
Abstract
Background
The literature on ankle valgus development after procuring non-vascularised fibular grafts in children is still scanty. The non-vascularised fibular graft has distinction of fibular regeneration occurring at the donor site.
Material and methods
We retrospectively analysed the valgus deformities at the donor leg following harvest of non-vascularised fibular graft to determine the various contributing factors in growing children. All these patients had minimum two years post index procedure follow up.
The radiological ankle valgus was quantified using Malhotra’s distal fibular station (0-3), Lateral distal tibial angle (LDTA <84 degrees) and Talar tilt angle >5 degrees. Clinical parameters, evaluated additionally were pain and neuromuscular deficits in the donor limb, if any.
Results
A total of 30 ankles in 23 patients were evaluated. The average patient age was 9.56 years. There was no pain or neuromuscular deficit in the examined limbs at a mean follow up of 39.4 months. The continuity of the fibula in the longitudinal dimension was already restored in 90% limbs. There was presence of radiological valgus deformity in 10 (33%) ankles. The LDTA was abnormal in 80% and talar tilt in 50% valgus ankles. The ankle valgus deformity was found despite the presence of a normal Malhotra station 0. The age of the patient did not seem to influence the ankle valgus deformity.
Conclusions
Radiological ankle valgus is a common occurrence even following non-vascularised fibular harvest. The presence of a regenerated fibula in continuity (90% legs) and almost of similar anatomical longitudinal dimensions (97%) did not deter development of valgus deformity at ankle.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
The fibula is a potential autogenous bone graft site in children. Both non-vascularised and vascularised fibular harvesting have remained an important armamentarium of the paediatric orthopaedic surgeon. In the last few years, there has been a spate of reports listing complications from vascularised fibular harvest in children. Of these, progressive ankle valgus following fibular harvest is a specific complication of the growing child. The morbidity has most commonly being associated with vascularised fibular grafts [1–6]. One of the prominent reasons cited for valgus deformity following vascularised fibular harvest is the mechanical disadvantage of fibular gap [1–6].
The literature on ankle valgus development after procuring non-vascularised fibular graft in children is still scanty [7]. The non-vascularised fibular graft has distinction from the vascularised graft as the fibular regeneration occurs at the donor site [7, 8].
We retrospectively analysed the valgus deformities at the donor leg following harvest of non-vascularised fibular graft to determine the various contributing factor in growing children. All these patients had minimum two years post index procedure follow up.
Material and methods
The retrospective study was conducted at a tertiary care paediatric super specialty hospital in a low income country between April-Sept 2016. Ethical clearance for the study was obtained from the Institution’s Scientific Committee. The operative details were checked from patient’s case records. All patients with age less than 12 years at the time of index procedure, who had undergone any orthopaedic operative procedure at least two years ago, utilizing non-vascularised fibular bone harvest were included in the study. In all included cases, the index procedure required harvest of the maximum possible length of fibular graft available. Patient with neuromuscular problems in donor leg or bony pathology in ipsilateral tibia or fibula and index procedures requiring osteoarticular or smaller fibula graft lengths were excluded.
Our institutional protocol prescribes using a periosteum preserving technique for fibular harvest and conserving a minimum of 10% of total length at either fibular ends to maintain ankle stability at distal end and for safety of deep peroneal nerve at proximal end [9, 10]. Following the harvest, patients were mobilised in a bulky bandage for support and weight bearing initiated soon after pain subsided.
At follow up, clinical parameters evaluated were pain and neuromuscular deficits in the donor limb, if any. The radiological measurements were done on standardized anteroposterior standing x-ray of both legs including knee and ankle joint with patella facing forward. The radiological ankle valgus was quantified using three parameters [11–13]: Distal fibular station using Malhotra grading (grade 0 is fibular growth plate at the level of the talar plateau, grade 1 is fibular growth plate between the top of the talus and the distal tibial growth plate, grade 2 is fibular growth plate in line with the distal tibial growth plate, grade 3 is severe migration with fibular growth plate proximal to the distal tibial growth plate), lateral distal tibial angle (LDTA, the angle between the tibial mechanical axis and the distal tibial joint surface; normal range, 84-92 degrees) and Talar tilt angle (The angle between tangential line along talar plateau and other line along distal tibial joint; normal range, 0-5 degrees). A Malhotra grading of 0 was considered normal [11, 12]. For the purpose of the study, significant radiological ankle valgus was defined as presence of LDTA < 84 degrees and/or talar tilt >5 degrees or both [12, 13].
Results
A total of 30 ankles in 23 patients were evaluated for valgus deformity. The harvest of fibula was bilateral in seven patients. The average patient age at time of follow up was 9.56 years (range, 5-14 years). The average follow up was 39.4 months (range, 24-83 months). The continuity of fibula in longitudinal dimension was restored in 27/30 legs (90%) by that time. Clinically, there was no pain or neuromuscular deficit in the examined limbs at final follow up. Further, there was no symptomatology related to harvest limb reported by any child. There was presence of radiological valgus deformity in ten (33%) ankles (Table 1). The various parameters associated with ankle valgus analysed are as follows:
-
1.
Ankle valgus, LDTA and Talar tilt angle (Table 1). The LDTA was <84 degrees in 8/10 (80%) and talar tilt was >5 degrees in 5/10 (50%) ankles. Thus, abnormal LDTA was more responsible for ankle valgus deformity than talar tilt in observed ankles. The combination of abnormal LDTA and talar tilt was seen in just 3/10 (30%) ankles.
-
2.
Ankle valgus and Malhotra grading (Table 1). In 7/10 (70%) valgus ankle, the Malhotra grading was beyond 0 (patients 1,2,5-7,9,10) (Fig. 1). The grade was 1 in four, 2 in two and 3 in one ankle. The contralateral ankles also showed altered Malhotra grading of 1 in 5 ankles (patients 1,2,6,7,9). No valgus was noted in these normal ankles despite the altered Malhotra grading (Fig. 2). Malhotra grading 0 was also found associated with abnormal LDTA/ talar tilt (patients 3,4,8,10) (Fig. 3).
Fig. 1 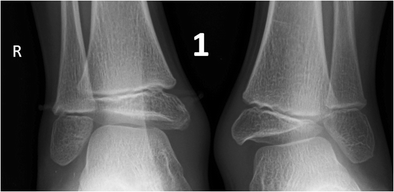
The combination of abnormal LDTA, talar tilt and a higher Malhotra’s fibular station was not a prerequisite for radiological ankle valgus deformity. Anteroposterior radiographs of patient 1 show LDTA within range of 84 degrees, talar tilt 15 degrees and a Malhotra grading of 3 in left ankle. The contralateral normal ankle also showed a fibular station of 1. The regenerated and contralateral fibular lengths were also comparable in this patient
Fig. 2 
The Malhotra grading of 1 was found in many patients with normal ankles. The Malhotra grading was 1 in both ankles in patients 7 and 9, but radiological ankle valgus deformity was on the harvested right side only
Fig. 3 
In many ankles, the abnormal LDTA and/ talar tilt was solely responsible for radiological ankle valgus. The Malhotra grading was 0 in both ankles, e.g. patient 3,4,8 (also see Fig. 1 above)
-
3.
Malhotra grading and fibular shortening (Table 1). No statistical difference was found in regenerated and contralateral fibular lengths in seven ankles (patients 1,2,5-7,9,10) with Malhotra grading above 0 (p = 0.10). However, in the above patients, the grading changed to 2 or 3 when LDTA or talar tilt was highly altered (patient 1, 2 and 6). These findings infer that Malhotra grading is not purely an index of fibular shortening. The dimensions of lower tibial epiphysis and talar tilt also influence Malhotra grading.
-
4.
Ankle valgus and non-continuity of regenerated fibula (Tables 1 and 2). Non-continuity was encountered in three regenerated fibulae all in middle segment (patients 2,10,12) (Fig. 4). The approximate shortening in these fibulae (gap/ length of contralateral fibula) due to non-continuity were 0.3/20.3(1.4%) (patient 2), 2.1/10.67 (19.7%) (patient 10) and 0.8/22.6 (3.5%) (patient 12). Radiological ankle valgus was present in 2 ankles (patients 2, 10) but absent in 1 (patient 12). The Malhotra grading was 1 in 2 ankles (patient 10, 12) and 2 in 1 ankle (patient 2).
Table 2 Patients with unilateral fibular harvest without radiological ankle valgus (n = 6) Fig. 4 
Non-continuity was encountered in three regenerated fibulae all in middle segment (patients 2,10,12). Patients 2 and 10 had radiological ankle valgus deformity but absent in patient 12. The Malhotra grading was 1 in patients 10 and 12 and at 2 in patient 2 on affected side
-
5.
Ankles with and without radiological valgus: age, duration of follow up, fibular shortening and Malhotra grading (Tables 1, 2 and 3). There was no statistical significant difference (p = 0.35) in age of patients with or without the presence of radiological valgus deformity. The ten patients who developed ankle valgus had a mean age of 10.4 ± 2.5 years while 13 patients who did not develop the valgus deformity at ankle had a mean age of 9.3 ± 2.5 years.
Table 3 Patients with bilateral fibular harvest with no radiological ankle valgus (n = 7)*




The follow up duration of these two subsets of patients was also not statistically significant (p = 0.08). Ten ankles developing valgus deformity had average follow up of 45.8 months (range, 25-83 months) while 20 ankles which did not develop valgus deformity had average follow up of 36.65 months (range, 27-58 months). The average regenerated fibular length was 97.17% in ten ankles which had valgus deformity. The average regenerated fibular length was 99.1% when compared to contralateral normal legs in cases where unilateral fibula was harvested (n = 6). This difference was not statistically significant (p = 0.67).
The Malhotra grading was 1 in four harvested fibulae without radiological ankle valgus deformity (patients 11,12,14,15) again strengthening the finding that Malhotra grading alone is not a predictor of ankle valgus (see 2 above) (Table 2).
Discussion
The fibular harvest is associated with several potential morbidities in a growing child. Progressive ankle valgus is one of the specific deformities encountered after this procedure. The incidence of valgus deformity is 16.1% according to Nathan [2]. Fragniere et al found that 45% of children had ankle valgus after free fibula harvest. In their series, the deformities were severe in 25% [6]. The morbidity has most frequently been reported from the vascularised fibular harvest series, where regeneration of donor fibular does not occur. Moreover, in several of these series, the purpose was oncological reconstruction requiring complete harvest of proximal or distal portions of fibula [1].
The non-vascularised bone graft has distinction of early donor fibular regeneration [8, 14]. Steinlechner and Mkandawire used non-vascularised fibular grafting for reconstruction of long bone defects after sequestrectomy in a series of seven children. They had six fibulae with regrowth in continuity within 19.3 weeks (range, 6 to 75 weeks) [14]. The authors opined that early restoration of fibular continuity led to stabilization of the ankle in the donor leg and even suggested reutilization of regenerated fibulae [14].
The literature on fibular regeneration and other long term impacts on donor site after procuring non-vascularised fibular graft in children is still scanty [7, 15]. A series of 23 children (24 harvested fibulae) with average age 8.9 years (range, 4-14 years) reported by González-Herranz et al showed incomplete fibular regeneration or non-union in 14 cases (58%) [15]. There were radiological findings of distal migration of the fibula head in 18 cases (75%, but without clinical relevance), lateral cortical tibial thickening in five cases (21%), talar tilt in 11 cases (46%), proximal migration of the distal end fibula in 13 cases (54%), and diaphyseal valgus of the tibia in five cases (21%). The average follow up in their series was 6.2 years (range, 4-11 years). The study however was quite heterogeneous with harvest of different anatomical fibular portions (head, proximal diaphysis, middle diaphysis, distal diaphysis, lateral malleolus) and variable lengths of fibula graft (2-24 cm, average 9.9 cm). There was primary tumour of fibula in seven cases. In half of their cases, the distal tibiofibular joint was stabilised with a suprasyndesmal screw or a Kirschner wire. Periosteum preservation of fibula was also not uniform in all cases [15].
Another series on harvest of non-vascularised fibula series by Xin et al described 17 children with an average age of 8.4 years (range, 2-13 years), and mean follow-up of 31 months (range, 7-65 months) [7]. The fibula was harvested using a periosteum-preserving technique. Variable lengths of fibula were harvested (average 28%; range 10-58%). The authors divided patients into two groups—nine harvest sites were filled with cancellous allograft and eight with calcium sulfate. No significant donor site complications were reported in this series with fibular regeneration being evident in all cases at a mean follow up of 12 weeks (range, 4-21 weeks) [7]. Our study did not involve resection of either proximal or distal fibular epiphysis and a uniform surgical procedure with periosteal preservation was utilised. The fibular graft site regeneration was a natural process and we did not use any allograft or calcium supplements to augment the harvest site in any of our patients.
Nathan et al investigated the timing of development of ankle valgus in vascularised fibular grafting [2]. Children were first noted to have ankle deformity 32 months (range, 20-38 months) after their primary surgical procedures. In our series, we could not predict at what age the ankle valgus started developing as this retrospective analysis was performed about 39.4 months (range, 24-83 months) after the index procedure. However, by this time 33% ankles had already developed radiological valgus deformity. A previous report from our institution has prospectively analysed short term donor site characteristics following non-vascularised fibula harvest [8]. There were 16 children with 21 harvested fibula. There was regeneration of fibula similar to the pre-operative dimensions as early as six months in 71% of cases. The non-continuous regeneration (29%) had no clinical implications including valgus in short term.
During weight bearing, approximately one sixth of the weight is transmitted by fibula [16]. In a normal ankle, a uniform axial load applied to distal tibia and fibula results in balanced growth of lower tibial epiphysis. In fibular gap nonunions, in weight bearing positions, there is loss of a normal physiological load transmission through fibular side. Further, there is upward dragging of the remaining distal fibula by the contracted fibrous scar around the gap (tethering effect). The epiphyseal growth at the lateral distal tibial epiphysis is thus inhibited by eccentrical ankle loading resulting in progressive ankle valgus [16]. The fibular resection also leaves a mobile distal remnant which is unable to resist pressure from the talus during weight-bearing. In fact, shortening of the fibula, lateral wedging of the distal tibial epiphysis, and lateral tilt of the talus at the ankle mortise are supposed to be closely related [11]. The anatomical obliquity of the ankle mortise in a normal child before the age of 10 years, general laxity of ligaments in children, and weakness of the tibialis posterior muscle are other factors postulated for ankle valgus [1, 2].
Multiple techniques have been deployed to tackle the ankle valgus following harvest: leaving a distal fibular remnant greater than 5-6 cm, the utilization of age—residual fibula index (age in years plus residual fibular length in centimetres) less than 16, distal tibiofibular arthodesis, donor site fibular osteosynthesis, scheduling surgical harvest at age older than eight years, distal medial tibial epiphysiodesis, supramalleolar corrective osteotomy [1–6].
A review of literature also highlights that none of the above postulated preventive procedures is absolutely capable of aborting the progressive valgus deformity [3, 16]. Clearly, there are factors other than the above described which are responsible for progressive ankle valgus. The development of ankle valgus is probably a delayed process >6 months after harvest [2, 8]. Adequate distal fibular support (10% of total fibular length) had been ensured for all our cases. The clinical examination for neuromuscular weakness in harvested limbs at follow up was normal. The fibular continuity in length had already been restored in 90% limbs by that time. The fibular shortening in these cases was also not statistically significant. The presence of a regenerated fibula in continuity and comparable dimensions in non-vascularised donor sites points to a different aetiology for ankle valgus rather than the commonly postulated mechanical theory. The lateral half of lower tibial epiphysis has different anatomical characteristics than its medial half. Vascular studies in rabbits have indicated that lower tibial end is a composite bone formed in two portions and each has its separate blood supply [17]. The medial half has a constant blood supply whereas the lateral half is supplied from an accessory nutrient artery. The differential physiological epiphysiodesis of lateral epiphysis causing triplanar fractures is already known. There was abnormal LDTA in 80%, talar tilt in 50% valgus ankles and in 30% both LDTA and talar tilt were abnormal. The LDTA is closely related to lower tibial epiphysis and talar angle to medial tibiotalar ligaments and talar dome obliquity. It still remains unknown whether their alteration is cause or effect of ankle valgus deformity. Development of progressive ankle valgus therefore appears more of a multifactorial phenomenon.
There were some limitations of our study. It was a retrospective study where initial and immediate post-operative radiographs of harvest site were not available. The calculation of residual fibular index was therefore not possible. Comparisons to a normal fibula were possible only in unilateral harvest cases. Only the longitudinal dimension of fibula in anteroposterior radiographs was taken into consideration for calculation purpose. The strengths of the current study were a dedicated long term follow up study performed on a homogenous group consisting of only healthy fibular harvest (excluding pathological fibulae). These grafts shared the uniform characteristics of a near total fibular harvest, preserved proximal and distal epiphysis with a reasonable distal fibular support.
Our study showed that radiological ankle valgus is a common occurrence (33%) even following non-vascularised fibular harvest. The presence of a regenerated fibula in continuity (90% legs) and almost of similar anatomical longitudinal dimensions (97%) did not deter development of valgus deformity at ankle. The ankle valgus was found despite the presence of a normal Malhotra grading of 0 (patients 3,4,8,10). Malhotra grading upto 1 may be considered normal in growing children with some inherent laxity in ligaments (patients 1,2,6,7,9). Further, abnormal Malhotra grading in isolation did not predict fibular shortening or ankle valgus deformity. Non-continuity of regenerated fibula may be one factor for ankle valgus deformity but is not an absolute indicator for its development (patient 12). Age of the patients too did not seem to influence the ankle valgus deformity (p = 0.35). Since, the development of ankle valgus deformity in children appears to be a delayed and a progressive phenomenon, there is a need to keep these children under regular follow up. More research is warranted to decipher the exact characteristics of this pathology.
References
Sulaiman AR, Wan Z, Awang S, Che Ahmad A, Halim AS, Ahmad Mohd Zain R (2015) Long-term effect on foot and ankle donor site following vascularized fibular graft resection in children. J Pediatr Orthop B 24:450–455
Nathan SS, Athanasian E, Boland PJ, Healey JH (2009) Valgus ankle deformity after vascularized fibular reconstruction for oncologic disease. Ann Surg Oncol 16:1938–1945
Iamaguchi RB, Fucs PM, da Costa AC, Chakkour I (2011) Vascularised fibular graft for the treatment of congenital pseudarthrosis of the tibia: long-term complications in the donor leg. Int Orthop 35:1065–1070
Kanaya K, Wada T, Kura H, Yamashita T, Usui M, Ishii S (2002) Valgus deformity of the ankle following harvesting of a vascularized fibular graft in children. J Reconstr Microsurg 18:91–96
Omokawa S, Tamai S, Takakura Y, Yajima H, Kawanishi K (1996) A long-term study of the donor-site ankle after vascularized fibula grafts in children. Microsurgery 17:162–166
Fragnière B, Wicart P, Mascard E, Dubousset J (2003) Prevention of ankle valgus after vascularized fibular grafts in children. Clin Orthop Relat Res 408:245–251
Xin Z, Kim K, Jung S (2009) Regeneration of the fibula using a periosteum-preserving technique in children. Orthopedics 32:820
Agarwal A, Kumar A (2016) Fibula regeneration following non-vascularized graft harvest in children. Int Orthop 40:2191–2197
Pacelli LL, Gillard J, McLoughlin SW, Buehler MJ (2003) A biomechanical analysis of donor-site ankle instability following free fibular graft harvest. J Bone Joint Surg Am 85:597–603
Soejima O, Ogata K, Ishinishi T, Fukahori Y, Miyauchi R (1994) Anatomic considerations of the peroneal nerve for division of the fibula during high tibial osteotomy. Orthop Rev 23:244–247
Malhotra D, Puri R, Owen R (1984) Valgus deformity of the ankle in children with spina bifida aperta. J Bone Joint Surg Br 66:381–385
Stevens PM (2015) Pediatric ankle valgus: background, anatomy, pathophysiology. emedicine.medscape.com/article/1358051-overview. Accessed 15 March 2016
Cox JS, Hewes TF (1979) “Normal” talar tilt angle. Clin Orthop Relat Res 140:37–41
Steinlechner CW, Mkandawire NC (2005) Non-vascularised fibular transfer in the management of defects of long bones after sequestrectomy in children. J Bone Joint Surg Br 87:1259–1263
González-Herranz P, del Río A, Burgos J, López-Mondejar JA, Rapariz JM (2003) Valgus deformity after fibular resection in children. J Pediatr Orthop 23:55–59
Kang SH, Rhee SK, Song SW, Chung JW, Kim YC, Suhl KH (2010) Ankle deformity secondary to acquired fibular segmental defect in children. Clin Orthop Surg 2:179–185
Morgan JD (1959) Blood supply of growing rabbit’s tibia. J Bone Joint Surg Br 41:185–203
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
There is no funding source.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Hospital Scientific Committee approved the study.
Informed consent
Informed consent was obtained from all individual (patient’s parents) participants included in the study.
Rights and permissions
About this article

Cite this article
Agarwal, A., Kumar, D., Agrawal, N. et al. Ankle valgus following non-vascularized fibular grafts in children—an outcome evaluation minimum two years after fibular harvest. International Orthopaedics (SICOT) 41, 949–955 (2017). https://doi.org/10.1007/s00264-017-3403-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-017-3403-8