
Abstract
Cushing’s disease manifests as symptoms of glucocorticoid excess secondary to the increased secretion of corticotropin by a corticotroph adenoma in the pituitary gland. Unfortunately, magnetic resonance imaging (MRI) performed at conventional clinical field strengths of 1.5 or 3 Tesla has limited sensitivity for the detection of these pituitary tumors, and radiologic uncertainty often necessitates more invasive workup to confirm diagnosis and guide resection. It has been postulated that higher static magnetic field strengths may increase the adenoma detection rate and thus the utility of MRI for this clinical application. In this report, we describe our initial experience using ultra-high field 7 Tesla (7 T) MRI in patients with suspected Cushing’s disease and negative or equivocal imaging at conventional field strengths. We performed contrast-enhanced 7 T pituitary MRI in 10 patients with up to three different T1-weighted sequences and correlated the imaging abnormalities identified with results of histologic evaluation in patients who subsequently underwent resection. We found that 7 T MRI enabled the identification of previously undetected areas of focal pituitary hypoenhancement in 9 patients (90%), of which 7 corresponded histologically to corticotroph adenomas. These early findings suggest an important adjunctive role for ultra-high field MR imaging in the noninvasive clinical workup of suspected Cushing’s disease.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Purpose
Cushing’s disease (CD) is caused by the increased secretion of adrenocorticotropic hormone (ACTH or corticotropin) from the anterior pituitary gland. If corticotropin-dependent Cushing’s syndrome is determined and ectopic corticotropin syndrome has been excluded, MRI of the pituitary gland is performed to assess for an adenoma causing CD. However, up to 40% of patients with CD have tumors undetectable by conventional MRI [1], and more invasive techniques such as inferior petrosal sinus sampling (IPSS) may be needed to localize the tumor [2], exposing the patient to endovascular procedural risks including bleeding, infection, and stroke.
Ultra-high field MRI, performed at static field strengths of 7 T or higher, provides improved signal-to-noise and contrast-to-noise characteristics compared with conventional MRI performed on 3 T or 1.5 T systems [3]. A recent case report has suggested that 7 T imaging may provide increased sensitivity for pituitary adenomas causing CD [4], with implications for reducing the potential morbidity associated with IPSS and accurately directing pituitary surgery. In this brief report, we detail our initial experience with 7 T pituitary MRI in a series of 8 patients, describe 7 T pituitary T1-weighted imaging sequence parameters, and evaluate the diagnostic performance of these ultra-high field MR sequences in the localization of corticotropin-secreting pituitary adenomas.
Methods
We prospectively identified outpatients presenting with symptoms of cortisol excess and enrolled individuals who fulfilled the following criteria: (1) endocrinological diagnosis of ACTH-dependent Cushing syndrome and suspected CD as per societal guidelines [5], (2) prior negative or equivocal conventional field strength pituitary MRI, and (3) absence of contraindications to contrast-enhanced 7 T MRI. The study was approved by our institutional review board, and all patients provided informed consent before undergoing 7 T imaging.
Twelve patients were scanned on a Siemens Terra 7 T system using a Nova Medical 1Tx/32Rx head coil. Pre- and post-contrast (0.2 mL/kg gadoterate meglumine) T1-weighted pituitary sequences included coronal and sagittal 2D TSE (TR = 960 ms, TE = 10 ms, voxel size = 0.2 × 0.2 × 2.0 mm), 3D SPACE (TR = 1200 ms, TE = 12 ms, variable flip angle, voxel size = 0.5 × 0.5 × 0.5 mm), and 3D MPRAGE (TR = 2300 ms, TE = 2.95 ms, flip angle = 7°, voxel size = 0.7 × 0.7 × 0.7 mm). Not all patients were scanned with all sequences due to changes in clinical protocol during the study period. Two patients requested termination of the examination prior to contrast agent administration and were excluded from further analysis.
The 7 T imaging was interpreted initially by a single board-certified neuroradiologist to guide the immediate treatment plan. Retrospectively, to ensure the validity of this report, the images were reviewed by a second neuroradiologist blinded to the initial interpretation and clinical history; there were no discrepancies in lesion detection. Patients in whom a potential adenoma was identified underwent resection, the histologic diagnosis corresponding to the imaging abnormality was recorded, and follow-up endocrinologic evaluations were reviewed for clinical and hormonal remission. One patient without a discrete lesion at 7 T did not undergo surgery, and one patient did not experience hormonal remission following resection of an area of hypoenhancement corresponding histologically to Crooke hyaline change; both of these cases were excluded from the subsequent analysis.
Results
Table 1 summarizes the visualization of focal hypoenhancing pituitary lesions in the 8 patients who completed 7 T MR assessment and experienced disease remission following surgery. The SPACE sequence depicted a lesion in all 8 patients, the mean size of these detected lesions was 6.0 mm (range 3.9–7.6 mm), and 7 of the 8 identified lesions (88%) were histologically consistent with corticotroph adenomas. The MPRAGE sequence identified a lesion in 4 out of 5 cases (80%), with mean lesion diameter 6.4 mm (range 5.5–7.4 mm), and all 4 of these lesions were found to correspond to corticotroph adenomas. The TSE sequence revealed a lesion in 3 out of 4 patients (75%), with a mean lesion size of 5.9 mm (range 4.0–7.2 mm), and all 3 of these lesions were histologically consistent with corticotroph adenomas. One corticotroph adenoma also exhibited components of prolactinoma. Overall, 7 of the 8 resected lesions in patients experiencing post-surgical disease remission demonstrated a component of corticotroph adenoma; the histological examination in the remaining case revealed Crooke hyaline change; however, the subsequent clinical response nevertheless favors a diagnosis of CD in this case.
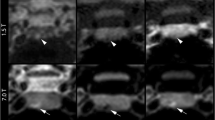
Figure 1 provides a representative illustration of the sellar contents in one patient (patient 5 from Table 1) as visualized by the contrast-enhanced SPACE (panel a), MPRAGE (panel b), and TSE (panel c) 7 T sequences used in this study. These coronal images all depict a hypoenhancing lesion in the right aspect of the gland with varying degrees of conspicuity. A 3 T TSE image of the same patient is also shown (panel d) which fails to demonstrate a lesion in the same region.

Contrast-enhanced MRI of the pituitary gland in patient 5 from Table 1 with a 7 T SPACE, b 7 T MPRAGE, c 7 T TSE, and d 3 T TSE sequences. Arrowheads indicate focal hypoenhancing regions in the right aspect of the gland visualized at 7 T field strength only. Images are cropped and scaled for size similarity and window level and center tuned for optimal lesion conspicuity
Conclusions
This initial work has demonstrated the effectiveness of 7 T MRI for localizing pituitary adenomas in patients with suspected Cushing’s disease and negative or equivocal conventional imaging. Despite the limitations introduced by the accentuated physiologically induced B0 field and coil-related B1 field inhomogeneities at 7 T [3], careful inspection and correlation between multiple sequences enables successful adenoma localization in the majority of cases. The strengths of 7 T imaging include improvements in both spatial and contrast resolution, but given the minimum lesion size of 3.9 mm in this series, we infer that contrast resolution may be the primary driver of the increased detection rate. Preliminarily, the three T1-weighted sequences described herein appear similar in diagnostic performance, and larger-scale analysis will be needed to determine the optimal choice. We note that despite the improvement in lesion detection, our data reveals that perfect sensitivity and specificity of MRI for corticotroph adenomas remain elusive even at 7 T field strength, highlighting the continuing challenges in the noninvasive diagnosis of CD. Ultimately, however, we expect accuracy to improve with refinement of technique and the clinical deployment of parallel transmission technology [6], establishing the role of 7 T MRI as an adjunctive tool for localizing corticotropin-secreting adenomas in cases of suspected CD.
References
Newell-Price J, Bertagna X, Grossman AB, Nieman LK (2006) Cushing's syndrome. Lancet 367:1605–1617. https://doi.org/10.1016/S0140-6736(06)68699-6
Deipolyi A, Karaosmanoğlu A, Habito C, Brannan S, Wicky S, Hirsch J, Oklu R (2012) The role of bilateral inferior petrosal sinus sampling in the diagnostic evaluation of Cushing syndrome. Diagn Interv Radiol 18:132–138. https://doi.org/10.4261/1305-3825.DIR.4279-11.0
Trattnig S, Springer E, Bogner W, Hangel G, Strasser B, Dymerska B, Cardoso PL, Robinson SD (2018) Key clinical benefits of neuroimaging at 7T. Neuroimage 168:477–489. https://doi.org/10.1016/j.neuroimage.2016.11.031
Law M, Wang R, Liu CJ et al (2018) Value of pituitary gland MRI at 7 T in Cushing’s disease and relationship to inferior petrosal sinus sampling: case report. J Neurosurg 130:347–351. https://doi.org/10.3171/2017.9.JNS171969
Nieman LK, Biller BM, Findling J, Newell-Price J, Savage MO, Stewart PM, Montori VM (2008) The diagnosis of Cushing’s syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 93:1526–1540. https://doi.org/10.1210/jc.2008-0125
Padormo F, Beqiri A, Hajnal JV, Malik SJ (2016) Parallel transmission for ultrahigh-field imaging. NMR Biomed 29:1145–1161. https://doi.org/10.1002/nbm.3313
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Patel, V., Liu, CS.J., Shiroishi, M.S. et al. Ultra-high field magnetic resonance imaging for localization of corticotropin-secreting pituitary adenomas. Neuroradiology 62, 1051–1054 (2020). https://doi.org/10.1007/s00234-020-02431-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-020-02431-x