
Abstract
We aimed to investigate the efficacy of two different doses of doxazosin, 4 and 8 mg, in medical expulsive therapy (MET). This prospective randomized study included a total of 66 patients with distal ureteral stones which were radio-opaque and ≤10 mm. All patients were randomly divided into three groups: Group 1 included 25 patients receiving 4 mg doxazosin. Group 2 included 22 patients receiving 8 mg doxazosin. Diclofenac 100 mg p.o. and daily 1500–2000 cc hydration were advised to the patients in Groups 1 and 2 to relieve pain. Group 3 consisted of 19 patients who were defined as control group and received only hydration and analgesics. The mean age of the patients was 30 ± 7.6, 37.9 ± 11.5 and 33 ± 11.3 in Group 1, Group 2 and Group 3, respectively. The mean stone size was 6.6 ± 1.4, 7.1 ± 1.5 and 6.6 ± 1.5 in Group 1, Group 2 and Group 3, respectively. The stone expulsion rate of the patient groups was 18/25 (72 %), 15/22 (68.1 %) and 5/19 (25.3 %). There were significantly fewer pain episodes and lower analgesic requirement in Groups 1 and 2 (p = 0.021). However, the difference between Group 1 and Group 2 was non-significant (p = 0.207). Given the data of the present study, doxazosin, an alpha receptor blocker, exhibited equal efficacy with 4 or 8 mg doses in MET and was used safely and efficiently in ureteral stones <10 mm. The findings of the present study showed that 4 mg dose is effective, when doxazosin is preferred for MET.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ureteral stones usually present with acute upper urinary system obstruction and associated pain, and, thus, mostly require rapid stone clearance contrary to the renal stones [1]. Medical expulsive therapy (MET) has entered the urology practice in the past decade for medical treatment of ureteral stones. It is a treatment modality which aims at facilitating the passage of ureteral stones with the possibility of spontaneous passage and minimizing potential pain and additional complication rate during this process. However, the question is which stones have the possibility of spontaneous passage. In addition to the factors such as stone localization, urinary anatomy, renal reserve and fluid intake, the most important factor affecting the spontaneous passage of the ureteral stones is the stone size. Early studies demonstrated that 95 % of stones <4 mm were likely to pass spontaneously during a 40-day follow-up period [2]. A meta-analysis, in turn, showed that the spontaneous passage possibility of stones <5 mm was 68 %, whereas this rate decreased to 47 % for stones >5 mm [3]. Briefly, the main goal of MET is to minimize pain episodes and to prevent infection and renal function impairment during follow-up, as well as to facilitate the spontaneous passage of the stones.
Review of the literature revealed that corticosteroids, prostaglandin inhibitors, and neuromuscular blockers were previously used in the treatment of MET; however, alpha-blockers and calcium channel blockers have been widely adopted recently. Although the literature also contains inconsistent results on whether alpha-blockers or calcium channel blockers are more effective, it is mostly considered that alpha-blockers are more effective than the others [4].
Although literature contains data on doxazosin use for MET purposes, almost all used a 4-mg investigational dose. In this study, we aimed to investigate the efficacy of two different doses of doxazosin, 4 and 8 mg, in MET.
Materials and methods
This prospective randomized study included a total of 66 patients with distal ureteral stones which were radio-opaque and ≤10 mm between December 2013 and June 2015. The study protocol was approved by the Ethics Committee of Gaziantep University (Date/No.: 03.04.2012/145).
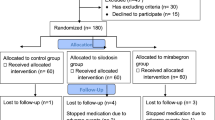
All patients were randomly divided into three groups. Group 1 included 25 patients receiving 4 mg doxazosin. Group 2 included 22 patients receiving 8 mg doxazosin. Diclofenac 100 mg p.o. and daily 1500–2000 cc hydration were given to the patients in Groups 1 and 2 to relieve pain. Group 3 consisted of 19 patients who were defined as the control group and received only hydration and analgesics. The study duration was determined as up to 3 weeks. All patients had routine biochemistry tests and urine cultures and antibiograms on admission. The presence of the ureteral stones was assessed using the direct urinary system graphy, urinary system ultrasonography, and intravenous pyelography or unenhanced computed tomography (CT). The patients were informed about the complications which might occur during the study and provided written consent forms. The patients with additional stones in kidney, urinary system anatomic abnormality, previous urinary system surgery, severe hydronephrosis or extreme symptoms, high serum levels of urea creatinine, diuretic or calcium channel blocker use and doxazosin hypersensitivity were excluded from the study.
All patients underwent a weekly assessment on a regular basis. During such controls, medical history was obtained and pain episodes and the amount of analgesics used were noted. Physical examinations were performed and vital signs (i.e., body temperature, pulse rate, and blood pressure) were recorded. Complete urinalysis, urine culture tests, and radiological assessments were repeated. We performed unenhanced CT only before the MET. If a stone was not visible on plain radiography during follow-up, patients were considered stone free with urinary system ultrasonography by an experienced radiologist. Unenhanced CT was performed only in case of any suspicion.
The study discontinuation criteria were defined as hypersensitivity to the agents used, advanced hydronephrosis, persistent pain despite proper and adequate analgesic use, urinary tract infection, and low blood pressure. The patients who were unable to pass the stone by the end of 3 weeks underwent ureterorenoscopy to achieve a stone-free status.
Statistical analysis
Randomization was performed with the MedCalc statistical software (MedCalc, 14.10.2; MedCalc, Belgium). All statistical analyses were made using the SPSS version 11.5 (SPSS Inc., Chicago, IL, USA). The Mann–Whitney U test was used to compare age, stone size, expulsion time, and pain episodes among the groups. The Chi square and Fisher’s exact tests were used to compare the success rates among the groups. Descriptive data were expressed in the mean ± standard deviation. A p value of <0.05 was considered to be statistically significant.
We planned a study of independent cases and controls with one control(s) per case. Our data indicate that the success rate among 4 mg intervention is 0.72 and rate for experimental subjects is 0.68; we would need to study 2060 experimental subjects and 2060 control subjects to be able to reject the null hypothesis that the success rates for experimental and control subjects are equal with probability (power) 0.8. The type I error probability associated with this test of this null hypothesis is 0.05.
Results
The mean age (median age) of the patients was 30 ± 7.6 (29) in group 1, 37.9 ± 11.5 (36) in group 2 and 33 ± 11.3 (33) in group 3. The mean stone transverse size (median) was 5.5 ± 0.9 (6.0), 6.3 ± 1.2 (6.5) and 6.0 ± 1.1 (7.0) in Group 1, Group 2 and Group 3, respectively. The stone expulsion rate of the patient groups was 18/25 (72 %), 15/22 (68.1 %) and 5/19 (25.3 %). The demographic and clinical characteristics of all groups are listed in Table 1.
Hydronephrosis and concomitant urinary infection developed in two patients in both Group 1 and Group 2 and hydronephrosis developed in five patients in Group 3 during the weekly patient assessment and, therefore, endoscopic surgical treatment was administered.
Nausea and vomiting as a doxazosin-related side effect occurred in three patients in Group 1 and four patients in Group 2, and drug-related hypotension occurred in two patients in Group 1 and one patient in Group 2. The study drug was discontinued and ureterorenoscopy was performed in these patients. At the end of a 3-week follow-up period, the stone expulsion rate was 18/25 (72 %) in Group 1, 15/22 (68.1 %) in Group 2 and 5/19 (25.3 %) in Group 3. Intragroup comparisons revealed no significant difference in the stone expulsion rates between doxazosin 4 mg and 8 mg (p = 0.307). When the group who did not receive any MET was compared individually with the groups receiving 4 and 8 mg doxazosin, doxazosin was found to be statistically significantly effective in the stone expulsion (p = 0.02). Stone expulsion rates are presented in Table 2.
The time from the first episodes of renal colic was 0.9 ± 0.4, 0.9 ± 0.5 and 1.2 ± 0.5 in Group 1, Group 2 and Group 3, respectively. In addition, there were significantly fewer pain episodes and lower analgesic requirement in Groups 1 and 2 (p = 0.021). However, the difference between Group 1 and Group 2 was non-significant (p = 0.207). The stone expulsion time and number of pain episodes of groups are also presented in Table 2.
Discussion
In the early treatment models for helping the expulsion of ureteral stones, methods such as anti-emetics, analgesics and increased fluid intake were tried to facilitate the stone passage. The revelation of the structure of the adrenergic receptors and the physiology of the smooth muscles in ureters has enlightened the development of targeted treatment [5].
Although the studies conducted upon the understanding of the role of the sympathetic nervous system in the contraction of ureteral smooth muscles demonstrated alpha adrenergic receptors in all ureteral segments, these receptors were shown to be present in the distal ureter most intensely [6].
With the blockage of this type of receptors, tonic propulsive contractions continue, while basal smooth muscle tonus and irregular excessive peristalsis frequency are reduced. Therefore, the stone passage toward the distal is achieved without inhibiting the physiological tonic propulsive contractions required for making the ureter reach the bladder. Alpha-blockers and calcium channel blockers have been demonstrated to have benefits in animal models and entered into daily practice upon the revelation of their positive effects in several subsequent randomized studies [7, 8].
Considering that the edema in the stone localization makes expulsion difficult, the use of glucocorticoid in MET has been introduced. Glucocorticoids are likely to prevent edema and inflammatory response caused by the stone by inhibiting prostaglandin release. There are reports showing that the combination of glucocorticoids and alpha-blockers help stone passage in clinical studies [9, 10]. Kumar et al. [11] used the combination of tamsulosin and naftopidil, which are alpha 1 receptor antagonists, with prednisolone in a series of 120 patients and reported a higher rate of stone expulsion in the alpha-blocker + prednisolone groups compared to the observation group. However, it has not attracted many supporters considering the potential side effects of glucocorticoid use (i.e., elevated blood glucose, gastric ulcer, adrenal insufficiency).
Almost all alpha-blockers have been used in MET and a study reported that tamsulosin facilitates stone expulsion with a success rate of 77.3 %, terazosin with 78.5 % and doxazosin with 75.8 % [12].
In the literature, Pickard et al. [13] and Fruyk et al. [14] found no benefit overall of 0.4 mg of tamsulosin daily for patients with distal ureteric calculi less than or equal to 10 mm in terms of spontaneous passage, time to stone passage, pain or analgesia requirements. In the subgroup with large stones (5–10 mm), tamsulosin did increase passage and should be considered. In our study, the stone size of patients was less than 10 mm. Our data showed that the use of doxazosin (4 or 8 mg) in patients with ureteral calculi located in the distal ureter might be sufficient in increasing the spontaneous passage of these calculi.
There are studies reporting the use of doxazosin, which is also used in the present study, as a single dose of 2 mg to investigate the efficacy in MET. Among these, Zehri et al. [15], who used 2 mg doxazosin and diclofenac in their series of 65 patients with a 4–7 mm size in the distal ureter and followed-up for a maximum of 28 days, reported that doxazosin combined with an analgesic provided considerable contribution to stone expulsion and minimization of colic. Again, the said study indicated that alpha-blockers are an important part of conservative treatment in patients with ureteral stone <7 mm.
The present study is of utmost importance, as it is the first and single study conducted on MET with two different doses of doxazosin. In addition, as in the study by Zehri et al. [15], it was found to be statistically significant in facilitating stone expulsion and minimizing colic number regardless of doxazosin dose. Any significant result was not produced also in side effect profile and statistically insignificant side effects occurred such as nausea, vomiting and hypotension at the minimum level.
In MET, alpha doxazosin has not been only used in adults, but also in children although the number is limited. In a study, Erturhan et al. [16] randomized patients into two groups of ibuprofen (20 mg/kg/day, divided into 2 equal doses) and ibuprofen + doxazosin (0.03 mg/kg/day, once daily). The stone expulsion rate was 28.5 % in the group administered ibuprofen alone, whereas this rate was 70.8 % in the combined group. Another study conducted in pediatrics demonstrated a stone expulsion rate of 70 % with doxazosin in small lower ureteral stones [17]. The present study included adult patients and doxazosin, regardless of the dose, can be considered effective and safe as it is in the previous pediatric patient series.
The literature contains various data on treatment duration in MET. Miller et al. [18] suggested that MET was allowed to be delayed 6 weeks for stone expulsion. In the present study, we defined the duration as 3 weeks and stone-free status was achieved using ureteroscopy in patients without stone expulsion by the end of such duration.
This study has certain limitations. There was no allocation and the investigators were not blinded to the therapy of the patient. In addition, the study has relatively small sample size on post-power analyses.
Conclusion
Given the data of the present study, doxazosin, an alpha receptor blocker, exhibited equal efficacy with 4 or 8 mg doses in MET and was used safely and efficiently in ureteral stones <10 mm. The findings of the present study showed that 4 mg dose is effective, when doxazosin is preferred for MET. The drug-specific side effects of doxazosin are within acceptable limits and keeps its place as an option in MET by positively affecting stone expulsion in proper patient groups and minimizing pain episodes and thereby analgesic requirement.
References
Hollingsworth JM, Norton EC, Kaufman SR et al (2013) Medical expulsive therapy versus early endoscopic stone removal for acute renal colic: an instrumental variable analysis. J Urol 190:882–887
Preminger GM, Tiselius HG, Assimos DG et al (2007) EAU/AUA nephrolithiasis guideline panel. Guidelines on urolithiasis. J Urol 178(6):2418–2434
Preminger GM, Tiselius HG, Assimos DG et al (2007) American Urological Association Education and Research, Inc; European Association of Urology. 2007 Guideline for the management of ureteral calculi. Eur Urol 52(6):1610–1631
Preminger GM, Tiselius HG, Assimos DG et al (2007) Guideline for the management ureteral calculi. J Urol 178:2418–2434
Malin JM Jr, Deane RF, Boyarsky S (1970) Characterisation of adrenergic receptors in human ureter. Br J Urol 42:171–174
Salehi M, Fouladi MM, Shiery H et al (2005) Does methylprednisolone acetate increase the success rate of medical therapy for passing distal üreteral stones? Eur Urol Suppl 4(3):25
Porpiglia F, Destefanis P, Fioric C et al (2000) Effectiveness of nifedipine and deflazacort in management of distal ureter Stones. Urology 56:579–582
Itoh Y, Kojima Y, Yasui T et al (2007) Examination of alpha 1 adrenoceptor subtypes in the human ureter. Int J Urol 14:749–753
Laird JM, Roza C, Cervero F (1997) Effects of artificial calculosis on rat ureter motility: peripheral contribution to the pain of ureteric colic. Am J Physiol 272:R1409–R1416
Maggi CA, Giuliani S (1995) A pharmacological analysis of calcium channels involved in phasic and tonic responses of the guinea-pig ureter to high potassium. J Auton Pharmacol 15:55–64
Kumar S, Kurdia KC, Ganesamoni R et al (2013) Randomized controlled trial to comparing the efficacy of naftopidil and tamsulosin as medical expulsive therapy in combination with prednisolone for distal ureteral Stones. Korean J Urol 54(5):311–315
Yılmaz E, Batislam E, Basar MM et al (2005) The comparison and efficacy of 3 different alpha1-adrenergic blockers for distal ureteral stones. J Urol 176(6):2010–2012
Pickard R, Starr K, MacLennan G et al (2015) Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial. Lancet 25 386(9991):341–349
Furyk JS, Chu K, Banks C et al (2016) Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized, multicenter trial. Ann Emerg Med 67(1):86–95
Zehri AA, Ather MH, Abbas F et al (2010) Preliminary study of efficacy of doxazosin as a medical expulsive therapy of distal ureteric Stones in a randomized clinical trial. Urology 75(6):1285–1288
Erturhan S, Bayrak O, Sarıca K et al (2013) Efficacy of medical expulsive treatment with doxazosin in pediatric patients. Urology 81(3):640–643
Aydogdu O, Burgu B, Gucuk A et al (2009) Effectiveness of doxazosin in treatment of distal ureter Stones in children. J Urol 182(6):2880–2884
Miller OF, Kane CJ (1999) Time to stone passage for observed ureteral calculi: a guide for patient education. J Urol 162:688–690
Acknowledgments
Thanks to Elzem Sen for final language revision.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflict of interest.
Ethical standards
All studies have been approved by the appropriate ethics committee and have, therefore, been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All persons gave their informed consent prior to their inclusion in the study. This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Sen, H., Erturhan, S., Sadioglu, E. et al. A comparison of efficacy of doxazosin 4 and 8 mg in medical expulsive therapy of distal ureteral stones: a prospective randomized clinical trial. Urolithiasis 45, 461–464 (2017). https://doi.org/10.1007/s00240-016-0927-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-016-0927-0