
Abstract
Ultrasound (US) is widely used in pediatric musculoskeletal pathology at all ages. Although the focus is often on soft tissues, joints and cartilage, the examiner might be confronted with changes in the underlying bone surface that are important to understand and integrate in the diagnosis. This article illustrates the normal US aspects of the cortical bone surface and periosteum, as well as the most common US anomalies seen in infections, trauma and bone tumors in children.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
During examination of any part of the body, the US beam is reflected at the interface between cortical bone and soft tissue. This interface can itself be analyzed in detail with high-frequency transducers. In pediatrics, the small size of the patients and the relatively low percentage of body fat make the bone surface easily accessible to high-resolution US. The lack of ionizing radiation means there is no restriction to obtaining comparative views, which are very helpful in distinguishing between normal and pathological features.
Ultrasound is widely used to examine soft tissues and joints, as well as unossified segments of the pediatric bone, but the focus of this pictorial essay is on the changes revealed by US at the surface of the cortical bone. We review normal findings and variants, as well as the most common changes of the bone surface seen in infection and inflammation, trauma and tumors in children.
Technical considerations and normal findings
Ultrasound analysis of the cortical bone surface is performed with high-frequency linear transducers (12–18 MHz), in standard longitudinal and transverse planes, as well as oblique planes adapted to each region. The skull, rib cage and peripheral skeleton are the easiest segments to examine. Analyzing the bones of the pelvis and the spine is more difficult, especially in older children, because of the limited access, depth of the structures and complexity of the anatomy. Longitudinal views in bidimensional (2-D) mode are the most useful to detect an anomaly in the bone surface, while transverse views add complementary information, especially in the case of periosteal anomalies or masses involving bone. Doppler US is not systematically needed, but it provides additional information regarding the vascularization of inflammatory or tumor tissue involving the bone cortex.
For the detection of subtle differences in paired bones, it is mandatory to obtain comparative views of the healthy side. Direct access to the child and careful identification of painful areas during the US examination are key guiding elements. This is particularly true in young children, who when asked, cannot localize pain precisely. In this way, examiners adapt each US investigation to their direct clinical evaluation of the child.
On US, the normal surface of the bone cortex is a continuous hyperechoic line, reflecting the US beam almost entirely (Fig. 1). The cortical bone surface of the diaphysis of long bones is smooth and uninterrupted, except by vascular grooves. At the metaphysis, normal variants can cause confusion with an anomaly: examples include a slight step-off or thickening at the metaphyseal collar [1], irregularities of the zone of provisional calcification at the junction between the metaphysis and growth cartilage, as well as cortical defects and cortical desmoids (Fig. 2). The multi-fragmented aspect of ossification centers of the epiphyses and apophyses in children can be a source of error on US, just as on conventional radiographs (Fig. 2). Being aware of these normal variants, which are very common in children, prevents overinterpretation.

Normal US of the cortical bone surface. a, b Longitudinal views of the knee in an 18-month-old boy (a) and the tibial shaft in a 17-month-old boy (b): the interface at the surface of the normal cortical bone is hyperechoic, regular and uninterrupted, reflecting the US beam almost entirely (arrow). The normal periosteum is visible as a thin hypoechoic line along the surface of the bone (arrowheads). The patella is not yet ossified, appearing entirely hypoechoic (*)

Normal US findings of the bone surface that can be confused with lesions. These findings are very common and do not require additional imaging; in uncertain cases, consideration of the clinical context and sometimes the addition of a complementary radiograph can be helpful. a Longitudinal US of the proximal humerus in an 18-month-old girl shows a slight step-off at the metaphyseal collar (solid arrow) and an irregular contour of the bone surface at the zone of provisional calcification (dashed arrows). b Longitudinal view of the normal proximal femur in a 33-month-old boy. US shows irregular surface of the ossification center of the femoral head (solid arrow) and slight loss of definition and irregularity at the metaphyseal collar (dashed arrow). c Longitudinal view of the distal femoral metaphysis in a 9-year-old girl shows deformation of the posterior cortex (arrows), with no interruption or soft-tissue anomaly at the insertion of the medial gastrocnemius head (arrowheads). The image and the location are typical of a cortical desmoid
The cortical bone surface is covered by a thin layer of periosteum, seen as a hypoechoic line on US (Figs. 1 and 2). In young children the periosteum is easier to identify because it is thicker than in adults. This is because of its richer metabolic activity in comparison to the adult periosteum [2, 3]. The periosteum is firmly attached at the physis, but more loosely along the bone shaft, especially in children. This explains the easier displacement of the periosteum by fluid collections such as abscess or hematoma, along the shaft of the bone [3]. On Doppler US, the normal periosteum appears avascular, but feeding vessels crossing it to reach and penetrate the bone cortex are well seen [4].
Many processes that disrupt the normal cortical bone surface and the overlying periosteum can be spotted with US. However, as illustrated in the examples presented later, some US findings lack specificity. It is therefore essential to integrate the images within the clinical context of the child and reflect on possible additional imaging, when necessary. The combination of US and radiography often yields sufficient information, especially in an emergency setting. If further imaging is necessary, the initial evaluation by US, with or without radiography, helps to guide the choice of additional examinations.
Infection and inflammation
Acute osteomyelitis in children is an infection of the bone marrow caused by hematogenous spread of bacteria [5]. Early diagnosis of suspected acute osteomyelitis is challenging; radiographs might demonstrate swelling of soft tissues, but periosteal reaction only becomes detectable when ossified, which can happen as late as 10 days to 3 weeks after onset of symptoms [6]. More sensitive imaging techniques, such as bone scan or MRI, are not always available and may require sedation in young children.
Ultrasound first reveals swelling and hyperemia of regional soft tissues, which are nonspecific, but also helps to pinpoint the region of interest. These changes appear as early as 1–2 days after the onset of symptoms [7]. As soon as the infection has reached the cortical bone, US changes in the bone surface and the periosteum become visible. This precedes radiographic findings by several days [8]. US demonstrates thickening of the periosteum, most commonly at the metaphysis of a long bone; hyperemia in the periosteum might also be present, but no earlier than 4 days after the onset of symptoms [7] (Fig. 3).

US in a 12-year-old boy referred to the emergency room for suspected arthritis of the knee. US findings at the distal femoral metaphysis are compatible with early osteomyelitis, at a stage where radiographs were still normal. a Longitudinal US of the distal femur shows soft-tissue edema (*) and thickening of the periosteum (arrows); the surface of the cortical bone is slightly irregular but uninterrupted (arrowheads). b The periosteum and soft tissues are hypervascular on longitudinal color Doppler US
Pus from the infected bone can reach the bone surface, creating a subperiosteal abscess. On US, this appears as a spindle-shape fluid collection on the surface of the bone, with displacement of the periosteum [9] (Fig. 4). Subperiosteal abscess is more common in children in comparison to adults [9, 10] because children’s periosteum is less firmly attached to the bone [2]. The fluid can be either hypo- or hyperechoic and appears avascular on color Doppler. The abscess is strictly located on the surface of the bone and is limited by the displaced periosteum, although this limit is often difficult to identify from the surrounding soft tissue. The detection of a subperiosteal abscess is important because surgical intervention is usually required in these cases [9, 11].

Acute osteomyelitis in a 20-month-old girl. Longitudinal US of the 4th metatarsal reveals a small fluid collection along the surface of the bone, representing a subperiosteal abscess (arrows) and edema in the soft tissues (*). The periosteal limit of the abscess is indistinguishable from the overlying soft tissue, but the spindle shape, the disposition along the bone shaft and the limit at the physis are all elements pointing to a subperiosteal abscess. Surgical drainage was performed based on the US findings, with positive cultures of the subperiosteal fluid for group A Streptococcus
As the infection progresses, changes in the cortical bone become visible on US, first as irregularities of the bone surface in comparison to the healthy opposite side and later as a defect in the bone surface (Fig. 5), corresponding to the radiologic finding of osteolysis [4, 5]. In cases of osteitis by spread of a regional infection, US detects disruption of the cortical bone surface with subperiosteal abscess formation, inflammation and fistulas in the overlying soft tissues. Some of the more common uses of US in the context of infection are detection of subperiosteal abscess in mastoiditis (Fig. 6) [12], intra-orbital abscess in retroseptal eye infections [13, 14] and mandibular osteomyelitis (Fig. 7).

Acute osteomyelitis in a 14-month-old boy. a, b Comparative longitudinal US views of the distal metaphysis of the left (a) and right (b) femurs demonstrate focal interruption of the bone surface (arrows) and periosteal thickening (*) on the right (R). The left (L) side is normal

US findings in mastoiditis. a Transverse oblique view of the retro-auricular region in a 6-year-old girl displays an irregular but uninterrupted surface of the mastoid (arrowhead) and a small subperiosteal abscess (*); the elevated periosteum is visible as a hyperechoic line limiting the fluid collection (arrows). b A more advanced case in a 4-month-old boy, transverse oblique US demonstrates destruction of the bone surface (arrows), with a large abscess extending into the soft tissues (*). c The same boy as in (b), the wall of the abscess appears vascularized on transverse oblique color Doppler US, with no signal in the central fluid area (*). Performing US in these cases allows a better selection of those children requiring additional CT imaging and drainage. In cases where neurologic complications are suspected based on the clinical presentation, CT is performed to exclude intracranial complications

Inflammatory swelling of the jaw in a 5-year-old girl with suspected abscess. US in transverse oblique view indicates interruption (*) of the horizontal branch of the mandible (arrowheads) with thick hypoechoic material fistulizing in the soft tissues (arrows). The source of the infection was a dental abscess. The child was referred to the maxillo-facial surgery department for further treatment
In the specific case of sickle cell disease, US has been advocated as a useful tool to distinguish between vaso-occlusive crisis and osteomyelitis [15]. In the appropriate clinical setting, identification of a subperiosteal abscess in these children might indicate osteomyelitis. Some findings are, however, nonspecific because US sometimes demonstrates thickening of the periosteum and slight elevation by subperiosteal fluid accumulation even in vaso-occlusive crisis. Careful correlation with biological markers, especially C-reactive protein and white blood cell count, as well as repeat US and sometimes US-guided aspiration of the fluid, are necessary to make this differential diagnosis [16].
The role of US in inflammatory conditions such as juvenile idiopathic arthritis (JIA) has been extensively documented [17,18,19] and is represented primarily by identification of changes in the joint space, synovium, cartilage and entheses, which is beyond the scope of this review. Alterations to the cortical bone surface by bony erosions can be identified with US (Fig. 8), but these are less common in young children than in adults and should not be confused with irregularities in recently ossified segments of the skeleton [20]. In adolescents, US depicts bony erosions in JIA with a similar yield to the adult population but with a lower accuracy in comparison to MRI [19].

Juvenile idiopathic arthritis (JIA) in a 9-year-old girl. a Longitudinal US view shows focal deformation of the anterior cortical surface at the metaphysis of the left distal femur, representing a bony erosion (arrows), associated with synovial thickening (*). b Longitudinal US of normal right side for comparison
Trauma
Although US is not the first-line imaging technique of choice in diagnosing pediatric fractures, it has a high sensitivity and specificity in their detection [21, 22]. Several authors advocate for a more extensive role for US in pediatric traumatology, which might reduce X-ray exposure in select cases [21,22,23,24].
Implementing US on a wide scale for detecting fractures is difficult and probably unnecessary. However, radiologists are sometimes confronted with a change in the bone surface on US in the setting of suspected or known trauma. It is therefore important to recognize US alterations in the bone surface that are indicative of fracture. These changes reflect the different types of fractures encountered in the pediatric population [25]. US can be used to identify an interruption of the cortical bone in the case of complete or greenstick fractures or simply a deformation in the bone surface in torus or plastic fractures (Fig. 9). Subperiosteal hematoma might accompany the fracture line, especially in neonates and toddlers [10] (Fig. 10).

Detection of fractures with US. a 12-month-old girl with a history of a prolonged hospital stay after liver transplantation and decreased movement of the right leg. Longitudinal US view identifies cortical interruption of the distal femur, indicating a non-displaced fracture (arrow). b A 17-month-old boy assessed for limping with no clear history of trauma. Longitudinal US of the left tibial shaft shows cortical deformation of the distal tibia (arrow), consistent with a torus fracture. c The same boy as in (b), subsequent lateral radiograph of the left ankle confirms a distal tibial torus fracture (arrow)

Subperiosteal hematoma at fracture site on US in a 5-day-old newborn girl who was not moving the left arm. Longitudinal US of the left clavicle shows interruption of the mid-clavicular shaft, confirming fracture with displacement (arrow). Subperiosteal hematoma (*) is evident at the fracture site
In cases of suspected fractures with negative radiographs, US can be a complementary tool to reveal fracture lines too fine to be detected by radiographs in the acute stage (Fig. 11). Comparative views of the opposite healthy side are often useful in cases of minimal deformation or cortical disruption.

Acute fracture in a 4-year-old boy presenting with a limp after mild trauma to his left foot. a Anteroposterior (AP) radiograph of the left foot taken the day after the trauma appears negative for fracture. b US performed the same day in longitudinal view revealed slight deformation of the anterior cortex of the 2nd, 3rd and 4th metatarsals on the left (L) side (arrow). c The normal right (R) side is presented for comparison. d Follow-up AP radiograph after 10 days confirms consolidation at suspected fracture sites (arrow)
The use of US to detect classic metaphyseal lesions (CMLs) in inflicted trauma has been described in several reports [26, 27] (Fig. 12). Although US has high specificity for CMLs, its sensitivity is rather low [27]. It therefore cannot exclude CMLs but might complement equivocal radiologic findings. Examiners should be particularly careful not to confuse CMLs with normal variations of the bone surface at the metaphyseal collar (Fig. 2) or with metaphyseal anomalies in relation to systemic metabolic diseases, such as rickets.

Classic metaphyseal lesion (CML) in a 1-month-old boy with suspected inflicted trauma. a, b Comparative longitudinal US views of the right (R) and left (L) proximal tibial metaphyses demonstrate a detached fragment at the border of the metaphyseal collar on the left side (arrow). This is consistent with a CML and highly suggestive of inflicted trauma. c Anteroposterior left tibia-fibula radiograph obtained the same day demonstrates “bucket-handle” fractures of the left proximal tibia and fibula, consistent with inflicted trauma (arrows)
In older children, US is useful in cases of repetitive traumatic injuries, such as those related to sports activities. It can be used to confirm or exclude a stress fracture and to look for signs of osteochondrosis (Fig. 13) or avulsions at tendon insertions. In cases of overuse periostitis, although the surface of the cortical bone is normal, US may identify abnormal thickening of the periosteum, without displacement (Fig. 14).

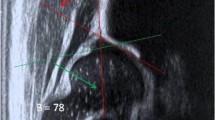
Osgood–Schlatter disease in an 11-year-old girl. a, b Comparative longitudinal views of the patellar tendon at the anterior tibial tuberosity insertion. a The cortical surface of the anterior tibial tuberosity on the right (R) side is irregular (arrowhead), reflecting fragmentation of the apophysis. This is, however, insufficient for the diagnosis because ossification centers are often fragmented or irregular; thickening of the patellar tendon (arrows) and inflammatory swelling of the subcutaneous fat (*) are key associated elements. b The normal left (L) side is presented for comparison. The diagnosis of Osgood–Schlatter disease is based on a typical clinical presentation, which may be confirmed by imaging with US and/or radiographs In cases with atypical clinical presentation, radiographs are necessary to exclude more ominous causes of pain in this region

Overuse injury in a 14-year-old boy complaining of lower limb pain after 2 weeks of intensive football training. a Longitudinal US view of the left tibial shaft shows a normal bone surface (arrowheads), thickening of the hypoechoic periosteum (arrows) and hyperechogenicity and swelling in the overlying subcutaneous tissue indicating edema (*). These findings suggest periostitis, probably due to overuse of the affected limb. b Longitudinal US of the tibial shaft on the opposite side is presented for comparison, demonstrating the normal bone surface (arrowheads), normal periosteum (barely visible) and normal soft tissues. Based on the US findings no further imaging was performed in this boy, and his symptoms resolved 2 weeks after interruption of physical activity
Mass lesions
One of the most common uses of US is to examine any kind of soft tissue bump or mass, which immediately depicts the mass and can demonstrate contact of the mass with the bone surface. Conversely, a bone tumor becomes visible with US only when it reaches and disrupts the cortex. Although not specific, US can point to the origin of the mass (bone versus soft tissues), its internal structure (solid versus liquid), vascularization and presence of periosteal reaction. As such, US provides the initial signs that indicate the need for more extensive imaging and can guide percutaneous biopsy of the mass, if required [28]. Careful correlation with radiographs will be necessary for most masses that are in contact with the bone, to allow more complete delineation of the extent of bone involvement.
Primary malignant bone tumors sometimes present as recent masses of the extremities, and in these cases, US often accompanies or precedes radiographs. The surface of the bone appears destroyed on US, irregular, with replacement of the normal bone by a vascularized solid mass (Fig. 15). US can be used to identify non-mineralized periosteal reaction as a thin, hyperechoic line, raised by the tumor [2] (Fig. 15). When the periosteal reaction becomes mineralized, US reproduces the aggressive types of periosteal reaction, such as hair-on-end, sunburst and Codman triangle, that are common on conventional radiographs (Fig. 16) [2, 29].

Primary bone tumor in a 10-year-old boy referred to the emergency room for recent painful swelling of the distal calf. US was the first examination performed and raised the suspicion of a malignant bone tumor based on the extensive destruction of the bone surface. a Panoramic US in the longitudinal plane reveals a solid mass causing irregular destruction of the normal cortical bone surface of the distal femur (*). E epiphysis M metaphysis. b Longitudinal US shows that normal bone is replaced by tumor tissue, with displaced periosteum (arrows) and rich, irregular sunburst periosteal reaction (*). c Corresponding anteroposterior radiograph of the left knee taken immediately after US shows osteolysis of the distal femoral metaphysis by an aggressive process, with sunburst periosteal reaction (arrow), consistent with osteosarcoma

Ewing sarcoma in a 7-year-old girl referred for US by her pediatrician for swelling of the forearm of several weeks’ duration. a Panoramic longitudinal US view demonstrates aggressive destruction of the proximal radius (arrowheads) by a large tumor mass (*). b Transverse US of the radial shaft shows hair-on-end periosteal reaction (arrowheads). The workup was continued with radiographs, MRI and surgical biopsy, confirming the diagnosis of Ewing sarcoma
For some bone tumors, US features may be highly characteristic, although never entirely pathognomonic. One example is Langerhans cell histiocytosis, in which 45% of bone lesions are in the skull [30]. US demonstrates a solid mass that interrupts the normal cortical bone, with regular contours and beveled edges, resulting from asymmetrical destruction of the inner and outer tables of the skull (Fig. 17) [31]. The mass is hypoechoic and homogeneous, with low vascularity on color Doppler [30] (Fig. 17). Although this US presentation is highly suggestive, it is not entirely specific. The differential diagnosis includes more aggressive lesions, such as myofibromatosis, leukemia, lymphoma and metastatic neuroblastoma [31]. In other skeletal locations, histiocytic lesions are less characteristic, and histological confirmation is almost always required (Fig. 18).

Langerhans cell histiocytosis in a 2-year-old boy. a US of swelling in the right frontal region reveals a solid mass with interruption of the inner and outer tables of the frontal bone, subperiosteal extension (*) and beveled edges (arrow). b The mass is hypovascular on color Doppler US. These findings were considered highly suggestive of Langerhans cell histiocytosis and the workup was completed with radiographs. The lesion proved to be solitary

Langerhans cell histiocytosis of the left 8th rib in a 9-year-old boy. a Longitudinal US of the rib reveals destruction at the anterior extremity, close to the chondrocostal junction, replaced by solid tissue (*), with subperiosteal extension (arrow). C cartilage, R rib. b Transverse US at the same level demonstrates persistence of a small portion of cortical bone (arrow), with the remainder being replaced by the tumor mass (*). Diagnosis was confirmed by surgical biopsy
One other common mass of the skull that must be distinguished from histiocytosis is the dermoid or epidermoid inclusion cyst. This is not a neoplasm but rather a congenital anomaly occurring in the region of the head and neck [32]. US shows a well-defined mass within the bone, with chronic deformation but no interruption of the inner table. The internal structure of the mass is also highly suggestive: hypoechoic, with small focal bright echoes and no vascularization on color Doppler (Fig. 19) [31, 33]. These US features, in conjunction with a chronic evolution and typical localization on the skull or at the outer edge of the orbit, are diagnostic of inclusion cysts and no further imaging is required.

Skull dermoid in a 4-year-old boy with a palpable chronic temporal mass. a Longitudinal US view shows a hypoechoic mass with small internal echoes. Its contours are regular, the inner table of the bone is intact (arrowhead) and there is no subperiosteal extension. b No vessels are identified within the lesion on color Doppler US
Although some US features are highly suggestive of certain types of tumors, as presented in the examples here, it is important to keep in mind the clinical context in each case. The US diagnosis requires consideration of the general and local symptoms, as well as chronology and evolution of the mass.
Conclusion
Ultrasound is a highly sensitive technique for detecting any changes in the cortical bone surface and overlying periosteum. Although some of the changes on US lack specificity, being aware of and correlating them with clinical and biological information is of real value to the diagnostic process. Because US requires no sedation and involves no ionizing radiation, it is a useful tool in children not only to examine the soft tissues, but also for the initial identification and characterization of underlying bone lesions.
References
Eide P, Djuve Ã, Myklebust R et al (2019) Prevalence of metaphyseal injury and its mimickers in otherwise healthy children under two years of age. Pediatr Radiol 49:1051–1055
Bisseret D, Kaci R, Lafage-Proust MH et al (2015) Periosteum: characteristic imaging findings with emphasis on radiologic–pathologic comparisons. Skeletal Radiol 44:321–338
Dwek JR (2010) The periosteum: what is it, where is it, and what mimics it in its absence? Skeletal Radiol 39:319–323
Moraux A, Gitto S, Bianchi S (2019) Ultrasound features of the normal and pathologic periosteum. J Ultrasound Med 38:775–784
Robben SG (2004) Ultrasonography of musculoskeletal infections in children. Eur Radiol 14:L65–77
Wenaden AET, Szyszko TA, Saifuddin A (2005) Imaging of periosteal reactions associated with focal lesions of bone. Clin Radiol 60:439–456
Chao HC, Lin SJ, Huang YC, Lin TY (1999) Color Doppler ultrasonographic evaluation of osteomyelitis in children. J Ultrasound Med 18:729–734
Riebel TW, Nasir R, Nazarenko O (1996) The value of sonography in the detection of osteomyelitis. Pediatr Radiol 26:291–297
Kaiser S, Rosenborg M (1994) Early detection of subperiosteal abscesses by ultrasonography. A means for further successful treatment in pediatric osteomyelitis. Pediatr Radiol 24:336–339
Karmazyn B (2011) Ultrasound of pediatric musculoskeletal disease: from head to toe. Semin Ultrasound CT MR 32:142–150
Azam Q, Ahmad I, Abbas M et al (2005) Ultrasound and colour Doppler sonography in acute osteomyelitis in children. Acta Orthop Belg 71:590–596
Mantsopoulos K, Wurm J, Iro H, Zenk J (2015) Role of ultrasonography in the detection of a subperiosteal abscess secondary to mastoiditis in pediatric patients. Ultrasound Med Biol 41:1612–1615
Mair MH, Geley T, Judmaier W, Gassner I (2002) Using orbital sonography to diagnose and monitor treatment of acute swelling of the eyelids in pediatric patients. AJR Am J Roentgenol 179:1529–1534
Falticeanu A, Tritschler P, Dumitriu D (2020) Ultrasound in pediatric orbital cellulitis. Med Ultrason 22:253–254
William RR, Hussein SS, Jeans WD et al (2000) A prospective study of soft-tissue ultrasonography in sickle cell disease patients with suspected osteomyelitis. Clin Radiol 55:307–310
Inusa BP, Oyewo A, Brokke F et al (2013) Dilemma in differentiating between acute osteomyelitis and bone infarction in children with sickle cell disease: the role of ultrasound. PLoS One 8:e65001
Ramos PC, Ceccarelli F, Jousse-Joulin S (2012) Role of ultrasound in the assessment of juvenile idiopathic arthritis. Rheumatology 51:vii10–12
Karmazyn B, Bowyer SL, Schmidt KM et al (2007) US findings of metacarpophalangeal joints in children with idiopathic juvenile arthritis. Pediatr Radiol 37:475–482
Sudoł-Szopińska I, Grochowska E, Gietka P et al (2016) Imaging of juvenile idiopathic arthritis. Part II: ultrasonography and MRI. J Ultrason 16:237–251
Chauvin NA, Doria AS (2017) Ultrasound imaging of synovial inflammation in juvenile idiopathic arthritis. Pediatr Radiol 47:1160–1170
Barata I, Spencer R, Suppiah A et al (2012) Emergency ultrasound in the detection of pediatric long-bone fractures. Pediatr Emerg Care 28:1154–1157
Patel DD, Blumberg SM, Crain EF (2009) The utility of bedside ultrasonography in identifying fractures and guiding fracture reduction in children. Pediatr Emerg Care 25:221–225
Herren C, Sobottke R, Ringe MJ et al (2015) Ultrasound-guided diagnosis of fractures of the distal forearm in children. Orthop Traumatol Surg Res 101:501–505
Moritz JD, Berthold LD, Soenksen SF, Alzen GF (2008) Ultrasound in diagnosis of fractures in children: unnecessary harassment or useful addition to X-ray? Ultraschall Med 29:267–274
Jadhav SP, Swischuk LE (2008) Commonly missed subtle skeletal injuries in children: a pictorial review. Emerg Radiol 15:391–398
Marine MB, Hibbard RA, Jennings SG, Karmazyn B (2019) Ultrasound findings in classic metaphyseal lesions: emphasis on the metaphyseal bone collar and zone of provisional calcification. Pediatr Radiol 49:913–921
Karmazyn B, Marine MB, Wanner MR et al (2020) Accuracy of ultrasound in the diagnosis of classic metaphyseal lesions using radiographs as the gold standard. Pediatr Radiol 50:1123–1130
Saifuddin A, Mitchell R, Burnett SJ et al (2000) Ultrasound-guided needle biopsy of primary bone tumours. J Bone Joint Surg Br 82:50–54
Saifuddin A, Burnett SJ, Mitchell R (1998) Pictorial review: ultrasonography of primary bone tumours. Clin Radiol 53:239–246
Kosiak W, Piskunowicz M, Swieton D et al (2012) Sonographic diagnosis and monitoring of localized Langerhans cell histiocytosis of the skull. J Clin Ultrasound 41:134–139
Bansal AG, Oudsema R, Masseaux JA, Rosenberg HK (2018) US of pediatric superficial masses of the head and neck. Radiographics 38:1239–1263
Smirniotopoulos JG, Chiechi MV (1995) Teratomas, dermoids and epidermoids of the head and neck. Radiographics 15:1437–1455
Riebel T, David S, Thomale UW (2008) Calvarial dermoids and epidermoids in infants and children: sonographic spectrum and follow-up. Childs Nerv Syst 24:1327–1332
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Dumitriu, D., Menten, R. & Clapuyt, P. Ultrasonography of the bone surface in children: normal and pathological findings in the bone cortex and periosteum. Pediatr Radiol 52, 1392–1403 (2022). https://doi.org/10.1007/s00247-022-05289-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-022-05289-8