
Abstract
We present a practical approach to imaging in suspected biliary atresia, an inflammatory cholangiopathy of infancy resulting in progressive fibrosis and obliteration of extrahepatic and intrahepatic bile ducts. Left untreated or with failure of the Kasai procedure, biliary atresia progresses towards biliary cirrhosis, end-stage liver failure and death by age 3. Differentiation of biliary atresia from other nonsurgical causes of neonatal cholestasis is challenging because there is no single method for diagnosing biliary atresia, and clinical, laboratory and imaging features of this disease overlap with those of other causes of neonatal cholestasis. Concerning imaging, our systematic literature review shows that ultrasonography is the main tool for pre- and neonatal diagnosis. Key prenatal features, when present, are non-visualisation of the gallbladder, cyst in the liver hilum, heterotaxy syndrome and irregular gallbladder walls. Postnatal imaging features have a very high specificity when present, but a variable sensitivity. Triangular cord sign and abnormal gallbladder have the highest sensitivity and specificity. The presence of macro- or microcyst or polysplenia syndrome is highly specific but less sensitive. The diameter of the hepatic artery and hepatic subcapsular flow are less reliable. When present in the context of acholic stools, dilated intrahepatic bile ducts rule out biliary atresia. Importantly, a normal US exam does not rule out biliary atresia. Signs of chronic hepatopathy and portal hypertension (portosystemic derivations such as patent ductus venosus, recanalised umbilical vein, splenomegaly and ascites) should be actively identified for — but are not specific for — biliary atresia.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Biliary atresia is an important cause of obstructive jaundice in infants, causing progressive fibrosis and obliteration of extrahepatic and intrahepatic bile ducts, resulting in biliary cirrhosis in the absence of early surgery. Jaundice with pale stools and dark urine are present within the first days or weeks after birth. The prevalence of biliary atresia ranges from 1 in 5,000 to 1 in 20,000 depending on the geographic area, with the highest prevalence reported in Taiwan [1,2,3]. Biliary atresia aetiology is unknown and different causes were proposed including viral infections, genetic factors or toxins [4]. There are two forms of biliary atresia: the non-syndromic form, accounting for about 80% of cases; and the syndromic form, also called biliary atresia splenic malformation syndrome, accounting for about 20% of cases. The syndromic form is associated with polysplenia, intestinal malrotation, preduodenal portal vein, absent inferior vena cava, aberrant hepatic artery and abdominal heterotaxia [5]. Whatever the form, there are different subtypes of biliary atresia according to the extent of fibrosis on extrahepatic bile ducts and the presence of a cyst of the extrahepatic bile duct. In all cases intrahepatic bile ducts are fibrotic, explaining the absence of bile duct dilatation despite complete obstruction [6] (Fig. 1). The histology is characterised by bile duct proliferation, bile plugs, portal or perilobular fibrosis, edema and preservation of the basic hepatic lobular architecture [7, 8]. Histology is not specific, and disorders such as parenteral-nutrition-associated cholestasis, cystic fibrosis and α-1-antitrypsin deficiency can mimic biliary atresia. Liver biopsy specimens obtained before 6 weeks of age might be indistinguishable from neonatal hepatitis [8,9,10]. If left untreated, children with biliary atresia die within the first years of life by complications of biliary cirrhosis and end-stage liver disease. The primary treatment is surgery, the Kasai hepatoportoenterostomy, which consists of resection of the choledochal remnants, gallbladder and portal plate and construction of a jejunal Roux-en-Y anastomosis or cholecystostomy to restore biliary drainage. If children with biliary atresia are operated within the first 60 days of age, bile flow can be established in 70% of cases; in those operated after 90 days of age, sufficient bile flow is achieved in only 20% of cases [11]. Liver transplantation is performed if Kasai hepatoportoenterostomy fails or for advanced cirrhosis. Prompt diagnosis is the main goal of imaging, considering the paramount importance of early surgical treatment, ideally between 30 days and 60 days of age. Yet, differentiation of biliary atresia from other nonsurgical causes of neonatal cholestasis is challenging. Gamma glutamyl transpeptidase is an important biomarker in the differential diagnosis of neonatal cholestasis, showing higher levels in children with biliary atresia than those without biliary atresia [12]. Ultrasound (US), MR cholangiopancreatography, hepatobiliary scintigraphy, liver percutaneous biopsy, percutaneous cholecysto-cholangiography and endoscopic retrograde cholangiopancreatography are used for biliary atresia diagnosis, but surgery with intraoperative cholangiography and biopsy is the reference standard for diagnosis. In this study, we systematically reviewed the relevant literature regarding the use of US in the diagnosis of biliary atresia and provide an accurate pooled estimate of the US diagnostic performance. We also reviewed the literature to analyze the accuracy of other imaging methods of biliary atresia. Based on this literature review and after discussions within the European Society of Paediatric Radiology (ESPR) abdominal task force, we propose a diagnostic pathway for children with suspected biliary atresia.

Different types of biliary atresia — in grey the obstructed bile ducts or gallbladder, in green the patent parts. a Complete atresia of the extrahepatic bile duct and the gallbladder. This is the most frequent type, accounting for about 2/3 of patients. b Patent gallbladder with atretic cystic duct and extrahepatic bile duct. c Patent gallbladder, cystic duct and choledochus with atretic main common bile duct. d–g Cystic forms with macrocyst at the liver hilum and variable atresia of the gallbladder and the extrahepatic bile ducts. Note that intrahepatic bile ducts are always pathological; hence, they do not display dilation. With permission from Pariente et al. [6]
Literature search
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. In December 2018 two independent authors (M.N. and M.B.D.) searched on PubMed all articles published from January 1999 to December 2018. Keywords included (triangular cord or gallbladder or ultrasound or US) AND (biliary atresia). The first selection was based on the title and abstract. Eligible articles were those reporting in the abstract, or likely in the text, true positives (TP), true negatives (TN), false positives (FP), and false negatives (FN). Eligible articles were read in full and references were hand-searched for further eligibility. Disagreement was settled by discussion and consensus. Only English articles with at least 10 biliary atresia patients using surgery as the reference standard for biliary atresia diagnosis were considered. We matched author names and affiliations to avoid data duplication, and we included only the most recent or complete study. No papers were dismissed because of children’s age.
In December 2019 two independent reviewers (M.N. and M.B.D.) searched on PubMed all articles published from January 1999 to December 2019. Keywords included (prenatal diagnosis) AND (biliary atresia). All relevant English-language papers were included.
Data were extracted by the same two readers, while discrepancies were discussed by consensus. A 2×2 contingency Table (TP, TN, FP and FN) was obtained independently for each of the US characteristics reported, and if more than one type of gallbladder abnormality was included, only the most frequent in the study was adopted for calculating data. Forest plot, summary receiver operating characteristic (sROC) curve, sensitivity, specificity, positive likelihood ratio (LR+), negative likelihood ratio (LR–) and diagnostic odds ratio (DOR) for each US sign were calculated if at least four studies were eligible. Statistical analysis was performed using R software (version 3.3.3, package metaphor in R; R Foundation for Statistical Computing, Vienna, Austria).
Review of reported findings
Prenatal diagnosis
Seventy-seven studies regarding prenatal diagnosis were identified for initial review. On the basis of title or abstract, 66 papers were excluded and 11 papers [13,14,15,16,17,18,19,20,21,22,23] were identified as relevant.
Prenatal diagnosis of biliary atresia is quite rare. Reported prenatal signs in foetuses with biliary atresia are non-visualisation of the gallbladder, cyst in the liver hilum, heterotaxy syndrome and irregular gallbladder walls [13,14,15,16,17,18,19,20, 22, 23]. Persistent non-visualisation of foetal gallbladder is rare, and 15–43% of cases with this condition have isolated gallbladder agenesis, a benign condition [22]. Persistent non-visualisation of foetal gallbladder could be associated with other abnormalities (such as renal agenesis, hydronephrosis, cerebral ventricular dilatation, chromosomal anomalies [particularly Trisomy 21], cystic fibrosis, biliary atresia and multiple malformations) [15, 22, 23]. Prenatal hepatic cysts have been reported in the context of biliary atresia. The main differential diagnosis is a choledochal cyst. Morel et al. [19] reported a case of prenatal biliary atresia characterised by irregular gallbladder wall associated with a cyst of the extrahepatic biliary tract. Prenatal differentiation between cystic biliary atresia and choledochal cyst is most often impossible because of the difficulty of showing intrahepatic bile duct dilatation (Fig. 2), which is either not yet present or not visible because of poor spatial resolution. Postnatal diagnosis is based on intrahepatic bile duct dilatation associated with choledochal cyst. US markers of left heterotaxy, especially in the presence of polysplenia, should raise the possibility of biliary atresia splenic malformation syndrome (Fig. 3). MRI is not specific but could help in visualising the gallbladder, characterising a heterotaxia syndrome and searching for bile duct dilatation in the context of cyst at the liver hilum [21].

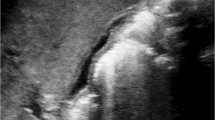
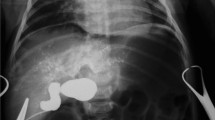
A female foetus with a cystic form of biliary atresia at 33 weeks of gestation and at 12 days old. a, b Foetal axial US with color Doppler (a) and coronal T2-weighted MR image (b; repetition time/echo time [TR/TE] 5,000/100 ms) show a macrocyst at the liver hilum (arrows) and non-visualisation of gallbladder. c Postnatal percutaneous transhepatic cysto-cholangiography shows the macrocyst (arrow) communicating with very abnormal atretic intrahepatic bile ducts, with no opacification of the extrahepatic bile duct and the duodenum, confirming the diagnosis of cystic biliary atresia

Syndromic biliary atresia in a 5-month-old girl. a Axial US image shows interrupted inferior vena cava with azygos continuation (arrow). b Sagittal US image shows polysplenia (arrows)
Neonatal ultrasound evaluation
We identified 599 studies for initial review. On the basis of title or abstract we excluded 553 papers and considered 46 papers to be relevant. After full review of the 46 articles, we found that 20 papers [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43] fulfilled all the inclusion criteria; these papers comprised 1,906 infants with an age range of 3–360 days (Table 1) [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]). The following US signs were evaluated: the triangular cord sign, gallbladder abnormalities, cysts, common bile duct visibility, hepatic subcapsular flow, hepatic artery enlargement, and polysplenia syndrome. Table 2 presents a summary of diagnostic performances of several US features in our meta-analysis [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43].
Triangular cord sign
Triangular cord sign consists of the obliterated fibrous ductal remnant and was first described by Choi [44] and further by Lee [29] and colleagues as the thickness of the echogenic anterior wall of the anterior branch of the right portal vein just distal to the right portal vein on a longitudinal image without including the right hepatic artery. Other authors evaluated for the triangular cord sign anterior to or near the bifurcation of the portal vein measured both in transverse and longitudinal scans. Triangular cord sign is usually reported positive if >3–4 mm, and the variability of its measurements is caused by the positioning of the measurement (Fig. 4). There is no consensus in the literature on how or where to measure, or on whether to include the hepatic artery. Biliary atresia is a progressive disease, as supported by Hwang et al. [45], who showed that triangular cord sign was present in 17% of infants younger than 30 days and 56% in the older group. Figure 5 shows the forest plots and sROC curve of the 19 papers using triangular cord sign for biliary atresia diagnosis included in our meta-analysis [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41, 43]. Table 2 presents the diagnostic performance of triangular cord sign, which shows the highest diagnostic odds ratio (40.2) among the signs in biliary atresia, with intermediate sensitivity (0.68) and high specificity (0.95). Only two papers included infants younger than 90 days: Tan Kendrick et al. [26] reported a triangular cord sign sensitivity of 84% and specificity of 100% (31/217 cholestatic infants with biliary atresia); Mittal et al. [37] reported that triangular cord sign has a sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of 23.3%, 97.1%, 77.8% and 74.4%, respectively (30/99 cholestatic infants with biliary atresia).

Triangular cord sign corresponding to the fibrotic transformation of the bile ducts at the site of the ductal plate in two infants. a Longitudinal US image in a 35-day-old girl shows triangular cord sign (arrow) as a hyperechoic area measured against the anterior wall of the anterior branch of the right portal vein just distal to the right portal vein without including the right hepatic artery. b Axial US image in a 59-day-old boy shows triangular cord sign (arrow) measured anterior to the bifurcation of the portal vein

Diagnostic efficacy of the triangular cord sign. a–c Forest plots for sensitivity (a), specificity (b) and summary receiver operating characteristic (SROC) curve (c) for triangular cord sign (TSC) data in our meta-analysis
Gallbladder abnormalities
Several gallbladder abnormalities associated with biliary atresia have been reported (Fig. 6):
-
absence of visibility of the gallbladder lumen (which is different from gallbladder agenesis because at surgery the fibrotic remnant of the gallbladder is found);
-
small gallbladder with a cut-off length <15–19 mm, according to different authors;
-
abnormal shape and wall of the gallbladder; and
-
no emptying of the gallbladder after feeding.

Oblique US imaging in infants with abnormal gallbladder related to biliary atresia. a Gallbladder is small with irregular margins (arrow) in a 50-day-old boy. b Hyperechoic fibrotic gallbladder with no lumen visible (star) in a 72-day-old girl. c Gallbladder (VB) has a normal size but irregular, thickened walls in a 35-day-old boy. d Gallbladder is very small, with interruption of the lumen and no wall clearly visible in a 60-day-old girl (arrow)
Figure 7 shows the forest plots and the sROC curve of the 17 papers using gallbladder abnormalities for biliary atresia diagnosis included in our meta-analysis [24,25,26,27,28, 30, 32, 33, 35,36,37,38,39,40,41,42,43]. Table 2 summarises the diagnostic performances of gallbladder abnormalities, which showed a good diagnostic odds ratio (16.5) among the signs in biliary atresia, with high sensitivity (0.79) and specificity (0.81). Figure 8 shows the forest plots and the sROC curve of the four papers included in our meta-analysis that used absence of the gallbladder for biliary atresia diagnosis [30, 36, 37, 43]. Table 2 summarises the diagnostic performance of gallbladder absence, which showed a good diagnostic odds ratio (17.5) among the signs in biliary atresia, with very low sensitivity (0.20) and very high specificity (0.98). Figure 9 shows the forest plots and the sROC curve of the four papers included in our meta-analysis that used gallbladder length abnormality for biliary atresia diagnosis [30, 33, 38, 39]. Table 2 summarises the diagnostic performances of gallbladder length, with a low diagnostic odds ratio (10.1) among the signs in biliary atresia, and with intermediate sensitivity (0.72) and good specificity (0.79).

Diagnostic efficacy of gallbladder abnormalities (GBA). a–c Forest plots for sensitivity (a), specificity (b) and summary receiver operating characteristic (SROC) curve (c)

Diagnostic efficacy of absent gallbladder (GB). a–c Forest plots for sensitivity (a), specificity (b) and summary receiver operating characteristic (SROC) curve (c)

Diagnostic efficacy of gallbladder length (GBL). a–c Forest plots for sensitivity (a), specificity (b) and summary receiver operating characteristic (SROC) curve (c)
Gallbladder abnormalities were common in infants in both biliary atresia age groups — younger and older than 30 days — without a statistically significant difference among the various abnormalities [45]. It is crucial to remember that a normal gallbladder does not rule out biliary atresia (Fig. 10). Irregular and thickened gallbladder wall might be a helpful sign for biliary atresia in infants with normal gallbladder length. Only three series [27, 30, 36] evaluated the diagnostic performance of irregular gallbladder wall as an isolated sign and reported sensitivity ranging from 0.50 to 0.91 and specificity ranging from 0.91 to 0.95. Tan Kendrick et al. [26] defined the “gallbladder ghost triad” as atretic gallbladder length (outer-to-outer wall) <1.9 cm; thinned or lack of smooth/complete echogenic mucosal lining and indistinct wall; and knobby, irregular or lobular gallbladder contour. The authors, using the search “gallbladder ghost triad” in a population younger than 90 days, found a sensitivity of 97% and a specificity of 100%. Mittal et al. [37] found in a population younger than 90 days that sensitivity, specificity, PPV and NPV of an abnormal gallbladder were 83%, 83%, 68% and 92%, respectively; for non-contractility of the gallbladder, these percentages were 87%, 73%, 51% and 94%, respectively.

Biliary atresia in a 19-day-old boy with normal-appearing gallbladder. a Oblique US shows normal aspect of the gallbladder. b Posteroanterior percutaneous cholecysto-cholangiography shows the communication of the gallbladder with the extrahepatic duct and no reflux in the intrahepatic ducts, confirming the diagnosis of biliary atresia
Combined triangular cord sign and gallbladder abnormalities
Figure 11 shows the forest plots and the sROC curve of the five studies included in our meta-analysis that used a combination of triangular cord sign and gallbladder abnormalities for biliary atresia diagnosis [24, 27, 32, 35, 37]. Table 2 summarises diagnostic performance of the combination of triangular cord sign and gallbladder abnormalities, which showed the best diagnostic odds ratio (99.0), with very high sensitivity (0.87) and specificity (0.90).

Diagnostic efficacy of triangular cord sign combined with gallbladder abnormalities (TSC+GBA). a–c Forest plots for sensitivity (a), specificity (b) and summary receiver operating characteristic (SROC) curve (c)
Cysts
Two types of cysts associated with biliary atresia were reported in the literature:
-
macrocysts along the hilar pediculum with a diameter ranging 0.5–4.0 cm [46]; and
-
microcysts located at the confluence of the intrahepatic bile ducts, at the porta hepatis, in the same area of the triangular cord sign, and a lot smaller in size (less than 0.5 cm) [47].
Macrocysts are reported in the cystic form of biliary atresia and can also be seen on prenatal diagnosis [43]. The differential diagnosis of cystic biliary atresia is a choledochal cyst; the latter is often associated with intrahepatic bile duct dilatation (Fig. 12). In an infant with acholic stools, a macrocyst at the hilar pediculum without intrahepatic bile duct dilation is almost pathognomonic of biliary atresia, according to the experience of ESPR abdominal task force members.

Cholestasis and prenatal diagnosis of cyst at the liver hilum. a, b A 54-day-old girl presents with macrocyst at the liver hilum (arrow) with no intrahepatic bile duct dilatation on oblique US Doppler (a). Posteroanterior perioperative cystography (b) confirms cystic biliary atresia with reflux of the iodine in very irregular and thin atretic intrahepatic bile ducts and no opacification of the choledochus and the duodenum. c, d A 4-day-old girl with choledochal cyst. Oblique color Doppler US shows a cyst at the liver hilum (arrow in c) communicating with dilated intrahepatic bile ducts visible in the more cranial image (d). A distance between calipers
Microcysts are located at the porta hepatis and have a small diameter ranging 2–4 mm. Because of their small size they are not visible on prenatal imaging. They can disappear during follow-up before surgery. Color Doppler is useful to differentiate microcysts from curving vessels (Fig. 13). Koob et al. [43] reported sensitivity and specificity for biliary atresia, respectively, for macrocysts (10% and 99%) and microcysts (20% and 98%) and a combination of macro- or microcysts (25% and 97%). Thus, the presence of macro- or microcysts is a sign with very high specificity and low sensitivity.

Biliary atresia with microcyst. a Oblique color Doppler US shows a microcyst within a triangular cord sign (arrow) and no bile duct dilatation in a 30-day-old girl. b Oblique color Doppler US shows a microcyst (arrow) with no triangular cord sign and intrahepatic bile duct dilation in a 37-day-old boy
Common bile duct visibility
Absent visibility of the extrahepatic bile duct has been proposed as a criterion for the diagnosis of biliary atresia, especially in MR studies. Only three series used absent extrahepatic bile duct visibility for biliary atresia diagnosis [30, 31, 37] and reported a sensitivity ranging from 0.93 to 0.95 and a large specificity range from 0.48 to 0.92. The visibility of part of the extrahepatic bile duct, whatever its diameter, does not rule out biliary atresia. The difficulty is to see the whole extrahepatic biliary tree from the right and left branches to the distal common bile duct.
Hepatic subcapsular flow
Analysis of hepatic subcapsular flow in infants with biliary atresia using color Doppler sonography can detect hyperplastic and hypertrophic changes in branches of the hepatic artery (Fig. 14) and this phenomenon has been proposed as a diagnostic criterion for biliary atresia. Only three papers using hepatic subcapsular flow for biliary atresia diagnosis were included in this review [33, 38, 39], and they reported sensitivities and specificities ranging from 0.96 to 1.00 and from 0.86 to 0.97, respectively. Reproducibility is a limiting factor because different US vendors, probes, Doppler settings and presets were used. There is no clear quantification available to allow for comparison of patients and objective follow-up.

Subcapsular flow in a 61-day-old boy with biliary atresia. Oblique color Doppler US shows hepatic arterial flow (arrows) extending to the hepatic surface
Hepatic artery diameter
The hepatic artery diameter is larger in children with biliary atresia compared to normal controls or children with hepatitis [31] from decreased portal flow secondary to developing cirrhosis. Biliary atresia is a progressive disease and hepatic artery diameter was significantly smaller in the biliary atresia group younger than 30 days [45]. Kim et al. [31] reported a range of diameters of the normal hepatic artery to be 1.0–1.4 mm. We have to underline the difficulty of correctly measuring these small vessels at this age, and the necessity for assuring a proper and not an oblique section and for using high-frequency probes with high resolution. Figure 15 shows the forest plots and the sROC curve of the four studies included in our meta-analysis that used hepatic artery diameter for biliary atresia diagnosis [31, 37,38,39]. Table 2 summarises the diagnostic performances of hepatic artery enlargement, including a low diagnostic odds ratio (12.8), with good sensitivity (0.82) and low specificity (0.70) for biliary atresia. Three series used hepatic artery diameter–to–portal vein diameter ratio >0.45 for biliary atresia diagnosis [25, 31, 33] and reported a sensitivity ranging from 0.67 to 0.77 and a large specificity range from 0.46 to 0.79.

Diagnostic efficacy of hepatic artery (HA) enlargement. a–c Forest plots for sensitivity (a), specificity (b) and summary receiver operating characteristic (SROC) curve (c)
Polysplenia syndrome
The syndromic form of biliary atresia is associated with polysplenia, intestinal malrotation, preduodenal portal vein, absent or interrupted inferior vena cava, aberrant hepatic artery and abdominal heterotaxia. Humphrey and Stringer [30] and Koob et al. [43] reported that elements of the polysplenia syndrome in the setting of cholestasis had a low sensitivity but a high specificity for biliary atresia diagnosis. Humphrey and Stringer [30] reported a sensitivity of 10% and a specificity of 100% for polysplenia and a sensitivity of 17% and a specificity of 100% for associated interrupted inferior vena cava. Koob et al. [43] reported a specificity of 99–100% for polysplenia syndrome elements and a sensitivity of 11% for polysplenia, 5% for abnormal situs, 7% for azygos continuation and 5% for preduodenal portal vein.
Liver stiffness
Liver US elastography allows for quantitative assessments of liver stiffness using, depending to the technique, either shear wave speed measurement in metres per second (m/s) or stiffness in kilopascals (kPa). We included four papers that used elastography for biliary atresia diagnosis [48,49,50,51] with sensitivity ranging from 0.81 to 0.97 and specificity ranging from 0.67 to 1.00. In these reports, liver shear wave speed measurements or liver stiffness measurements were significantly higher in infants with biliary atresia when compared to infants with other causes of cholestatic jaundice. However, there was a large overlap of the values in the two groups. In one study, grey-scale US was reported to have better diagnostic performance for biliary atresia than elastography [48]. In another paper [50], shear wave elastography not only helped differentiate biliary atresia from cholestatic hepatic diseases but also increased the diagnostic specificity when combined with grey-scale US. Elastography improved the diagnostic performance on prognosis assessment, especially in infants >30 days (Fig. 16) (Dabadie expert presentation ESPR 2018). Still there was no cut-off value to differentiate cirrhosis caused by biliary atresia from other causes of cirrhosis. A normal elastography does not rule out biliary atresia.

A 12-day-old girl born preterm with pale stools with biliary atresia. a Oblique color Doppler US shows triangular cord sign and microcyst (arrow). b Oblique hepatic shear wave elastography measurements at diagnosis are in the normal range. c Oblique splenic shear wave elastography measurements at diagnosis are in the normal range. d Two years later in the same girl, after a successful Kasai hepatoportoenterostomy, oblique shear wave elastography liver measurements show normal values in relation with an exceptional excellent outcome with the absence of liver fibrosis
Discussion
Based on our systematic review, we confirm that US signs are very useful for biliary atresia diagnosis. When assessing infants for biliary atresia we suggest using microconvex and linear US probes with the highest frequency applicable to achieve the best spatial resolution.
Among the potential US signs, triangular cord sign showed the highest diagnostic odds ratio (40.2) among the signs in biliary atresia, with intermediate sensitivity (0.68) and high specificity (0.95). Gallbladder abnormalities showed a good diagnostic odds ratio (16.5), with high sensitivity (0.79) and specificity (0.81). Absence of the gallbladder showed a good diagnostic odds ratio (17.5) with very low sensitivity (0.20) and the highest specificity (0.98), so this sign is not frequent but is highly suggestive of biliary atresia. Gallbladder length showed a low diagnostic odds ratio (10.1) with intermediate sensitivity (0.72) and good specificity (0.79). A combination of triangular cord sign and gallbladder abnormalities had the best diagnostic odds ratio (99.0), with the highest sensitivity (0.87) and very high specificity (0.90), and is very suggestive of biliary atresia. Hepatic artery enlargement had a low diagnostic odds ratio (12.8) with low specificity (0.70) and a sensitivity of 0.82. Macro- or microcysts or a combination was a very specific sign but had a low sensitivity. Polysplenia syndrome elements had very high specificity but low sensitivity.
Zhou [52] and Yoon [53] and colleagues’ meta-analyses also included papers that used surgery or liver biopsy as a reference standard for biliary atresia. Our results are not so different from Zhou et al.’s [52] regarding triangular cord sign, gallbladder abnormalities, triangular cord sign + gallbladder abnormalities, and hepatic artery enlargement. Yoon et al.’s [53] meta-analysis evaluated only triangular cord sign and reported higher values for sensitivity and specificity. Table 3 compares the results of our meta-analysis with those of Yoon and Zhou and colleagues.
The results of our meta-analysis are in accordance with the European Society for Paediatric Gastroenterology, Hepatology & Nutrition (ESPGHAN) and the North American Society for Pediatric Gastroenterology, Hepatology & Nutrition (NASPGHAN) guidelines [54]:
-
Postnatal US is useful to exclude choledochal cyst, intrahepatic bile duct dilatation and gallstones.
-
Postnatal US is useful to demonstrate features suggestive but not diagnostic of biliary atresia and a normal US does not rule out biliary atresia.
-
The US features suggestive of biliary atresia are: (1) triangular cord sign, (2) gallbladder abnormalities and (3) micro- or macrocysts and malformations related to polysplenia syndrome.
-
The US features that do not seem reliable for suggesting biliary atresia are: (4) hepatic subcapsular flow, (5) hepatic artery enlargement and (6) non-visualisation of common bile duct.
Signs of portal hypertension (portosystemic derivations such as patent ductus venosus, recanalised umbilical vein, splenomegaly and ascites) should be actively searched for but are not specific for biliary atresia.
According to the limited number of papers available, further evaluation is necessary to assess the role of liver elastography for biliary atresia diagnosis and prognosis [48,49,50,51].
In Table 4, we propose a standardised US report in infants evaluated for cholestasis.
Our study has several limitations. The papers included showed a patient age range of 3–360 days, which is very large for an evolutive pathology that must be diagnosed as early as possible, and it creates a bias because some US signs (triangular cord sign and hilar cysts) are age-dependent. Only two papers [26, 37] included infants younger than 90 days and four papers [38,39,40, 42] did not report the age range of patients. The criteria used to define a positive triangular cord sign or gallbladder abnormalities differed across studies. Patient characteristics among studies were different; for example, some included cystic biliary atresia and some excluded cystic biliary atresia. There was a heterogeneity of study design: nine papers were prospective [24,25,26, 28, 30, 31, 37,38,39] and the remainder were retrospective [27, 29, 32,33,34,35,36, 40,41,42,43]. We included only English-language papers with surgery used as a reference standard for biliary atresia and with at least 10 patients, which excluded some types of publications.
Conclusion
Early diagnosis is challenging but is the main goal of imaging in suspected biliary atresia and is of paramount importance for a favourable outcome. Biliary atresia is a progressive disease; hence, our presented numbers are not absolute but rather an indication of the sensitivity and specificity of the various signs because the literature is inhomogeneous, both in terms of age-span and of definitions of the different pathological signs. US is a major imaging tool for biliary atresia and US signs have a high specificity, especially when associated with one another. They include triangular cord sign, gallbladder abnormalities, and macro- and microcysts and malformations related to polysplenia syndrome. However, a normal US examination does not rule out biliary atresia diagnosis.
Change history
24 December 2020
A Correction to this paper has been published: <ExternalRef><RefSource>https://doi.org/10.1007/s00247-020-04936-2</RefSource><RefTarget Address="10.1007/s00247-020-04936-2" TargetType="DOI"/></ExternalRef>
References
The NS, Honein MA, Caton AR et al (2007) Risk factors for isolated biliary atresia, National Birth Defects Prevention Study, 1997–2002. Am J Med Genet A 143A:2274–2284
Schreiber RA, Barker CC, Roberts EA et al (2007) Biliary atresia: the Canadian experience. J Pediatr 151:659–665
McKiernan PJ, Baker AJ, Kelly DA (2000) The frequency and outcome of biliary atresia in the UK and Ireland. Lancet 355:25–29
Sokol RJ, Mack C (2001) Etiopathogenesis of biliary atresia. Semin Liver Dis 21:517–524
Schwarz KB, Haber BH, Rosenthal P et al (2013) Extrahepatic anomalies in infants with biliary atresia: results of a large prospective North American multicenter study. Hepatology 58:1724–1731
Pariente D, Franchi-Abella S (2012) [Pathology of the child’s bile ducts]. EMC – Radiologie et imagerie médicale: Abdominale - Digestive 7:1–17
Balistreri WF (1985) Neonatal cholestasis. J Pediatr 106:171–184
Morotti RA, Dhanpat J (2013) Pediatric cholestatic disorders. Approach to pathologic diagnosis. Surg Pathol Clin 6:205–225
Russo P, Magee JC, Boitnott J et al (2011) Design and validation of the biliary atresia research consortium histologic assessment system for cholestasis in infancy. Clin Gastroenterol Hepatol 9:357–362
Rastogi A, Krishnani N, Yachha SK et al (2009) Histopathological features and accuracy for diagnosing biliary atresia by prelaparotomy liver biopsy in developing countries. J Gastroenterol Hepatol 24:97–102
Balistreri WF, Bezerra JA (2006) Whatever happened to “neonatal hepatitis”? Clin Liver Dis 10:27–53
Chen X, Dong R, Shen Z et al (2016) Value of gamma-glutamyl transpeptidase for diagnosis of biliary atresia by correlation with age. J Pediatr Gastroenterol Nutr 63:370–373
Di Pasquo E, Kuleva M, Rousseau A et al (2019) Outcome of non-visualization of fetal gallbladder on second-trimester US: cohort study and systematic review of literature. Ultrasound Obstet Gynecol 54:582–588
Koukoura O, Kelesidou V, Delianidou M et al (2019) Prenatal sonographic diagnosis of biliary tract malformations. J Clin Ultrasound 47:292–297
Shen O, Sela HY, Nagar H et al (2017) Prenatal diagnosis of biliary atresia: a case series. Early Hum Dev 11:16–19
Ruiz A, Robles A, Salva F et al (2017) Prenatal nonvisualization of the gallbladder: a diagnostic and prognostic dilemma. Fetal Diagn Ther 42:150–152
Bardin R, Ashwal E, Davidov B et al (2016) Nonvisualization of the fetal gallbladder: can levels of gamma-glutamyl transpeptidase in amniotic fluid predict fetal prognosis? Fetal Diagn Ther 39:50–55
Berger Y, Superina RA, Zbar A et al (2015) A case series of congenital hepatic hilar cyst: recommendations for diagnosis and management. Isr Med Assoc J 17:32–36
Morel B, Kolanska K, Dhombres F et al (2015) Prenatal ultrasound diagnosis of cystic biliary atresia. Clin Case Rep 3:1050–1051
Cong X, Sun X, Liu S (2015) Evaluation and screening ultrasonic signs in the diagnosis of fetal biliary cystic malformation. J Matern Fetal Neonatal Med 28:2100–2105
Nori M, Venkateshwarlu J, Vijaysekhar, Prasad GR (2013) Extrahepatic biliary atresia with choledochal cyst: prenatal MRI predicted and post natally confirmed: a case report. Indian J Radiol Imaging 23:238–242
Shen O, Rabinowitz R, Yagel S, Gal M (2011) Absent gallbladder on fetal ultrasound: prenatal findings and postnatal outcome. Ultrasound Obstet Gynecol 37:673–677
Boughanim M, Benachi A, Dreux S et al (2008) Nonvisualization of the fetal gallbladder by second-trimester US scan: strategy of clinical management based on four examples. Prenat Diagn 28:46–48
Park WH, Choi SO, Lee HJ (1999) The ultrasonographic ‘triangular cord’ coupled with gallbladder images in the diagnostic prediction of biliary atresia from infantile intrahepatic cholestasis. J Pediatr Surg 34:1706–1710
Kotb MA, Kotb A, Sheba MF et al (2001) Evaluation of the triangular cord sign in the diagnosis of biliary atresia. Pediatrics 108:416–420
Tan Kendrick AP, Phua KB, Ooi BC, Tan CE (2003) Biliary atresia: making the diagnosis by the gallbladder ghost triad. Pediatr Radiol 33:311–315
Visrutaratna P, Wongsawasdi L, Lerttumnongtum P et al (2003) Triangular cord sign and US features of the gall bladder in infants with biliary atresia. Australas Radiol 47:252–256
Kanegawa K, Akasaka Y, Kitamura E et al (2003) Sonographic diagnosis of biliary atresia in pediatric patients using the “triangular cord” sign versus gallbladder length and contraction. AJR Am J Roentgenol 181:1387–1390
Lee HJ, Lee SM, Park WH, Choi SO (2003) Objective criteria of triangular cord sign in biliary atresia on US scans. Radiology 229:395–400
Humphrey TM, Stringer MD (2007) Biliary atresia: US diagnosis. Radiology 244:845–851
Kim WS, Cheon J-E, Youn BJ et al (2007) Hepatic arterial diameter measured with US: adjunct for US diagnosis of biliary atresia. Radiology 245:549–555
Takamizawa S, Zaima A, Muraji T et al (2007) Can biliary atresia be diagnosed by ultrasonography alone? J Pediatr Surg 42:2093–2096
Lee MS, Kim MJ, Lee MJ et al (2009) Biliary atresia: color Doppler US findings in neonates and infants. Radiology 252:282–289
Imanieh MH, Dehghani SM, Bagheri MH et al (2010) Triangular cord sign in detection of biliary atresia: is it a valuable sign? Dig Dis Sci 55:172–175
Sun Y, Zheng S, Qian Q (2011) Ultrasonographic evaluation in the differential diagnosis of biliary atresia and infantile hepatitis syndrome. Pediatr Surg Int 27:675–679
Aziz S, Wild Y, Rosenthal P, Goldstein RB (2011) Pseudo gallbladder sign in biliary atresia — an imaging pitfall. Pediatr Radiol 41:620–626
Mittal V, Saxena AK, Sodhi KS et al (2011) Role of abdominal sonography in the preoperative diagnosis of extrahepatic biliary atresia in infants younger than 90 days. AJR Am J Roentgenol 196:W438–W445
El-Guindi MA, Sira MM, Konsowa HA et al (2013) Value of hepatic subcapsular flow by color Doppler ultrasonography in the diagnosis of biliary atresia. J Gastroenterol Hepatol 28:867–872
El-Guindi MA, Sira MM, Sira AM et al (2014) Design and validation of a diagnostic score for biliary atresia. J Hepatol 61:116–123
Hanquinet S, Courvoisier DS, Rougemont AL et al (2015) Contribution of acoustic radiation force impulse (ARFI) elastography to the US diagnosis of biliary atresia. Pediatr Radiol 45:1489–1495
Lee SM, Cheon JE, Choi YH et al (2015) Ultrasonographic diagnosis of biliary atresia based on a decision-making tree model. Korean J Radiol 16:1364–1372
Ağın M, Tümgör G, Alkan M et al (2016) Clues to the diagnosis of biliary atresia in neonatal cholestasis. Turk J Gastroenterol 27:37–41
Koob M, Pariente D, Habes D et al (2017) The porta hepatis microcyst: an additional sonographic sign for the diagnosis of biliary atresia. Eur Radiol 27:1812–1821
Choi SO, Park WH, Lee HJ, Woo SK (1996) Triangular cord: a sonographic finding applicable in the diagnosis of biliary atresia. J Pediatr Surg 31:363–366
Hwang SM, Jeon TY, Yoo SY et al (2018) US findings of biliary atresia in infants younger than 30 days. Eur Radiol 28:1771–1777
Caponcelli E, Knisely AS, Davenport M (2008) Cystic biliary atresia: an etiologic and prognostic subgroup. J Pediatr Surg 43:1619–1624
Kim MJ, Park YN, Han SJ et al (2000) Biliary atresia in neonates and infants: triangular area of high signal intensity in the porta hepatis at T2-weighted MR cholangiography with US and histopathologic correlation. Radiology 215:395–401
Zhou LY, Jiang H, Shan QY et al (2017) Liver stiffness measurements with supersonic shear wave elastography in the diagnosis of biliary atresia: a comparative study with grey-scale US. Eur Radiol 27:3474–3484
Wang X, Qian L, Jia L et al (2016) Utility of shear wave elastography for differentiating biliary atresia from infantile hepatitis syndrome. J Ultrasound Med 35:1475–1479
Duan X, Peng Y, Liu W et al (2019) Does supersonic shear wave elastography help differentiate biliary atresia from other causes of cholestatic hepatitis in infants less than 90 days old? Compared with grey-scale US. Biomed Res Int 2019:9036362
Dillman JR, DiPaola FW, Smith SJ et al (2019) Prospective assessment of ultrasound shear wave elastography for discriminating biliary atresia from other causes of neonatal cholestasis. J Pediatr 212:60–65
Zhou L, Shan Q, Tian W et al (2016) Ultrasound for the diagnosis of biliary atresia: a meta-analysis. AJR Am J Roentgenol 206:W73–W82
Yoon HM, Suh CH, Kim JR et al (2017) Diagnostic performance of sonographic features in patients with biliary atresia: a systematic review and meta-analysis. J Ultrasound Med 36:2027–2038
Fawaz R, Baumann U, Ekong U et al (2017) Guideline for the evaluation of cholestatic jaundice in infants: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric [sic] Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr 64:154–168
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Napolitano, M., Franchi-Abella, S., Damasio, M.B. et al. Practical approach to imaging diagnosis of biliary atresia, Part 1: prenatal ultrasound and magnetic resonance imaging, and postnatal ultrasound. Pediatr Radiol 51, 314–331 (2021). https://doi.org/10.1007/s00247-020-04840-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-020-04840-9