
Abstract
Purpose
Hybrid positron emission tomography/computed tomography (PET/CT) has now become available, as well as whole-body, low-dose multidetector row computed tomography (MDCT) or magnetic resonance imaging (MRI). The radioactive glucose analogue 18F-fluorodeoxyglucose (FDG) is the most widely used tracer but has a relatively low sensitivity in detecting multiple myeloma (MM). We compared FDG with a more recent metabolic tracer, 18F-fluorocholine (FCH), for the detection of MM lesions at time of disease relapse or progression.
Methods
We analyzed the results of FDG and FCH imaging in 21 MM patients undergoing PET/CT for suspected relapsing or progressive MM. For each patient and each tracer, an on-site reader and a masked reader independently determined the number of intraosseous and extraosseous foci of tracer and the intensity of uptake as measured by their SUVmax and the corresponding target/non-target ratio (T/NT).
Results
In the skeleton of 21 patients, no foci were found for two cases, uncountable foci were observed in four patients, including some mismatched FCH/FDG foci. In the 15 patients with countable bone foci, the on-site reader detected 72 FDG foci vs. 127 FCH foci (+76 %), whereas the masked reader detected 69 FDG foci vs. 121 FCH foci (+75 %), both differences being significant. Interobserver agreement on the total number of bone foci was very high, with a kappa coefficient of 0.81 for FDG and 0.89 for FCH. Measurement of uptake in the matched foci that took up both tracers revealed a significantly higher median SUVmax and T/NT for FCH vs. FDG. Almost all unmatched foci were FCH-positive FDG-negative (57/59 = 97 % on-site and 56/60 = 93 % on masked reading); they were more frequently observed than matched foci in the head and neck region.
Conclusions
These findings suggest that PET/CT performed for suspected relapsing or progressive MM would reveal more lesions when using FCH rather than FDG.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Multiple myeloma (MM) is a malignant disorder characterized by uncontrolled proliferation of clonal plasma cells accompanied by evidence of end organ damage due to the underlying plasma cell proliferative disorder (i.e., hypercalcemia, renal insufficiency, anemia, and/or bone lesions) [1].
The International Staging System (ISS) prognostic score established in 2005 did not include imaging criteria [2]. However, imaging is mandatory to assess bone lesions and extraosseous disease at diagnosis and relapse [3], to define prognosis better [4, 5], and to evaluate treatment response [6]. Moreover, functional imaging should enable earlier diagnosis of residual disease or relapse [7].
In 2005, the Durie and Salmon PLUS staging system (D/S) introduced 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) and magnetic resonance imaging (MRI) of the spine and pelvis for the evaluation of MM extent and severity at initial staging [8, 9]. In 2009 and 2014, the International Myeloma Working Group (IMWG) endorsed a variety of newer imaging technologies for MM diagnosis and management [1, 10, 11]. Whole-body, low-dose multidetector row computed tomography (MDCT) replaced whole-body X-ray (WBXR). Depending upon availability and resources, hybrid PET/CT, MDCT or MRI (whole-body or spine) were recommended for all patients with suspected low tumor load (“smoldering”) MM [10]. In 2009 also, the National Comprehensive Cancer Network (NCCN) recommended imaging with PET/CT and/or CT and/or MRI, in addition to bone marrow aspiration, for MM surveillance and follow-up [12]. FDG PET/CT allows earlier and better evaluation of therapeutic efficacy in relapsed or early progressive MM [13] than does MRI with signal abnormalities persisting years after treatment [14].
A recent systematic review supported the use of FDG PET in MM [15]. Indeed, FDG allows for whole-body evaluation in a single session [13], can assess the extent of active disease [9], detect extraosseous involvement with higher sensitivity than other imaging techniques, and evaluate treatment response [1, 16, 17]. However, FDG PET/CT does not detect “smoldering” MM [18], has low sensitivity in detecting diffuse bone marrow disease in residual or recurrent MM [3, 19] compared to whole-body MRI [20], and can present misleading physiologic uptake by other tissues (brain, heart, vessel, and muscle) [21].
To increase the sensitivity observed with FDG, several other PET tracers have been proposed for PET/CT imaging in MM patients. These include 11C-methionine [22, 23], 11C-acetate [24, 25], and 11C-choline [26]. However, because of its short half-life (20 min), 11C use is restricted to PET centers with an on-site cyclotron, whereas 18F can be produced and delivered industrially. The choline analogue 18F-fluorocholine (FCH) is registered in several European countries for the detection of neoplastic lesions with increased choline uptake, particularly for prostatic or hepatic primary cancers [27–30]. Multiple FCH foci in lytic skeletal structures have been reported in one patient referred to FCH PET/CT for prostate cancer but also presenting with MM [31].
The aim of the study was to compare the detection rate of MM-related lesions using FCH and FDG in MM patients with suspected relapse or progression.
Patients and methods
Patients
We reviewed the data of 21 patients with suspected progressive or relapsing MM who underwent both FDG and FCH PET/CT between September 2014 and October 2015. The patients were diagnosed, treated, and followed up in the hematology department of St. Antoine Hospital (Paris). They were classified according to ISS prognostic score (1 to 3) and the S/D staging system (I, II, or III). All patients who had both examinations and presented with a clinical and/or a biochemical suspicion of relapse or progression were included. Patients who were referred for staging or early monitoring of treatment were not included. The main patient characteristics at diagnosis are given in Table 1.
FDG is registered in France for the detection of suspected relapsing lymphoma or myeloma. Patients were informed that FCH had been approved as a diagnostic agent in France in 2010 and that the use of FCH PET/CT imaging to “search for enhanced choline influx” as worded in its marketing authorization, was based in MM on a recent case report [31]. The study was approved by the institutional review board (Ethics Committee of Ile de France V; n°15063) and all patients signed an informed consent form.
PET/CT procedures
Before PET/CT imaging, all patients except diabetic ones had to fast for at least 6 h. Diabetic patients fasted for 4.5 h after taking their oral medication during a meal. FCH (3 MBq/kg of body mass of Iasocholine, Iason Laboratory, Graz, Austria) or FDG (2.5 MBq/kg of body mass of Gluscan, Advanced Accelerator Applications SA, St Genis-Pouilly, France or Metatrace, PetNet solutions, Camberley, UK) was administered intravenously in an infusion line connected to saline.
A Gemini Dual PET/CT camera (Philips) with time of flight (TOF) technology was used for imaging. Low-dose CT (120 kVp, 30–50 mA.s) was acquired first, followed by PET acquisition 10–20 min after FCH injection or 60–90 min after FDG injection, covering a complete whole-body field of view, from the skull to the feet. Image reconstruction and display were performed according to European Association of Nuclear Medicine guidelines [32].
PET/CT readings
FDG and FCH PET/CT images were interpreted by two experienced readers, first by an on-site reader, then by a masked external reader. The on-site reader was a nuclear medicine specialist of the PET/CT. Radiologic examinations and medical history were available for reporting and his/her report was quoted without modification.
The masked reader was blinded to the history of the patient and to the results of other imaging modalities. He read the two paired FDG and FCH PET/CTs of a given patient in one single session, in order to determine whether each focus was matched or unmatched for FCH and FDG uptake.
Foci were considered positive when high tracer uptake occurred in non-physiological locations, either intraosseous or extraosseous. High tracer uptake was defined as either visually greater than that of the liver [13] or visually greater than that of the contralateral healthy bone or of the healthy adjacent tissue in unpaired structures [33]. Since the physiological uptake by the liver is clearly greater for FCH than for FDG, the second alternative was the most frequently used for reporting FCH PET/CT. Readers recorded all cases with no suspicious focus (without any SUVmax or T/NT measurement) and all cases with bone foci.
The total number of countable intraosseous foci per patient was determined for each tracer by both readers, according to three anatomical sites: head and neck (including the cervical spine), torso, or limbs. All foci were quoted as matched if visible with both tracers or unmatched if visible with one single tracer. Each reader recorded the maximum standardized uptake value (SUVmax) of all matched or unmatched foci from the attenuation-corrected PET data of each tracer. The target/non-target (T/NT) ratio of SUVmax was calculated for each tracer, the non-target region of interest being selected in the contralateral bone, or in adjacent bone in unpaired structures. Extraosseous foci and their SUVmax were recorded separately; the reader quoted if they were likely to be MM or of another origin.
The presence of areas of focal uptake of FCH or FDG in this type of patients (MM patients with suspected relapse or progression) represents in itself the presence of disease without the need for confirmation using a direct or composite standard of truth.
Statistical analysis
We compared the ability of FDG and FCH PET/CTs to detect suspected malignant lesions on per-patient, per-site, and per-lesion bases. Wilcoxon’s test was used to compare the number of foci detected by each tracer and the kappa coefficient was calculated to assess between-reader agreement on the number of foci. FCH and FDG SUVmax values and T/NT ratios were compared on a per-lesion basis by Wilcoxon’s test and their correlation was evaluated by Spearman’s rank correlation test. The Mann–Whitney test was used to compare the tracer uptake observed in matched or in unmatched foci. The Chi-square test was used to compare the spatial distribution of foci. We used MedCalc statistical software (Ostend, Belgium).
Results
Patient-based analysis
Population
In 21 patients with suspected progressive or relapsing MM (eight males, 13 females; mean age 64.2 years, median 64, range 46–81), 19 were biochemically confirmed with monoclonal or free light spike progression. The mean interval between the two imaging sessions was 10.4 days (median 7, range 3–35). Six patients were treated at the time of imaging: lenalidomide (n = 2), lenalidomide and dexamethasone (n = 1), bortezomib (n = 1), pomalidomide (n = 1), pomalidomide, cyclophosphamide, and dexamethasone (n = 1) (Table 1).
Bone involvement
No bone focus was detected visually with both tracers in 2/21 patients (#8, #14) by both the on-site and masked readers (Table 2). In patient #14, femoral osteonecrosis explained the clinical suspicion of progression. In patient #8, progression was suspected on the basis of a clinical and biological inflammatory syndrome that turned out to be related to breast malignancy. Those cases corresponded to true negative results for relapse of MM.
Among the 19 patients with positive PET/CT for intraosseous relapse or progression of MM, both readers reported innumerable bone foci with both tracers in four patients (#10, #11, #15, #19). Bone marrow infiltration was confirmed on bone marrow evaluation. A clear mismatch between FCH and FDG uptake of some foci was observed in patient #19 (Fig. 1).

Patient #19: FDG PET MIP (a), FDG PET/CT axial slices (sacrum, pelvis, and Th10) (b), CT (c), FCH PET/CT axial slices (sacrum, pelvis, and Th10) (d), and FCH PET MIP (e). Patient with innumerable bone foci on both FDG and FCH PET/CTs. The majority of foci are matched, taking-up both tracers (white full arrow). However, some foci appear more intense with FDG (black full arrow) and other with FCH (black dotted arrow). Furthermore, some lesions visible on CT take-up neither FDG nor FCH (white dashed arrow), probably as a consequence of the previous treatment
In the remaining 15 patients, both readers detected significantly more bone foci with FCH than with FDG. The on-site reader described 72 foci on FDG PET/CT vs. 127 with FCH (+76 %). The mean number of foci per patient was 4.8 (median 4, range 0–15) with FDG vs. 8.4 with FCH (median 6, range 1–27) (Wilcoxon p = 0.001). The masked reader described 69 in FDG PET/CT vs. 121 foci on FCH (+75 %) and a mean number of 4.6 FDG foci (median 3, range 0–14) per patient vs. 8.1 FCH foci (median 6, range 1–25) (Wilcoxon p < 0.001). No significant difference in the number of foci was observed according to type of MM (i.e., producing IgG kappa, free light chains, or other type of chain). Kruskal–Wallis test did not show any significant difference: p > 0.3 for both tracers and both readers. The kappa coefficient for interobserver agreement for the total foci number per patient was very high and somewhat higher for FCH (κ = 0.89 [CI 0.82–0.97]) than for FDG (κ = 0.81 [CI 0.71–0.91]). Unmatched intraosseous foci visible on FCH but not on FDG PET/CT were observed in 13 patients by both readers (Fig. 2). Unmatched foci visible on FDG but not on FCH PET/CT were observed in two of those 15 patients by the on-site reader and in three patients by the masked reader, all those patients also having one or several foci visible only with FCH (Table 2).

Maximum intensity pixel (MIP) visualization of PET in two different patients. FCH shows much more bone foci than FDG in patient #2 (a). FCH and FDG show the same bone foci in patient #3 (b)
Presence of extraosseous foci
Extraosseous foci were reported concordantly by both readers as 11 FCH foci in five patients and seven FDG foci in four patients. Only three matched foci in two patients (#2, #11) were evocative of MM and confirmed as such by the clinician based on independent biochemical and imaging data (Table 2). Concerning foci that were not evocative of MM, two patients had extraosseous foci only visible on FCH PET/CT: one in the right breast of patient #8 that lead to the discovery of a breast cancer, which was responsible for the inflammatory syndrome, and one in the liver of patient #6 that was not further explored. Matched foci that were not evocative of MM were due to paraneoplastic inflammatory syndrome in patient #8 or to pneumopathy in patient #18.
Lesion-based analysis
Countable bone foci in 15 patients (Table 3)
According to on-site reading, 70 of the 72 FDG foci also took up FCH, whereas 57 FCH foci were not matched with FDG foci. According to masked reading, 65 of the 69 FDG foci were matched with FCH foci, whereas 56 FCH foci were unmatched with FDG foci. One FDG focus in the 5th rib of patient #5 that was not matched with a FCH focus was noted by both readers and proved to be a post-traumatic lesion, i.e., a wrong FDG result. No conclusion can be obtained for the other FDG foci that were not matched by FCH, one noted by both readers and two by the masked reader only.
The appearance on CT of the 51 unmatched foci on PET (FCH-positive and FDG-negative) that were common to the on-site and the masked readers was determined by consensus reading as follows: osteolytic lesion in 35 % of foci, osteoblastic lesion in 24 % of foci, mixed type in 6 % of foci and no definite morphological abnormality in the remaining 35 % of foci.
Localization of countable bone foci
Overall, the largest number of foci was seen in the torso and, with rather similar numbers, in the limbs or the head and neck. However, the proportion of unmatched FCH-positive FDG-negative foci was significantly greater compared with that of matched foci in the head and neck (17/26 = 65 % by on-site reading, 14/23 = 61 % by masked reading) (Fig. 3) than in the torso (33/74 = 45 % by on-site reading, 35/71 = 48 % by masked reading) and even less in the limbs (7/27 = 26 % for both readings) (Chi-square test, p < 0.03 for both readings).

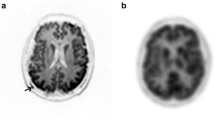
Coronal slices of the same patient. Negative FDG PET/CT (a), small lytic lesions in the skull on CT (b), and positive FCH PET/CT (c) in patient #2
Intensity of uptake by countable bone foci (Table 3)
In case of matched foci, median SUVmax and T/NT were significantly greater for FCH than for FDG. The SUVmax and T/NT ratios of both tracers were significantly correlated. According to on-site reading, the SUVmax of matched foci was greater for FCH than for FDG in 51/70 = 73 % of foci; this frequency was 46/65 = 71 % according to masked reading. The median FCH SUVmax and T/NT ratios of matched foci were significantly greater than those of the unmatched FCH foci, which were not visible with FDG.
If the criterion of visual intensity of focal uptake greater than that of the liver had been applied alone, FDG PET/CT would have been considered wrongly as negative for MM in two further patients (#12, #18) (Fig. 4) by on-site reading and even a third (#20) by masked reading. The total number of FDG lesions would have been reduced to 42 instead of 71 by on-site reading and to 44 instead of 69 by masked reading.

MIP, transversal, and coronal slices. In patient #18, one single mild intraosseous focus was visible on FDG PET/CT (a) in the left femoral shaft, SUVmax = 2.5 according to both readers whereas SUVmax of the liver was 3.4. The focus was more easily detected on FCH PET/CT (b) SUVmax = 3.1
Interobserver agreement on tracer uptake level in 62 common matched and 51 common unmatched foci was fair. There was no significant difference between the readers in mean SUVmax or T/NT values for a given tracer (Wilcoxon’s tests all p > 0.35). The correlation coefficients between the values measured by the two readers for a given tracer were all highly significant (all p < 0.005).
Extraosseous foci
All extraosseous foci had a greater SUVmax with FCH than with FDG. Two foci, which were not evocative of MM, were only visible on FCH PET/CT: one in the right breast (SUVmax = 2.1) and one in the liver (SUVmax = 13).
Discussion
Choline and choline analogues seem promising agents for PET/CT imaging of malignancies because choline is a component of phosphatidylcholine, an essential constituent of cell membrane phospholipids, and may be actively taken up by some malignant cells, like MM, to facilitate rapid duplication. Serum lysophospholipid levels (lysophosphatidylcholine and lysophosphatidic acid) are significantly increased in MM patients compared to healthy subjects [34]. These metabolic characteristics may explain the excellent delineation of MM lesions that we observed with FCH PET/CT in 19/21 MM patients with suspected relapsing or progressive disease.
All other studies in search for an alternative to FDG in MM PET imaging used 11C labeled tracers. Compared to 18F, which is the radionuclide used for FDG and FCH labeling, 11C has the advantage of a reduced radiation exposure of the patient and offers the possibility of performing a complementary FDG PET on the same day. On the other hand, the 20-min half-life of 11C leads to very tough logistical constraints that can be met by only very few nuclear medicine centers so far, whereas FCH may be produced industrially and delivered as a ready to use radiopharmaceutical similarly to FDG.
In our study, the readers reported on PET/CTs with both tracers no visible focus in two patients, true-negative results, and innumerable bone foci in four patients, true-positive results. In the 15 patients with countable bone foci, around 75 % more bone foci were detected with FCH than with FDG. Those results that were obtained using a fluorinated analogue of choline are entirely consistent with the higher detection rate and greater uptake intensity (SUVmax) for MM bone lesions previously observed using other tracers of lipid metabolism, either 11C-choline or 11C-acetate, in comparison with FDG [24–26]. Similar results were also reported when comparing the uptake in the skeletal lesions of MM patients of an amino acid for PET imaging, 11C-methionine, with that of FDG [23] or with the 11C-methionine uptake in the skeleton of control patients with hyperparathyroidism [22].
Observations by the on-site and masked readers were highly consistent; interobserver agreement on the total number of foci and their SUVmax was very high for both tracers, confirming that PET/CT readings have satisfactory reproducibility. None of the above-mentioned studies checked the reproducibility of visual or quantitative reporting.
The study closest to ours is that of Nanni et al. [26] using 11C-choline. Although they gave consistent results concerning the detection of a greater number of foci with a more intense uptake using the non-FDG tracer, the other pilot studies recruited all patients at an earlier phase of MM management, staging, or initial treatment evaluation, and used non-choline tracers, either 11C-methionine [22, 23] or 11C-acetate [24, 25]. A review of their main results has been recently published [35]. They are not directly comparable to the present study.
In the study of Nanni et al. [26], MM relapse was suspected in four patients out of the ten patients who underwent 11C-choline and FDG PET/CTs. In two of them, the same number of foci was observed with both tracers (17 foci in total), but in the two other patients, a greater number of foci was visible with 11C-choline than with FDG (respectively 18 vs. 3 in total). In our larger series, both readers described unmatched foci that were only visible on FCH PET/CT in a larger proportion of patients (13/21 = 62 %) than that of Nanni et al. (2/4 = 50 %). This is probably due to the very limited number of patients with suspected MM relapse in this series.
According to the tables of the article of Nanni et al. [26], 20 foci were detected with FDG vs. 35 with FCH, i.e., +75 %, which is the same rate as in our study. The SUVmax was greater with FCH in 26/35 = 74 % of foci, in full accordance with 73 % of foci by on-site reading in our series.
In our study, the unmatched FCH-positive and FDG-negative bone foci had a significantly lower median FCH SUVmax and T/NT ratio than foci positive with both tracers. This was not tested by Nanni et al. They might correspond to lesions detected early and/or at a less aggressive stage when glucose metabolism was not yet substantially enhanced, whereas choline turnover was already enhanced but not as intensely as in more advanced lesions. This hypothesis seems to be supported by the corresponding aspect of those foci on CT which was osteolytic only in a minority of lesions (35 %), whereas Nakamoto et al. [23] found osteolytic CT pattern in 56 % of PET/CT-positive foci, regardless whether they took-up one or both tracers (Chi-square test p < 0.001). The proportion of PET/CT foci that did not correspond to a definite morphological abnormality on CT was 39 % in their series, similar to 35 % of unmatched foci in our series. Although the exact histology of those foci is not known, they constitute important information to warn about MM relapse while CT is still unaffected. Furthermore, in our series, the anatomic distribution of those unmatched foci in the skeleton was significantly different from that of the matched lesion: bone foci in head and neck were quoted as unmatched significantly more frequently. This poor performance of FDG in visualizing lesions of the skull is probably related to the high FDG uptake by the brain cortex, which can mask the presence of skull foci on FDG PET (Fig. 3). A case report already suggested that another choline analogue labeled with 18F, 18F-fluoroethyldimethyl-2-hydroxyethylammonium (FEC), is superior to FDG in detecting bone skull lesions in MM patients [36].
In one patient (#16) whose MM produced free light chains, only FCH was able to show bone foci. According to Machida et al. [37], FDG does not accumulate in bone marrow lesions of IgD-λ type MM, whereas Nakamoto et al. [23] observed non-FDG avid myelomas other than IgD-λ type MM. Our study found no relationship between MM type and number of visible lesions regardless of which tracer was used.
In the study of Nanni et al. [26], the discovery of a large number of foci on 11C-choline PET/CT, unmatched on FDG PET/CT, radically changed the management of two of the four patients suspected of MM relapse. In our pilot study, the management of patients suspected of persistent or relapsing MM was not expected to be modified on the basis of FCH PET/CT. However, the potential role of FCH to influence patient management is confirmed by the discovery of a breast cancer that did not take up FDG in the context of an inflammatory syndrome.
Reverse unmatched bone foci taking up only FDG were much rarer in our study: two or four according to the readers in the 15 patients with countable bone foci, and also some innumerable bone foci (Fig. 1). In the study of Nanni et al. [26], only one patient referred for post-therapy evaluation had one FDG-positive 11C-choline-negative focal area located in the pelvis. The mechanism and significance of those foci may actually be multiple. Both readers reported a focus visible with FDG only in a rib of patient #5 that proved to be a post-traumatic lesion. This wrong result observed with FDG was avoided with FCH. The three other foci could not be characterized but their FDG SUVmax was significantly less than that of matched foci (Table 3). They could correspond to non-specific bone focal uptake of FDG rather than to aggressive lesions. However, in the case of innumerable bone foci (Fig. 1), this pattern might correspond to dedifferentiation of the cancer cells and thus correspond to a poorer prognosis, similarly to what has been shown in hepatocellular carcinoma [30].
Extraosseous matched foci were correctly classified by both readers as MM or of a different nature: inflammatory or infectious lymph nodes. A FCH focus in the breast corresponded to an unknown carcinoma and the nature of a FCH-positive FDG-negative focus in the liver was not demonstrated. The hypotheses were either well-differentiated hepatocellular carcinoma or focal nodular hyperplasia [30], more probable in a young woman.
The main limitation of this pilot study, shared with all the above-mentioned pilot studies using other tracers, is the lack of standard of truth on a per lesion level. The confirmation (or the exclusion in two cases) of relapsing or progressive MM was based on a composite evidence without an evaluation of all individual lesions, in particular intraosseous lesions.
Another limitation is the fact that the on-site reader was not blinded to the FDG results when interpreting the FCH images and that the masked reader interpreted both PET/CTs of a patient in the same session. Actually, a possible carryover of information could occur in both senses, and most probably from FCH to FDG since fewer lesions were visible on FDG PET/CT. This possible carryover of information would contribute to reduce the difference between detection rates of the tracers. Thus the very clear superiority of detection rate with FCH over FDG could have been even more obvious by performing one reading session per tracer with a wash-out period between the two sessions. However, the classification of each lesion as matched or unmatched using this procedure would have been far less precise.
Conclusions
Tracer uptake was more intense and detection of bone foci was better using FCH than FDG in patients with relapsing or progressive MM. These findings require confirmation in large prospective series, in a variety of settings (e.g., initial MM staging, assessment of treatment response including after stem cell transplantation), analyzing the impact of FCH PET/CT on patient management, the adequacy of changes, and the prognostic significance of mismatched foci in the same patient. FCH PET/CT is widely available in several countries and might constitute a promising imaging modality in MM.
References
Dimopoulos M, Terpos E, Comenzo RL, et al. International Myeloma Working Group consensus statement and guidelines regarding the current role of imaging techniques in the diagnosis and monitoring of multiple Myeloma. Leukemia. 2009;23:1545–56.
Greipp PR, San Miguel J, Durie BG, et al. International staging system for multiple myeloma. J Clin Oncol. 2005;23:3412–20.
Derlin T, Weber C, Habermann CR, et al. (18)F-FDG PET/CT for detection and localization of residual or recurrent disease in patients with multiple myeloma after stem cell transplantation. Eur J Nucl Med Mol Imaging. 2012;39:493–500.
Zamagni E, Patriarca F, Nanni C, et al. Prognostic relevance of 18-F FDG PET/CT in newly diagnosed multiple myeloma patients treated with up-front autologous transplantation. Blood. 2011;118:5989–95. Erratum in: Blood. 2012;120:2349.
Mai EK, Hielscher T, Kloth JK, et al. A magnetic resonance imaging-based prognostic scoring system to predict outcome in transplant-eligible patients with multiple myeloma. Haematologica. 2015;100:818–25.
Ailawadhi S, Abdelhalim AN, Derby L, et al. Extent of disease burden determined with magnetic resonance imaging of the bone marrow is predictive of survival outcome in patients with multiple myeloma. Cancer. 2010;116:84–92.
Elliott BM, Peti S, Osman K, et al. Combining FDG-PET/CT with laboratory data yields superior results for prediction of relapse in multiple myeloma. Eur J Haematol. 2011;86:289–98.
Durie BG. The role of anatomic and functional staging in myeloma: description of Durie/Salmon PLUS staging system. Eur J Cancer. 2006;42:1539–43.
Mihailovic J, Goldsmith SJ. Multiple Myeloma: 18F-FDG-PET/CT and diagnostic imaging. Semin Nucl Med. 2015;45:16–31.
Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15:538–48.
Rajkumar SV, Harousseau JL, Durie B, et al. Consensus recommendations for the uniform reporting of clinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood. 2011;117:4691–5.
Anderson KC, Alsina M, Bensinger W, et al. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: multiple myeloma. J Natl Compr Canc Netw. 2009;7:908–42.
Mesguich C, Fardanesh R, Tanenbaum L, Chari A, Jagannath S, Kostakoglu L. State of the art imaging of multiple myeloma: comparative review of FDG PET/CT imaging in various clinical settings. Eur J Radiol. 2014;83:2203–23.
Hillengass J, Ayyaz S, Kilk K, et al. Changes in magnetic resonance imaging before and after autologous stem cell transplantation correlate with response and survival in multiple myeloma. Haematologica. 2012;97:1757–60.
Weng WW, Dong MJ, Zhang J, Yang J, Xu Q, Zhu YJ, et al. A systematic review of MRI, Scintigraphy, FDG-PET and PET/CT for diagnosis of multiple myeloma related bone disease - Which is best? Asian Pac J Cancer Prev. 2014;15:9879–84.
Schirrmeister H, Bommer M, Buck AK, et al. Initial results in the assessment of multiple myeloma using 18F-FDG PET. Eur J Nucl Med Mol Imaging. 2002;29:361–6.
Bredella MA, Steinbach L, Caputo G, Segall G, Hawkins R. Value of FDG PET in the assessment of patients with multiple myeloma. AJR Am J Roentgenol. 2005;184:1199–204.
Durie B, Waxman A, D’Agnolo A, Williams CM. Whole-body (18)F-FDG PET identifies high-risk myeloma. J Nucl Med. 2002;43:1457–63.
Spinnato P, Bazzocchi A, Brioli A, et al. Contrast enhanced MRI and 18F-FDG PET-CT in the assessment of multiple myeloma: a comparison of results in different phases of the disease. Eur J Radiol. 2012;81:4013–8.
Shortt CP, Gleeson TG, Breen KA, et al. Whole-body MRI versus PET in assessment of multiple myeloma disease activity. AJR Am J Roentgenol. 2009;192:980–6.
Yasar Z, Acat M, Onaran H, Dincer HE, Cetinkaya E, Korkmaz AN. False-positive 18-fluorodeoxyglucose positron emission tomography-computed tomography (FDG PET/CT) scans mimicking malignancies. Med Glas (Zenica). 2015;12:40–6.
Dankerl A, Liebisch P, Glatting G, et al. Multiple myeloma: molecular imaging with 11C-methionine PET/CT – initial experience. Radiology. 2007;242:498–508.
Nakamoto Y, Kurihara K, Nishizawa M, et al. Clinical value of 11C-methionine PET/CT in patients with plasma cell malignancy: comparison with 18F-FDG PET/CT. Eur J Nucl Med Mol Imaging. 2013;40:708–15.
Ho CL, Chen S, Leung YL, et al. 11C-Acetate PET/CT for metabolic characterization of multiple myeloma: a comparative study with 18F-FDG PET/CT. J Nucl Med. 2014;55:749–52.
Lin C, Ho CL, Ng SH, et al. (11)C-acetate as a new biomarker for PET/CT in patients with multiple myeloma: initial staging and postinduction response assessment. Eur J Nucl Med Mol Imaging. 2014;41:41–9.
Nanni C, Zamagni E, Cavo M, et al. 11C-choline vs. 18F-FDG PET/CT in assessing bone involvement in patients with multiple myeloma. World J Surg Oncol. 2007;5:68.
Seo S, Hatano E, Higashi T, et al. Fluorine-18 fluorodeoxyglucose positron emission tomography predicts tumor differentiation, P-glycoprotein expression, and outcome after resection in hepatocellular carcinoma. Clin Cancer Res. 2007;13:427–33.
Talbot JN, Gutman F, Fartoux L, et al. PET/CT in patients with hepatocellular carcinoma using [18F]fluorocholine: preliminary comparison with [18F]FDG PET/CT. Eur J Nucl Med Mol Imaging. 2006;33:1285–9.
DeGrado TR, Coleman RE, Wang S, et al. Synthesis and evaluation of 18F-labeled choline as an oncologic tracer for positron emission tomography: initial findings in prostate cancer. Cancer Res. 2001;61:110–7.
Talbot JN, Fartoux L, Balogova S, et al. Detection of hepatocellular carcinoma with PET/CT: a prospective comparison of 18F-Fluorocholine and 18F-FDG in patients with cirrhosis or chronic liver disease. J Nucl Med. 2010;51:1699–706.
Calabria F, Chiaravalloti A, Schillaci O. 18F-Choline PET/CT pitfalls in image interpretation. An update on 300 examined patients with prostate cancer. Clin Nucl Med. 2014;39:122–30.
Boellaard R, O’Doherty MJ, Weber WA, et al. FDG PET and PET/CT: EANM procedure guidelines for tumour PET imaging: version 1.0. Eur J Nucl Med Mol Imaging. 2010;37:181–200.
Bartel TB, Haessler J, Brown TL, et al. F18-fluorodeoxyglucose positron emission tomography in the context of other imaging techniques and prognostic factors in multiple myeloma. Blood. 2009;114:2068–76.
Sasagawa T, Okita M, Murakami J, Kato T, Watanabe A. Abnormal serum lysophospholipids in multiple myeloma patients. Lipids. 1999;34:17–21.
Vij R, Fowler KJ, Shokeen M. New approaches to molecular imaging of multiple myeloma. J Nucl Med. 2016;57:1–4.
Xin C, Ruixue C, Fang L, Hongming Z. Lesions of multiple myeloma adjacent to the skull are better visualized on F-18 fluoroethyldimethyl-2-hydroxyethylammonium (FECH) PET images than on F-18 FDG PET images. Clin Nucl Med. 2011;36:912–4.
Machida H, Shinohara T, Hino H, et al. Immunoglobulin D-lambda type multiple myeloma presenting with FDG-PET/CT negative bone marrow involvement. Intern Med. 2011;50:1483–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments. The study was approved by the institutional review board (Ethics Committee of Ile de France V; n°15063).
Conflicts of interest and funding
The authors declare that they have no conflict of interest.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Cassou-Mounat, T., Balogova, S., Nataf, V. et al. 18F-fluorocholine versus 18F-fluorodeoxyglucose for PET/CT imaging in patients with suspected relapsing or progressive multiple myeloma: a pilot study. Eur J Nucl Med Mol Imaging 43, 1995–2004 (2016). https://doi.org/10.1007/s00259-016-3392-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-016-3392-7