
Abstract
Purpose
There remains little consensus regarding the optimal management of distal radius fractures. Fixed angle volar devices have gained recent popularity, but have also been associated with soft tissue complications. Intramedullary (IM) devices offer fixed angle stabilisation with minimally invasive surgical technique and low, IM profile. No formal review of outcomes could be identified.
Methods
We conducted a systematic review of clinical studies regarding the use of fixed angle IM devices in acute extra-articular or simple intra-articular distal radius fractures. Preferred Reporting Items for Systematic Reviews (PRISMA) guidance was followed. Numerical data regarding functional scores, ranges of movement, radiological outcomes and complications were pooled to produce aggregate means and standard deviation.
Results
A total of 310 titles and abstracts were identified. Fourteen papers remained for analysis. Total patient number was 357, mean age 63.72 years and mean follow-up 12.77 months. Mean functional scores were all rated as ‘excellent’. Aggregate means: flexion 53.62°, extension 56.38°, pronation 69.10°, supination 70.29°, ulnar deviation 28.35°, radial deviation 18.12°, radial height 8.98 mm, radial inclination 16.51°, volar tilt 5.35°, ulnar variance 0.66 mm and grip strength 90.37 %. Overall complication rate was 19.6 %. Tendon rupture was unreported. Tendon irritation was 0.88 %. Radial nerve paraesthesia was 11.44 %.
Conclusions
Fixed angle IM devices facilitate excellent functional outcomes, with radiological and clinical parameters at least equivalent to volar plate devices. Low rates of tendon irritation and absence of tendon rupture are advantageous. Significant limitations include a lack of application for complex articular injuries and the propensity to cause a transient neuritis of the superficial branch of the radial nerve.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Distal radius fractures are the most common of all fractures [1] and account for around 2.5 % of all emergency department visits [2]. The number of distal radius fractures are expected to rise due to the aging population [3].
Treatment remains controversial; a recent Cochrane review offers little consensus with regard to how best to manage these injuries [4]. Historically, they were generally treated non-operatively in a plaster cast. However, some studies have demonstrated a correlation between restoration of normal anatomy and improvement in function [5–7]
Locking plate devices facilitate a stable anatomical reduction, as well as early mobilisation, and the volar locking plate has become increasingly popular over the last decade [8]. A recent epidemiological study from Sweden found a threefold increase in the use of volar plates over the last five years [9]. Despite this recent surge in use, other studies have found clinical outcomes following volar plating for distal radius fractures in elderly patients are no better than the results of plaster cast treatment [10].
Bentohami et al. [10] conducted a recent systematic review of complications following volar locking plate fixation for distal radius fractures and reported an overall complication rate of 16 % including tendon rupture and irritation, carpal tunnel syndrome (CTS) and neuritis. Furthermore, between 15 and 34 % of patients required their hardware to be removed within a year [11, 12].
Whilst their application in the management of complex fractures is likely to contribute to the above figures, the review nonetheless illustrates that volar locking plates are not without issue. This has prompted others to seek alternative methods for fixation, and in 2005 Tan et al. [13] introduced the first fixed angle intramedullary (IM) device, the Micronail® (Wright Medical Technology, Inc., Memphis, TN, USA). This provides an alternative treatment modality for unstable extra-articular, or simple intra-articular fracture, with proposed advantages including minimal soft tissue disruption and periosteal stripping, and a low IM profile.
Two similar systems have subsequently been released, the Sonoma WRx® (Sonoma Orthopedic Products, Inc., Buffalo Grove, IL, USA) and the Targon® DR (B. Braun, Melsungen, Germany). All three devices are inserted via the radial styloid and facilitate fixed angle stabilisation via distal locking screws. Both the Micronail® and Targon® DR derive axial and rotational stability via proximal screws inserted using a jig. The WRx® utilises an expanding mechanism on the proximal end, which anchors the device in the medullary canal.
Several studies have reported promising results with these devices, but to date no formal review of outcomes has been published and they have not yet reached the same level of popularity as volar locking plates. We therefore performed a systematic review to evaluate the clinical, functional and radiological outcomes for primary fixation of unstable extra-articular or simple intra-articular distal radius fractures using a fixed angle IM device.
Materials and methods
We performed a systematic review of clinical studies (Level of evidence II–IV) related to the use of fixed angle IM devices for extra-articular or simple intra-articular distal radius fracture using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Search
Publically available data were searched using the Healthcare Databases Advanced Search (HDAS) tool to identify studies from both the MEDLINE (PubMed) and Excerpta Medica (EMBASE) databases on 15 December 2014. Keywords were identified via discussion between the first and third authors (Appendix 1). The following search terms were then derived using standard Boolean logic:
(“distal radi*” OR “radi* fracture OR colles OR smiths) AND (intramedullary OR IM OR nail OR micronail OR “targon dr” OR “sonoma wrx”). Additionally, the reference lists of the full papers identified for analysis were searched for any further relevant articles. Only studies in English were included.
Inclusion criteria
Skeletally mature adults (>18 years) with acute extra-articular or simple intra-articular distal radius fractures were eligible. Simple intra-articular fracture included AO types A2, B1, B2, B3, C1 and C2, as per manufacturers’ recommendations for IM fixation.
Exclusion criteria
Polytrauma, skeletally immature patients, revision procedures or complex intra-articular fractures (AO C3) were excluded. Biomechanical studies, systematic reviews/meta-analyses, novel techniques, perception-based studies and single case reports were not included. Data given without ranges or standard deviation (SD) were not included for analysis.
Evaluated outcomes
Functional scores [e.g. Disabilities of the Arm, Shoulder and Hand (DASH) score, Mayo wrist score and Gartland and Werley score], ranges of movement (ROM), grip strength (units of force, or as a percentage of the uninjured hand), radiological outcomes (e.g. radial height, radial inclination, volar tilt and ulnar variance) and reported complications were evaluated.
Study selection
Duplicate results were removed by the HDAS search tool, and the remaining titles and abstracts were screened by the first and third authors for eligibility. In the event of any discrepancy, the senior author would have the final decision as to whether the study was included for analysis. Eligible full-text articles were assessed against the above inclusion and exclusion criteria.
Numerical data were pooled to produce aggregate means and SD. Where SD was not stated in the original text, it was calculated using raw data where available. Failing this, an estimated SD was calculated from the sample mean and data ranges, using the statistical methods described elsewhere by Hozo et al. [14].
Results
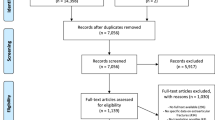
A total of 310 titles and abstracts were identified from the primary search, as well as a further two from reference lists; 91 duplicates were removed, and 201 titles and abstracts deemed inappropriate. Of the remaining 20, four were in non-English languages, one detailed use in comminuted fracture and one reported on outcomes following malunion. Fourteen papers remained for analysis [13, 15–27]. See Fig. 1 for PRISMA flow diagram. Study type, characteristics, post-operative protocol and categories of outcomes reported are summarised in Table 1 (Fig. 2).

Distal radius fracture prior to management with an intramedullary device

Distal radius fracture managed with an intramedullary device
Total patient number across all studies was 357, with a mean age of 63.72 (SD 11.28) years and mean time to follow-up 12.77 months (range three to 24). Pooled numerical data regarding functional scores, ROM, radiological parameters and grip strength are summarised in Table 2.
Clinical outcomes
Numerical DASH scores were reported in seven studies, Mayo scores in four and Gartland and Werley in three. Dremsurp et al. [15] reported the Gartland and Werley scores as the ascribed level of patient satisfaction, with 30 patients scoring excellent, 11 good, two fair and one poor. Similarly, Tajima et al. [23] reported on Mayo scores as 12 patients rating excellent, three fair and one good. Neither of these was included in the pooled data.
Results for flexion and extension were analysed from nine studies, pronation and supination from eight and ulnar and radial deviation from seven. Both Gradl et al., and Tan et al. reported antagonistic movements as a single movement arc. Respective values were: flexion/extension 113° (±22) and 125° (±19), ulnar/radial deviation 53° (±14) and 51° (±9) and pronation/supination 174° (±10) and 165° (±16). These values were not included in the pooled data.
Grip strength was reported as a percentage of the unaffected side in five papers. Both Tajima et al. [23], and Ilyas and Thoder [18] reported mean results of 84 and 91 %, respectively, but neither included a range or SD. These figures were not included in the pooled data. Three papers reported grip strength as an absolute figure in kilograms. All were included for analysis.
Radiological outcomes
Data regarding radial height, radial inclination, volar tilt and ulnar variance were reported in ten, 12, 12 and six studies, respectively. All were included in the pooled data.
Complications
Complications were documented in 13 papers, with an aggregate patient number of 341. Tajima et al. [23] do not comment on their complications and so were excluded from the pooled data. Total figures are summarised in Table 3.
Radial nerve paraesthesia was the most common complication, occurring in a total of 39 patients (11 %). All cases were transient and had resolved at final follow-up without further intervention. Of the five patients going on to require further surgery: one was for loss of reduction, one for loosening of implant, one required carpal tunnel release, one poorly placed distal screw warranted re-positioning and one implant was removed at the patient’s request. Of the three cases where infection was reported, all were superficial in nature and resolved with simple antibiotic management.
Discussion
This study provides the only comprehensive review of expected outcomes using fixed angle IM devices in the management of distal radius fracture. Mean values for functional outcomes were rated as ‘excellent’, independent of the scoring system employed [28–30], and there were no reported incidents of tendon rupture using these devices. There were, however, a significant number of cases where transient radial nerve paraesthesia was reported.
Clinical outcomes
The absolute values for ROM were sufficient to facilitate excellent functional outcomes.
Two studies compared clinical outcomes between IM nail and volar plate fixation. Neither treatment option was observed to have a consistently significant clinical advantage.
In their randomised trial, Gradl et al. [17] identified a significant improvement in pronation/supination using the IM system [nail 177° vs plate 174° (p = 0.05)]. However, Safi et al. [21] did not demonstrate a statistically significant advantage here [supination: nail 83° vs plate 79° (p = 0.06), pronation: nail 82° vs plate 77° (p = 0.08)]. Neither study identified significant differences in flexion, extension or radial and ulnar deviation.
Similarly, no significant difference in grip strength was observed by Gradl et al. [17] [nail 93 %, volar plate 89 % (p = 0.42)]. Safi et al. [21] do not comment on this parameter.
Radiological outcomes
The radiological outcomes reported here show that radial height was the parameter restored closest to the normal anatomical value (mean 8.98 mm, normal values 11–12 mm [31]). Loss of radial height has been associated with pain [32] and diminished grip strength [33], and restoration of this parameter has been considered the most significant for achieving a good functional outcome [5].
Three randomised studies with a total patient number of 128 compared radiological parameters between volar plate and IM nail devices [17, 21, 27]. All commented on volar tilt and radial inclination. Zehir et al. and Safi et al. also commented on radial height, and both Gradl et al. and Safi et al. commented on ulnar variance. No study identified any statistically significant advantage with either device across any of the radiological parameters reported.
Complications
One of the key intended advantages of the IM devices is to minimise soft tissue complications associated with more invasive surgical fixation, and the above results are promising in this regard. There were no reported cases of tendon rupture, and tendon irritation occurred at a low rate (0.88 %). It is however worth noting that whilst standard open techniques may involve more extensive soft tissue dissection than is involved with IM devices, some authors have more recently reported success using minimally invasive techniques in volar plate application [34, 35].
As one might expect, given its proximity to the insertion site, disruption of the superficial branch of the radial nerve was not uncommon, occurring at a rate of over 11 %, and accounting for 58 % of all complications reported. These were, however, all transient lesions and resolved without the need for further intervention.
Orientation of the subchondral screws creates potential for penetration into the distal radio-ulnar joint when malpositioned. The three instances of intra-articular screw placement observed here all came from a single centre and were noted to have arisen from early experiences with the IM system [18]. This suggests a degree of user dependence which may be improved with experience.
Of the three randomised trials comparing plate and nail techniques, none were able to establish a statistically significant difference in overall complication rate [17, 21, 27]. Zehir et al. [27] identified one incidence of tendon irritation, and both Gradl et al. [17] and Safi et al. [21] each reported one incidence of tendon rupture. All three patients were from the volar plate groups of their respective study. No tendon-related complications occurred in the IM nail groups of these studies.
A recent review of published data regarding complications of volar plate fixation between 2000 and 2013 [10] demonstrated comparable rates of superficial infection (0.5 %), loss of reduction (1 %), chronic regional pain syndrome (1.6 %) and CTS (2.8 %) to those seen here. The rate of neuritis was appreciably lower (1.9 %); however, this comparison does not reflect the duration or severity of the deficit. The incidence of tendon rupture (1.7 %) and tendon irritation (3.8 %) after locked volar plating are both higher than observed in this review for IM devices.
It is difficult to make a meaningful statistical comparison here due to the heterogeneity of the patient groups and fracture types. However, the less frequent occurrence of tendon rupture, higher observed rates of tendon irritation and lower rates of neuritis seen after IM fixation are of interest. It is also worth noting that a recent review of patients undergoing volar plate fixation has failed to establish a link between complication rate and severity of fracture, age or sex [36].
Another proposed advantage of the IM devices is the low rate of device removal. Only one case of device removal was reported here, and this was at the patient’s request. Rates of 15–34 % have been reported for volar plates [11, 12].
A major disadvantage with these systems is that the minimally invasive operative technique does not facilitate direct fracture reduction, and the devices are not indicated for comminuted (AO C3 type) fracture. This is a significant limitation, and volar plate devices have a clear advantage in this regard.
Whilst promising, the results of this review are limited by the paucity of existing data. Four Level II studies were identified, but did not consistently comment on all outcomes to facilitate meaningful analysis.
Classification of fracture pattern is also a limiting factor. Severity of injury has been shown to relate to functional outcome [37]. However, the studies identified here did not consistently state the number of patients with each fracture type, so the exact composition of the cohort is not definitely known.
It is also worth noting that neither IM nor volar locking systems are inexpensive solutions to the management of distal radius fractures and that good outcomes can be achieved in simple fractures with use of standard AO plates [38].
Conclusion
Existing data demonstrate that the use of fixed angle IM devices in extra-articular, or simple intra-articular fractures, gives excellent functional outcomes and provides radiological and clinical parameters at least equivalent to those observed using volar plate devices. Tendon rupture remains unreported and rates of tendon irritation low. These devices may have an advantage over more invasive fixed angle implants in this regard. The main drawbacks of the IM systems are the lack of utility to aid fracture reduction, limited application for complex articular injuries and the propensity to cause neuritis of the superficial branch of the radial nerve. However, these nerve injuries are reported here only as a transient, self-limiting issue.
References
Nellans KW, Kowalski E, Chung KC (2012) The epidemiology of distal radius fractures. Hand Clin 28:113–125
Larsen CF, Lauristen J (1993) Epidemiology of acute wrist trauma. Int J Epidemiol 22:911–916
Shauver MJ, Yin H, Banarjee M et al (2011) Current and future national costs to Medicare for the treatment of distal radius fracture in the elderly. J Hand Surg Am 36:1282–1287
Handoll H, Madhok R (2003) Surgical interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev 3:CD003209
Ng CY, McQueen MM (2011) What are the radiological predictors of functional outcome following fractures of the distal radius? J Bone Joint Surg Br 93:145–150
McQueen M, Caspers J (1988) Colles fracture: does the anatomical result affect the final function? J Bone Joint Surg Br 70:649–651
Wilcke MK, Abbaszadegan H, Adolphson PY (2007) Patient-perceived outcomes after displaced distal radius fractures. A comparison between radiological parameters, objective physical variables, and the DASH score. J Hand Ther 20:290–298
Chung KC, Watt AJ, Kotsis SV et al (2006) Treatment of unstable distal radial fractures with the volar locking plate system. J Bone Joint Surg Am 88:2687–2694
Mellstrand-Nevaro C, Pettersson HJ, Tornqvist H, Ponzer S (2014) The operative treatment of fractures of the distal radius is increasing: results from a nationwide Swedish study. Bone Joint J 96-B:963–969
Bentohami A, de Burtlet K, de Korte N, van den Bekerom JC, Goslings JC, Schep NW (2014) Complications following volar locking plate fixation for distal radius fractures: a systematic review. J Hand Surg Eur Vol 39(7):745–754
Williksen JH, Frighagen F, Hellund JC, Kvernmo HD, Husby T (2013) Volar locking plates versus external fixation and adjuvant pin fixation in unstable distal radius fractures: a randomized, controlled study. J Hand Surg Am 38:1469–1476
Knight D, Hajducka C, Will E, McQueen M (2010) Locked volar plating for unstable distal radial fractures: clinical and radiological outcomes. Injury 41:184–189
Chen Y, Chau Y, Cheng C, Tsai M, Chen A (2012) Treatment of extra-articular distal radius fractures using an intramedullary nail. Formos J Musculoskelet Dis 3:116–120
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13
Dremstrup L, Skærbæk M, Olesen S, Høgh S, Hansen T (2013) Good radiological and functional results after intramedullary nailing of distal radius fractures. J Plast Surg Hand Surg 47:286–288
Geerts RW, Toonen HG, van Unen JM, van Vugt R, Werre AJ (2011) A new technique in the treatment of distal radius fractures: the Micronail®. Acta Orthop Traumatol Turc 45(2):85–93
Gradl G, Mielsch N, Wendt M, Falk S, Mittlmeirer T, Gierer P et al (2014) Intramedullary nail versus volar plate fixation of extra-articular distal radius fractures. Two year results of a prospective randomized trial. Injury 45(Suppl 1):S3–S8
Ilyas A, Thoder J (2008) Intramedullary fixation of displaced distal radius fractures: a preliminary report. J Hand Surg Am 33:1706–1715
Nishiwaki M, Tazaki K, Shimizu H, Ilyas A (2011) Prospective study of distal radius fractures treated with an intramedullary nail. J Bone Joint Surg Am 93:1436–1441
Rhee PC, Shin AY (2012) Minimally invasive flexible insertion and rigid intramedullary nail fixation for distal radius fractures. Tech Hand Up Extrem Surg 16:159–165
Safi A, Hart R, Těknědžjan B, Kozák T (2013) Treatment of extra-articular and simple articular distal radial fractures with intramedullary nail verus volar locking plate. J Hand Surg Eur Vol 38:774–779
Schønnemann JO, Hansen TB, Søballe K (2011) Randomised study of non-bridging external fixation compared with intramedullary fixation of unstable distal radial fractures. J Plast Surg Hand Surg 45:232–237
Tajima K, Koba T, Takao E (2012) A simple reduction technique in intramedullary nailing (MICRONAIL) of distal radius fracture - intrafocal elastic-spring pinning method. Hand Surg 17(2):279–285
Takada N, Otsuka T, Kondo A, Fukuta M, Suzuki H, Yamada K (2011) Minimally invasive osteosynthesis with an intramedullary nail for osteoporotic distal radius fractures. Eur J Orthop Surg Traumatol 21:503–509
Tan V, Bratchenko W, Nourbakhsh A, Capo J (2012) Comparative analysis of intramedullary nail fixation versus casting for treatment of distal radius fractures. J Hand Surg Am 37:460–468
van Vugt R, Geerts RW, Werre AJ (2010) Osteosynthesis of distal radius fractures with the Micronail®. Eur J Trauma Emerg Surg 36:471–476
Zehir S, Calbiyik M, Zehir R et al (2014) Intramedullary repair device against volar plating in the reconstruction of extra-articular and simple articular distal radius fractures; a randomized pilot study. Int Orthop 38:1655–1660
Amadio PC, Berquist TH, Smith DK, Ilstrup DM, Cooney WP, Linscheid RL (1989) Scaphoid malunion. J Hand Surg Am 14(4):679–687
Gartland J, Werley CW (1951) Evaluation of healed Colles’ fractures. J Bone Joint Surg Am 33-A(4):895–907
Mattyasovszky SG, Burkhart KJ, Ahlers C et al (2011) Isolated fractures of the greater tuberosity of the proximal humerus: a long-term retrospective study of 30 patients. Acta Orthop 82(6):714–720
Fernandez DL, Jupiter JB (1995) Fractures of the distal radius: a practical approach to management. Springer, New York, pp 54–65
Jenkins NH, Mintowt-Czyz WJ (1988) Mal-union and dysfunction in Colles’ fracture. J Hand Surg Br 13:291–293
McQueen MM, Hajducka C, Court-Brown CM (1996) Redisplaced unstable fractures of the distal radius: a prospective randomised comparison of four methods of treatment. J Bone Joint Surg Br 78:404–409
Fei JL, Liang B, Jiang CZ, Wang LM (2014) Minimally invasive treatment for distal radial fracture and dislocation of type IV based on Fernandez classification. Zhongguo Gu Shang 27(4):341–345
Chmielnicki M, Prokop A (2015) New minimally invasive approach for palmar plating in distal radius fractures. Z Orthop Unfall 153(1):25–28
Ward CM, Kuhl TL, Adams BD (2011) Early complications of volar plating of distal radius fractures and their relationship to surgeon experience. Hand (N Y) 6:185–189
Braziulus K, Rimdeika R, Kregždyté R, Tarasevičius S (2013) Associations between the fracture type and functional outcomes after distal radial fractures treated with a volar locking plate. Medicina (Kaunas) 49(9):399–402
Twigt B, Bemelman M, Lansink K, Leenen L (2013) Type C distal radius fractures treated with conventional AO plates: an easy and cost-saving solution in a locking plate era. Int Orthop 37(3):483–488
Acknowledgments
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
Rights and permissions
About this article

Cite this article
Hardman, J., Al-Hadithy, N., Hester, T. et al. Systematic review of outcomes following fixed angle intramedullary fixation of distal radius fractures. International Orthopaedics (SICOT) 39, 2381–2387 (2015). https://doi.org/10.1007/s00264-015-2763-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-2763-1