
Abstract
Purpose
Highly cross-linked polyethylenes (PE) have been developed with encouraging results in terms of wear. Another body of the literature has indicated potential catastrophic failures related to reduced fatigue properties and oxidation. Each PE available on the market has its own processing characteristics. The aim of this retrospective study was to evaluate the minimum five-year wear properties of an original highly cross-linked PE in a consecutive series of primary THAs.
Methods
Between August 2005 and December 2007, 80 patients with a mean age of 62.7 years were included. All patients had a 28-mm CoCr femoral head articulating with a highly cross-linked insert (Highcross®, Medacta SA) that was 100 Mrads gamma radiated, remelted at 150 °C, and ethylene oxide sterilized. The primary criterion for evaluation was the femoral head penetration, as measured by Hip Analysis Suite software. The steady state wear was also calculated. Functional results were evaluated according to the WOMAC score.
Results
Complete data were available for analysis in 67 patients at a mean follow-up of 5.5 years. The mean femoral head penetration was 0.128 ± 0.62 mm and the steady state wear was−0.025 ± 0.22 mm/year. The WOMAC score significantly decreased from 16.5 ± 5.93 pre-operatively to 4.12 ± 5.5 at the latest follow-up (p <0.001).
Conclusions
The minimal five-year results of this retrospective study indicate that this particular highly cross-linked and remelted polyethylene had a low wear rate. Longer-term results are needed to warrant that these mid-term data will generate less osteolysis and resultant aseptic loosening.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Metal-on-polyethylene bearing couple remains the gold standard in total hip arthroplasty (THA). The main reason for revision and failure using these bearings is related to high polyethylene (PE) wear and periprosthetic osteolysis, leading to implant loosening [1]. Therefore, it seems clear that efforts should be made to increase the wear resistance of ultra-high molecular weight PE. One method of research is the use of highly cross-linked material. Current methods of cross-linking include gamma- or electron-beam radiation at doses between 5 and 10.5 Mrads, followed by a post-radiation thermal treatment to reduce (annealing) or extinguish (remelting) the free radicals in the material [2]. After a decade of clinical use, the reported results with first generation highly cross-linked material have been consistent showing reduced wear rates [3, 4]. However, the potentially reduced mechanical properties of highly cross-linked PE remain a subject of concern. In addition, recent publications have indicated that these first generation highly cross-linked materials could oxidized through lipids absorption and fatigue mechanisms [5]. In fact, each PE candidate to total joint arthroplasty has its own processing characteristics. Pre-clinical results may differ from in vivo measurements. Therefore, each of these materials should be specifically evaluated in order to assess their in vivo behaviour.
The aim of this study was to evaluate the minimum five-year follow-up clinical and radiological performance of an original highly cross-linked PE insert in a consecutive series of cementless primary THAs.
Materials and methods
Study design
Between June 2005 and December 2007, 80 consecutive patients (80 hips) with primary (65 %) or secondary osteoarthritis (35 %) of the hip requiring total hip arthroplasty were included in the study. There were 39 females and 41 males with a mean age of 62.7 ± 8.9 years (range, 22–83 years), a mean height of 168.6 cm (range, 157–186 cm), a mean weight of 79.7 kg (range, 60–150 kg), and a mean body mass index of 27.3 kg/m² (range, 22.5–46.8 kg/m²). They all had given informed consent.
Implants
All patients had a Highcross® (Medacta SA, Castel San Pietro, Switzerland) insert made from compression-moulded GUR 1020 ultra-high molecular weight polyethylene bars gamma irradiated to an absorbed dose level of 10 Mrads. After cross-linking, the material was heated to a temperature above the material’s crystalline melting point until complete melting was achieved (150 °C), and then controlled cooling to room temperature. The material was sterilised using ethylene oxide gas (EtO). The cementless acetabular component (Versafitcup CC®) was made of titanium and coated with hydroxy-apatite (Medacta). All patients received Quadra-H® cementless stems (Medacta SA,) made of titanium-niobium alloy coated with hydroxy-apatite, and a 28-mm diameter femoral head made of cobalt-chromium (CoCr).
Surgical technique
Three senior surgeons carried out all the procedures through an anterior mini-invasive approach using a leg positioner (AMIS®, Medacta). The shell was impacted into an iso-reamed acetabulum (interference-fit). Additional fixation with screws was not required to achieve primary stability.
Postoperative treatment
The postoperative management included the administration of systemic antibiotics for 24 hours, and preventive anticoagulation therapy (enoxaparin; 40 mg/day) for five weeks. The patients were free to walk under the supervision of a physiotherapist with two crutches the day after surgery. Full weight bearing was allowed immediately as tolerated.
Methods of evaluation
Radiological evaluation
The primary criterion for evaluation was linear head penetration measurement, as an assessment of true wear and creep of the material, using the Hip Analysis Suite software (version 8.0.1.5, UCTech, University of Chicago) [6]. All measurements were done on anteroposterior radiographs of the pelvis, made with the X-ray beam centred on the symphysis pubis. Radiographs were made with the patient supine within three months after the operation (baseline radiograph), at one year, and at the latest follow-up. The radiographs were digitized (digitizer Vidar VRX-plus, Vidar System Corporation, Herdon, Virginia) using a pixel density of 150 dots per inch and linked to an IBM-compatible computer. The Martell Hip Analysis Suite (version 8.0.1.5, UCTech, University of Chicago) is a validated computer-assisted edge detection method. Only a two-dimensional penetration analysis was performed in the present study, although it has a lower accuracy and detects 10 % less penetration than the three-dimensional technique, but has a four times higher precision [7]. This software allows measurement of the linear vector of socket penetration, based on the magnitude of femoral head displacement, the direction of displacement with respect to the cup face, and the femoral head size. Its accuracy has been published to be 0.033 mm [8]. Moreover, this updated version of the Martell system allows for comparability of the radiographs analysed, excluding pairs with more than 25° in rotational difference of the pelvis. In addition, excluding the first year of femoral head penetration (mainly bedding-in and creep deformation of the PE insert), we properly assessed the steady state wear rate by calculating a regression line from the penetration-over-time data (between the first year and the latest follow-up). Values of socket abduction were calculated with use of the Hip Analysis Suite. The same independent observer trained to the technique performed all radiological analyses. His repeatability for femoral head penetration measurement was assessed from 20 preliminary double examinations performed in a random order, and calculated to be 0.073 mm (standard deviation, or sr) and 0.143 mm (95 % confidence limits, or r) based on the latest ATSM recommendations.
Clinical evaluation
Clinical results were evaluated according to the three components of the WOMAC score, including physical function, stiffness and pain. The operating surgeon performed the clinical follow-up.
Statistical analysis
Wilcoxon’s non-parametric matched pairs tests were used to evaluate the difference between the pre and postoperative clinical data. Significance was determined with StatView statistical software (version 5.0; SAS Institute, Cary, North Carolina) and was defined as a p value of < 0.05.
Results
Of the 80 patients included in the study, 67 (85 %) completed the clinical and radiological evaluation at a minimum of five-year follow-up, with a mean follow-up of 5.5 ± 0.6 years (range, 4.1–6.8 years). The mean acetabular component inclination was 46.7° ±7.1° (range, 30.1–65.3°).
Complications
One acute (one month after surgery) infection was treated by open large debridement and PE liner exchange. One patient had a grade III heterotopic ossification. No other patient required revision surgery at the time of the last follow-up. No case of insert fracture was recorded.
Wear results
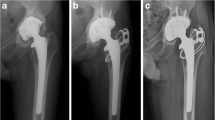
At the latest follow-up, the mean femoral head penetration was measured to be 0.128 ± 0.62 mm (range, −0.28 to 0.56 mm) (Fig. 1). The mean penetration rate was therefore 0.025 ± 0.124 mm/year. The steady state wear rate was –0.025 ± 0.22 (median of 0.01, range −0.8 to 0.3 mm). There were no cases of radiolucent lines and no hip had signs of osteolysis on either the acetabular or the femoral side (Fig. 2).

Femoral head penetration over time

Antero-posterior X-rays at three months (a) and at last follow up (b). No signs of osteolysis are seen
Clinical results
The mean global WOMAC score significantly decreased from 16.5 ± 5.93 pre-operatively to 4.12 ± 5.5 at the latest follow-up (Mann–Whitney, p < 0.001). The results of each component of the WOMAC were also significantly decreased at last follow-up (Table 1).
Discussion
At a minimum of five-year follow-up, the mean femoral head penetration measured using Highcross® first generation of highly cross linked polyethylene liner was 0.128 ± 0.62 mm, and the steady state wear from the first to the fifth year was as low as –0.025 ± 0.22 mm/year.
We acknowledge some limitations to our study, including the fact that we built a retrospective non-comparative study. We did not have a control group to analyse with the same observer a significant reduction of polyethylene wear with this first generation of highly cross-linked polyethylene compared to conventional polyethylene. Also, only one femoral head size (28 mm) and one type of femoral head (CrCo) were analysed in this study. While few authors have demonstrated wear rate differences between ceramic and metal femoral head against conventional polyethylene [9], it has not been evaluated yet against highly cross-linked polyethylene. Besides, since increasing femoral head size is known to increase volumetric polyethylene wear rate, our 28-mm femoral diameter size constituted experimental favourable conditions to lower the steady-state wear rate [10].
No accurate osteolysis evaluation has been performed in the present study at the latest follow-up. But given the relatively short (five years) follow-up and the satisfactory radiologic findings, in association with the low wear rates anticipated and confirmed, far below the osteolysis threshold defined by Dumbleton et al. (0.1 mm/year), no CT scan evaluation could have been ethically indicated [11]. The influence of several patient-related factors on polyethylene penetration, including the age of the patient at the time of arthroplasty, activity, gender, and BMI was not assessed either.
The two-dimensional Martell technique measuring femoral head penetration based on the sole use of anteroposterior pelvis view has been reported to have an accuracy averaging 0.025 mm [6]. These figures are inferior to the results obtained by the same authors when assessing the precision and accuracy of radiostereometric analysis (RSA) under similar conditions [12]. But our study was retrospective and RSA was not available when our study was started. Another limitation of the Martell method was the negative wear values. However, when measuring very low wear rates (<1 mm), Ranawat et al. demonstrated that up to 50 % of the liners could show negative values [13]. We chose to report the average penetration of both positive and negative values following experienced researchers [14]. The use of supine position anteroposterior pelvis views was also recognized by some authors as an imprecision risk for the measure, but remains controversial for others [15, 16].
First generation highly cross-linked polyethylene was introduced during the past decade, and results from well-designed controlled studies with up to 12-year follow up are now available in the literature. All study of remelted highly cross-linked polyethylene (Table 2) show significantly reduced wear rates when compared to conventional polyethylene. Our results of steady state wear were consistent with the literature. In fact Triclot et al., Digas et al., Garcia Rey et al. and Dorr et al.[17–20] at five years of follow-up found a steady state wear between 0.006 and 0.03 mm/year for Durasul® (Zimmer, Warsaw, IN) polyethylene that is remelted and ethylene oxide sterilized highly cross linked polyethylene. Our mean result of steady state wear was lower but our median value is comparable. Our results could be explained by the penetration measuring technique, using consequently a distinct baseline radiograph, or by the different type of PE irradiation, type of metal-back cup, or different size of femoral head. However, our cumulative femoral head penetration (0.128 mm) was measured in a similar range of order as compared with Dorr et al. (0.150) who also used a 28-mm femoral head.
Data from retrievals have indicated that these first generation remelted materials could oxidize, and also be associated with specific complications such as fracture of acetabular inserts [23]. Some studies have demonstrated that high dose of radiation can reduce the resistance to crack propagation [24]. Moreover the post irradiation thermal treatment that aims at extinguishing (remelted, >150°) the free radicals of the material could also lead to reduce mechanical properties of the material. In regards to decrease of highly cross-linked polyethylene mechanical properties, no insert cracking was described in the present series. However, isolated cases of fatigue cracks described in literature were matched with low insert thickness and incorrect positioning of acetabular cup [25]. Using a 28-mm femoral head with a minimum thickness of the polyethylene socket of 6 mm and a mean of 46° inclination of our acetabular cup probably helped us to avoid any mechanical failures of the polyethylene.
In summary, this study supports the use of this first highly cross-linked type of polyethylene, with a low oxidation risk and a wear rate comparable with other first generation highly cross-linked materials. It is of absolute importance to continue to monitor this series, evaluating in addition to its long-term wear rate, potential complications of this first generation of highly cross-linked polyethylene including osteolysis, oxidation and fracture of acetabular inserts.
References
Caton J, Prudhon JL (2011) Over 25 years survival after Charnley's total hip arthroplasty. Int Orthop 35:185–188
Harris WH, Muratoglu OK (2005) A review of current cross-linked polyethylenes used in total joint arthroplasty. Clin Orthop Relat Res 430:46–52
Mu Z, Tian J, Wu T, Yang J, Pei F (2009) A systematic review of radiological outcomes of highly cross-linked polyethylene versus conventional polyethylene in total hip arthroplasty. Int Orthop 33:599–604
Kuzyk PRT, Saccone M, Sprague S, Simunovic N, Bhandari M, Schemitsch EH (2011) Cross-linked versus conventional polyethylene for total hip replacement: a meta-analysis of randomised controlled trials. J Bone Joint Surg Br 93(5):593–600
Wannomae KK, Bhattacharyya S, Freiberg A, Estok D, Harris WH, Muratoglu O (2006) In vivo oxidation of retrieved cross-linked ultra–high-molecular-weight polyethylene acetabular components with residual free radicals. J Arthroplast 21:1005–1011
Martell J, Berdia S (1997) Determination of polyethylene wear in total hip replacements with use of digital radiographs. J Bone Joint Surg Am 79(11):1635–1641
Martell JM, Berkson E, Berger R, Jacobs J (2003) Comparison of two and three-dimensional computerized polyethylene wear analysis after total hip arthroplasty. J Bone Joint Surg Am 85-A(6):1111–1117
McCalden RW, Naudie DD, Yuan X, Bourne RB (2005) Radiographic methods for the assessment of polyethylene wear after total hip arthroplasty. J Bone Joint Surg Am 87:2323–2334
Meftah M, Klingenstein GG, Yun RJ, Ranawat AS, Ranawat CS (2013) Long-term performance of ceramic and metal femoral heads on conventional polyethylene in young and active patients: a matched-pair analysis. J Bone Joint Surg 95:1193–1197
Lee PCP, Shih CHC, Chen WJW, Tu YKY, Tai CLC (1999) Early polyethylene wear and osteolysis in cementless total hip arthroplasty: the influence of femoral head size and polyethylene thickness. J Arthroplasty 14:976–981
Dumbleton JH, Manley MT, Edidin AA (2002) A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 17:649–661
Bragdon CR, Martell JM, Greene ME, Estok II DM, Thanner J, Kärrholm J, Harris WH, Malchau H (2006) Comparison of femoral head penetration using RSA and the Martell method. Clin Orthop Relat Res 448:52–57
Ranawat AS, Tsailis P, Meftah M, Koob TW, Rodriguez JA, Ranawat CS (2012) Minimum 5-year wear analysis of first-generation highly cross-linked polyethylene in patients 65 years and younger. J Arthroplast 27:354–357
Bragdon CR, Kwon YM, Geller JA, Greene ME, Freiberg AA, Harris WH, Malchau H (2007) Minimum 6-year followup of highly cross-linked polyethylene in THA. Clin Orthop Relat Res 465:122–127
Smith PN, Ling RS, Taylor R (1999) The influence of weight-bearing on the measurement of polyethylene wear in THA. J Bone Joint Surg Br 81:259–265
Bragdon CR, Thanner J, Greene ME, Malchau H, Digas G, Harris WH, Kärrholm J (2006) Standing versus supine radiographs in RSA evaluation of femoral head penetration. Clin Orthop Relat Res 448:46–51
Digas G, Kärrholm J, Thanner J, Herberts P (2007) 5-year experience of highly cross-linked polyethylene in cemented and uncemented sockets: two randomized studies using radiostereometric analysis. Acta Orthop 78:746–754
Dorr LD, Wan Z, Shahrdar C, Sirianni L, Boutary M, Yun A (2005) Clinical performance of a Durasul highly cross-linked polyethylene acetabular liner for total hip arthroplasty at five years. J Bone Joint Surg Am 87:1816–1821
Triclot P, Grosjean G, El Masri F, Courpied JP, Hamadouche M (2007) A comparison of the penetration rate of two polyethylene acetabular liners of different levels of cross-linking. A prospective randomised trial. J Bone Joint Surg Br 89-B:1439–1445
Garcia-Rey E, Garcia-Cimbrelo E, Cruz-Pardos A, Ortega-Chamarro J (2008) New polyethylenes in total hip replacement: a prospective comparative clinical study of two types of liner. J Bone Joint Surg Br 90-B:149–153
McCalden RW, MacDonald SJ, Rorabeck CH, Bourne RB, Chess DG, Charron KD (2009) Wear rate of highly cross-linked polyethylene in total hip arthroplasty. A randomized controlled trial. J Bone Joint Surg Am 91:773–782
Thomas GER, Simpson DJ, Mehmood S, Taylor A, McLardy-Smith P, Gill HS, Murray DW, Glyn-Jones S (2011) The seven-year wear of highly cross-linked polyethylene in total hip arthroplasty: a double-blind, randomized controlled trial using radiostereometric analysis. J Bone Joint Surg Am 93:716–722
Bradford L, Baker DA, Graham J, Chawan A, Ries MD, Pruitt LA (2004) Wear and surface cracking in early retrieved highly cross-linked polyethylene acetabular liners. J Bone Joint Surg Am 86:1271–1282
Baker DA, Bellare A, Pruitt L (2003) The effects of degree of crosslinking on the fatigue crack initiation and propagation resistance of orthopedic-grade polyethylene. J Biomed Mater Res A 66:146–154
Blumenfeld TJ, McKellop HA, Schmalzried TP, Billi F (2011) Fracture of a cross-linked polyethylene liner: a multifactorial issue. J Arthroplasty 26:666.e5–8
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Scemama, C., Dora, C., Langlois, J. et al. Minimum five-year wear rate of metal-on-highly cross-linked polyethylene in primary total hip arthroplasty. International Orthopaedics (SICOT) 39, 1051–1055 (2015). https://doi.org/10.1007/s00264-014-2609-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-014-2609-2