
Abstract
To identify the best material (soil or dust) to be selected for health-risk assessment studies, road dust and urban soil from three cities with different population densities were collected, and size fractions were analysed for metal content (Pb, Zn, Cu, Cd, Cr, Co, and Ni). Results showed similar distribution of the size particles among cities, predominating fractions between 75 and 2000 μm in road dust and particles below 75 μm in soil. Metals were mainly bound to PM10 in both soil and road dust increasing the risk of adverse health effects, overall through inhalation exposure. The risk assessment showed that the most hazardous exposure pathway was the ingestion via, followed by dermal absorption and inhalation route. Values of hazard quotient showed that the risk for children due to the ingestion and dermal absorption was higher than adults, and slightly larger at PM10 comparing to <75-μm fraction for the inhalation route. Higher risk values were found for road dust, although any hazard index or cancer risk index value did not overreach the safe value of 10−6.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Urban activities release a variety of potentially harmful pollutants to the environment, especially metals and organic compounds (Wong et al. 2006). Atmospheric particles deposition induces metal accumulation in surface soil and road dust causing environmental and health risk (Acosta et al. 2015). Recent researches are focused on the concentration of metals in bulk soil and road dust (Shi et al. 2008; Sun et al. 2010; Duong and Lee 2011); however, the concentration in different particles size fractions is critical to estimate the potential contributions to environmental safety and health (Han et al. 2008).
Generally, trace metals are found associated with finer particles, especially PM10 and PM2.5, causing serious risk on human health because of the incorporation of metals to the human body through the mouth and nose (Ljung et al. 2008; Kong et al. 2011; Cao et al. 2011; Boisa et al. 2014).
Human health risk assessment is the process to estimate the nature and probability of adverse health effects in humans who may be exposed to chemicals (US-EPA 2016a). Human are exposed to pollutants by three main pathways: ingestion, inhalation, and dermal absorption of soil and dust. The health risk assessment has usually been investigated separately for soil (Izquierdo et al. 2015; Teng et al. 2015; Huang et al. 2016; Chen et al. 2016) and dust (Ferreira-Baptista and De Miguel 2005; Kong et al. 2011; Du et al. 2013; Li et al. 2013; Liu et al. 2014; Wang et al. 2016; García-Rico et al. 2016), and few authors have investigated both soil and dust (De Miguel et al. 2007).
The purpose of this study was to assess the health risk of metal exposure for children and adults in three cities with different population densities and elucidate which material, soil, or dust contributed more to increase the health risk. In addition, inhalation hazard quotient from PM10 and from <75-μm fraction were calculated and compared between each other to evaluate the difference.
Materials and Methods
Study Area
The study area consisted of three different populated urban settlement located in Murcia Region (SE of Spain). Murcia city represents high density (HD = 498 people km−2), whereas Totana and Abaran cities have medium (MD = 106 people km−2) and low (LD = 27.8 people km−2) population densities, respectively.
The climate of the region is Mediterranean semiarid with 18 °C annual mean temperature and 350-mm annual mean rainfall. The weather and the social habits invite people to spend time at streets and gardens, especially children.
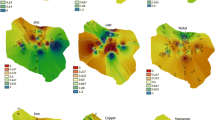
Difficulty collecting soil samples in urban areas limited the sampling to parks and urban gardens. Most parks from each city were sampled and were selected based on spatial distribution, size, and population use. Thirty surface soil samples were collected in the three cities (Fig. 1). Each soil sample was taken from the surface (0–5 cm) using a soil spade and was composed by three subsamples collected 1-m apart from the vertices of a triangle to form a composite sample. We used surface soil, because metal additions to soils in urban areas occur mostly on topsoil (De Miguel et al. 1998; Porta et al. 1999).

Sampling map. Top HD city (left) and MD city (right). Bottom LD city; black speckles represent soil samples and white triangles represent dust samples
During the sampling, we tried to collect both materials: soils and dusts; however, sampling of dust was restricted to those roads where dust is accumulated in enough amount to be sampled (Fig. 1). Specifically, 13 street dust samples were collected by sweeping an area of 1 m2 using a polyethylene brush and getting three subsamples for each site. The sweep was slow and directly into the plastic bag to avoid dust resuspension (Acosta et al. 2011; Zhang et al. 2012; Du et al. 2013).
Sample Analysis
Soil and dust samples were dried for 48 h at 40 °C and passed through a 2-mm metal-free sieve. A subsample of bulk sample is separated for fractionating in three particle size fractions using two methodologies. For fine particles (PM10), 50 g of soil/dust was dispersed with Na-polyphosphate for 8 h by horizontal shaking (250 rpm). Then, a 1-L glass column was filled with the soil dispersion, and the fractions were separated by repeated sedimentation and decanting based on Stokes’ law (Ljung et al. 2008; Boisa et al. 2014; Li et al. 2017a). For particles larger and smaller than 75 μm, after oven-dry, 75-μm sieve was used, shaking 10 min for each sample. The weight of each size fraction (<75 and >75 μm) was determined to calculate the distribution of each particle size fraction using a laser diffraction particle sizer (Mastersizer 2000).
One gram of each fraction, >75, <75, and <10 μm, and the bulk soil/dust sample were grounded and digested using 20-mL nitric/perchloric acid at 210 °C during 90 min. After cooling, 0.1 N HCl was added to fill a 100-mL volumetric flask (Risser and Baker 1990), and the total amounts of metals (Cd, Co, Cr, Cu, Ni, Pb, and Zn) were measured with ICP-OES and ICP-MS. Samples were analysed in triplicate and reference material (BAM-U110), and reagents blanks were used as quality control during the analysis.
Health Risk Assessment
Human health risk assessment consists of four stages: (1) hazard identification, (2) toxicity assessment, (3) exposure assessment, and (4) risk characterization (Lim et al. 2008). The exposure assessment evaluates the type and magnitude of exposure to chemicals of potential concern at a site (US-EPA 2004). In general, exposure duration, exposure frequency, and contact rate are likely to be the most sensitive parameters in an exposure assessment (US-EPA 1989). Direct ingestion, fugitive dust inhalation, and dermal absorption are common routes of human exposure to contaminant in the residential setting (US-EPA 1996).
The methodology used to calculate the exposure risk of soil and road dust metals has been recently used in risk-assessment studies (Dehghani et al. 2017; Gope et al. 2017; Li et al. 2017a, b) and was based on the U.S. Environmental Protection Agency (U.S. EPA) methodology for risk assessment. The daily dose received through ingestion (D ing), dermal (D dermal), and inhalation (D in h) routes were calculated using the Eqs. (1)–(3) adapted from the US-EPA (1989, 1992a, 1996, 2002a, 2004).
For carcinogens elements (Cd, Cr, Ni, and Co), the lifetime average daily dose (LADD) was calculated for the inhalation route in order to assess the cancer risk (Eq. 4) (Li et al. 2013; Lu et al. 2014; Dehghani et al. 2017).
D (mg kg−1 day−1) is the daily dose intake through ingestion (D ing), dermal absorption (D dermal), and inhalation (D inh). C is the concentration of metal (mg kg−1) in the soil or dust. The ingestion rate (IngR) for this study is estimated at 100 mg day−1 for adults and 200 mg day−1 for children (US-EPA US-EPA 2002a). The inhalation rate (InhR) is estimated at 20 m3 day−1 for adults (US-EPA 1986) and 7.6 m3 day−1 for children (Lu et al. 2014). Exposure frequency (EF) is 122 day year−1. The exposure duration (ED) is 24 years for adults and 6 years for children (US-EPA 2002a). Standard body weight (BW) from US-EPA (1986) is 70 kg for adults and 15 kg for children. Data for dermal dose were recovered from RAGS part E (US-EPA 2004); SL, the skin adherence factor for this study, was 0.07 mg cm−2 for adults and 0.2 mg cm−2 for children. SA is the exposed skin area in this study: 5700 cm2 for adults and 8000 cm2 for children. The ABS is the dermal absorption factor, which was 0.001 (unitless) for all metals of this study.
The particulate emission factor (PEF) relates the concentration of contaminant in soil with the concentration of dust particles in the air. The default value calculated by US-EPA (1996) 1.32 × 109 m3 kg−1 has been used for this study. The average time (AT) for noncarcinogens is calculated as ED × 365 days and for carcinogens 70 × 365 days (US-EPA 1989).
The concentration term (C) in the intake equation is an estimate of the arithmetic average concentration for a contaminant based on a set of site sampling results. Because of the uncertainty associated with estimating the true average concentration at a site, the 95% upper confidence limit (UCL) of the arithmetic mean should be used (US-EPA 1992b). For this study, we used a nonparametric UCL method: the Chebyshev Inequality (US-EPA 2002b).
Risk characterization was assessed from the hazard quotient (HQ) for each metal at each site for noncarcinogens (Eq. 5) and cancer risk (CR) for carcinogens (Eq. 6).
D is the ingestion, dermal, or inhalation calculated dose from Eqs. 1–3; RfD is the corresponding reference dose that is defined as the intake or dose per unit of body weight (mg kg1 day−1) that is unlikely to result in toxic (noncarcinogenic) effects to human populations, including sensitive subgroups. For carcinogenic metals, the dose (D) has been calculated as the lifetime average daily dose that is multiplied by the corresponding slope factor (SF). It is used to express the cancer risk as an estimate of the upper-bound probability of an individual developing cancer as a result of exposure to a particular carcinogen.
Reference doses and slope factors (Cd, Co, Cr, Cu, Ni, and Zn) used in the study were taken from the Risk Assessment Information System (RAIS, accessed April 2016) and lead (Pb) values from De Miguel et al. (2007). Toxicity values for dermal absorption were calculated by multiplying oral reference dose by gastrointestinal absorption factor. The inhalation reference dose for Cd, Co, Cu, Pb, and Zn were substituted by oral reference dose, because after inhalation, the absorption of the particle bound toxicants will result in similar health effects as if the particles have been ingested (Van der Berg 1995; Ferreira-Baptista and De Miguel 2005; Li et al. 2013, 2017a, b).
The hazard index (HI) was the sum of the hazard quotient (HQ) from each pathway. Hazard index values <1 means that there is no significant risk of noncarcinogenic effects, whereas HI values >1 suggest that adverse effects may occur (US-EPA 2001 in Lu et al. 2014). For cancer risk, the acceptable value to ensure no risk ranges from 10−4 to 10−6 (Lu et al. 2014) that means from one additional case in a population of 1 million to one in 10,000 people is acceptable (Lim et al. 2008).
Results and Discussion
Particle Size Distribution and Metal Concentration in the Soil and Road Dust
Particle distribution was focused in three specific particles sizes: (1) >75 μm (coarse fraction); (2) <75 μm (fine fraction); and (3) particulate matter <10 μm (PM10). The mass proportion for each particle size fraction is referred to the total mass of particles in the soil or road dust samples. Thus, a similar pattern distribution was found for HD, MD, and LD cities (Fig. 2).

Particle size distribution (%) in soil and dust samples
Among the fractions, the highest percentages in the soil were obtained for fractions below 75 μm in the HD city, while the coarse fraction (75–2000 μm) ranges 35–50% of the total particles. Contrary, road dust samples were governed by the coarse fraction, overreaching 70% of the total particles in the three cities.
Figure 3 shows the concentration of metals (Cd, Co Cr, Cu, Ni, Pb, and Zn) in different particle size fractions and the bulk sample for both soil and road dust. The percentages of metals loadings in different size fractions were calculated by multiplying metal concentrations with the mass percentage of each size fraction (Li et al. 2017b).


Metals concentration by particle size in soil and dust
Highest metal concentration in the bulk soil was found at MD city for Pb, HD city for Co, and HD and LD cities for Cu, whereas Zn, Cd, Cr, and Ni showed similar values for soils of the whole studied cities. Contrary, Pb, Cu, Cd, and Cr of dust samples reported the highest values at HD city and Co and Ni for HD and LD cities. Metal values obtained for the bulk soil were mostly higher than obtained by Acosta et al. (2011) and Chen et al. (2016) and lower those reported by Shi et al. (2008) for urban soil of Spain, Beijing, and Shanghai.
When focusing on differences among particles larger and smaller than 75 μm, the highest concentrations of Pb, Zn, Cu, and Cr were observed in fine particles (<75 μm) for soil and dust, except for Pb in HD city and Cu in LD city dust where both metals are mainly bonded to the coarse fraction (>75 μm). The same has been observed with Co for dust in the three cities and Ni in HD and MD cities dust.
Highest metal concentration in the fine fraction (<75 μm) of soil was found at MD city for Pb (75.5 mg kg−1), Co (35 mg kg−1), and Cr (43 mg kg−1) and at HD city for Cu (123 mg kg−1), whereas Zn, Cd, and Ni showed similar values for soils of the whole cities studied. Those values were higher than reported by Tang and Han (2017) for urban soils of Beijing and Dehghani et al. (2017) for urban soils of Teheran. Contrary, the highest metal concentrations in the fine fraction of the road dust were reported for the HD city, whose dust concentrations of Cu, Co, and Ni were higher than reported by Tang and Han (2017) and Li et al. (2017a) for road dust of Beijing and Chengdu (China).
Particles <10 μm (PM10) represented approximately 20% of weight in the bulk soil samples and approximately 10% in the road dust samples. The impact of PM10 on human health have been acknowledged to reduce cardiopulmonary function and increase mortality from cardiovascular disease, the occurrence of asthma in children, and the risk of cancer (Hou et al. 2016). As a consequence, this fraction could become more hazardous for human health than the amount of harmful elements bound to others fractions.
Highest concentrations of trace metals were reported for dust samples in the fine fraction, especially in PM10, suggesting that road dust is a more interesting media than soil to understand the risk assessment for human health in urban environment, especially on this particle fraction. The accumulation of metals in fine particle fractions might be contributed to the increased surface area and negative charges (Luo et al. 2015; Qin et al. 2016).
HD city showed the highest values of Pb and Cu for the soil and road dust samples within the PM10 fraction (91/170 and 146/217 mg kg−1, respectively), whereas in HD and MD cities the values of Zn reach 130 mg kg−1 in soil and 450 mg kg−1 in dust samples of PM10. Similar values among cities were found for Cd (0.4 mg kg−1) and Cr (45 mg kg−1) in soil while for dust HD city showed the highest values for both metals Cd (0.97 mg kg−1) and Cr (85 mg kg−1). Results obtained were higher than those reported by Acosta et al. (2009) but lower than obtained by Amato et al. (2009) at different Mediterranean regions.
Human Risk Assessment
After the particle size distribution analysis showed that most metals were bound to the finer fraction (<75 μm), the potential adverse effect to human health was assessed. The Upper Confidence Limit (UCL) from total metal in the fraction below 75 μm, toxicity values, and results from hazard quotient (HQ), hazard index (HI), and cancer risk (CR) are shown in Table 1.
Results of HQs for noncarcinogenic effects showed the ingestion route as the main contributor to the total risk, followed by dermal absorption and inhalation of particles from the soil and road dust samples. Similar results were found in previous studies for soil and road dust samples (Ferreira-Baptista and De Miguel 2005; De Miguel et al. 2007; Du et al. 2013; Li et al. 2013; Lu et al. 2014; Gope et al. 2017) in urban environments.
Conversely, the inhalation route for Ni in soil and road dust showed an HQ 10–100 times higher than dermal, suggesting higher contribution of the inhalation route to the total risk for Ni. The contribution of the particulate matter could reach more than 50% of importance for some metals, such as Ni, whereas for others is less than 1% (Boisa et al. 2014).
Observed children risk values for trace metals were one order of magnitude higher than for adults from ingestion and dermal absorption routes in the three studied cities (Table 1), which is the same as observed Li et al. (2017b). Children may ingest significant quantities of the soil due to their tendency to play on the ground outdoors and to mouth objects or their hands, whereas adults also may ingest soil or dust particles adhered to food, cigarettes, or their hands (US-EPA 2011a).
The Hazard Quotient from inhalation route was in the same order of magnitude for adults and children although higher values for children were observed. The inhalation HQs for Pb and Ni were 100 times lower than HQs for dermal and ingestion routes (Table 1). A similar behaviour was observed for the other noncarcinogenic metals. Thus for adults, the HQinh value of Zn range from 104 to 106 times lower than dermal and ingestion HQs, Cu among 110,000, Cd from 103 to 104, Cr range from 10 to 100 and Co from a hundred to a thousand time lower than the others HQs.
For children, the difference of the HQ inhalation with the ingestion and dermal HQs of noncarcinogenic metals was increased one or two orders of magnitude than adults mainly due to the higher values of the ingestion quotient. Similar results have been observed by Gope et al. (2017).
Hazard Index soil values for adults and children in HD, MD, and LD cities decreased as follows: Zn > Cr > Ni > Cu > Co > Cd > Pb. The highest soil risk values for adults and children were found for Cu (2.94E−03/2.74E−02) and Ni (4.70E−03/3.20E−0) in HD city, Zn (2.43E−02/2.25E−01), Cr (1.19E−02/1.05E−01), Co (1.19E−03/1.11E−02), and Pb (2.03E−04/1.87E−03) in MD city, and Cd (4.25E−04/3.63E−03) in LD city. Those values were below the safe level (HI ≤ 1) suggesting nonadverse health effect derived to the metal exposure.
For dust samples, the HI values decreased as Zn > Cr > Cu > Ni > Co > Cd > Pb in HD and LD cities for adults and children and in MD city for children, whereas for adults in MD city the metal distribution was as showed for the soil. Highest risk values in dust samples were found at HD city for both subpopulations, although no value indicates adverse effects for human health. The HI values shown by soils and road dust were one order of magnitude higher for adults than children. This behaviour also has been observed on previous researches (Wang et al. 2016; Li et al. 2017b).
Cadmium, Cr, Co, and Ni involve a cancer risk because of the exposure to soil and dust by inhalation route. Table 1 showed CR values (10−8–10−11) lower than the maximum value accepted, 10−6 (US-EPA 2002a; Li et al. 2013; Lu et al. 2014). Cancer risk (CR) values decreased as Co > Ni > Cr > Cd in soil from HD, MD, and LD cities were slightly higher than the risk for Co in HD city and for Cr in MD and LD cities. The CR values for the other metals were similar in all studied cities.
In dust samples, cancer risk values decreased as Co > Ni > Cr > Cd in HD and LD city, whereas in MD city Cr showed higher risk than Ni. Hence, soil or dust cancer risk values never overreached the tolerable values (10−4–10−6), indicating no adverse health effects.
This model has been proved to be a useful tool to assess the human health risk, although some uncertainties exist due to the exposure to hazard pollutants in urban pathways. Those uncertainties are linked to the missing or incomplete information needed to define exposure and dose fully (scenario uncertainty), regarding some parameter (parameter uncertainty) and gaps in scientific theory required to make predictions on the basis of causal inferences (model uncertainty) (US-EPA 2011b; De Miguel et al. 2007; Li et al. 2013). Regardless, human risk assessment is useful to supply information for public agencies and government about the potential risks associated with trace metals exposure in a given location.
Inhalation of Particulate Matter (PM10)
PM10 is mainly primary in origin, having been emitted as fully formed particles derived from abrasion and crushing processes, soil disturbances, plant and insect fragments, pollens, and other microorganisms (US-EPA 2009). The size of particles is directly linked to their potential for causing health problems. Particles smaller than 10 μm pose the greatest problems, because they can get deep into the lungs and some may even get into the bloodstream (US-EPA 2016b). According to US-EPA and due to higher concentrations of trace metals that were found in particle size below 10 μm (Fig. 3), only the inhalation exposure route was studied for particulate matter in the fine fraction (Table 2).
Inhalation HQ values for noncancer trace metals in the soil decreased as follows: Ni > Cr > Pb > Cu > Co > Cd > Zn for both adults and children at the three cities, except for MD where Zn showed a slightly higher value than Cd for adults. Although no large differences among cities were found for inhalation HQs, the highest risk values were observed for adults and children respectively at HD city for Cu (5.36E−7/5.65E−6) and Ni (1.03E−3/1.83E−3), at MD city for Pb (3.19E−6/5.65E−6), Zn (4.59E−8/8.13E−8), Cd (4E−8/7.09E−8), and Co (1.49E−7/2.6E−7), and at LD city only Cr (1.64E−4/2.9E−4).
In road dust samples, the HQ inhalation values decreased as Ni > Cr > Pb > Cu > Co > Cd > Zn for both adults and children at HD city and as Ni > Cr > Pb > Cu > Co > Zn > Cd in LD city. In MD city, a similar order as HD city was observed, although the Zn place is inverted with Co. All metals showed highest hazard quotients (HQ) for adults and children at HD city, except for Pb and Zn, which was higher at MD city.
Comparing results of hazard quotient for inhalation exposure from particle size below 75 and PM10 (Tables 1, 2), it can be observed that in adults, the hazard quotient derived to inhalation of trace metals was slightly higher for all the metals in the 10 μm fraction for the soil samples in HD and LD city and road dust of MD city.
Regarding children, the main difference between 10- and <75-μm fractions was observed for the Pb hazard quotient in MD city which presented one order of magnitude higher in PM10. In the same way as adults, Zn, Cu, Cr, Co and Ni showed slight increments in the 10-μm fraction for soil samples at HD city, road dust samples in LD city, and both the soil/dust in MD city.
Cancer risk (CR) values calculated for PM10 decrease in the soil samples as Co > Ni > Cr > Cd in HD, MD, and LD showing Co in HD city the highest CR value. In road dust samples, the CR values decrease as Co > Cr > Ni > Cd in MD and LD cities, whereas in HD city showed similar distribution to the soil. In both type of samples, CR values never reached the accepted maximum range values (10−4–10−6), suggesting noncancer effects in the exposed population.
Comparing CR results from PM10 and the <75-μm fraction showed that both fractions are in the same order of magnitude, except Cd and Cr in the road dust from the MD city, which was one order of magnitude higher than in the fraction <75 μm. Also, Cd and Cr showed values slightly high in the PM10 fraction for the soil and road dust of HD and LD cities despite being in the same order of magnitude. Contrary, Ni and Co showed slightly lower values in the PM10 fraction, especially in the HD city.
Conclusions
The predominance of fine particles sizes (<75 μm and PM10) in soil samples and the link to a major concentration of metals showed that this soil represents a higher risk for human health. However, dust samples have been shown to be the most hazardous, because dust is more prone to accumulate trace metals than soil (Acosta et al. 2015). Consequently, major HI values were reported.
The health risk analysis of the fine particles showed that the most hazardous exposure route was ingestion, followed by dermal absorption and inhalation for all metals except Ni. Therefore, the inhalation exposure route is relevant as shown by the HQ for the inhalation route (HQinh) in both fractions (<75 μm and PM10). Results from the HQ showed that the risk for children due to exposure to ingestion and dermal absorption pathways is higher than for adults, whereas the HI for noncancer trace metals pointed to Zn, Cr, and Ni as the most hazardous trace metals at the studied urban sites.
The largest risk index values and the highest concentrations of metals were found in road dust, indicating that road dust is acting as a sink of metals and a source of potential hazard for human health. Fortunately, the Hazard Index and the Cancer Risk Index showed that the exposure to the soil and road dust for children and adults at studied sites is not a cause enough to induce harmful health effects.
Particulate matter below 10 μm (PM10) reported slightly higher values of inhalation HQ than the fine fraction (<75 μm), which suggests that metals in PM10 must be monitored in urban areas to evaluate the metal affect on human health. However, because some factors, such as weather conditions (especially wind) or the feet action of people walking, could mobilize respirable particles (larger than PM10), monitoring fractions <75 μm can help to evaluate the health risk in urban environments.
Results from hazardous equations should be taken carefully because of the uncertainties that influence them. Despite this, the human health risk model is a useful tool to supply the government to identify the elements and the pathways more relevant in urban sites and to develop the most suitable actions as remedial responses or feasibility studies.
References
Acosta JA, Faz A, Arocena JM, Debela F, Martínez-Martínez S (2009) Distribution of metals in soil particle size fractions and its implication to risk assessment of playgrounds in Murcia City (Spain). Geoderma 149:101–109
Acosta JA, Faz A, Kalbitz K, Jansen B, Martinez-Martinez S (2011) Heavy metal concentrations in particle size fractions from street dust of Murcia (Spain) as the basis for risk assessment. J Environ Monit 13:3087–3092
Acosta JA, Gabarrón M, Faz A, Martínez-Martínez S, Zornoza R, Arocena JM (2015) Influence of population density on the concentration and speciation of metals in the soil and street dust from urban areas. Chemosphere 134:328–337
Amato F, Pandolfi M, Viana M, Querol X, Alastuey A, Moreno T (2009) Spatial and chemical patterns of PM10 in road dust deposited in urban environment. Atmos Environ 43:1650–1659
Boisa N, Entwistle J, Dean JR (2014) A new simple, low-cost approach for generation of the PM10 fraction from soil and related materials: application to human health risk assessment. Anal Chim Acta 852:97–104
Cao Z, Yang Y, Lu J, Zhang C (2011) Atmospheric particle characterization, distribution, and deposition in Xi’an, Shaanxi Province, Central China. Environ Pollut 159:577–584
Chen H, Teng Y, Lu S, Wang Y, Wu J, Wang J (2016) Source apportionment and health risk assessment of trace metals in surface soils of Beijing metropolitan, China. Chemosphere 144:1002–1011
De Miguel E, Jimenez de Grado J, Llamas JF, Martin-Dorado A, Mazadiego LF (1998) The overlooked contribution of compost application of the trace element load in the urban soil of Madrid (Spain). Sci Total Environ 215:113–122
De Miguel E, Iribarren I, Chacón E, Ordoñez A, Charlesworth S (2007) Risk-based evaluation of the exposure of children to trace elements in playgrounds in Madrid (Spain). Chemosphere 66:505–513
Dehghani S, Moore F, Keshavarzi B, Hale BA (2017) Health risk implications of potentially toxic metals in street dust and surface soil of Tehran, Iran. Ecotoxicol Environ Saf 136:92–103
Du Y, Gao B, Zhou H, Ju X, Hao H, Yin S (2013) Health risk assessment of heavy metals in road dusts in urban parks of Beijing, China. Proc Environ Sci 18:299–309
Duong TT, Lee BK (2011) Determining contamination level of heavy metals in road dust from busy traffic areas with different characteristics. J Environ Manag 92:554–562
Ferreira-Baptista L, De Miguel E (2005) Geochemistry and risk assessment of Street dust in Luanda, Angola: a tropical urban environment. Atmos Environ 39:4501–4512
García-Rico L, Meza-Figueroa D, Gandolfi A, Del Rio-salas R, Romero F, Meza-Montenegro MM (2016) Dust-metal sources in an urbanized arid zone: implications for health-Risk assessment. Arch Environ Contam Toxicol 70:522–533
Gope M, Masto RE, George J, Hoque RR, Balachandran S (2017) Bioavailability and health risk of some potentially toxic elements (Cd, Cu, Pb and Zn) in street dust of Asansol, India. Ecotoxicol Environ Saf 138:231–241
Han Y, Cao J, Posmentier E, Fung K, Tian H, An Z (2008) Particulate-associated potentially harmful elements in urban road dusts in Xi’an, China. Appl Geochem 23:835–845
Hou Q, An X, Tao Y, Sun Z (2016) Assessment of resident’s exposure level and health economic costs of PM10 in Beijing from 2008 to 2012. Sci Total Environ 563–564:557–565
Huang J, Liu W, Zeng W, Li F, Huang X, Gu Y, Shi L, Shi Y, Wan J (2016) An exploration of spatial human health risk assessment of soil toxic metals under different land uses using sequential indicator simulation. Ecotoxicol Environ Saf 129:199–209
Izquierdo M, De Miguel E, Ortega MF, Mingot J (2015) Bioaccessibility of metals and human health risk assessment in community urban gardens. Chemosphere 135:312–318
Kong S, Lu B, Ji Y, Zhao X, Chen L, Li Z, Han B, Bai Z (2011) Levels, risk assessment and sources of PM10 fraction heavy metals in four types dust from a coal-based city. Microchem J 98:280–290
Li H, Qian X, Hu W, Wang Y, Gao H (2013) Chemical speciation and human health risk of trace metals in urban street dusts from a metropolitan city, Nanjing, SE China. Sci Total Environ 456–457:212–221
Li H-H, Chen L-J, Yu L, Guo Z-B, Shan C-Q, Lin J-Q, Gu Y-G, Yang Z-B, Yang Y-X, Shao J-R, Zhu X-M, Cheng Z (2017a) Pollution characteristics and risk assessment of human exposure to oral bioaccessibility of heavy metals via urban street dusts from different functional areas in Chengdu, China. Sci Total Environ 586:1076–1084
Li HX, Ji HB, Shi CJ, Gao Y, Zhang Y, Xu XY, Ding HJ, Tang L, Xing YX (2017b) Distribution of heavy metals and metalloids in bulk and particle size fractions of soils from coal-mine brownfield and implications on human health. Chemosphere 172:505–515
Lim H, Lee J, Chon H, Sager M (2008) Heavy metal contamination and health risk assessment in the vicinity of the abandoned Songche on Au–Ag mine in Korea. J Geochem Explor 96:223–230
Liu E, Yan T, Birch G, Zh Y (2014) Pollution and health risk of potentially toxic metals in urban road dust in Nanjing, a mega-city of China. Sci Total Environ 476–477:522–531
Ljung K, Torin A, Smirk M, Maley F, Cook A, Weinstein P (2008) Extracting dust from soil: a simple solution to a tricky task. Sci Total Environ 407:589–593
Lu X, Wu X, Wang Y, Chen H, Gao P, Fu Y (2014) Risk assessment of toxic metals in street dust from a medium-sized industrial city of China. Ecotox Environ Saf 106:154–163
Luo XS, Xue Y, Wang YL, Cang L, Xu B, Ding J (2015) Source identification and apportionment of heavy metals in urban soil profiles. Chemosphere 127:152–157
Porta J, López-Acevedo M, Roquero C (1999) Edafología para la agricultura y el medio ambiente, 2 Edición. Ediciones Mundi-Prensa, Madrid, España
Qin JH, Nworie OE, Lin CX (2016) Particle size effects on bioaccessible amounts of ingestible soil-borne toxic elements. Chemosphere 159:442–448
RAIS-The Risk Assessment Information System (2016) https://rais.ornl.gov/tools/tox_profiles.html. Accessed April 2016
Risser JA, Baker DE (1990) Testing soils for toxic metals. In: Westerman RL (ed) Soil testing and plant analysis. Special Publication, 3.3rd edn. Soil Science Society of America, Madison, pp 275–298
Shi G, Chen Z, Xu S, Zhang J, Wang L, Bi C, Teng J (2008) Potentially toxic metal contamination of urban soils and roadside dust in Shanghai, China. Environ Pollut 156:251–260
Sun Y, Zhou Q, Xie X, Liu R (2010) Spatial, sources and risk assessment of heavy metal contamination of urban soils in typical regions of Shenyang, China. J Hazard Mater 174:455–462
Tang Y, Han G (2017) Characteristics of major elements and heavy metals in atmospheric dust in Beijing, China. J Geochem Explor 176:114–119
Teng Y, Li J, Wu J, Lu S, Wang Y, Chen H (2015) Environmental distribution and associated human health risk due to trace elements and organic compounds in soil in Jiangxi province, China. Ecotoxicol Environ Saf 122:406–416
US-EPA (1986) Superfund public health evaluation manual. Office of Emergency and Remedial Response. U.S. Environmental Protection Agency Washington, 20460. EPA/540/1-86/060
US-EPA (1989) Risk assessment guidance for superfund volume I human health evaluation manual (Part A). Office of Emergency and Remedial Response. U.S. Environmental Protection Agency Washington, 20450. EPA/540/1-89/002
US-EPA (1992a) Guidelines for exposure assessment. Risk Assessment Forum. U.S. Environmental Protection Agency Washington, EPA/600/Z-92/001
US-EPA (1992b) Supplemental guidance to RAGS: Calculating the Concentration Term. Office of Solid Waste and Emergency Response Washington, 20460. PB92-963373
US-EPA (1996) Soil screening guidance: Technical Background Document. Office of Solid Waste and Emergency Response. Washington, 20460. EPA/540/R95/128
US-EPA (2002a) Supplemental guidance for developing soil screening levels for superfund sites. Office of Solid Waste and Emergency Response. OSWER 9355.4-24
US-EPA (2002b) Calculating upper confidence limits for exposure point concentrations at hazardous waste sites. Office of Emergency and Remedial Response U.S. Environmental Protection Agency Washington, 20460. OSWER 9285.6-10
US-EPA (2004) Risk assessment guidance for superfund volume I: human health evaluation manual (Part E, Supplemental Guidance for Dermal Risk Assessment). Office of Superfund Remediation and Technology Innovation U.S. Environmental Protection Agency Washington, EPA/540/R/99/005
US-EPA (2009) Integrated science assessment for particulate matter. National Center for Environmental Assessment-RTP Division. Office of Research and Development. U.S. Environmental Protection Agency. Research Triangle Park, EPA/600/R-08/139F
US-EPA (2011a) Exposure factors handbook: 2011 edition. National Center for Environmental Assessment Office of Research and Development U.S. Environmental Protection Agency Washington, 20460. EPA/600/R-09/052F
US-EPA (2011b) Highlights of the exposure factors handbook. National Center for Environmental Assessment.Office of Research and Development, Washington, 20460. EPA/600/R-10/030
US-EPA (2016a) in: https://www.epa.gov/risk/human-health-risk-assessment. Accessed April 2016
US-EPA (2016b) https://www3.epa.gov/pm/health.html. Accessed April 2016
Van der Berg R (1995) Human exposure to soil contamination: a qualitative and quantitative analysis towards proposal for human toxicological intervention values. Report no. 725201011. National institute of Public Health and Environmental protection. Bilthoven
Wang J, Li S, Cui X, Li H, Qian X, Wang C, Sun Y (2016) Bioaccessibility, sources and health risk assessment of trace metals in urban park dust in Nanjing, Southeast China. Ecotoxicol Environ Saf 128:161–170
Wong CSC, Li X, Thornton I (2006) Urban environmental geochemistry of trace metals. Environ Pollut 142:1–16
Zhang C, Qiao Q, Appel E, Huang B (2012) Discriminating sources of anthropogenic heavy metals in urban street dusts using magnetic and chemical methods. J Geochem Explor 119–120:60–75
Acknowledgements
Financial support to conduct this study was provided by the Fundación Séneca of Comunidad Autónoma de Murcia (Spain).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Gabarrón, M., Faz, A. & Acosta, J.A. Soil or Dust for Health Risk Assessment Studies in Urban Environment. Arch Environ Contam Toxicol 73, 442–455 (2017). https://doi.org/10.1007/s00244-017-0413-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00244-017-0413-x