bike riding were allowed at eight weeks from the injury in all patients. Avoidance of hard impacts and jumps was strictly recommended for six months after the surgery. Full sporting activity was allowed at six months after the surgery for all patients. X-ray control was performed at six weeks and six, 12 and 24 months after the surgery. On X-rays, signs of worsening of osteoarthritis, formation of para-articular ossifications and avascular necrosis of the femoral head were recorded.
Post-operative evaluation
The surgical time, traction time and portal setup time were recorded and evaluated. During the surgery, the type of reconstructive procedure performed was also recorded. All patients were evaluated clinically using NAHS score [8] pre-operatively, six weeks and three, six, 12 and 24 months post-operatively. In all patients, the most severe complications such as development of para-articular ossifications (PAO), avascular femoral head necrosis (AVN), worsening of osteoarthritis needing total hip arthroplasty (THA), major bleeding, and femoral or perineal hypesthesia were recorded and evaluated. Correlation between surgical time and the type of procedure was performed for all three patient groups. NAHS score in 24 months was evaluated and compared between all three groups. Complication rates were also compared.
Statistical analysis
Statistical analysis using the ANOVA method and paired t-tests between the groups were used, the level of significance was set as p = 0.05. Based on this evaluation, we constructed graphs of the learning curve based on surgical time, number of cases and clinical results in 24 months.
Results
Types of procedures performed in all cases are summarised in Table 2, and the evaluation of surgical times, clinical outcomes and major complications are summarised in Table 3.
Patient group 1 (case 1–50)
The mean total surgical time was 95 minutes (58–129 minutes), the mean traction time 55 minutes, and the portal setup time was 15 minutes on average. The main types of procedures performed in this group were CAM lesion resection and labral debridement. No labral reconstruction was performed in this group. Clinical evaluation based on the mean NAHS score was 57/100 pre-operatively, 74/100 in six weeks and 80/100 in two years. The main complications in this group were AVN in three cases and severe worsening of hip arthritis in five cases, all of these resulting in conversion to THA. No signs of deep infection were noticed. We had six cases of perineal hypesthesia that spontaneously resolved, and PAO treated conservatively was present in three patients in 12 months.
Patient group 2 (51–100 cases)
In this group, the mean levels for the total surgical time decreased to 75 minutes (45–115 minutes), the traction time was 52 minutes and the portal setup 12 minutes. The primary type of procedure was still CAM lesion resection, the second most frequent procedure was labral re-fixation, followed by labral resections. Clinical outcomes measured by the NAHS score improved from 57/100 pre-operatively to 73/100 in six weeks, and at 24 months the mean NAHS score was 82/100. We saw one case of AVN in this group and three cases of severe worsening of osteoarthritis on X-ray with severe pain. All of these patients needed conversion to THA. Femoral or perineal hypesthesia was present in seven cases. Treatment of this complication was conservative with no sequelae. Formation of PAO was present in four patients, of which one case underwent open surgical revision with good results.
Patient group 3 (101–150 cases)
The mean surgical time was 85 minutes (57–122 minutes), the traction time 56 minutes and the portal placement time five minutes. The most common procedures were CAM resection, labral refixation, and cartilage repair. Clinical outcomes were also good; preoperative NAHS was 57/100, at six weeks NAHS score improved to 75/100, and at 24 months the score was 87/100. In this group, we observed no AVN, one conversion to THA due to worsening of osteoarthritis, and one minor superficial portal infection treated conservatively by antibiotics and local wound treatment. Upon X-ray check-up, PAO was present in five patients with no surgical revision needed. Femoral or perineal hypesthesia was observed in five cases with spontaneous resolve.
All tested criteria were evaluated and compared among the individual groups. When we focused on the mean surgical time for all three groups according to the type of procedure we found no statistical difference among the three groups. The traction time was also comparable with no statistical differences. The only statistically significant difference was in the portal placement time between group 3 and both previous groups (p < 0.01).
Considering the clinical outcomes based on NAHS score, there was a pre-operative average of 57/100 for all groups. Post-operatively at six weeks, the score was 74/100 for group 1, 73/100 for group 2 and 75/100 for group 3. There was statistically significant improvement of the clinical outcomes in all groups compared to the pre-operative value. No statistical difference was found between the tested groups at six weeks. Twenty-four months after surgery, the mean NAHS score was 80/100 for group 1, 82/100 for group 2 and 87/100 for group 3. There was a statistically significant difference in the clinical outcomes based on NAHS score between group 3 and the other two groups in 24 months (p < 0.043).
In the post-operative complication rate, we found that the most common complication was perineal hypaesthesia—it was present in all groups with no statistical difference. This complication was associated with longer time (over 55 minutes) and in 86% of cases it was associated with male gender. This complication resolved with no sequelae in all cases within three weeks.
The formation of PAO was present in all groups at a comparable percentage and also with no significant difference observed.
The main complication was AVN and worsening of osteoarthritis. For groups 1 and 2 it was always associated with longer anamnesis of hip pain and it occurred in patients over 50 years of age. All cases of AVN were treated by a total hip arthroplasty with good results. In all patients, AVN manifested in the period of six to 12 months after the arthroscopic surgery with femoral head collapse noticed on X-rays. The total incidence of AVN was 3.3% (5/150) with no AVN present in group 3. This difference was assessed to be statistically significant. The conversion rate due to worsening of hip arthritis was also significantly lower for group 3, compared to the other groups.
Based on the statistical outcome evaluation, we constructed two separate graphs comparing the NASH score, the difference in surgical time, and complication rates for all groups in order to demonstrate the learning curve difference (Figs. 1 and 2).

Comparison of clinical results and complication rate during the learning curve

Comparison of surgical time during the learning curve
Discussion
Hip arthroscopy is a demanding procedure for treatment of various hip pathologies. Good clinical outcomes are based on learning the basic surgical skills, and it is essential to follow specific safety measures to reduce the complication rate and maintain safety of the procedure [9]. In our study, we concentrated on prospective comparison of surgical times and clinical results for a single surgeon performing hip arthroscopy. This evaluation may help to improve the education and training of surgeons willing to perform hip arthroscopy and help them to focus on the main problems and pitfalls of hip arthroscopy.
In literature, there are several studies comparing merely the surgical time of procedures or radiologic outcome findings for hip arthroscopy as the leading criteria to evaluate the learning curve after the surgery [10, 11]. In our study, we observed that the total surgical time as a sole measure is not good enough to evaluate the hip arthroscopy learning curve, as it depends more on the type of procedure performed. We found that with more experience the time necessary to set up portals is significantly shorter, leaving more time to perform more complex reconstruction procedures while maintaining comparable traction time.
In our study, we evaluated clinical outcomes and complication rates after hip arthroscopy as major indicators of success. As we observed, most of the severe complications such as worsening of OA or AVN were recorded at the beginning of the learning curve. We assume that the main reason of the relatively high complication rate is improper patient selection during the initial phase of the learning curve rather than a surgical mistake. In our hands, patient selection improved with the more cases performed, based on the surgeon’s experience and feedback, and along with improved surgical technique, the complication rate dropped significantly.
In recent literature, there is a consensus that hip arthroscopy is more complicated compared to knee arthroscopy and a greater number of surgical cases is needed to gain the basic surgical skills [5,6,7]. Konan suggests that 30 cases of hip arthroscopy are enough to establish good surgical skills [4]. In our study, we found that the number of cases to gain appropriate surgical skills and achieve good clinical results is at least 100 cases, even for surgeons previously trained in shoulder and knee arthroscopy, as previously reported by Boden [3]. Our study concentrated mainly on the cumulative number of cases needed to produce stable clinical results and to gain basic surgical skills, assuming the surgeon preforms at least 20 procedures per year. For surgeons that specialise in hip arthroscopy, it is essential to maintain a constant number of cases per year to maintain their skills. The total number needed for routine performance is based not only on clinical outcome evaluation, but also on the types of procedures performed.
We did not aim to concentrate on a comparison between different joint arthroscopies, but we decided to evaluate specific types of procedures performed at hip arthroscopy by a single surgeon during the initial learning curve, as this evaluation may lead to improvement of the training process. Dietrich also proved in his study that supervision during initial stages of the hip arthroscopy learning curve significantly minimises the occurrence of complications [12].
We observed that in the early stages of training for hip arthroscopy, the portal set up consumes a significant amount of surgical and traction time that may be used to perform more complex procedures. This phenomenon was not yet observed and quantified in literature. In our study, we did not observe a gradual decrease of the surgical time during the learning curve, but the stabilisation of surgical time was observed with more complex procedures being performed in later stages of the learning curve. We assume that stabilisation of surgical time goes in correlation with better understanding of hip pathology and principles of treatment.
The biggest challenge for the hip arthroscopy surgeon is certainly learning the indications and limitations for the hip arthroscopy [13]. The main indication remains FAI syndrome and associated pathology of the hip joint with limitations that must be respected [14]. According to the literature, there is not a significant difference between hip arthroscopy and surgical hip dislocation in radiographic outcomes of CAM lesion treatment. However, hip dislocation is considered to be a more precise and safe method of treatment of large CAM lesions [15]. According to these findings, surgeons should concentrate on small CAM lesions or mild combined type of impingement, especially in the beginning of the learning curve. Large CAM lesions or pincer type of pathology are more suitable for open surgical hip dislocation or very experienced hip arthroscopy surgeons [16]. Our study also supports this theory, as we observed severe complications in the beginning of the learning curve such as AVN or the worsening of osteoarthritis. These complications come more often from improperly chosen patients or imprecise indication, rather than from surgical mistakes [11, 17].
Conclusion
Hip arthroscopy is a complex procedure that needs a longer time to stabilise surgical skills compared to reconstructive arthroscopy in other joints. It is however a useful tool to achieve very good results in hip reconstructive surgery, if proper indications and techniques are respected. The results support our theory that at the beginning of the learning curve, surgeons should concentrate on simple procedures such as CAM lesion resection and proper portal establishment to avoid prolonged surgical time and increased complication rate.
References
de Amorim Cabrita HA, de Castro Trindade CA, de Campos Gurgel HM, Leal RD, de Souza Marques Rda F (2014) Hip arthroscopy. Rev Bras Ortop 50(3):245–253
Hoppe DJ, de Sa D, Simunovic N, Bhandari M, Safran MR, Larson CM, Ayeni OR (2014) The learning curve for hip arthroscopy: a systematic review. Arthroscopy 30(3):389–397
Boden RA, Wall AP, Fehily MJ (2014) Results of the learning curve for interventional hip arthroscopy: a prospective study. Acta Orthop Belg 80(1):39–44
Konan S, Rhee SJ, Haddad FS (2011) Hip arthroscopy: analysis of a single surgeon’s learning experience. J Bone Joint Surg Am 93(Suppl 2):52–56
Lee YK, Ha YC, Hwang DS, Koo KH (2013) Learning curve of basic hip arthroscopy technique: CUSUM analysis. Knee Surg Sports Traumatol Arthrosc 21(8):1940–1944
Hodgins JL, Veillette C, Biau D, Sonnadara R (2014) The knee arthroscopy learning curve: quantitative assessment of surgical skills. Arthroscopy 30(5):613–621
Howells NR, Auplish S, Hand GC, Gill HS, Carr AJ, Rees JL (2009) Retention of arthroscopic shoulder skills learned with use of a simulator. Demonstration of a learning curve and loss of performance level after a time delay. J Bone Joint Surg Am 91(5):1207–1213
Christensen CP, Althausen PL, Mittleman MA, Lee JA, McCarthy JC (2003) The nonarthritic hip score: reliable and validated. Clin Orthop Relat Res 406:75–83
Gupta A, Redmond JM, Hammarstedt JE, Schwindel L, Domb BG (2014) Safety measures in hip arthroscopy and their efficacy in minimizing complications: a systematic review of the evidence. Arthroscopy 30(10):1342–1348
Park MS, Yoon SJ, Kim YJ, Chung WC (2014) Hip arthroscopy for femoroacetabular impingement: the changing nature and severity of associated complications over time. Arthroscopy 30(8):957–963
Oak N, Mendez-Zfass M, Lesniak BP, Larson CM, Kelly BT, Bedi A (2013) Complications in hip arthroscopy. Sports Med Arthrosc 21(2):97–105
Dietrich F, Ries C, Eiermann C, Miehlke W, Sobau C (2014) Complications in hip arthroscopy: necessity of supervision during the learning curve. Knee Surg Sports Traumatol Arthrosc 22(4):953–958
Burrus MT, Cowan JB, Bedi A (2016) Avoiding failure in hip arthroscopy: complications, pearls, and pitfalls. Clin Sports Med 35(3):487–501
Fayad TE, Khan MA, Haddad FS (2013) Femoroacetabular impingement: an arthroscopic solution. Bone Joint J 95-B:26–30
Bedi A, Zaltz I, De La Torre K, Kelly BT (2011) Radiographic comparison of surgical hip dislocation and hip arthroscopy for treatment of cam deformity in femoroacetabular impingement. Am J Sports Med 39(Suppl):20S–28S
Byrd JW (2017) Editorial commentary: hip femoroacetabular impingement correction: risk versus reward, or how much is too much? Arthroscopy 33(4):780–782
Souza BG, Dani WS, Honda EK, Ricioli W Jr, Guimarães RP, Ono NK, Polesello GC (2010) Do complications in hip arthroscopy change with experience? Arthroscopy 26:1053–1057
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors state that this study was in compliance with regional ethical standards and laws. This study was supported by a grant from the Ministry of Health, Czech Republic - conceptual development of research organisation, Motol Univesity Hospital, Prague, Czech Republic No.00064203. On behalf of all authors, the corresponding author states that there are no other conflicts of interest.
Rights and permissions
About this article

Cite this article
Kautzner, J., Zeman, P., Stančák, A. et al. Hip arthroscopy learning curve: a prospective single-surgeon study. International Orthopaedics (SICOT) 42, 777–782 (2018). https://doi.org/10.1007/s00264-017-3666-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-017-3666-0