
Abstract
Mastering pediatric echocardiography (PE) requires a substantial knowledge base of echo theory and congenital heart disease (CHD), along with technical proficiency. Online self-directed learning has become increasingly utilized among medical trainees to promote competency within medical subspecialties. We sought to evaluate the impact of online learning combined with lecture-based and hands-on teaching on the acquisition of PE knowledge and confidence in pediatric cardiology and pediatric critical care fellows. We prospectively enrolled 124 learners from 2016 to 2019. These included 40 incoming cardiology and critical care fellows at Texas Children’s Hospital (TCH) as well as 84 national and international participants recruited from our online echo education website. All participants completed online learning modules through our website (www.pedecho.org), which covers pediatric echo physics, Doppler, technique, normal anatomy, atrial septal defects, and ventricular septal defects. TCH cardiology and critical care fellows subsequently participated in an Echo Boot Camp (BC), a 3-day training program with hands-on workshops and didactic lectures. Knowledge was assessed using an 80-question pre and post-test multiple choice exams. The online learning group demonstrated improvement in exam scores following online learning (PRE 49.1 ± 15.3 vs. POST 67.8 ± 17%; p ≤ 0.01). Echo Boot Camp fellows were noted to have further incremental improvement in test scores following BC (PRE 48% ± 13% vs. POST MODULE 68.6% ± 15% vs. POST BC 75.7% ± 13%; p ≤ 0.01). Self-assessment regarding confidence in context areas showed a substantial gain in self perceived interpretive confidence across all groups as well as procedural confidence in BC participants. Online learning significantly promotes the acquisition of echocardiography knowledge. Additional lecture-based and hands-on teaching in the form of an Echo Boot Camp can further enhance knowledge and interpretative skills. Both of these learning platforms appear to work in concert as powerful and effective tools in fellow education.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pediatric cardiology had its origins as a distinct field in the 1940s [1]. Despite almost 60 years of experience in training cardiology fellows, there is a paucity of literature with regard to the training of pediatric cardiology fellows [1]. Echocardiography has become the gold standard for non-invasive assessment of congenital and acquired heart disease in the pediatric population [1,2,3]. Within echocardiography, there are two core skill sets which must be mastered: procedural technique and interpretive skill.
Procedural technique is the “act” of performing an echocardiogram and obtaining all of the relevant imaging views. Interpretive skill involves having an understanding of all of the relevant anatomy and physiology obtained from each image and cognitively applying the information to formulate a medically sound diagnosis. Competence in both procedural and interpretive echocardiography is essential to the practice of pediatric cardiology [3]. Echocardiography is an operator-dependent imaging technique and requires a high level of competence in these technical and interpretive skills to maximize diagnostic accuracy [4]. Delayed or inaccurate diagnoses can place children with congenital heart disease at risk for adverse outcomes [5].
On average, cardiology fellows experience 4–6 months of dedicated echocardiography training during a standard 3-year fellowship [3]. Much of this time is spent learning the procedural side of echocardiography. Often, cardiology fellows obtain much of their exposure to interpretive echocardiography during on-call duty when they perform echocardiograms required on nights and weekends. However, changes in training schedules and work-hour restrictions have introduced new challenges into the training of fellows in echocardiography [1].
The current assessment of competency relies heavily on subjective assessments typically performed by faculty overseeing the fellows’ clinical performance. A more objective evaluation would be very beneficial to the fellows and allow faculty to provide a comprehensive, data-derived assessment of performance [6, 7]. Objective testing is advocated by specialty boarding agencies [7,8,9]. There are currently no established objective tools for evaluating trainees’ progress and performance in PE [9,10,11]. More objective measures would enhance: (a) fellows’ self-assessment in mastering essential knowledge and skills in echocardiography; and (b) faculty’s capability of assessing learner performance and the overall impact of the pediatric cardiology curriculum [8]. Among the few pediatric cardiology training programs that have implemented objective online echocardiography testing, improvement in trainee performance on the American Board of Pediatrics examination has been documented [8].
Recently, the TCH Pediatric Cardiology Fellowship Program introduced a pediatric echocardiography “Boot Camp” in an effort to reduce training inconsistencies. This training is designed for incoming first-year pediatric cardiology fellows and was expanded to critical care fellows. It provides expanded exposure to the procedural side of pediatric echocardiography; results to date indicate improved competency in procedural echocardiography [1]. While boot camp places an emphasis on procedural skills, a solid foundation in interpretive echocardiography is of equal importance.
A growing body of literature suggests that the traditional model of exclusively lecture-based education is less effective and less appealing to millennial learners with many learners seeing e-learning and simulation as an important compliment. Many favor a blended learning strategy [10,11,12,13]. E-learning has the advantage of offering learners the opportunity to have control over content, learning sequence, pace, time, and often media, allowing the learner to tailor the educational experience to meet their personal learning objectives [12]. It offers advantages over face to face learning as it can be done in an environment and time interval which suits the learner [14]. It allows for long-distance, multimedia, module-based sessions which can be utilized independently by an unlimited number of users and can even reach previously underserved populations [15]. This educational method is particularly useful in cardiology where images such as echocardiograms and angiograms are widely used [14]. Studies have shown that multimedia learning improves procedural knowledge [16, 17]. Online learning modules have also been shown to be effective in improving knowledge about common cardiac conditions [14]. Most importantly, online education may establish a stimulus for translation of medical knowledge into daily clinical practice [18].
Pediatric cardiologists at TCH have developed an online curriculum designed to improve competency in interpretive echocardiography and reduce errors. It complements the previous introductory training program which was focused more on procedural echocardiography. We sought to evaluate the incremental impact of online learning in combination with lecture-based learning and hands-on teaching on the acquisition of echocardiography knowledge and interpretative skills in incoming pediatric cardiology and critical care fellows. We hypothesize that an interactive, online instructional resource with learning modules will be an effective educational tool in improving short and medium-term retention of knowledge in pediatric echocardiography. We also hypothesize that there will be an additive effect of boot camp in reinforcing these interpretive skills with the additional benefit of reinforcing procedural skills required to perform a pediatric echocardiogram.
Methods
Online Learning Modules
In February 2016, TCH launched an instructional website (www.pedecho.org), an online learning platform developed by pediatric cardiologists for learners in pediatric echocardiography.
The educational website consisted of the following:
-
(A)
An initial 80-question multiple choice pre-test to assess users’ baseline level of knowledge.
-
(B)
A series of three comprehensive interactive learning modules covering the following topics: normal cardiac anatomy (which included a basic introduction to ultrasound physics and Doppler), atrial septal defects and ventricular septal defects. The learning modules consisted of written learning content, along with numerous echocardiographic videos and still images to illustrate the relevant anatomy and Doppler patterns along with image/video captions.
-
(C)
A final post-test to determine what knowledge users had acquired from the learning modules
We prospectively enrolled first-year pediatric cardiology and critical care fellows (fellows having completed standard critical care training now undergoing an additional year of training in cardiac ICU) at TCH from 2016 to 2019. All fellows completed the three online learning modules. Fellows were given one month to complete the learning modules and pre-test prior to the start of fellowship training. In addition, 84 additional online learners from around the world without prior cardiology experience participated in the online learning modules and testing. These learners were categorized using a detailed demographics questionnaire and served as part of the online learning group. Exclusion criteria included any online learner or fellow with prior cardiology experience or any learner who did not complete the modules and testing.
Outcome measures included an 80-question multiple choice exam administered prior to the online modules and following completion of the online modules as well as a self-assessment questionnaire. TCH cardiology and critical care fellows also underwent a cardiology echo boot camp. These individuals took a second post-test within 24 h following the completion of boot camp. In addition, a small subset of these fellows underwent a hands-on testing session in which they were scored on 21 echocardiographic objectives.
Boot Camp
At the beginning of fellowship, TCH Cardiology and first-year cardiac ICU fellows participated in an Echo Boot Camp, a 3-day training program with hands-on workshops and didactic lectures. There were a total of 15 sessions throughout boot camp. Five of these sessions were lecture-based and 10 were hands-on echocardiography scanning sessions. Lecture-based sessions consisted of the following:
-
(1)
Basic anatomy: Detailed overview of normal cardiac anatomy, nomenclature with pathology correlates.
-
(2)
Echo physics/knobology: An introduction to ultrasound reviewing basic concepts such as frequency, wavelength, sound propagation in various mediums, principles and types of Doppler, features and settings on an echocardiography machine, and how these principles relate to image acquisition and optimization.
-
(3)
Multimedia echo planes: 2-h session reviewing the normal echo imaging planes using a model patient (scanned by a pediatric cardiologist). Simultaneous PowerPoint illustrations are used to depict and label relevant normal anatomy from each echo view while live images are obtained.
-
(4)
Ventricular function: Introduction to the assessment of ventricular systolic function using echo-based quantification techniques (M-mode with shortening fraction and ejection fraction with bullet and Simpson’s biplane method for the left ventricle and fractional area change and TAPSE for the right ventricle). Echocardiographic correlates are utilized to provide appropriate examples for assessment of normal ventricular function and ventricular dysfunction.
-
(5)
Fundamentals of Doppler: Introduction to the basic principles of color and spectral Doppler with an overview of Doppler patterns in the normal heart while comparing and contrasting these normal Doppler patterns with abnormal Doppler patterns that occur in common congenital heart disease lesions.
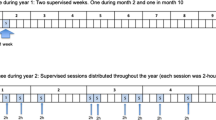
With the exception of one educational session (2-h session reviewing echo imaging planes using a live model), all educational sessions were one hour in duration. All lectures were given by cardiology faculty members or advanced imaging fellows. All hands-on sessions were proctored by cardiac sonographers, cardiology faculty or senior fellows (3rd year and advanced imaging fellows) from TCH. The hands-on sessions took place in dedicated echocardiography rooms within the cardiology clinic and cardiovascular clinic research core. Echocardiograms were performed with the use of GE Healthcare Vivid 7 and E9, Philips IE33 and Siemens ACUSON Sequoia C512 ultrasound machines. The details of the structure of boot camp is provided in Fig. 1.

Pediatric echocardiography boot camp curriculum. White boxes represent didactic and interactive lectures. Shaded boxes represent hands-on echocardiography scanning sessions
Boot Camp Assessment
Prior to the start of boot camp, all fellows completed three online learning modules as well as pre and post-tests. Fellows were provided access to the learning modules 1 month prior to the start of boot camp. Following boot camp, all fellows (cardiology and critical care) took a second identical online post-test within 24 h of completion of boot camp. Consideration was given during the boot camp lectures to providing introductory education to basic echocardiography concepts without teaching directly to the online examination or specific test questions. The pediatric cardiology fellows (n = 24) also underwent a hands-on testing session proctored by a pediatric cardiologist using a model patient in which fellows were required to assess 21 echocardiographic objectives, graded on a seven-point scale (1 = minimum, 4 = satisfactory, 7 = proficient). Objectives included the attainment of standard echocardiographic views, assessment of valvar pathology, systolic function by various methods, assessment for arch obstruction and assessment for pericardial effusion consistent with similar assessments previously performed by Maskatia et al. at our institution [1]. Testing was performed on preselected model patients with normal cardiac anatomy and excellent acoustic windows (critical care fellows were excluded from this hands-on testing session). Cardiology fellows were assessed by a single observer with expertise in training fellows in echocardiography (C.A.A, T.R.S., or J.A.K.). The goal was to assess all fellows on all 21 objectives, but in cases of technical limitations and time constraints, some objectives may not have been completely evaluated and a score was not assigned.
Data Analysis
We compared pre and post-test scores for the online learning modules in the boot camp fellows and the online learning populations. For boot camp fellows, we compared their pre boot camp learning module test scores (pre and post module) as well as test scores following boot camp (second post-test following boot camp). For fellows undergoing hands-on testing the assigned scores were evaluated. Self-assessment scores were evaluated to assess learner confidence levels (using a 7-point Likert scale). Wilcoxon signed-rank and Friedman tests were used for analysis.
Results
A total of 124 learners participated in this study. Of this cohort, 84 were exclusively online learners. The learning cohort consisted of incoming first-year cardiology fellows (n = 53), residents (n = 31), medical students (n = 6) and individuals stating they had no prior cardiology training (n = 34). 40 fellows from this cohort (23 cardiology and 17 critical care fellows) also participated in an echo boot camp and underwent additional testing and self-assessment (Fig. 2).

Pie Chart depicting online learning cohort and boot camp cohort and respective subgroups within each cohort
The mean pre-test score for the boot camp group was 48.2% ± 13.1% with an average post module test score of 68.5% ± 14.8%. The mean post boot camp test score was 75.7% ± 13.3%. The boot camp group demonstrated significant improvement in test scores following completion of the online modules (p < 0.01) with an additional incremental improvement following boot camp (p < 0.01) (Fig. 3). On self-assessment, boot camp fellows reported increased confidence scores in interpretive competency of normal anatomy prior to and following learning modules with an incremental improvement following boot camp. In addition, boot camp fellows reported increased confidence scores in perceived procedural competency following boot camp (Fig. 4).

Boot camp cohort exam scores. The figure demonstrates an improvement in test scores following online learning modules as well as further incremental improvement in test scores following boot camp. Standard deviation bars are included. All p values were ≤ 0.01

Boot camp cohort confidence scores. Panel a demonstrates confidence scores in interpreting a normal echocardiogram prior to, following the online learning modules and following echo boot camp. The subsequent panel b depicts confidence scores in performing a normal echocardiogram prior to and following boot camp. Confidence scores were expressed using a 7-point Likert scale. All p values for both figures were ≤ 0.01
Online learners (n = 124) had a mean pre-test score of 49.1% ± 15.3%. Interval improvement following completion of the learning modules was noted in the online learning group, with an average post-test score of 67.8% ± 17.4% (p < 0.01). All subgroups within the online learning group demonstrated a statistically significant (p < 0.01) improvement in exam scores following online learning. Confidence scores revealed a significant increase in interpretive confidence across all subgroups with an initial mean score for the entire cohort of 2.7 and a final mean score of 4.3 (Fig. 5).

Online learning cohort exam and confidence scores. Panel a demonstrates pre and post-test scores for the online learning cohort and subgroups within that group. The subsequent panel b depicts confidence scores in interpreting a normal echocardiogram prior to and following the online learning modules for the online learning cohort and subgroups within that group. Confidence scores were expressed using a 7-point Likert scale. All p values for both figures were ≤ 0.01
A subset of cardiology fellows (n = 24) also underwent hands-on testing following completion of boot camp. Fellows were graded on a seven-point Likert scale for 21 separate objectives. In 12/21 objectives, ≥ 75% of fellows obtained a satisfactory score (defined as a score ≥ 4) or greater. The lowest objective scores were noted in the assessment of ejection fraction (Simpson’s and bullet), assessment of pulmonary veins, use of gain/time-gain compensation and use of focal zone (Table 1).
Discussion
The mastery of echocardiography is a complex skill set which requires interpretive and procedural knowledge. It requires a detailed comprehension of normal anatomy and physiology as well as an understanding of ultrasound physics [1]. It also requires the development and reinforcement of fine motor manipulations in order to maneuver the echocardiographic probe and acquire the necessary images [1].
Our study demonstrates the benefits to online learning modules in the short and medium-term retention of echocardiographic learning content. Medical learners from around the world who had not been previously exposed to echocardiographic learning content exhibited a clear benefit from this online platform and learning materials. These differences appear to be consistent as a whole and across learner subgroups. Cardiology and critical care boot camp fellows also demonstrated the successful acquisition of echocardiographic knowledge following completion of the learning modules. In addition, echocardiography boot camp appeared to further reinforce these core educational echocardiographic concepts as evidenced by incremental increases in test scores following the second post-test. These findings are consistent with Newberry et al. and Windish et al. who both have demonstrated the benefit of a blended approach utilizing web-based resources and modules coupled with classroom learning to promote short and medium-term retention of knowledge [15, 19].
Our study re-affirms and supports existing data from Maskatia et al. on the feasibility and short-term effectiveness of echocardiography boot camp [1]. Boot camp appears to provide a good introduction reinforcing procedural echocardiographic skills as evidenced by the majority of fellows achieving satisfactory competence in the majority of echocardiographic core objectives. There were some challenges noted in more complex imaging (such as pulmonary veins), quantitative assessments (such as ejection fraction) and image optimization which require a higher degree of technical skill and repeated exposure and reinforcement for proper mastery. Our study emphasizes the importance of such high yield educational symposia to promote basic knowledge and skill acquisition in medical trainees.
Limitations
This study was focused on short and medium-term retention of an educational intervention. Fellows were given access to learning modules one month prior to the start of boot camp. Differences in when individual fellows completed the learning modules may introduce additional variability with some fellows having completed the modules weeks prior to the start of boot camp versus shortly before boot camp. In addition, the online only learning group post-test completion times varied considerably introducing additional potential bias of test scores which may have been affected by time from module completion. Consideration of additional follow up testing at longer time intervals would be useful to assess long term retention of learning content. Another limitation of this study is that it may be underpowered to detect more subtle differences as it relates to prior experience within echocardiography and cardiology. Finally, given that the same assessment was taken multiple times, it is possible that the post-test scores may have improved as a consequence of the learner using additional resources to gain insight into incorrect answers. Therefore, some degree of improvement in score may be secondary to test familiarity and outside study, although using outside resources was discouraged and the learners did not receive the answers and explanations to the test until the final post-test was completed in order to minimize these potential confounders.
Conclusion
Our innovative hybrid approach to echocardiography education appears to demonstrate significant benefit. Online tutorials in echocardiography coupled with echocardiography boot camp appear to promote additive short and medium-term retention of echocardiographic knowledge in this population of learners. Training programs should strongly consider a blended educational approach through the implementation of online learning platforms with lecture and procedural-based educational modalities like boot camps. Through this integrated learning method, learners will be better equipped to obtain a fundamental understanding of the basic principles of cardiac ultrasound and the application of these principles in clinical management of infants, children, adolescents, and adults with CHD. Self-directed learning utilizing an online education platform dedicated to pediatric echocardiography significantly promoted the acquisition of background knowledge and improved learner confidence. Online learning platforms can serve as powerful and effective tools in medical education.
References
Maskatia SA, Altman CA, Morris SA, Cabrera AG (2013) The echocardiography “boot camp”: a novel approach in pediatric cardiovascular imaging education. J Am Soc Echocardiogr 26(10):1187–1192. https://doi.org/10.1016/j.echo.2013.06.001
Mertens L, Friedberg MK (2009) The gold standard for noninvasive imaging in congenital heart disease: echocardiography. Curr Opin Cardiol. https://doi.org/10.1097/HCO.0b013e328323d86f
ACCF/AHA/AAP Recommendations for Training in Pediatric Cardiology (2005) A Report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians Task Force on Clinical Competence (ACC/AHA/AAP Writing Committee to develop training recommendations for pediatric cardiology). Circulation 112(16):2555–2580. https://doi.org/10.1161/CIRCULATIONAHA.105.170308
Lai WW, Geva T, Shirali GS et al (2006) Guidelines and standards for performance of a pediatric echocardiogram: a report from the task force of the pediatric council of the American Society of Echocardiography. J Am Soc Echocardiogr 19(12):1413–1430. https://doi.org/10.1016/j.echo.2006.09.001
Benavidez OJ, Gauvreau K, Jenkins KJ, Geva T (2008) Diagnostic errors in pediatric echocardiography: development of taxonomy and identification of risk factors. Circulation 117(23):2995–3001. https://doi.org/10.1161/CIRCULATIONAHA.107.758532
Quiñones MA, Douglas PS, Foster E et al (2003) ACC/AHA clinical competence statement on echocardiography: a report of the American College of Cardiology/American Heart Association/American College of Physicians–American Society of Internal Medicine Task Force on Clinical Competence (Committee on Echocardiography). J Am Soc Echocardiogr 16(4):379–402. https://doi.org/10.1016/S0894-7317(03)00113-5
Kugler JD, Beekman RH III, Rosenthal GL et al (2009) Development of a pediatric cardiology quality improvement collaborative: from inception to implementation. From the Joint Council on Congenital Heart Disease Quality Improvement Task Force. Congenital Heart Dis 4(5):318–328. https://doi.org/10.1111/j.1747-0803.2009.00328.x
Hao M, Ippisch HM, Cook RS et al (2007) Implementation of an objective testing system in noninvasive cardiac imaging for evaluation of pediatric cardiology fellows. J Am Soc Echocardiogr 20(10):1211–1218. https://doi.org/10.1016/j.echo.2007.03.012
Thomas JD, Zoghbi WA, Beller GA et al (2009) ACCF 2008 training statement on multimodality noninvasive cardiovascular imaging. J Am Coll Cardiol 53(1):125–146. https://doi.org/10.1016/j.jacc.2008.10.004
Shappell E, Ahn J (2017) A needs assessment for a longitudinal emergency medicine intern curriculum. WestJEM 18(1):31–34. https://doi.org/10.5811/westjem.2016.9.31493
Maddry JK, Varney SM, Sessions D et al (2014) A Comparison of simulation-based education versus lecture-based instruction for toxicology training in emergency medicine residents. J Med Toxicol 10(4):364–368. https://doi.org/10.1007/s13181-014-0401-8
Ruiz JG, Mintzer MJ, Leipzig RM (2006) The impact of E-learning in medical education. Acad Med 81(3):207–212. https://doi.org/10.1097/00001888-200603000-00002
Little-Wienert K, Hsu D, Torrey S et al (2017) Pediatric emergency medicine online curriculum improves resident knowledge scores, but will they use it? Pediatr Emerg Care 33(11):713–717. https://doi.org/10.1097/PEC.0000000000000679
Walsh K, Rafiq I, Hall R (2007) Online educational tools developed by heart improve the knowledge and skills of hospital doctors in cardiology. Postgrad Med J 83(981):502–503. https://doi.org/10.1136/pgmj.2007.059501
Newberry L, Kennedy N, Greene EA (2016) Development of a subspecialty cardiology curriculum for paediatric registrars in Malawi: implementation of a long-distance hybrid model. Malawi Med J 28(2):57–60. https://doi.org/10.4314/mmj.v28i2.6
Friedl R, Höppler H, Ecard K, Scholz W, Hannekum A, Stracke S (2006) Development and prospective evaluation of a multimedia teaching course on aortic valve replacement. Thorac Cardiovasc Surg 54(1):1–9. https://doi.org/10.1055/s-2005-865871
Gold JP, Begg WB, Fullerton DA, Mathisen DJ, Orringer MB, Verrier ED (2005) Evaluation of web-based learning tools: lessons learned from the thoracic surgery directors association curriculum project three-year experience. Ann Thorac Surg 80(3):802–810. https://doi.org/10.1016/j.athoracsur.2005.03.052
Vollmar HC, Schürer-Maly C-C, Frahne J, Lelgemann M, Butzlaff M (2006) An e-learning platform for guideline implementation–evidence- and case-based knowledge translation via the Internet. Methods Inf Med 45(4):389–396
Windish R, Stuart P, Cruz R, Murray A (2019) Enhancing intern emergency medicine education using a combined didactic and web-based learning curriculum: the EDGE programme. Emerg Med Austral 31(5):837–842. https://doi.org/10.1111/1742-6723.13352
Funding
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No disclosures and no conflict of interest.
Consent to Participate
Consent was obtained for all participants. This was an IRB approved study.
Consent for Publication
The author consent to have this manuscript published as an original work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kailin, J.A., Kyle, W.B., Altman, C.A. et al. Online Learning and Echocardiography Boot Camp: Innovative Learning Platforms Promoting Blended Learning and Competency in Pediatric Echocardiography. Pediatr Cardiol 42, 389–396 (2021). https://doi.org/10.1007/s00246-020-02494-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-020-02494-w