
Abstract
Purpose
Most factors considered to affect blood metal ions following metal-on-metal hip replacement are based on hip resurfacing patients. The study aims were to determine which factors affect blood metal ion concentrations following metal-on-metal total hip replacement (MoM THR).
Methods
All unilateral MoM THR patients at one centre with whole-blood cobalt (Co) and chromium (Cr) concentrations measured up to May 2013 were included. Blood sampling was at a mean of 4.5 years (range 1.1–11.8 years) postoperatively.
Results
Of 496 patients (mean age 59.1 years; 52.8 % male), blood metal ions >7 μg/l were observed in 9.7 % (n = 48). Large femoral head sizes (≥38 mm) had significantly higher (p < 0.0001) blood metal ions than smaller sizes (28/36 mm). Corail–Pinnacle implants produced significantly lower blood metal ions compared to other implant designs (p < 0.01 Co and Cr). Univariate linear regression demonstrated the only significant predictors of both blood Co and Cr concentrations were femoral head size (R 2 = 8.6 % Co and R 2 = 3.3 % Cr, both p < 0.0001) and implant design (R 2 = 8.8 %, p = 0.005 Co and R2 = 5.1 %, p = 0.003 Cr). When the three THR implant design groups (Corail–Pinnacle, Synergy, Other) were analysed separately, femoral head size no longer significantly affected blood metal ions in any of the three implant design groups.
Conclusions
Implant design was the most important factor affecting blood metal ion concentrations. We recommend the regularity of follow-up be tailored to survival rates of various MoM THR designs rather than according to femoral head size.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Large-diameter metal-on-metal total hip replacement (MoM THR) became popular for treating patients with hip arthritis over the last decade [1–4], with more than 1 million patients worldwide receiving MoM hip bearings [5]. A number of patients with MoM THRs have developed adverse reactions to metal debris (ARMD), resulting in high short-term revision rates [6–8]. The risk of ARMD is greater in THRs compared with hip resurfacings given the additional metal wear debris, which can be generated at the taper–head interface and other modular junctions [2, 7, 9]. This has led to withdrawal from the market of poorly performing devices [10] and the opinion that MoM THR should no longer be performed [2].
In light of these problems, the Medical and Healthcare Products Regulatory Agency (MHRA) recommend annual follow-up for the life of the implant of all MoM THR patients with femoral head diameters of ≥36 mm and those with recalled implants, regardless of symptoms [11]. This follow-up includes blood metal ion sampling, which is both an accepted surrogate marker of MoM bearing wear and useful in identifying patients with ARMD [12]. Although little is known about the natural history of ARMD [13, 14], it is possible that not all MoM THR patients will develop it [15]. Therefore, it remains unclear how patients should be followed up, especially in the long term.
If MoM THR patients at highest risk of ARMD were identified, resources could be distributed efficiently, allowing more clinically and cost-effective patient care. Risk factors associated with ARMD development include female gender, small femoral component size and acetabular component malposition [8, 16–19]. However, these risk factors were identified in predominantly hip resurfacing populations and therefore may not necessarily apply in MoM THR patients due to the additional taper and modular junctions [20, 21]. Indeed, few studies have analysed factors affecting blood metal ion concentrations in modern MoM THRs, with the findings from those studies being less conclusive compared with reports in hip resurfacings [22–25].
This study aimed to determine which patient, surgeon and implant factors affect blood metal ion concentrations following modern MoM THR. It was expected this would identify which patient subgroup(s) are at greatest risk of developing ARMD, which will have implications for rationalising future clinical follow-up.
Patients and methods
Study design and patient demographics
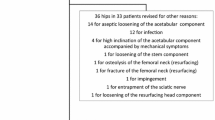
This prospective cohort study was undertaken at one specialist arthroplasty centre and was approved and registered with the institutional review board. All patients undergoing primary MoM THR implanted at this centre since January 2001 with blood metal ion concentrations measured up to May 2013 were eligible for inclusion (805 MoM THRs in 717 patients). As renal impairment is an established contraindication for MoM hip arthroplasty, all patients considered suitable for MoM THR at this centre had normal renal function confirmed prior to bearing implantation. Patients with bilateral hip replacements, regardless of bearing type, were excluded from this analysis due to difficulties associated with interpreting raised blood metal ions in the presence of two hip bearings [26]. After other exclusions (Fig. 1), 496 MoM THRs in 496 patients were included in the final cohort, with a mean follow-up of 4.5 years (range 1.1–11.8 years) since the index arthroplasty (Table 1).

Study inclusion criteria for metal-on-metal total hip replacements
Operations were performed by 13 surgeons, with two surgeons performing half of the cases (n = 251; 50.1 %). Each operation was performed in a clean-air laminar flow operating theatre using a posterior (n = 386) or an anterolateral (n = 110) surgical approach. Five different MoM THR designs were used according to surgeon preference (Table 1). All components were uncemented, with each implanted as for a routine THR but in line with the manufacturer’s instructions.
Description of follow-up routine
All patients were invited for clinical review at six weeks, six months and one year postoperatively, with invitations for annual clinical review thereafter. Each consultation included clinical examination, anteroposterior pelvic radiographs and completion of the Oxford Hip Score (OHS) questionnaire [27]. Blood metal ion sampling was not performed in patients reviewed prior to 2010. After the 2010 MHRA alert highlighting concerns with MoM hips [10], this institution contacted all MoM THR patients by post to explain the situation at the time (“Electronic Supplementary Material”). All patients, regardless of symptoms, were offered an appointment for clinical review and blood metal ion sampling.
Blood metal ion sampling
Whole blood was collected from patients and transported to a laboratory approved by the MHRA for blood metal ion analysis (City Hospital, Birmingham, UK). Cobalt (Co) and chromium (Cr) concentrations were measured in all samples using an inductively coupled plasma mass spectrometer (Agilent 7500cx, Agilent Technologies Inc., Santa Clara, CA, USA). Detection and reporting limits were 0.06 μg/l and 0.6 μg/l, respectively. Blood metal ions were considered raised if Co and/or Cr concentrations were greater than the MHRA upper limit of 7 μg/l [11].
Description of outcome measures
All study data except for acetabular inclination angle were extracted from the institution’s prospectively maintained database (MySQL database, Oracle Corporation, Redwood Shores, CA, USA). Acetabular component inclination was measured in each anteroposterior pelvic radiograph using the teardrop line for reference, as previously described [28]. Two authors (GSM and DJD) each measured acetabular inclination in half of the cohort after interobserver and intraobserver reliability had been evaluated on a random sample of 30 radiographs (intra-observer and interobserver 95 % limits of agreement were −2.2° to 1.6° and −2.5° to 3.5°, respectively, and 95 % confidence intervals (CI) for intraclass coefficients were 0.994–0.998 and 0.984–0.994, respectively [29, 30]).
The OHS was used to assess postoperative pain and disability following MoM THR [27]. At this institution, the OHS is expressed as a percentage (0 % = healthy joint and 100 % = worst possible joint) [31]. However, as the OHS is frequently scored on a scale of 0–48 points (0 = worst possible joint and 48 = healthy joint) [32], these scores have also been provided for comparison with previous reports.
Statistical analysis
Data were extracted from the outcomes database and analysed using the R statistical programming language [33]. Summary statistics were calculated for all variables. Linear regression and t tests were performed to investigate relationships between the base 10 logarithm of blood metal ion concentrations and the different patient, surgeon and implant covariates. Similar to previous studies [25, 34, 35], the logarithm was necessary to transform the asymmetric blood metal ion concentration distributions so that the residuals in the regression models were more normally distributed. Adjusted R 2 was also calculated to give the percentage of variance in the logarithm blood metal ion concentrations explained by the models.
Not all 496 patients submitted an OHS at the time of blood sampling. Therefore, all covariates apart from OHS were analysed in the cohort of 496 patients, whilst the OHS analysis was only performed in the 298 patients providing eligible questionnaires (Table 1). For completeness, all covariates analysed in the full cohort were also assessed in the subgroup of 298 patients.
Femoral head sizes were grouped into small (28/36 mm, n = 300) and large (38–58 mm, n = 196) for t testing with multiple comparisons. Similarly, acetabular inclination angles were grouped (<30° (n = 16), 30°−50° (n = 412), >50° (n = 68)) using the previously described safe inclination zone for THR [36]. The five different MoM THR implant designs were grouped as follows: Corail–Pinnacle (n = 300), Synergy (n = 150), and Other (Caparo Amoda, Conserve and Adept; n = 46). The Holm method was used for adjusting the p values in this t testing to allow for multiple comparisons. A p value <0.05 was considered statistically significant.
Results
Blood metal ions >7 μg/l for either Co or Cr were observed in 9.7 % (n = 48). The large femoral head-size group had significantly higher blood metal ion concentrations than the small head-size group (Table 2, Fig. 2). Blood metal ion concentrations >7 μg/l were observed in 4.3 % (13/300) of small-head MoM THRs compared with 17.9 % (35/196) of large-head THRs. The small head-size group all had Corail–Pinnacle implants, so further analysis was performed by implant design. Patients with Corail–Pinnacle implants had significantly lower log blood metal ion concentrations compared with both the Synergy and Other groups, but there were no significant differences between the Synergy and Other implant groups (Table 2, Fig. 3). No other variables significantly affected both blood Co and Cr concentrations (Table 2).

Log10 blood a cobalt and b chromium concentrations for small (28 mm and 36 mm) and large (38–58 mm) femoral head sizes following metal-on-metal total hip replacement. The Medical and Healthcare Products Regulatory Agency (MHRA) upper limit of 7 μg/l is indicated by the dashed red horizontal line. Box widths are proportional to the number of hips in the group; notch size is an indication of the 95 % confidence interval around the median of the distribution

Log10 blood a cobalt and b chromium concentrations for different implant designs following metal-on-metal total hip replacement. The Medical and Healthcare Products Regulatory Agency (MHRA) upper limit of 7 μg/l is indicated by the dashed red horizontal line. Box widths are proportional to the number of hips in the group; notch size is an indication of the 95 % confidence interval around the median of the distribution
Univariate linear regression analysis demonstrated that most variables, including the OHS (Fig. 4), had no significant effects on log Co or Cr (Table 3). Femoral head size (Fig. 5) and implant design were the only factors significantly affecting both log blood Co and Cr concentrations. When linear regression analysis was repeated separately for the three implant design groups (Corail–Pinnacle, Synergy, Other), femoral head size did not significantly affect log blood metal ion concentrations.

Log10 whole blood cobalt concentration modelled on Oxford Hip Score with regression line (solid), 95 % confidence limits (dotted) and 95 % prediction limits (dashed). Medical and Healthcare Products Regulatory Agency (MHRA) upper limit of 7 μg/l is indicated by the dot–dashed horizontal line. Hips from women are indicated by + and from men by o. Similar results were obtained for log10 blood chromium concentrations (adjusted R 2 < 1 %, p value = 0.442, y = 0.0007x + 0.075)

Log10 whole blood cobalt concentration modelled on femoral head size with regression line (solid), 95 % confidence limits (dotted) and 95 % prediction limits (dashed). Medical and Healthcare Products Regulatory Agency (MHRA) upper limit of 7 μg/l is indicated by the dot–dashed horizontal line. Hips from women are indicated by + and from men by o. Similar results were obtained for log10 blood chromium concentrations (adjusted R 2 = 3.3 %, p value < 0.0001, y = 0.010x−0.302)
Multivariate linear regression modeling demonstrated the best fitting model was one combining femoral head size, gender and time since index arthroplasty (R 2 13.6 % for log Co and 7.5 % for log Cr). When this modeling was repeated separately for the three implant design groups, the only significant covariates were gender and time since index arthroplasty in an additive model for Co in the Corail–Pinnacle group (R 2 = 8.3 %) and for Cr in the Synergy group (R 2 = 9.2 %). When repeating all statistical analysis in patients with eligible postoperative OHSs (n = 298), although there were some minor differences in t test results and R 2 values, the conclusions reached were the same as those for the entire cohort (n = 496).
Of the 48 patients with blood metal ions >7 μg/l, there have been 15 revisions (13 ARMD; one infection; one periprosthetic stem fracture). The remaining 33 patients with high blood metal ions remain under regular clinical surveillance. Sixteen further MoM THRs were revised (13 ARMD, and one each for unexplained pain, acetabular loosening and femoral loosening) where blood metal ion levels were ≤7 μg/l. Mean time from index MoM THR to revision in these 31 cases was 4.5 years (range 1.6−12.2 years).
Discussion
Most risk factors for developing ARMD have been identified in hip resurfacing populations [8, 16–19]. These factors have frequently and possibly incorrectly been assumed to apply in modern MoM THR patients, given that few studies have formally analysed factors affecting blood metal ion concentrations in MoM THR patients [22–25]. Such studies are limited by short-term follow-up as well as the inclusion of hip resurfacing patients and those with bilateral MoM hip bearings. Our study provides a comprehensive analysis of the affect of patient, surgeon and implant factors on blood metal ion concentrations using the largest cohort of modern MoM THRs with the longest follow-up reported to date.
The main findings were that although larger femoral head sizes appear to be associated with higher blood metal ion concentrations, this was no longer the case when implant design was controlled for. In addition, there were significant differences in blood metal ion concentrations between implant designs, with Corail–Pinnacle THRs having lower levels compared with other implants. This remained the case when individual surgeon was controlled for (Table 2). Therefore, implant design was the most important factor affecting blood metal ion concentrations in MoM THR patients.
The serious concerns raised regarding high failure rates of all modern MoM THR devices [2, 6–8, 11] suggest there is a universal design problem. However, registry-reported revision rates of various MoM THR designs range from 11.1 % to 43.3 % at eight years [37]. Our findings support these observations, with evidence suggesting the risk of wear-related problems differs between implant designs. A smaller study of 144 MoM THRs with four different implant designs also demonstrated significant differences in blood Co between designs [23].
As well as the bearing surface, MoM THRs have a taper junction with or without modular junctions, which are subject to wear debris and/or corrosion [38, 39]. It has been observed that taper wear produces Co in preference to Cr [20]. Our findings suggest the taper is the main source of metal ions generated, given that blood Co concentrations were nearly twice that of Cr (Table 1). The number and nature of taper and modular junctions vary between implants, which may be responsible for differences observed in blood metal ions between MoM THR designs and the risk of failure. It is clear by comparing hip resurfacing patients with stemmed MoM THRs with identical bearing designs that adding a taper junction increases blood metal ions [7, 40, 41]. In addition, different MoM THR designs from the same manufacturer have been observed to have significantly different volumetric and linear wear rates [39].
This study provides evidence that variations in implant design can affect blood metal ion concentrations. Excluding the bearing surface and the interface between the cup and liner, the Corail–Pinnacle has one modular junction (taper–head). By contrast, implants with significantly higher blood metal ion concentrations had additional design features. The later Synergy device has an adapter sleeve applied to the stem taper, whilst the Caparo Amoda THR has a modular junction between the stem and neck. Furthermore, cobalt concentration was significantly higher (p=0.008) in Synergy devices with an adapter sleeve (n=98; 65%) compared with the pre-2006 sleeveless femoral-component design (n=52; 35%). Similar metal ion levels were observed in the sleeveless Synergy design and Corail-Pinnacle THRs (p=0.187). Similar to previous authors [39], we were unable to obtain more detailed information on implant metallurgy and design from the manufacturers, given this is sensitive data and these implants are no longer used. However, we suspect variations in taper design, tolerance, and metallurgy between THR designs play an important role in metal ion generation.
Although registry data suggests larger MoM femoral head sizes have higher failure rates, this has not yet been stratified according to implant design [2, 37]. Similar to our findings, other studies have not demonstrated significant relationships between femoral head size and blood metal ions when analysing single MoM THR brands [7, 22, 24]. Furthermore, a retrieval analysis observed increasing femoral head size was only weakly associated with MoM THR taper wear rates [39]. It would therefore be interesting to use registry data to determine whether large femoral head size remains a risk factor for failure when implant design is controlled for.
Despite female gender and acetabular component malposition being risk factors for raised blood metal ions and hip resurfacing failure [8, 16–19], these factors did not affect blood metal ions in MoM THRs in this cohort. Previous studies have almost universally demonstrated that gender and acetabular component position do not significantly affect blood metal ions following MoM THR [23–25, 42]. In one study assessing 213 ASR XL MoM THRs, the authors concluded that acetabular inclination was not a meaningful determinant of blood metal ions and that the high failure rates were design related [25]. By assessing large numbers of different THR designs, our findings provide further evidence that implant design, and not modifiable factors, is the major factor affecting blood metal ion levels. It is suspected that risk factors associated with hip resurfacing are not apparent in THRs given that wear predominantly arises from taper and modular junctions; therefore, failure may be inevitable regardless of patient selection and surgical technique.
Symptoms assessed using the OHS did not reflect blood metal ion concentrations. This supports previous findings of ARMD in asymptomatic patients [43, 44] and the MHRA recommendations that follow-up of large-head MoM THRs is irrespective of symptoms [11]. Symptoms alone should therefore not be used to decide on blood sampling.
This study has some recognised limitations. Factors such as acetabular anteversion and combined anteversion, which may affect blood metal ion concentrations, were not assessed, as they could not be measured accurately using the available software. Furthermore, some patients may develop ARMD with normal blood metal ions [45, 46] and therefore would not be identified in our analysis. Renal function was not assessed at metal ion sampling; however, all patients had normal renal function prior to MoM THR.
Conclusions
Implant design was the most important factor affecting blood metal ion concentrations following MoM THR. Follow-up regularity should therefore be tailored according to registry survival rates of the various THR designs rather than according to femoral head size [11]. This should allow more effective distribution of clinical resources, with implants known to have higher failure rates reviewed more frequently.
References
Bozic KJ, Kurtz S, Lau E, Ong K, Chiu V, Vail TP et al (2009) The epidemiology of bearing surface usage in total hip arthroplasty in the United States. J Bone Joint Surg (Am) 91-A:1614–1620
Smith AJ, Dieppe P, Vernon K, Porter M, Blom AW (2012) Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. Lancet 379:1199–1204
Zijlstra WP, van den Akker-Scheek I, Zee MJ, van Raay JJ (2011) No clinical difference between large metal-on-metal total hip arthroplasty and 28-mm-head total hip arthroplasty? Int Orthop 35:1771–1776
Fink Barnes LA, Johnson SH, Patrick DA Jr, Macaulay W (2014) Metal-on-metal hip resurfacing compared with total hip arthroplasty: two to five year outcomes in men younger than sixty five years. Int Orthop 38:2435–2440
Cohen D (2012) How safe are metal-on-metal hip implants? BMJ 344:e1410
Bolland BJ, Culliford DJ, Langton DJ, Millington JP, Arden NK, Latham JM (2011) High failure rates with a large-diameter hybrid metal-on-metal total hip replacement: clinical, radiological and retrieval analysis. J Bone Joint Surg (Br) 93-B:608–615
Langton DJ, Jameson SS, Joyce TJ, Gandhi JN, Sidaginamale R, Mereddy P et al (2011) Accelerating failure rate of the ASR total hip replacement. J Bone Joint Surg (Br) 93-B:1011–1016
Langton DJ, Jameson SS, Joyce TJ, Hallab NJ, Natu S, Nargol AV (2010) Early failure of metal-on-metal bearings in hip resurfacing and larger-diameter total hip replacement: a consequence of excess wear. J Bone Joint Surg (Br) 92-B:38–46
Smith AJ, Dieppe P, Howard PW, Blom AW, National Joint Registry for England and Wales (2012) Failure rates of metal-on-metal hip resurfacings: analysis of data from the National Joint Registry for England and Wales. Lancet 380:1759–1766
Medical and Healthcare Products Regulatory Agency (MHRA) (2010) Medical device alert: ASR™ hip replacement implant manufactured by DePuy International Ltd. MDA/2010/069. http://www.mhra.gov.uk/. Accessed 19 Nov 2014
Medical and Healthcare products Regulatory Agency (MHRA) (2012) Medical device alert: all metal-on-metal (MoM) hip replacements. MDA/2012/036. http://www.mhra.gov.uk/. Accessed 19 Nov 2014
Sidaginamale RP, Joyce TJ, Lord JK, Jefferson R, Blain PG, Nargol AV et al (2013) Blood metal ion testing is an effective screening tool to identify poorly performing metal-on-metal bearing surfaces. Bone Joint Res 2:84–95
Almousa SA, Greidanus NV, Masri BA, Duncan CP, Garbuz DS (2013) The natural history of inflammatory pseudotumors in asymptomatic patients after metal-on-metal hip arthroplasty. Clin Orthop Relat Res 471:3814–3821
Ebreo D, Bell PJ, Arshad H, Donell ST, Toms A, Nolan JF (2013) Serial magnetic resonance imaging of metal-on-metal total hip replacements. Follow-up of a cohort of 28 mm Ultima TPS THRs. Bone Joint J 95:1035–1039
Bernstein M, Desy NM, Petit A, Zukor DJ, Huk OL, Antoniou J (2012) Long-term follow-up and metal ion trend of patients with metal-on-metal total hip arthroplasty. Int Orthop 36:1807–1812
De Haan R, Pattyn C, Gill HS, Murray DW, Campbell PA, De Smet K (2008) Correlation between inclination of the acetabular component and metal ion levels in metal-on-metal hip resurfacing replacement. J Bone Joint Surg (Br) 90-B:1291–1297
Glyn-Jones S, Pandit H, Kwon YM, Doll H, Gill HS, Murray DW (2009) Risk factors for inflammatory pseudotumour formation following hip resurfacing. J Bone Joint Surg (Br) 91-B:1566–1574
Grammatopoulos G, Pandit H, Glyn-Jones S, McLardy-Smith P, Gundle R, Whitwell D et al (2010) Optimal acetabular orientation for hip resurfacing. J Bone Joint Surg (Br) 92-B:1072–1078
Langton DJ, Joyce TJ, Jameson SS, Lord J, Van Orsouw M, Holland JP et al (2011) Adverse reaction to metal debris following hip resurfacing: the influence of component type, orientation and volumetric wear. J Bone Joint Surg (Br) 93-B:164–171
Langton D (2014) Are metal ion levels a trigger for surgical intervention? In: Jones LC, Greenwald AS, Haggard WO (eds) Metal-on-metal bearings. A clinical practicum. Springer, New York, pp 63–82, Chapter 5
Reito A, Moilanen T, Puolakka T, Pajamäki J, Eskelinen A (2014) Repeated metal ion measurements in patients with high risk metal-on-metal hip replacement. Int Orthop 38:1353–1361
Bernstein M, Walsh A, Petit A, Zukor DJ, Huk OL, Antoniou J (2011) Femoral head size does not affect ion values in metal-on-metal total hips. Clin Orthop Relat Res 469:1642–1650
Lavigne M, Belzile EL, Roy A, Morin F, Amzica T, Vendittoli PA (2011) Comparison of whole-blood metal ion levels in four types of metal-on-metal large-diameter femoral head total hip arthroplasty: the potential influence of the adapter sleeve. J Bone Joint Surg (Am) 93-A(Supp 2):128–136
Chang EY, McAnally JL, Van Horne JR, Van Horne JG, Wolfson T, Gamst A et al (2013) Relationship of plasma metal ions and clinical and imaging findings in patients with ASR XL metal-on-metal total hip replacements. J Bone Joint Surg (Am) 95-A:2015–2020
Emmanuel AR, Bergin KM, Kelly GE, McCoy GF, Wozniak AP, Quinlan JF (2014) The effect of acetabular inclination on metal ion levels following metal-on-metal hip arthroplasty. J Arthroplasty 29:186–191
Van Der Straeten C, Grammatopoulos G, Gill HS, Calistri A, Campbell P, De Smet KA (2013) The 2012 Otto Aufranc Award: the interpretation of metal ion levels in unilateral and bilateral hip resurfacing. Clin Orthop Relat Res 471:377–385
Dawson J, Fitzpatrick R, Carr A, Murray D (1996) Questionnaire on the perceptions of patients about total hip replacement. J Bone Joint Surg (Br) 78-B:185–190
Pandit H, Glyn-Jones S, McLardy-Smith P, Gundle R, Whitwell D, Gibbons CL et al (2008) Pseudotumours associated with metal-on-metal hip resurfacings. J Bone Joint Surg (Br) 90-B:847–851
Shrout PE, Fleiss JL (1979) Intraclass correlations: uses in assessing rater reliability. Psychol Bull 86:420–428
Bland JM, Altman DG (1999) Measuring agreement in method comparison studies. Stat Methods Med Res 8:135–160
Pynsent PB, Adams DJ, Disney SP (2005) The Oxford hip and knee outcome questionnaires for arthroplasty. J Bone Joint Surg (Br) 87-B:241–248
Murray DW, Fitzpatrick R, Rogers K, Pandit H, Beard DJ, Carr AJ et al (2007) The use of the Oxford hip and knee scores. J Bone Joint Surg (Br) 89-B:1010–1014
R Core Team (2013) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna
Davda K, Lali FV, Sampson B, Skinner JA, Hart AJ (2011) An analysis of metal ion levels in the joint fluid of symptomatic patients with metal-on-metal hip replacements. J Bone Joint Surg (Br) 93-B:738–745
Matthies AK, Henckel J, Cro S, Suarez A, Noble PC, Skinner J et al (2014) Predicting wear and blood metal ion levels in metal-on-metal hip resurfacing. J Orthop Res 32:167–174
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR (1978) Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg (Am) 60-A:217–220
National Joint Registry for England and Wales. 10th Annual Report 2013. http://njrcentre.org.uk. Accessed 19 Nov 2014
Cooper HJ, Della Valle CJ, Berger RA, Tetreault M, Paprosky WG, Sporer SM et al (2012) Corrosion at the head-neck taper as a cause for adverse local tissue reactions after total hip arthroplasty. J Bone Joint Surg (Am) 94-A:1655–1661
Langton DJ, Sidaginamale R, Lord JK, Nargol AV, Joyce TJ (2012) Taper junction failure in large-diameter metal-on-metal bearings. Bone Joint Res 1:56–63
Garbuz DS, Tanzer M, Greidanus NV, Masri BA, Duncan CP (2010) The John Charnley Award: metal-on-metal hip resurfacing versus large-diameter head metal-on-metal total hip arthroplasty: a randomized clinical trial. Clin Orthop Relat Res 468:318–325
Beaulé PE, Kim PR, Hamdi A, Fazekas A (2011) A prospective metal ion study of large-head metal-on-metal bearing: a matched-pair analysis of hip resurfacing versus total hip replacement. Orthop Clin N Am 42:251–257
Brodner W, Grübl A, Jankovsky R, Meisinger V, Lehr S, Gottsauner-Wolf F (2004) Cup inclination and serum concentration of cobalt and chromium after metal-on-metal total hip arthroplasty. J Arthroplasty 19:66–70
Fehring TK, Odum S, Sproul R, Weathersbee J (2014) High frequency of adverse local tissue reactions in asymptomatic patients with metal-on-metal THA. Clin Orthop Relat Res 472:517–522
Hart AJ, Satchithananda K, Liddle AD, Sabah SA, McRobbie D, Henckel J et al (2012) Pseudotumors in association with well-functioning metal-on-metal hip prostheses: a case–control study using three-dimensional computed tomography and magnetic resonance imaging. J Bone Joint Surg (Am) 94-A:317–325
Malek IA, King A, Sharma H, Malek S, Lyons K, Jones S et al (2012) The sensitivity, specificity and predictive values of raised plasma metal ion levels in the diagnosis of adverse reaction to metal debris in symptomatic patients with a metal-on-metal arthroplasty of the hip. J Bone Joint Surg (Br) 94-B:1045–1050
Matthies AK, Skinner JA, Osmani H, Henckel J, Hart AJ (2012) Pseudotumors are common in well-positioned low-wearing metal-on-metal hips. Clin Orthop Relat Res 470:1895–1906
Acknowledgments
The authors thank the Royal College of Surgeons of England and the Arthritis Research Trust for providing one of the authors with funding in the form of a Surgical Research Fellowship.
Conflict of interest
The author or one or more of the authors have received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article. In addition, benefits have been or will be directed to a research fund, foundation, educational institution or other nonprofit organisation with which one or more of the authors are associated.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 39 kb)
Rights and permissions
About this article

Cite this article
Matharu, G.S., Berryman, F., Brash, L. et al. Influence of implant design on blood metal ion concentrations in metal-on-metal total hip replacement patients. International Orthopaedics (SICOT) 39, 1803–1811 (2015). https://doi.org/10.1007/s00264-014-2644-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-014-2644-z