
Abstract
Purpose
Anemia of chronic kidney disease (CKD) has traditionally been treated with recombinant human erythropoietin (rhEPO). Recently, daprodustat, a hypoxia-inducible factor prolyl-hydroxylase inhibitor, has also been shown to increase hematocrit. It remains unclear whether daprodustat or rhEPO should be the treatment of choice for anemia of CKD. We aimed to assess the efficacy and cardiovascular safety of daprodustat versus rhEPO in CKD patients.
Methods
Online databases were queried in April 2022 for articles comparing the efficacy and safety of daprodustat in DD-CKD and NDD-CKD subgroups. Results from trials were pooled using a random-effects model.
Results
Data on 8245 CKD patients from eight clinical trials were included. Our results show that in comparison to rhEPO, daprodustat maintained the same efficacy in increasing hemoglobin levels in both the DD-CKD (MD: 0.10; 95% CI [− 0.13,0.34]; p = 0.50) and NDD-CKD (MD: − 0.01; 95% CI [− 0.38,0.35]; p = 0.95) subgroups. Daprodustat significantly lowered hepcidin levels and significantly increased TIBC in both subgroups. Additionally, daprodustat significantly reduced the incidence of major adverse cardiovascular events (MACE) (RR: 0.89; 95% CI: 0.89–0.98; p = 0.02) and its myocardial infarction (MI) component (RR: 0.74; 95% CI: 0.59–0.92; p = 0.006) in the DD-CKD subgroup.
Conclusion
Daprodustat has similar efficacy compared to rhEPO for the treatment of anemia of CKD. On treatment, the reduced experience of MACE was reported in DD-CKD patients as compared to rhEPO. Furthermore, effects on iron metabolism varied by parameter, with daprodustat being superior to rhEPO in some cases and inferior in others.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
CKD is a highly prevalent condition and the third most rapidly growing cause of mortality worldwide [1, 2]. The 2021 European Society of Cardiology (ESC) guidelines highlighted CVD to be the leading cause of mortality in CKD patients, with poor mortality outcomes being prognosticated even after adjusting for coronary artery disease (CAD) comorbidities, including diabetes mellitus and hypertension [2]. Anemia is a common complication of CKD [3], and the currently recommended recombinant human erythropoietin (rhEPO) or its analogs (erythropoiesis-stimulating agents [ESAs]) and iron supplementation (intravenous and/or oral) [4,5,6] are subject to safety concerns [7] with high dose ESAs being associated with an elevated risk of cardiovascular events and all-cause mortality [7, 8] in anemic patients with CKD.
Daprodustat, a novel hypoxia-inducible factor prolyl hydroxylase inhibitor (HIF-PHI), offers a potential alternative as an erythropoiesis stimulant in both patients with DD-CKD and NDD-CKD. While daprodustat is known to significantly increase hemoglobin levels as compared to placebo [9], its efficacy and cardiovascular safety in comparison to rhEPO remain uncertain, especially considering emerging evidence from new trials.
Recently, a meta-analysis [10] evaluating the cardiovascular safety of this drug revealed that daprodustat did not significantly reduce the risk of the composite cardiovascular outcome as compared to control (placebo or an active comparator, like erythropoietin). However, they did not compare results against rhEPO specifically. Additionally, their analysis was restricted to a single broad composite outcome and individual components namely cardiovascular death, MI, stroke, and hospitalization for heart failure (HHF) decompensation, were not evaluated independently. In addition, the recently published Anemia Studies in CKD: erythropoiesis via a Novel PHI Daprodustat in Incident Dialysis (ASCEND-ID) trial [11] studied the effects of daprodustat in incident dialysis patients Therefore, given the conflicting findings and paucity of evidence, we conducted an updated meta-analysis to evaluate the efficacy and cardiovascular safety of daprodustat in patients with DD-CKD and NDD-CKD in comparison to those of rhEPO.
Material and methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the A Measurement Tool to Assess Systematic Reviews (AMSTAR 2) criteria [12].
Search strategy
A comprehensive database search of MEDLINE (via PubMed), Embase, Scopus, Cochrane Central Register of Controlled Trials (CENTRAL), and International Clinical Trials Registry Platform (ICTRP) was performed on 19 April 2022 to search for all relevant articles between the search date and the conception of the databases, using keywords related to “daprodustat,” “GSK1278863,” and “chronic kidney disease.” Additional studies were identified by manual searching and snowballing by examining the references of narrative reviews, systematic reviews, and meta-analyses done on similar and related topics. Furthermore, all available gray literature was searched, and no time or language restrictions were set. Only relevant randomized controlled trials (RCTs) were considered eligible for inclusion in the study.
Study selection criteria
The inclusion criteria consisted of (1) studies that were RCTs; (2) studies with participants who have CKD and are over the age of 18; (3) studies reporting and/or comparing patient outcomes between rhEPO (epoetins or their biosimilars or darbepoetin) versus daprodustat; (4) studies that assessed at least one of the following outcomes: change in hemoglobin levels, change in iron metabolism parameters (hepcidin, ferritin, transferrin saturation (TSAT), total iron binding capacity (TIBC), and total serum iron (TSI)) and incidence of all-cause mortality, stroke, MI, MACE, and HHF.
The exclusion criteria consisted of (1) studies without a comparison group; (2) studies that involved individuals without chronic kidney disease; (3) studies with data that was neither extractable nor analyzable based on our study aim.
Screening process and data extraction
Two reviewers (W.A. and M.U.M.) independently screened the initially retrieved articles based on titles and abstracts, with all relevant articles undergoing a subsequent full-text review to determine whether they met the study selection criteria mentioned above. Any discrepancies were resolved via consensus or by a third reviewer (A.S.F.). If data were missing from the manuscript or the supplementary files, corresponding authors were contacted to gather additional data. If SD were missing, these were imputed using the average relative standard deviation (RSD) among studies reporting the same outcome. This is calculated by expressing the SD as a percentage of the sample mean. Wherever RSD could not be calculated due to the mean being reported as 0, a mean of the available standard deviations was used to estimate the SD. These approaches are approved by the Cochrane Guide for Systematic Review for use in cases of missing data [13].
Graphical data extraction was performed for studies (where needed) with WebPlotDigitizer version 4.5 [14], which is a free-to-use application employed to accurately extract graphical data. It has been validated and proven to have outstanding inter-rater correlations [15] (> 95%) and has been recommended for use in systematic reviews to extract otherwise inaccessible graphical data.
Extracted parameters
Data extraction was performed by two authors, and inconsistencies were resolved by a third reviewer who referred to the full-text manuscripts of the included articles. Parameters extracted included general article publication information, study participant characteristics, and details regarding change in hemoglobin levels, change in iron metabolism parameters (hepcidin, ferritin, TSAT, TIBC, and TSI), and incidence of all-cause mortality, stroke, MI, MACE, and hospitalization for HHF. For studies that reported the measured outcomes at more than one time-point after the administration of the treatment, the most recent measurement was used.
Quality assessment (risk of bias) and certainty in evidence
The risk of bias in individual studies was assessed using the Cochrane risk-of-bias tool for randomized trials [16], while certainty in evidence was assessed using the GRADE approach [17] using the GRADEpro Software (McMaster University and Evidence Prime Inc, Ontario, Canada). These were done by two reviewers independently (A.A. and M.T.M.), and in case of any disagreements, a third reviewer was consulted (A.S.F.). Publication bias was not assessed for any outcome since our meta-analysis included less than ten studies [13].
Statistical analysis
All meta-analyses were performed using Review Manager version 5.4.1 (the Cochrane Collaboration, Copenhagen, Denmark). In the case of different follow-up intervals or time periods, the value of the most recent available follow-up time point was used for analysis. The pooled measure of effect was reported as risk ratios (RRs) with a 95% confidence interval (CIs) for dichotomous outcomes and as mean differences (MDs) with 95% CIs for continuous outcomes. Forest plots were generated for all meta-analyzed outcomes, with a minimum of two studies being used to meta-analyze an outcome.
Due to variations among the studies, such as differences in the study setting and patient population, we used the Mantel–Haenszel random effects model to report the pooled RRs and the inverse variance random effects model to report the pooled MDs. Heterogeneity was assessed using the Higgins I2 statistic, with an I2 > 50% being considered significant heterogeneity. All p-values were two-sided, and a p-value < 0.05 was considered significant for all analyses. Sensitivity analyses were performed for outcomes by removing one study at a time. Furthermore, subgroup analyses were performed based on whether patients were undergoing dialysis or not.
Results
Literature search
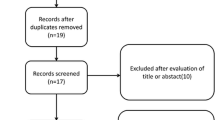
The initial literature search yielded 391 potentially relevant articles. After applying our predetermined eligibility criterion, eight studies [11, 18,19,20,21,22,23,24] were included in this meta-analysis. The PRISMA flow chart (Supplementary Fig. S9.2) depicts the search and study selection process.
Study characteristics and risk of bias assessment
Our shortlisted studies included 8245 patients (51.5% males; mean age, 62 years) with 3839 patients with DD-CKD (daprodustat, 2013; control, 1826) and 4406 patients with NDD-CKD over a median follow-up of 52 weeks. Supplementary Table S9.1 outlines the baseline characteristics of included studies. All our included studies had an overall minimal risk of bias (Supplementary Figs. S2.1 and S2.2).
Effects on hemoglobin level
This outcome was reported by all eight studies (Fig. 1).

Forest plot displaying the effects of daprodustat vs rhEPO on hemoglobin levels of patients with DD-CKD and NDD-CKD. Legend: SD, standard deviation; IV, inverse variance; CI, confidence interval; df, degrees of freedom; P, probability value; DD-CKD, dialysis-dependent chronic kidney disease; NDD-CKD, non-dialysis dependent chronic kidney disease
There was no difference between the daprodustat and rhEPO arms in altering hemoglobin levels overall (MD: 0.05; 95% CI [− 0.10,0.21]; p = 0.50; I2 = 96%), as well as independently in both the DD-CKD (MD: 0.10; 95% CI [− 0.13,0.34]; p = 0.50; I2 = 97%) and NDD-CKD (MD: − 0.01; 95% CI [− 0.38,0.35]; p = 0.95; I2 = 91%) subgroups. No significant difference was observed between the two subgroups (p = 0.60; I2 = 0%). On performing sensitivity analysis, removing the study by Holdstock et al. [24] from the NDD-CKD group reduced the heterogeneity (MD: 0.14; 95% CI [− 0.08,0.36]; p = 0.21; I2 = 43%), while results pertaining to DD-CKD patients remained unchanged.
Effect on iron metabolism parameters
The outcomes concerning iron metabolism, including changes in ferritin, hepcidin, TSAT, TIBC, and TSI were reported by all studies (Table 1, Supplementary Figs. S8.1–S8.5).
The overall effect of daprodustat in improving ferritin levels (MD: − 17.29; 95% CI [− 29.69, − 4.89]; p = 0.006; I2 = 40%), hepcidin levels (MD: − 26.27; 95% CI [− 34.22, − 18.33]; p < 0.00001; I2 = 11%), and TIBC (MD: 6.10; 95% CI [4.60, 7.59]; p < 0.00001; I2 = 96%), was significant, when compared to rhEPO. In DD-CKD patients, daprodustat significantly decreased hepcidin levels (MD: − 32.37; 95% CI [− 41.16, − 23.28]; p < 0.00001; I2 = 0%) and significantly increased TIBC (MD: 5.98; 95% CI [4.26, 7.71]; p < 0.00001; I2 = 95%), but demonstrated no significant improvement in ferritin levels (MD: − 17.14; 95% CI [− 39.41,5.14]; p = 0.13; I2 = 34%), TSAT (MD: − 1.23; 95% CI [− 4.54, 2.08]; p = 0.47; I2 = 76%), and TSI (MD: 1.43; 95% CI [− 0.45, 3.30]; p = 0.14; I2 = 77%), when compared to rhEPO. In NDD-CKD patients, daprodustat, in comparison to rhEPO, significantly lowered hepcidin levels (MD: − 19.77; 95% CI [− 30.86, − 8.67]; p = 0.0005; I2 = 0%) and TSAT (MD: − 12.06; 95% CI [− 22.89, − 1.22]; p = 0.03; I2 = 99%) while significantly increasing TIBC (MD: 5.98; 95% CI [4.26,7.71]; p < 0.00001; I2 = 95%). Additionally, in this subgroup, there was no difference between the daprodustat and rhEPO arms in decreasing ferritin levels (MD: − 18.30; 95% CI [− 39.84, 3.25]; p = 0.10; I2 = 56%) and TSI (MD: − 0.30; 95% CI [− 1.36, 0.77]; p = 0.59; I2 = 38%).
On performing sensitivity analysis, removing the study by Akizawa et al. [22] caused daprodustat to demonstrate a significant decrease in TSAT levels in the DD-CKD subgroup (MD: − 3.67; 95% CI [− 4.77, − 2.56]; p < 0.00001; I2 = 0%), while eliminating heterogeneity as well.
Cardiovascular safety of daprodustat
MACE
This outcome was reported by five studies (Fig. 2).

Forest plot displaying the risk of MACE for daprodustat vs rhEPO in patients with DD-CKD and NDD-CKD. Legend: M-H, Mantel–Haenszel method; CI, confidence interval; df, degrees of freedom; P, probability value; DD-CKD, dialysis-dependent chronic kidney disease; NDD-CKD, non-dialysis dependent chronic kidney disease
The overall effect of daprodustat in reducing occurrences of MACE was similar to rhEPO (RR: 0.98; 95% CI: 0.84–1.14; p = 0.80; I2 = 45%). However, in the DD-CKD subgroup, daprodustat significantly reduced the incidence of MACE (RR: 0.89; 95% CI: 0.89–0.98; p = 0.02; I2 = 0%) when compared with rhEPO. In contrast, in the NDD-CKD subgroup, only two trials were available for analysis, and there was no difference in the risk of incidence of MACE between the daprodustat and rhEPO arms (RR: 1.05; 95% CI: 0.94–1.18; p = 0.37; I2 = 0%). Meanwhile, a significant difference was observed between the two subgroups (p = 0.03; I2 = 78.9%).
All-cause mortality
This outcome was reported by five studies (Supplementary Fig. S8.6). The overall effect of daprodustat in reducing the incidence of all-cause mortality was similar to rhEPO (RR: 1.00; 95% CI: 0.90–1.11; p = 1.00; I2 = 0%). Furthermore, there was no difference between the daprodustat and rhEPO arms in reducing the risk of all-cause mortality in both the DD-CKD (RR: 0.99; 95% CI: 0.86–1.14; p = 0.88; I2 = 0%) and NDD-CKD (RR: 1.01; 95% CI: 0.87–1.17; p = 0.87; I2 = 0%) subgroups. No significant subgroup differences (p = 0.83; I2 = 0%) were observed.
Myocardial infarction
This outcome was reported by five studies (Supplementary Fig. S8.7). The overall effect of daprodustat in reducing occurrences of MI was similar to rhEPO (RR: 0.88; 95% CI: 0.68–1.15; p = 0.37; I2 = 30%). However, in the DD-CKD subgroup, daprodustat significantly reduced the incidence of MI (RR: 0.74; 95% CI: 0.59–0.92; p = 0.006; I2 = 0%) when compared with rhEPO. In the NDD-CKD subgroup, only two studies were available for analysis, and the effect of daprodustat in increasing the risk of MI was similar to rhEPO (RR: 1.08; 95% CI: 0.84–1.38; p = 0.55; I2 = 0%). A significant difference was, however, observed between the two subgroups (p = 0.02; I2 = 80.8%).
Stroke
This outcome was reported by five studies (Supplementary Fig. S8.8). The overall effect of daprodustat in increasing occurrences of stroke was similar to rhEPO (RR: 1.01; 95% CI: 0.61–1.67; p = 0.96; I2 = 42%). Additionally, there was no difference between the daprodustat and rhEPO arms in reducing the incidence of stroke in both the DD-CKD (RR: 0.78; 95% CI: 0.50–1.20; p = 0.26; I2 = 0%) and NDD-CKD (RR: 1.41; 95% CI: 0.86–2.29; p = 0.17) subgroups. No significant difference existed between the two subgroups (p = 0.08; I2 = 68.3%).
Hospitalization for heart failure
This outcome was reported by four studies, with only two studies reporting data for each subgroup (Supplementary Fig. S8.9). The overall effect of daprodustat in increasing the risk of HHF was similar in the daprodustat and rhEPO arms (RR: 1.15; 95% CI: 0.83–1.61; p = 0.40; I2 = 61%) and the results of both the DD-CKD (RR: 1.01; 95% CI: 0.82–1.25; p = 0.90; I2 = 0%) and NDD-CKD (RR: 1.02; 95% CI: 0.36–2.87; p = 0.97; I2 = 62%) subgroups were also consistent with the overall effect. No significant difference was observed between the two subgroups (p = 0.99; I2 = 0%).
Discussion
The salient finding of our study was that changes in Hb levels were similar across patients in both the daprodustat and rhEPO arms and overall and across sub-groups. Meta-analysis of iron metabolism data further attributed a significant advantage to daprodustat in raising TIBC and in lowering hepcidin and ferritin levels, regardless of dialysis status. However, interestingly, daprodustat was found to be significantly disadvantaged when compared to rhEPO in raising TSAT levels in the NDD-CKD subgroup. Another notable finding was a statistically significant decrease in the risk of MACE for patients in the DD-CKD subgroup when treated with daprodustat vs rhEPO. In the context of their different pharmacological properties, our results suggest that daprodustat may be the better choice for some anemic CKD patients beyond simply being a viable alternative therapy.
Our meta-analysis revealed no significant difference in change in Hb levels between patients in the daprodustat and rhEPO treated arms, overall and across both DD-CKD and NDD-CKD subgroups. The preceding meta-analysis [25] on the subject also demonstrated such findings for both DD-CKD (MD: − 0.01; 95% CI [− 0.38,0.35]; p = 0.95; I2 = 91%) and NDD-CKD (MD: 0.15; 95% CI [− 0.29,0.60]; p = 0.50; I2 = 93%) subgroups. It is important to recognize and assess the heterogeneity seen in these results. One possible cause of this variation in study effect sizes may be the differences in the durations of these studies. For instance, in the NDD-CKD subgroup, removing the study from 2019 by Holdstock et al. lowered the heterogeneity to 43%. This may be because the study was less than half the duration of the others. Similarly, the 2016 study by the same author in the DD-CKD subgroup was less than a 10th duration of some of the others. Interpreted in the context of this heterogeneity, which we discuss further in the limitations section ahead, our results incorporate new evidence and confirm previous studies’ conclusions that the efficacy of daprodustat in managing anemia in patients with CKD is similar to that of rhEPO/ESAs. This suggests that daprodustat is a potentially viable alternative to the current standard therapy—rhEPO/ESAs (and iron supplementation). Importantly, daprodustat is a once-daily oral medication, whereas the current standard treatment options are injectables. Given that their efficacy is the same, the alleviation of risks and discomfort associated with injections by switching to an oral drug could improve the quality of life in anemic patients with CKD. This may be especially true for patients requiring dialysis who are already subject to repeated cannulation. This represents an avenue for future research.
Our results also highlight significant differences between daprodustat and rhEPO therapy with respect to their effects on iron metabolism in patients. Daprodustat lowered hepcidin and ferritin levels and increased TIBC significantly more than rhEPO. For hepcidin and TIBC, these findings persisted down to the individual subgroups. Our results for TIBC concur with those of the most recent meta-analysis, which demonstrated a significant increase in both the DD-CKD (MD: 33.85; 95% CI [25.06,42.64]; p < 0.01; I2 = 76%) and NDD-CKD MD: 29.00; 95% CI [19.65,38.35]; p < 0.01; I2 = 70%) subgroups. However, our results update their findings regarding hepcidin levels, for which the former study did not find a significant advantage to daprodustat in lowering hepcidin levels in the DD-CKD subgroup (MD: − 9.26; 95% CI [− 33.69,15.16]; p = 0.46; I2 = 87%). Furthermore, our analysis suggests that daprodustat was significantly disadvantaged to rhEPO in raising TSAT levels in the NDD-CKD subgroup. The implications of these findings are of the utmost importance since deranged iron metabolism directly contributes to the pathogenesis of anemia in CKD patients and comes to bear on their risk of cardiovascular disease. For instance, hepcidin is a key mediator in the anemia of chronic inflammation and sequesters iron in a manner that precipitates a functional iron deficiency [26]. In fact, in patients with higher levels of inflammation, hypo-responsiveness to rhEPO can manifest as a challenge in the effective management of anemia [25].
Moreover, TIBC is used as a biomarker for anemias of several etiologies and is a prognostic indicator for patients post-operatively or for those on hemodialysis, where lower levels indicate a poorer prognosis, malnutrition, muscle loss, and protein-energy wasting [27]. These results may thus help illustrate aspects of daprodustat’s clinical value. Similarly, daprodustat’s significant disadvantage to rhEPO in raising TSAT levels in the NDD-CKD subgroup may be a factor limiting its clinical benefit. In addition to being a biomarker for iron deficiency, low TSAT levels indicate an increased risk for cardiovascular and cerebrovascular incidents and death, including in dialysis-dependent patients [28, 29]. It is interesting, then, to note that daprodustat did not have a significantly lower risk of MACE in the NDD-CKD group than rhEPO, where it also had a significant disadvantage to rhEPO in raising TSAT levels. Whether or not these differences in the risk of MACE between daprodustat and rhEPO are related to the corresponding differences in TSAT level changes is a question that remains to be answered by future research. Regarding TSAT results for the DD-CKD subgroup, it was noted that excluding Akizawa et al.’s [22] data from the analysis lowered the I2 value from 76 to 0%, conferring a statistically significant disadvantage to daprodustat in raising TSAT levels, similar to the findings seen in the NDD-CKD group. This suggests that the proportion of variance in effect size due to sampling error, for this result, decreased significantly with the inclusion of this study and that actual differences in the true effect size came into play. These differences could be associated with the fact that Akizawa et al.’s study was restricted to Japan, whereas the other studies in the subgroup analysis were multinational. Whether restricted only to the NDD-CKD subgroup or also applicable to the DD-CKD subgroup, differences in TSAT level changes and how they are associated with cardiovascular adverse events in patients require further investigation.
The efficacy and safety of these drugs are thus significantly affected by and reflected in their effects on patients’ iron metabolism. To that end, our analysis demonstrates daprodustat to be superior to current therapies in several regards, while inferior in a few cases. However, the iron supplementation received by patients along with these treatments must also be considered. In patients showing hyporesponsiveness to rhEPO as described previously, those treated with daprodustat required lower doses of parenteral iron than those treated with rhEPO [18]. Investigating if this represents a decrease in the risk to patients of adverse effects associated with excess iron supplementation, such as toxicity due to free radical generation or the increased risk of bacterial growth and infection, may yield valuable insight that helps identify clinical scenarios where daprodustat is the preferred treatment [25].
A major source of concern in the management of anemic patients with CKD is the adverse effects associated with treatment. These include the risks and ill effects of iron supplementation, as discussed previously, as well as those associated with rhEPO/ESAs. Cardiovascular disease and complications such as stroke and hypertension are particularly important causes of patient morbidity and mortality. Our analysis revealed daprodustat to significantly decrease the risk of MACE when compared to rhEPO in DD-CKD patients. Further analysis revealed this to be attributable primarily to MI, which was the only MACE component whose occurrence significantly decreased in response to daprodustat therapy. Our results refine those of a recent meta-analysis by Patoulias et al. [10] which demonstrated no significant effect of daprodustat in reducing the incidence of a composite outcome of CV death, MI, stroke, and HHF decompensation in DD-CKD patients (RR: 0.95; 95% CI: 0.84–1.07; p = 0.39; I2 = 0%). Thus, in analyzing adverse outcomes separately, we were able to identify the heightened MACE/MI risk in some patients, as described previously. It is pertinent to note that studies involving hemodialysis patients have shown that levels of endogenous erythropoietin produced in response to daprodustat are significantly lower than those administered exogenously as rhEPO/ESAs [20]. This may be of significance as, like some of the derangements in iron metabolism discussed earlier, the administration of high doses of ESAs are also associated with the heightened risk of cardiovascular adverse events [25]. It has been stated in the literature, therefore, that decreased EPO levels like those seen with the use of daprodustat instead of rhEPO may translate to lower rates of related adverse effects [3]. However, the DD-CKD subgroup analysis included just three studies, and only one of these independently demonstrated a risk reduction for MACE. Similarly, the NDD-CKD subgroup analysis was based on just 2 studies. The result seen thus warrants cautious interpretation and perhaps serves to raise questions for future research to answer. In summary, further insights into CVD risk and patient EPO levels across therapies are needed. These may emerge from more investigations of the interplay between the choice of therapeutic agent, renal function, iron metabolism, and EPO levels in DD-CKD patients.
It is crucial to emphasize that additional questions remain to be addressed before the clinical utility of daprodustat, in comparison to current standard therapies, is clearly delineated. Since daprodustat acts on patients’ kidneys to stimulate endogenous EPO production, long-term studies to assess changes in the drug’s efficacy with the disease progression of CKD may be required. Moreover, the effect of daprodustat in producing increased VEGF levels, which is implicated in several pathological processes such as diabetic retinopathy and tumor metastases, also merits the use of caution and highlights the need for further investigation [25].
Conclusions
In conclusion, our findings incorporate new evidence and confirm the comparative efficacy of daprodustat and standard therapy as seen in previous systematic reviews. Furthermore, we highlight differences in the changes in iron metabolism in anemic CKD patients across treatments. In assessing the difference in MACE risk between patients treated with daprodustat and rhEPO, we found that DD-CKD patients are less likely to experience MACE if treated with daprodustat. When examining these findings in the context of the differences between the pharmacology of daprodustat and current treatment options, it becomes clear that there are patient cohorts where daprodustat may be a superior choice beyond just a viable alternative medication. However, concerns raised in previous articles regarding the effects of daprodustat on VEGF levels and subsequent consequences [3, 24] coupled with the need for more long-term studies and a greater understanding of the implications of the benefits to iron metabolism, represent the scope for further research before major conclusions can be drawn. The results of ongoing phase III trials, as well as the clinical use of daprodustat in Japan, where it has now been approved, will add further clarity to our understanding of the potential applications of this drug to improve patient outcomes.
Limitations
There are several limitations to our meta-analysis which must be emphasized. Firstly, among the studies pooled, only two assessed the effect of daprodustat on the outcomes of NDD-CKD; the accurate estimation of the true effect of the drug on the group’s outcomes is thus difficult and will require the availability of more evidence. Furthermore, only two included studies investigated the impact of daprodustat on HHF for DD-CKD, precluding the drawing of conclusions in this context for either subgroup. It is important to recognize possible sources of heterogeneity seen in some of our results, in addition to those discussed previously. Various forms of rhEPO were used across the studies analyzed, which may have contributed to some of the heterogeneity seen in the results, such as the change in Hb levels and TIBC levels that was not attributable to chance. Moreover, heterogeneity may have been produced by the variation in the cardiovascular disease history, disease stage, and erythropoietin sensitivity/hypo-responsiveness in patients. Furthermore, the dosages of the drugs in both daprodustat and control groups varied between different trials and across different time points within the same studies. Fortunately, the observed heterogeneity does not invalidate the findings of our meta-analysis since the adverse effects investigated (cardiovascular and iron metabolism) are associated with erythropoiesis-stimulating agents (ESA) and all studies use rhEPO agents as controls that act by stimulating erythropoiesis. As for the results regarding the change in Hb levels, our findings confirm those of the previous meta-analysis. However, it remains true that the effect sizes reported by the various RCTs investigating daprodustat are quite variable. While our meta-analysis does synthesize the overall results of these trials, more and larger clinical trials will better clarify the specific use cases of these drugs and identify the causes of these variations. Another challenge we faced was the unresponsiveness of corresponding authors whom we emailed. This necessitated the graphical extraction of data that was not provided in tables or the manuscript in numerical form. In addition, in several studies, the standard deviation was not reported in certain outcomes. As a result, we imputed these missing standard deviations, as has been described in the methods section. This reduced the accuracy of computed results where relevant and produced an inferior estimate when compared to the true standard deviations that were not reported. Lastly, it was challenging to standardize the change from baseline measurements of the hemoglobin levels and iron metabolism parameters as different time points and evaluation periods were used in the included studies.
Availability of data materials
The data that support the findings of this study were sourced directly from the published studies included in this systematic review and meta-analysis.
References
Bikbov B, Purcell CA, Levey AS, Smith M, Abdoli A, Abebe M, Adebayo OM, Afarideh M, Agarwal SK, Agudelo-Botero M, Ahmadian E (2020) Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England) 395(10225):709–33
Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M et al (2021) 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: developed by the task force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With. Eur Heart J 42(34):3227–3337
Portolés J, Martín L, Broseta JJ, Cases A (2021) Anemia in chronic kidney disease: from pathophysiology and current treatments, to Future Agents. Front Med 26(8):328
Shepshelovich D, Rozen-Zvi B, Avni T, Gafter U, Gafter-Gvili A (2016) Intravenous versus oral iron supplementation for the treatment of anemia in CKD: an updated systematic review and meta-analysis. Am J Kidney Dis 68(5):677–690
McMurray J, Parfrey P, Adamson JW, Aljama P, Berns JS, Bohlius J et al (2012) Kidney disease: Improving global outcomes (KDIGO) anemia work group. KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl 279–335
US Food and Drug Administration (2011) FDA drug safety communication: modified dosing recommendations to improve the safe use of erythropoiesis-stimulating agents (ESAs) in chronic kidney disease
Bonomini M, Del Vecchio L, Sirolli V, Locatelli F (2016) New treatment approaches for the anemia of CKD. Am J Kidney Dis 67(1):133–142
Locatelli F, Bárány P, Covic A, De Francisco A, Del Vecchio L, Goldsmith D et al (2013) Kidney disease: improving global outcomes guidelines on anaemia management in chronic kidney disease: a European Renal Best Practice position statement. Nephrol Dial Transplant 28(6):1346–1359
Zheng Q, Wang Y, Yang H, Sun L, Fu X, Wei R et al (2020) Efficacy and safety of daprodustat for anemia therapy in chronic kidney disease patients: a systematic review and meta-analysis. Front Pharmacol 11:573645
Patoulias D, Papadopoulos C, Doumas M (2022) Meta-analysis addressing the cardiovascular safety of daprodustat in patients with chronic kidney disease undergoing dialysis or not. Am J Cardiol 170:166–167
Singh AK, Cizman B, Carroll K, McMurray JJ V, Perkovic V, Jha V et al (2022) Efficacy and safety of daprodustat for treatment of anemia of chronic kidney disease in incident dialysis patients: a randomized clinical trial. JAMA Intern Med
amstar-2_-a-critical-appraisal-tool-for-systematic-reviews-that-include-randomised-or-non-randomised-studies-of-healthcare-interventions,-or-both. Available from: https://www.bmj.com/content/358/bmj.j4008
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors) (2022) Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane. Available from www.training.cochrane.org/handbook
Rohatgi A (2021) WebPlotDigitizer Version 4.5 [Internet]. Available from: https://automeris.io/WebPlotDigitizer
Burda BU, O’Connor EA, Webber EM, Redmond N, Perdue LA (2017) Estimating data from figures with a web-based program: considerations for a systematic review. Res Synth Methods [Internet] 8(3):258–62. Available from: https://pubmed.ncbi.nlm.nih.gov/28268241/. [cited 2022 Mar 8]
Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC (2019) Assessing risk of bias in a randomized trial. Cochrane Handbook for Systematic Reviews of Interventions p. 205–28. Wiley Online Books
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P et al (2008) GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336(7650):924–926
Singh AK, Carroll K, Perkovic V, Solomon S, Jha V, Johansen KL et al (2021) Daprodustat for the treatment of anemia in patients undergoing dialysis. N Engl J Med 385(25):2325–2335
Singh AK, Carroll K, McMurray JJV, Solomon S, Jha V, Johansen KL et al (2021) Daprodustat for the treatment of anemia in patients not undergoing dialysis. N Engl J Med 385(25):2313–2324
Holdstock L, Meadowcroft AM, Maier R, Johnson BM, Jones D, Rastogi A et al (2016) Four-week studies of oral hypoxia-inducible factor–prolyl hydroxylase inhibitor GSK1278863 for treatment of anemia. J Am Soc Nephrol [Internet] 27(4):1234–44. Available from: https://pubmed.ncbi.nlm.nih.gov/26494831/. [cited 2022 Apr 27]
Meadowcroft AM, Cizman B, Holdstock L, Biswas N, Johnson BM, Jones D et al (2019) Daprodustat for anemia: a 24-week, open-label, randomized controlled trial in participants on hemodialysis. Clin Kidney J 12(1):139–148
Akizawa T, Nangaku M, Yonekawa T, Okuda N, Kawamatsu S, Onoue T et al (2020) Efficacy and safety of daprodustat compared with darbepoetin alfa in Japanese hemodialysis patients with anemia: a randomized, double-blind, phase 3 trial. Clin J Am Soc Nephrol 15(8):1155–1165
Nangaku M, Hamano T, Akizawa T, Tsubakihara Y, Nagai R, Okuda N et al (2021) Daprodustat compared with epoetin beta pegol for anemia in Japanese patients not on dialysis: a 52-week randomized open-label phase 3 trial. Am J Nephrol 52(1):26–35
Holdstock L, Cizman B, Meadowcroft AM, Biswas N, Johnson BM, Jones D et al (2019) Daprodustat for anemia: a 24-week, open-label, randomized controlled trial in participants with chronic kidney disease. Clin Kidney J 12(1):129–138
Fu Z, Geng X, Chi K, Song C, Wu D, Liu C et al (2022) Efficacy and safety of daprodustat vs rhEPO for anemia in patients with chronic kidney disease: a meta-analysis and trial sequential analysis. Front Pharmacol 13
Coyne DW (2011) Hepcidin: clinical utility as a diagnostic tool and therapeutic target. Kidney Int [Internet] 80(3):240–4. Available from: http://www.kidney-international.org/article/S0085253815550345/fulltext. [cited 2022 Apr 27]
Ikeda-Taniguchi M, Takahashi K, Shishido K, Honda H (2022) Total iron binding capacity is a predictor for muscle loss in maintenance hemodialysis patients. Clin Exp Nephrol [Internet] 26(6):583–92. https://doi.org/10.1007/s10157-022-02193-1. [cited 2022 Sep 20]
Stack AG, Mutwali AI, Nguyen HT, Cronin CJ, Casserly LF, Ferguson J (2014) Transferrin saturation ratio and risk of total and cardiovascular mortality in the general population. QJM An Int J Med [Internet] 107(8):623–33. Available from: https://academic.oup.com/qjmed/article/107/8/623/2948338. [cited 2022 Sep 20]
Kuragano T, Joki N, Hase H, Kitamura K, Murata T, Fujimoto S et al (2020) Low transferrin saturation (TSAT) and high ferritin levels are significant predictors for cerebrovascular and cardiovascular disease and death in maintenance hemodialysis patients. PLoS One [Internet] 15(9). Available from: https://pubmed.ncbi.nlm.nih.gov/32877424/. [cited 2022 Apr 30]
Author information
Authors and Affiliations
Contributions
K.F conceptualized and, together with T.A, supervised the investigation. Search strings were designed by A.S.F, and abstract and title screening, as well as full-text review screening, were performed by W.A and M.U.M with conflicts being resolved by A.S.F. Data extraction was performed independently by M.B.I and M.T.N, with conflicts being resolved by A.A. W.A and M.U.M were major contributors in analyzing the data. Quality assessment and certainty of evidence assessment were performed independently by W.A and M.T.M, with conflicts being resolved by A.S.F. Supplementary material was prepared by A.S.F, M.B.I, M.T.M, M.T.N, A.A, and S.R.A. W.A, O.M, A.S.F, and S.R.A were major contributors in writing and editing the manuscript. All authors critically reviewed the results, approved the final manuscript for publication, and agree to be accountable for all aspects of the work done in producing this manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was exempt from full ethical approval by an institutional review board as no original data was included. There were no interactions with any human or animal participants across the duration of this study.
Consent to participate
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Fatima, K., Ahmed, W., Fatimi, A.S. et al. Evaluating the safety and efficacy of daprodustat for anemia of chronic kidney disease: a meta-analysis of randomized clinical trials. Eur J Clin Pharmacol 78, 1867–1875 (2022). https://doi.org/10.1007/s00228-022-03395-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-022-03395-y