
Abstract
Breast cancer is a multifactorial disease and its etiology is linked to multiple risk factors. There are shreds of controversial evidence that exposure to organochlorine pesticides (OCPs) are important in the etiology of breast cancer. The present study aimed to determine the circulating levels of OCPs in patients with breast tumors in Southeastern of Iran. This case–control study included 27 patients with malignant breast tumors (MBT), 31 patients with benign breast tumors (BBT), and 27 healthy women as a control group. Serum OCPs levels, including α-hexachlorocyclohexane (α-HCH), β-HCH, γ-HCH, 2,4-dichlorodiphenyltrichloroethane (2,4-DDT), 4,4-DDT, 2,4-dichlorodiphenyldichloroethylene (2,4-DDE), and 4,4-DDE, were measured using gas chromatography. Our data revealed significantly higher concentrations of 2,4-DDT in MBT and BBT groups compared with control ones (P < 0.001 for both comparisons). Patients with breast cancer suffered significantly higher accumulation levels of 4,4-DDE compared with control subjects (P = 0.04). Significant correlations were found among organochlorine compounds with each other in both patients’ groups. There was a significant positive correlation between body mass index and serum levels of 2,4-DDT in BBT group (r = 0.407, P = 0.02). The present findings suggest that the serum levels of 4,4-DDE and 2,4-DDT are associated with an increase in the risk of breast cancer in Southeastern women of Iran.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Breast cancer is the most commonly diagnosed cancer and the second leading cause of cancer death in women worldwide (Siegel et al. 2018). In Iran, 24.4% of all diagnosed cancers are breast cancer, which is responsible for more than 1063 deaths each year (Farhood et al. 2018). Although breast cancer etiology is not fully understood, some hereditary and nonhereditary factors can contribute to the development of this malignancy, including age, sex, race, familial history of cancer, lower age of menarche, late childbearing, not lactating, later menopause, obesity, alcohol consumption, inactivity, hormone replacement therapy (HRT), and environmental chemicals (Kamińska et al. 2015; Rodgers et al. 2018).
Among environmental chemicals linked to breast cancer, preceding studies have revealed a significant association between organochlorine pesticides (OCPs) and an increase in breast cancer risk (He et al. 2017; Romieu et al. 2000). Pesticides are a group of chemical compounds used for destructing and/or controlling different kinds of pests, including insects, weeds, fungi, bacteria, etc. (Jayaraj et al. 2016). OCPs are organic compounds with heterogeneous structures composed predominantly of carbon, hydrogen, and chlorine atoms (Mrema et al. 2013). There are three main groups of OCPs, including DDT and its derivative products, hexachlorocyclohexane (HCH) and chlorinated cyclodiene (Pirsaheb et al. 2015). These chemicals belong to the persistent organic pollutants (POPs) group, which persist in the environment because of their resistance against various types of degradation and might be accumulated in animal and human food chains for a long time (Wong et al. 2012). Serious concerns about POPs are attributed to their adverse health effects in humans, including immunosuppressive, oxidative, proinflammatory, neurotoxic, hormone-disrupting, metabolic, and carcinogenic effects (Carpenter 2013; Porta 2012). Accumulating evidence given by epidemiological and agricultural health studies disclosed that OCPs exposure could be associated with the risk of cancers, such as breast, prostate, lung, stomach, colorectal, bladder cancer, etc. (Abolhassani et al. 2019; Jayaraj et al. 2016; Mortazavi et al. 2019). OCPs may interfere with female hormonal functions and affect breast cell proliferation by acting as estrogen mimics, interfering with hormone transport and disrupting hormone synthesis, thereby increasing breast cancer risk (Bretveld et al. 2006). Despite the application of OCPs was banned in the 1980s, they can accumulate in the human body due to its lipophilicity and persistence for many years (Bayat et al. 2011; He et al. 2017).
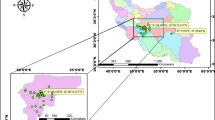
Exposure to OCPs has been studied in the Iranian population and the results have revealed a high degree of contamination by OCPs (Arzi et al. 2009; Behrooz et al. 2012; Cok et al. 1999; Hashemy-Tonkabony and Soleimani-Amiri 1978). Therefore, the possible presence of OCPs in our environment still causes concerns. Because Kerman province is considered as one of the most important regions for agricultural activities and regarding the alarming mortality rate of breast cancer among Iranian women, we sought to determine whether breast cancer risk is associated with serum levels of OCPs in Southeastern women of Iran.
Materials and Methods
Subjects
This case–control study involved 27 female patients with malignant breast tumor (MBT) and 31 female patients with benign breast tumor (BBT) who underwent surgical resection at Shahid Bahonar and Afzalipour hospitals from March 2015 to November 2016 as described elsewhere (Paydar et al. 2018). Detection of breast cancer from benign breast diseases was performed based on clinical and pathological documents following surgery. Among patients with breast cancer, 24 had ductal carcinoma (invasive, infiltrative, and in situ ductal carcinoma) and 3 had invasive lobular carcinoma. Among patients with benign breast diseases, 17, 9, 2, 2, and 1 had fibroadenoma, fibrocystic disease, chronic granulomatous mastitis, glandular adenosis, and hydradenoma respectively.
In addition, 27 healthy women were enrolled as controls (CON) in this study. According to inclusion criteria in the current study, all patients were new cases and patients who had any treatments, such as surgery, radiotherapy, and chemotherapy, were excluded from the study. All the studied patients previously had no history of alcohol consumption and smoking. The control group was women who had no acute and chronic diseases and known cancer as well as they were not smoking or consuming alcohol. Moreover, all the participated women in this study were local inhabitant (Kerman, Iran) for more than 40 years. Written, informed consent was obtained from all the subjects participating in the study before enrollment. The study was conducted in accordance with the principles of the revised Declaration of Helsinki and approved by the Ethics Committee of Kerman University of Medical Sciences, Kerman, Iran (IR.KMU.REC.1394.315). Because surgery may change the blood levels of OCPs, blood specimens were obtained from studied patients before surgery. Blood samples were collected from the participants in the morning after overnight fasting and immediately centrifuged and serum samples kept frozen at −70 °C in preparation for OCPs detection.
Chemicals
The standards of OCPs include α-HCH, β-HCH, γ-HCH, 2,4-DDT, 4,4-DDT, 2,4-DDE, and 4,4-DDE and internal standard (4,4-dichlorobenzophenone, DBP) were purchased from Ehrenstorfer company (Germany). N-hexane, anhydrous sodium sulfate, and ethyl acetate were obtained from Merck (Germany), and sulphuric acid was purchased from Scharlab (Spain).
OCPs Extraction from Serum Specimens
Serum OCPs residues of all subjects were identified and quantified using a gas chromatographic analyzer (Agilent 7890A, USA) coupled to flame ionization detector (GC-FID). Identification of OCPs residues was performed by a slightly modified version of the method as described by Zumbado et al. (2005). Briefly, the internal standard (IS) was added to 0.5 ml of serums. Samples were extracted twice with 2 ml of hexane. Then, with adding 200 µL of concentrated sulphuric acid to combined extracts, organic part of it became separated. We dehydrated this organic part using 100 mg of anhydrous sodium sulfate. Followed by centrifugation, the transferred organic layer was completely concentrated at room temperature. Finally, we added 100 µL of ethyl acetate to each sample for solving extracted OCPs.
GC Condition and OCPs Analysis
An HP5 capillary column (30-m length, 0.22-mm ID, 0.25-µm film thickness) was utilized with nitrogen as carrier gas at a flow rate of 1.5 ml/min. The initial temperature of the oven was maintained at 50 °C for 2 min and then elevated by 30 °C/min to 200 °C and finally programmed to increase at 5 °C/min to 280 °C. Injector and flame ionization detector temperatures were set to 320 °C and 350 °C respectively. A volume of 1 µL of samples and standards were injected into the gas chromatograph with a 5-µL syringe. Under this condition, the seven OCPs were successively detected within a very reasonable time (Fig. 1). The measurement of OCP levels was performed by determination of the retention time and peak area with an internal standard method that are qualitative and quantitative analysis respectively. In this regard, a set of pesticides’ standards solutions with known concentrations (0.78, 1.56, 3.12, 6.25, 12.5, 25, 50, 100, 200, and 400 µg/ml) was prepared, and 100 µg/ml of IS was added to each standard solution. Peak areas of OCP standards and IS were measured and standard curves of OCPs separately constructed by plotting the analyte-to-IS ratio versus the known concentrations of analyte in each sample. The analytical limit of detection (LOD) was estimated 0.7 µg/ml for α-HCH, β-HCH, γ-HCH, 2,4-DDE, and 4,4-DDE and 3 µg/ml for 2,4-DDT and 4,4-DDT.

The chromatogram of seven kinds of OCPs. Under the condition of gas chromatography, these pesticides were detected successively
Statistical Analysis
All continuous and categorical variables were presented as mean ± standard deviation (SD) and numbers (percentages) respectively. Kolmogorov–Smirnov test was utilized to determine the distribution of data. The differences among groups were analyzed using one-way analysis of variance (ANOVA)/Kruskal–Wallis with post hoc Tukey/Mann–Whitney U tests as well as Chi-square/Fisher’s exact tests. Correlations between continuous variables were evaluated using Pearson and Spearman correlation of coefficients. The statistical analyses were performed using SPSS software version 23.0 for Windows (SPSS Inc., Chicago, IL). P values < 0.05 were considered statistically significant.
Results
Participants’ demographic and clinical characteristics are listed in Table 1. No significant differences were found in age, body mass index (BMI), residence, menopause status, and clinical stages of the three studied groups (P > 0.05 for all comparisons).
Comparison of serum levels of OCPs (ng/L) is presented in Fig. 2 and Table 2. The chromatograms of serum OCPs from a breast cancer patient and the matched normal subject are shown in Figs. 3 and 4. The most prevalent OCPs were 2,4-DDT and 2,4-DDE, which were detected in almost all the samples (Table 2). α-HCH was only found in few patients with breast cancer and 4,4-DDT detected in none of three groups. Nevertheless, β-HCH and γ-HCH were detected in the serum of both MBT and BBT groups. Both serum levels of α-HCH and β-HCH showed no significant differences between both MBT and BBT groups (P = 0.40 and P = 0.52, respectively). The serum levels of 2,4-DDT were remarkably different in patients with MBT and BBT compared with healthy women (P < 0.001). The mean serum concentrations of 2,4-DDT were significantly higher in patients with MBT (547.38 ± 480.59 ng/L) and BBT (488.43 ± 453.53 ng/L) than the control group (68.00 ± 29.44 ng/L) (P < 0.001 for both comparisons). It should be noted that the mean serum levels of 2,4-DDT were not significantly different between MBT and BBT groups (P = 0.64).

The scatter dot plot of five kinds of OCPs in patients with MBT, BBT and control subjects. No significant differences were observed in the mean serum levels β-HCH, γ-HCH and 2,4-DDE pesticides among the three studied groups (P > 0.05 for all comparisons) (a, b and d). However, statistically significant differences were found in the mean levels of 2,4-DDT in MBT and BBT groups compared to control group (P < 0.001 for both comparisons) (c) and there was also a significant difference in 4,4-DDE levels between the MBT and control groups (P = 0.04) (e). P values < 0.05 were considered statistically significant. OCPs Organochlorine pesticides, MBT malignant breast tumor, BBT benign breast tumor, CON control

The chromatogram of OCPs and internal standard (DBP) in a normal subject. DBP and 2,4-DDE were detected in the serum sample of this subject. OCPs organochlorine pesticides, DBP, 4,4-dichlorobenzophenone

The chromatogram of OCPs and internal standard (DBP) in a patient with MBT. The OCPs such as α-HCH, β-HCH, γ-HCH, 2,4-DDT, 2,4-DDE and 4,4-DDT were detected in the serum sample of the patient. OCPs organochlorine pesticides, DBP, 4,4-dichlorobenzophenone, MBT malignant breast tumor
The mean serum levels of 2,4-DDE in MBT, BBT, and CON groups were 640.86 ± 348.06, 634.63 ± 295.55, and 643.29 ± 359.68 ng/L, respectively (Table 2). There were no significant differences in 2,4-DDE levels among the three groups (P = 0.99). Furthermore, two by two comparisons did not reveal any considerable differences between groups [P = 0.99 (MBT vs. BBT), P = 1 (MBT vs. CON), and P = 0.99 (BBT vs. CON)].
No significant differences were found in the mean serum levels of 4,4-DDE among the three groups (P = 0.052; Table 2). Nonetheless, the post hoc Tukey test demonstrated significant higher levels of 4,4-DDE in patients with MBT (110.65 ± 48.00 ng/L) compared to healthy (72.42 ± 23.98 ng/L) women (P = 0.04). Likewise, the Tukey test showed higher levels of 4,4-DDE, but not significant, in patients with BBT (83.07 ± 33.28 ng/L) compared with control group (P = 0.73). In addition, it was shown that mean serum levels of 4,4-DDE were not markedly different between MBT and BBT patients (P = 0.27). The serum levels of OCPs were independent of the demographic characteristics of the participants (data are not shown). Tables 3 and 4 illustrate the correlations among age, BMI, and OCPs within MBT and BBT groups. A significant positive correlation was found between BMI and serum 2,4-DDT concentrations in the BBT group (r = 0.40, P = 0.02). Furthermore, the mean serum levels of all OCPs were positively correlated with each other.
Discussion
Breast cancer, a recognizable major public health problem, is one of the common malignant tumors among women worldwide. Although the precise cause of breast cancer development is not fully understood, some possible risk factors are related to its occurrence, including genetic, reproductive, lifestyles, and environmental factors (Paydar et al. 2019). It has been suggested that OCPs can act as endocrine disruptors and increase the risk of developing breast cancer through an estrogen-like effect (Bretveld et al. 2006). In general, some research groups in various countries have investigated the presence of OCPs in different diseases, particularly breast cancer, but until now, the results were still controversial. Several lines of evidence support our hypothesis about the association between body burden of OCPs and breast cancer risk. In the present study, we demonstrated that serum levels of 2,4-DDT and 4,4-DDE may enhance the risk of breast cancer development. In exploring of OCPs in three studied groups, we found that the higher levels of 2,4-DDT and 4,4-DDE residues were accumulated in the serum of patients with MBT compared with normal subjects. Moreover, elevated serum levels of 2,4-DDT were detected in patients with BBT as compared to the control group.
In agreement with current result, He et al. found an association between p,p′-DDE and breast cancer risk. They showed the presence of p,p′-DDE in breast tissues of more than 90% breast cancer cases (He et al. 2017). In the study conducted by Mathur et al. blood OCPs, including DDT and its metabolites DDD and DDE, heptachlor, dieldrin, and HCH, were found significantly higher in the breast cancer patients than normal participants (Mathur et al. 2002). Romieu et al. indicated that serum levels of DDE are positively related to breast cancer risk and this association is more apparent among postmenopausal women. Based on their report, no association was found between serum levels of DDT and breast cancer risk (Romieu et al. 2000). Attaullah et al. (2018) reported higher serum levels of 4,4-DDE in breast cancer cases compared with controls that are consistent with our result. Taken together, the high levels of 2,4-DDT and 4,4-DDE in the serum of patients with MBT are remarkable findings, which suggest the possible involvement of OCPs in the development of breast cancer. On the other hand, high levels of serum 2,4-DDT in breast cancer patients describe the presence of this pesticide in Iran, which is consistent with a study conducted by Behrooz et al. (2012) that revealed the presence of organochlorine contaminants in the hair of Iranian pregnant women.
Based on present results, β-HCH and γ-HCH were found in the serum specimens of patients with MBT and BBT and the levels of these pesticides were not statistically significant between two groups. Furthermore, α-HCH was detected in the serum samples of the small numbers of patients with MBT. In line with current findings, Lopez and coworkers revealed no relationship between β-HCH and breast cancer risk (Lopez-Carrillo et al. 2002). Moreover, Itoh et al. reported the lack of association of breast cancer risk with the serum concentration of β-HCH in the Japanese population (Itoh et al. 2009). In contrast, Yang et al. demonstrated the higher levels of β-HCH in serum and adipose tissue of breast cancer patients with positive estrogen receptor than those with negative estrogen receptor, suggesting that OCPs can disturb endocrine pathways (Yang et al. 2015).
According to our result, no significant difference was observed in the serum concentrations of 2,4-DDE in three studied groups, and none of the participants had detectable levels of 4,4-DDT. Contrary to our results, Boada and coworkers indicated that the organochlorine pesticide mixtures, such as aldrin, DDE, and DDD, may play a relevant role in the development of breast malignancy (Boada et al. 2012). Apart from these human studies, multiple research on animal models and cell culture supports our result regarding the involvement of OCPs in breast cancer development. Johnson et al. (2012) demonstrated p,p′-DDE exposure at concentrations relevant to human exposure in adipose tissue surrounding mammary epithelium promotes mammary tumorigenesis in mice. It is noteworthy that we also found higher concentrations of 4,4-DDE in serum samples of breast cancer patients compared with control subjects. Furthermore, Bratton et al. (2012) indicated that o,p-DDT is able to stimulate genes expression in breast cancer cells through initiating crosstalk between MAPK signaling pathways and transcriptional coactivators. Interestingly, we observed the higher serum levels of 2,4-DDT in patients with breast tumors compared with healthy individuals.
Although some studies have shown the roles of OCPs in the development of breast cancer, two meta-analysis studies in 2013 and 2014 explained that exposure to OCPs, such as DDT and DDE, could not be associated with human breast cancer risk (Ingber et al. 2013; Park et al. 2014). These contraries may be due to the delay time between exposure to pesticides and cancer diagnosis, age exposed to pesticides, the effect of susceptible populations, and combined exposure with other environmental carcinogens (Park et al. 2014).
Based on the correlation analysis in our study, the concentrations of β-HCH, γ-HCH, 2,4-DDT, 2,4-DDE, and 4,4-DDE were correlated with each other in MBT and BBT groups. This is consistent with previous reports, which suggested the presence of correlations among OCPs with each other (Lind et al. 2018; Yang et al. 2012). These correlations support the concept that the collective effects of OCPs may increase breast cancer risk and affect clinical outcomes of cancer.
In this study, we also observed a significant relationship between BMI and serum 2,4-DDT concentrations in BBT group. This finding emphasizes that OCPs levels are directly related to the fat content in view of the lipophilic nature of OCPs. In agreement with this data, a study showed a correlation between p,p-DDE, but not 2,4-DDT, and BMI in breast cancer patients (Ellsworth et al. 2018).
Generally, the present findings warrant further analysis and consideration of possible exposure routes. Because carcinogenesis is considered as a multifactorial event, it is substantial to try to clarify the role of environmental chemicals in the development of cancer.
Some limitations of our study warrant mention. Because the sampling process was demanding and time-consuming, the sample size is rather small. In our study, serum levels of OCPs were strongly correlated with each other, thus they also can be correlated with unmeasured other OCPs and environmental substances. Hence, the current findings might not have represented the direct effect of studied OCPs in the development of breast tumors. The present study, however, enjoys a strong point including the presence of a link between exposure to OCPs and risk of breast cancer. In addition, the status of serum OCPs due to their biological persistence reflects long-term cumulative exposure to these environmental compounds in our study. Moreover, the present research is the first study that has explored the presence of serum OCPs in patients with breast cancer in Iran. Therefore, the outcome of our study opens a new avenue for understanding the possible causes of the rapid growth of breast cancer in Iran.
Conclusions
The results of the present study support the hypothesis that exposure to OCPs, particularly 2,4-DDT and 4,4-DDE, may be associated with breast cancer risk. We demonstrated that exposure to 2,4-DDT may increase the risk of benign breast diseases. Because significant correlations were found among the different OCPs in the serum samples of MBT and BBT groups, it could be concluded that total body burden of OCPs may mediate the involvement of these pesticides in development of different malignancies. Moreover, the presence of a correlation between BMI and the levels of 2,4-DDT obviously suggests that obese women may bear higher levels of OCPs compared with nonobese in the same condition.
References
Abolhassani M, Asadikaram G, Paydar P, Fallah H, Aghaee-Afshar M, Moazed V, Moradi A (2019) Organochlorine and organophosphorous pesticides may induce colorectal cancer: a case–control study. Ecotoxicol Environ Saf 178:168–177
Arzi L, Nazari KZ, Arzi A (2009) Comparison of the organochlorine pesticide residue levels among Benni fish of Shadegan, Mahshahr and Susangerd cities, Khouzestan Province, Iran. Toxicol Lett 189:207
Attaullah M, Yousuf MJ, Shaukat S, Anjum SI, Ansari MJ, Buneri ID, Khan SU (2018) Serum organochlorine pesticides residues and risk of cancer: a case–control study. Saudi J Biol Sci 25(7):1284–1290
Bayat S, Sari AE, Bahramifar N, Younesi H, Behrooz RD (2011) Survey of organochlorine pesticides and polychlorinated biphenyls in commercial pasteurized milk in Iran. Environ Monitor Assess 175(1–4):469–474
Behrooz RD, Barghi M, Bahramifar N, Esmaili-Sari A (2012) Organochlorine contaminants in the hair of Iranian pregnant women. Chemosphere 86(3):235–241
Boada LD, Zumbado M, Henríquez-Hernández LA, Almeida-González M, Álvarez-León EE, Serra-Majem L, Luzardo OP (2012) Complex organochlorine pesticide mixtures as determinant factor for breast cancer risk: a population-based case–control study in the Canary Islands (Spain). Environ Health 11(1):1–9. https://doi.org/10.1186/1476-069X-11-28
Bratton MR, Frigo DE, Segar HC, Nephew KP, McLachlan JA, Wiese TE, Burow ME (2012) The organochlorine o, p’-DDT plays a role in coactivator-mediated MAPK crosstalk in MCF-7 breast cancer cells. Environ Health Perspect 120(9):1291–1296. https://doi.org/10.1289/ehp.1104296
Bretveld RW, Thomas CMG, Scheepers PTJ, Zielhuis GA, Roeleveld N (2006) Pesticide exposure: The hormonal function of the female reproductive system disrupted? Reprod Biol Endocrinol 4(1):30–44
Carpenter DO (2013) Effects of persistent and bioactive organic pollutants on human health. Wiley, Hoboken
Cok I, Karakaya AE, Afkham BL, Burgaz S (1999) Organochlorine pesticide contaminants in human milk samples collected in Tebriz (Iran). Bull Environ Contam Toxicol 63(4):444–450
Ellsworth RE, Kostyniak PJ, Chi L, Shriver CD, Costantino NS, Ellsworth DL (2018) Organochlorine pesticide residues in human breast tissue and their relationships with clinical and pathological characteristics of breast cancer. Environ Toxicol 33:876–884
Farhood B, Geraily G, Alizadeh A (2018) Incidence and Mortality of various cancers in Iran and compare to other countries: a review article. Iran J Public Health 47(3):309–316
Hashemy-Tonkabony SE, Soleimani-Amiri MJ (1978) Chlorinated pesticide residues in the body fat of people in Iran. Environ Res 16(1–3):419–422
He T-T, Zuo A-J, Wang J-G, Zhao P (2017) Organochlorine pesticides accumulation and breast cancer: a hospital-based case–control study. Tumor Biol 39(5):1–6. https://doi.org/10.1177/1010428317699114
Ingber SZ, Buser MC, Pohl HR, Abadin HG, Murray HE, Scinicariello F (2013) DDT/DDE and breast cancer: a meta-analysis. Regul Toxicol Pharmacol 67(3):421–433
Itoh H, Iwasaki M, Hanaoka T, Kasuga Y, Yokoyama S, Onuma H, Tsugane S (2009) Serum organochlorines and breast cancer risk in Japanese women: a case–control study. Cancer Causes Control 20(5):567–580
Jayaraj R, Megha P, Sreedev P (2016) Organochlorine pesticides, their toxic effects on living organisms and their fate in the environment. Interdisciplinary Toxicology 9(3–4):90–100. https://doi.org/10.1515/intox-2016-0012
Johnson NA, Ho A, Cline JM, Hughes CL, Foster WG, Davis VL (2012) Accelerated mammary tumor onset in a HER2/Neu mouse model exposed to DDT metabolites locally delivered to the mammary gland. Environ Health Perspect 120(8):1170–1176
Kamińska M, Ciszewski T, Łopacka-Szatan K, Miotła P, Starosławska E (2015) Breast cancer risk factors. Przeglad Menopauzalny 14(3):196–202. https://doi.org/10.5114/pm.2015.54346
Lind PM, Salihovic S, Lind L (2018) High plasma organochlorine pesticide levels are related to increased biological age as calculated by DNA methylation analysis. Environ Int 113:109–113
Lopez-Carrillo L, Lopez-Cervantes M, Torres-Sanchez L, Blair A, Cebrian ME, Garcia RM (2002) Serum levels of beta-hexachlorocyclohexane, hexachlorobenzene and polychlorinated biphenyls and breast cancer in Mexican women. Eur J Cancer Prev (ECP) 11(2):129–135
Mathur V, Bhatnagar P, Sharma RG, Acharya V, Sexana R (2002) Breast cancer incidence and exposure to pesticides among women originating from Jaipur. Environ Int 28(5):331–336
Mortazavi N, Asadikaram G, Ebadzadeh M, Kamalati A, Pakmanesh H, Dadgar R, Abolhassani M (2019) Organochlorine and organophosphorus pesticides and bladder cancer: a case–control study. J Cell Biochem 2019:1–13
Mrema EJ, Rubino FM, Brambilla G, Moretto A, Tsatsakis AM, Colosio C (2013) Persistent organochlorinated pesticides and mechanisms of their toxicity. Toxicology 307:74–88. https://doi.org/10.1016/j.tox.2012.11.015
Park J-H, Cha ES, Ko Y, Hwang M-S, Hong J-H, Lee WJ (2014) Exposure to dichlorodiphenyltrichloroethane and the risk of breast cancer: a systematic review and meta-analysis. Osong Public Health Res Perspect 5(2):77–84. https://doi.org/10.1016/j.phrp.2014.02.001
Paydar P, Asadikaram G, Zeynali Nejad H, Moazed V, Poursayedi B, Nematollahi MH, Khosravi Shadmani F (2018) The role of acetylcholinesterase, paraoxonase, and oxidative stress in breast tumors. Int J Cancer Manag 11(11):1–8. https://doi.org/10.5812/ijcm.83370
Paydar P, Asadikaram G, Nejad HZ, Akbari H, Abolhassani M, Moazed V, Fallah H (2019) Epigenetic modulation of BRCA-1 and MGMT genes, and histones H4 and H3 are associated with breast tumors. J Cell Biochem 2019:1–11. https://doi.org/10.1002/jcb.28645
Pirsaheb M, Limoee M, Namdari F, Khamutian R (2015) Organochlorine pesticides residue in breast milk: a systematic review. Med J Islam Repub Iran 29(1):1–10
Porta M (2012) Human contamination by environmental chemical pollutants: Can we assess it more properly? Prev Med 55(6):560–562
Rodgers KM, Udesky JO, Rudel RA, Brody JG (2018) Environmental chemicals and breast cancer: an updated review of epidemiological literature informed by biological mechanisms. Environ Res 160:152–182. https://doi.org/10.1016/j.envres.2017.08.045
Romieu I, Hernandez-Avila M, Lazcano-Ponce E, Weber JP, Dewailly E (2000) Breast cancer, lactation history, and serum organochlorines. Am J Epidemiol 152(4):363–370. https://doi.org/10.1093/aje/152.4.363
Siegel RL, Miller KD, Jemal A (2018) Cancer statistics, 2018. CA Cancer J Clin 68(1):7–30. https://doi.org/10.3322/caac.21442
Wong MH, Armour M-A, Naidu R, Man M (2012) Persistent toxic substances: sources, fates and effects. Rev Environ Health 27:207–213
Yang J-H, Lee Y-M, Bae S-G, Jacobs DR Jr, Lee D-H (2012) Associations between organochlorine pesticides and vitamin D deficiency in the US population. PLoS ONE 7(1):1–6
Yang J-Z, Wang Z-X, Ma L-H, Shen X-B, Sun Y, Hu D-W, Sun L-X (2015) The organochlorine pesticides residues in the invasive ductal breast cancer patients. Environ Toxicol Pharmacol 40(3):698–703. https://doi.org/10.1016/j.etap.2015.07.007
Zumbado M, Goethals M, Álvarez-León EE, Luzardo OP, Cabrera F, Serra-Majem L, Domínguez-Boada L (2005) Inadvertent exposure to organochlorine pesticides DDT and derivatives in people from the Canary Islands (Spain). Sci Total Environ 339(1–3):49–62. https://doi.org/10.1016/j.scitotenv.2004.07.022
Acknowledgements
The authors are very grateful to all participants in the present study who kindly donated blood samples and their time. This study was supported by a grant from Kerman University of Medical Sciences, Kerman, Iran (Grant No.: 94/413) and is a part of a Ph.D. thesis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Paydar, P., Asadikaram, G., Fallah, H. et al. Serum levels of Organochlorine Pesticides and Breast Cancer Risk in Iranian Women. Arch Environ Contam Toxicol 77, 480–489 (2019). https://doi.org/10.1007/s00244-019-00648-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00244-019-00648-3