
Abstract
Purpose
There is a large inter-individual variation in the efficacy of valproic acid (VPA) against epilepsy. The genetic polymorphism influence of sodium channels on VPA response remains a matter of debate. The aim of the study was to explore the effect of SCN1A and SCN2A gene polymorphisms on VPA response in the treatment of epilepsy among Chinese patients.
Methods
A total of 354 epileptic patients with VPA treatment were genotyped for five single nucleotide polymorphisms (SNP), including SCN1A rs10188577 T>C, rs2298771 T>C, rs3812718 G>A, and SCN2A rs2304016 A>G, rs17183814 G>A. A binary logistic regression analysis was performed to evaluate the association of genotype with VPA antiepileptic effects, adjusting the influence of confounding factors.
Results
Genotype distributions of all selected SNPs were consistent with the Hardy–Weinberg equilibrium in epilepsy patients. SCN1A rs3812718 and SCN2A rs2304016 were found to be significantly associated with VPA response, both in monotherapy and in VPA-based polytherapy. Patients with the rs3812718 A allele were more frequently seen in the VPA-responsive group (P < 0.05), and the rs2304016 G allele was related to an increased risk of resistance to VPA therapy (P < 0.05).
Conclusions
Our study revealed that SCN1A rs3812718 and SCN2A rs2304016 polymorphisms might be markers of VPA response in Chinese epilepsy patients.
Trial registration
ChiCTR-1800016477
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Epilepsy is a severe neurological disease that affects 65 million people worldwide. Seizure-related disability, mortality, comorbidity, stigma, and costs are major burdens for epileptic patients [1, 2]. Antiepileptic drugs (AEDs) are the mainstay treatment for epileptic seizures, and both traditional and new-generation AEDs are used. However, even with the most effective medication, about 30% of patients still experience recurrent seizures [3, 4]. Drug resistance is multifactorial and accumulating evidence indicates that genetic variations can affect an individual response to a drug at pharmacokinetics and pharmacodynamics levels [5].
Valproic acid (VPA) is one of the most frequently prescribed AEDs in epilepsy treatment with unsurpassed efficacy against most generalized seizure types and focal seizures [6]. VPA is also recommended as the preferred treatment for seizures that are difficult to classify at the time of diagnosis [7]. However, large inter-patient variations of VPA antiepileptic efficacy exist, and variations in VPA plasma concentrations can only explain part of the difference in pharmacodynamics.
Epilepsy is an ion channel disease involving multiple ion channels, such as chloride, calcium, potassium, and sodium. About 25% of genes identified in epilepsy encode ion channels [8]. Voltage-gated sodium (Nav) channels are vital for the initiation and propagation of neuronal action potentials [9]. Nav channels are the major targets for many first-line AEDs, such as carbamazepine (CBZ), oxcarbazepine (OXC), phenytoin (PHT), lamotrigine (LTG), and VPA. VPA eliminates the high-frequency repetitive electrical activation of central nervous cells and delays the recovery of inactivated sodium ion channels, persistently reducing the electrical conduction of sodium ions [10,11,12]. In addition, long-term VPA treatment can upregulate the expression of sodium channels on cell surfaces [12].
Nav channels are composed of both α and β subunits, of which the α subunit is the functional subunit. VPA and other sodium channel blockers bind to the α subunit to exert their therapeutic effects [13]. The defects of the sodium channel subunit slow down its inactivation and prolong the time of depolarization of cell membranes, leading to the generation and propagation of seizures [14]. Nav1.1 and Nav1.2 channel subtypes are the primary sodium channels in the central nervous system (CNS), which are encoded by SCN1A and SCN2A, respectively [9]. Nav1.1 is mainly expressed in GABAergic neurons [14, 15]. SCN1A, encoding the α subunit of the Nav1.1 channel, is the gene most frequently associated with epilepsy. Mutations in SCN1A are responsible for genetic epilepsy with a wide range of severities [9]. Similarly, the SCN2A gene, which codes for the α subunit of the Nav1.2 channel, is closely associated with many types of epilepsy. Genetic variations in SCN1A and SCN2A may be the major determinants of individual phenotypic differences in response to AEDs, which has aroused a great interest among researchers.
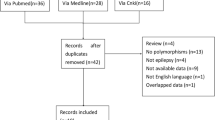
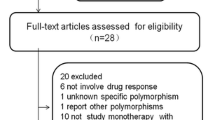
At present, many investigators have studied the association between gene polymorphisms of SCN1A and SCN2A, and AED response, but few studies focused on VPA response and results were conflicting. A cohort study in Hong Kong Chinese and Malaysian epilepsy patients with VPA monotherapy did not show that SCN1A gene polymorphism influenced VPA response [16]. A study carried out by Yip and colleagues in Caucasian patients found that SCN1A rs10188577 was the only single nucleotide polymorphism (SNP) associated with an AED response (including VPA) [17]. Moreover, a study in a Chinese epilepsy cohort revealed that SCN2A rs2304016 was related to VPA response [18].
In this study, we intended to explore the effect of SCN1A and SCN2A gene polymorphisms on VPA efficacy in a Chinese Han epileptic population. We aimed to provide genetic evidence for personalized VPA treatment by identifying genetic markers that can predict VPA treatment resistance.
Materials and methods
Patients
The study recruited a total of 419 unrelated Chinese Han epilepsy patients from the neurology outpatient department at Xiangya Hospital, Central South University. All patients had a history of two or more clinically definite, unprovoked epileptic seizures. Out of the 419 patients, 318 were treated with oral VPA monotherapy, and the other 101 patients received at least 3 AEDs because their initial VPA monotherapy failed. Patients’ demographic and clinical data were collected at their first visit, such as gender, age, body weight, height, seizure type, age at onset of seizure, family history of epilepsy, medical and neurological history, frequency and duration of seizures, and epilepsy treatment regimen. Medical records were subsequently collected every 3 months during 1-year VPA treatment, and recordings from each follow-up phone call or visit included doses of AEDs at the time of follow-up, patient compliance, and responsiveness to AEDs. The final evaluated value of VPA concentration represented the most recent trough plasma level at the maximum maintenance dose during the study period. Patients were excluded if treating physician or patient thought that VPA treatment was contraindicated or if there was a history of other progressive neurological disease. Patients with poor medication adherence were also excluded.
Written informed consent was given for all patients or their guardians before recruitment. The study was approved by the hospital Medical Ethics Committee and was registered in the Chinese Clinical Trial Registry (ChiCTR-1800016477).
Definition of drug resistance and responsiveness
In accordance with the consensus proposal of the International League Against Epilepsy (ILAE) Commission [4], VPA monotherapy patients were divided into two groups according to their VPA response: VPA-responsive and VPA-resistant. VPA-responsive patients were defined as those who were completely free of seizures for at least 1 year during VPA monotherapy. VPA-resistant patients were defined as those with an occurrence of at least four seizures during 1 year of VPA monotherapy at the maximum tolerated dose.
Genotyping
Candidate SNPs were selected based on database results and published papers. First, data on SCN1A and SCN2A SNPs in the southern Chinese population (CHS) were downloaded from the 1000 Genomes Project. Second, tag SNPs were selected using the Haploview software. SNPs with minor allele frequency > 0.1 were selected for tag SNP screening, and an R2 > 0.8 was considered to represent a linkage disequilibrium. Finally, referring to the published literatures and F-scores from F-SNP database (http://compbio.cs.queensu.ca/F-SNP/.), the following five SNPs were identified: SCN1A rs10188577 T>C, rs2298771 T>C, rs3812718 G>A, SCN2A rs2304016 A>G, and rs17183814 G>A. Details of the selected SNPs are presented in Table 1.
Peripheral venous blood samples (2 mL) were obtained from each patient. Following the manufacturer’s instructions, genomic DNA was extracted from blood samples using E.Z.N.A.SQ Blood DNA Kit II (Omega Bio-Tek, GA, USA). The selected SNPs were genotyped using the SNPscan™ assay technique (cat#: G0104K, Genesky Inc. Shanghai, China) as previously described [19]. To ensure the quality of genotyping, random duplicated sample genotyping was undertaken as an internal control and no genotyping error was observed for all SNPs.
Statistical analysis
Statistical analyses were performed using the SPSS software (IBM SPSS Statistics 24.). Continuous variables were analyzed by Kolmogorov–Smirnov test to confirm normal distribution. Normal distributed data were expressed as mean ± standard deviation (SD) and mean comparisons were calculated by an independent samples t test. For non-normal distribution, data were presented as median (1st–3rd quartile) and were compared by Mann–Whitney U test. Categorical variables were reported as frequency and percentage. The differences in the categorized data between the responsive group and the resistant group were analyzed using chi squared test (χ2 test) or Fisher’s exact test when it is appropriate. The χ2 test was also used to assess deviations from the Hardy–Weinberg equilibrium (HWE). Genotypes containing fewer than five individuals were combined with heterozygotes to create a dominant model. Binary logistic regression was applied to adjust potential covariates. Associations of VPA response and sodium channel gene polymorphisms were expressed as odds ratios (ORs) and risks were estimated with 95% confidence intervals (CIs). A two-tailed P value < 0.05 was considered to be statistically significant.
Results
Association study in VPA monotherapy
A total of 318 epilepsy patients undergoing VPA monotherapy were enrolled in this study. However, 19 patients did not complete their 1-year follow-up. The drug responses of 46 patients were undetermined because their seizures occurred less than four times during 1 year of VPA treatment. Hence, 253 VPA monotherapy patients were included in the final analysis. The demographics and clinical characteristics of patients with VPA monotherapy are depicted in Table 2. Among these patients, 125 patients were classified into the VPA-responsive group and 128 were in the VPA-resistant group. No statistically significant differences were found between the two groups regarding their gender, age, seizure type, course of epilepsy, and VPA daily dose. Patients in the VPA-responsive group were much younger when experienced their first seizure than those in the VPA-resistant group (P = 0.048). Additionally, VPA trough concentration in the VPA-resistant group was significantly higher than that in the VPA-responsive group (53.38 ± 27.10 vs. 45.54 ± 23.49 μg/mL, P = 0.016).
Table 3 lists the allelic and genotypic frequencies of SCN1A and SCN2A SNPs in patients on VPA monotherapy. Genotypic distributions agreed with the HWE (P > 0.05, Table S1). Distributions of alleles and genotypes were similar between the VPA-responsive and the VPA-resistant groups. After correcting for confounding factors (age, age at onset of seizures, and course of epilepsy), the results of binary logistic regression analysis revealed that SCN1A rs3812718 G>A was associated with a positive response to VPA monotherapy, and SCN2A rs2304016 was associated with a weaker response to VPA monotherapy. Regarding the genotypic frequencies of the SCN1A rs3812718 G>A polymorphism, carriers with a GA or AA genotype were more common in the VPA-responsive group (GG vs. GA: OR = 0.40, 95% CI = 0.18–0.93, P = 0.034; GG vs. AA: OR = 0.41, 95% CI = 0.18–0.90, P = 0.027). In the dominant model, both GA and AA genotypes were significantly more frequent in the VPA-responsive group than the VPA-resistant group (88.0% vs. 78.1%, P = 0.037), as confirmed in logistic analysis (OR = 0.41, 95% CI = 0.19–0.87, P = 0.020). Compared with the SCN2A rs2304016 AA genotype, the AG genotype was associated with an increased risk of VPA resistance (OR = 2.36, 95% CI = 1.08–5.16, P = 0.031). However, the difference was only marginally significant under the dominant model (OR = 2.07, 95% CI = 0.99–4.34, P = 0.054).
Association study in VPA-based polytherapy
We also recruited 101 VPA-based polytherapy patients who were resistant to initial VPA monotherapy. Consistent with the definition of VPA resistance, those patients, who experienced more than four seizures with VPA-based polytherapy at maximum tolerated doses during 1-year follow-up, were combined with 128 VPA monotherapy-resistant patients as the VPA-resistant group. The VPA-responsive group included 125 VPA monotherapy-responsive patients. As can be seen in Table 2, the two groups were similar in age, age at study entry and onset of seizures, course of epilepsy, and duration of VPA treatment. The distributions of gender and seizure type between groups had no statistical difference. However, at an equivalent VPA daily dose, patients in the VPA-resistant group had a significantly higher VPA trough concentration than the VPA-responsive group (56.96 ± 25.72 vs. 45.54 ± 23.49 μg/mL, P = 0.00006).
As shown in Table 4, SCN1A rs3812718 G>A was significantly associated with VPA response. Patients with GA or AA genotypes were more prone to have a better response to VPA treatment (GG vs. GA: OR = 0.38, 95% CI = 0.19–0.78, P = 0.008; GG vs. AA: OR = 0.40, 95% CI = 0.19–0.85, P = 0.017). In the dominant model, the GG genotype was less common in the VPA-responsive group compared with the VPA-resistant group (OR = 0.39, 95% CI = 0.20–0.77, P = 0.007). In addition, the A allele was a protective factor for complete freedom from seizures (OR = 0.70, 95% CI = 0.50–0.99, P = 0.043). SCN2A rs2304016 was also significantly related to an increased risk of VPA resistance. Compared with the responsive group, AG genotype was more frequent in the resistant group (OR = 2.47, 95% CI = 1.19–5.12, P = 0.015). In the dominant model, G-containing genotype carriers were more likely to be resistant to VPA therapy (OR = 2.14, 95% CI = 1.07–4.25, P = 0.031).
SCN1A rs10188577, rs2298771, and SCN2A rs17183814 had no effect on VPA therapy in our cohorts.
Discussion
VPA is a broad-spectrum AED and it is widely used in the treatment of various seizures. Individual responses to VPA are significantly varied and pharmacogenetics plays an important role in explaining this difference. In the present study, SCN1A rs3812718 G>A was significantly associated with a drug response both in VPA monotherapy and VPA-based polytherapy. Compared with wild homozygote carriers, patients with rs3812718 AA and GA genotypes were more sensitive to VPA therapy and had better seizure control. Patients with the SCN2A rs2304016 A allele were more likely to achieve seizure freedom after VPA treatment.
Our results are similar to a subgroup analysis in Malay idiopathic generalized epilepsy (IGE) patients, which revealed that the rs3812718 G allele might be a risk factor for resistance to VPA monotherapy [16]. Results of previous studies on the correlation between patients’ response to sodium channel blockers and rs3812718 polymorphism were inconclusive. Some suggested that the G allele was a protective factor resulting in a better response [20,21,22], while others found that rs3812718 had no effect on AED response [23,24,25,26]. A meta-analysis published in 2013 revealed that rs3812718 polymorphism and AED response were unrelated [27]; however, the result warrants for an update. Hung and colleagues found that in the Taiwanese population, maintenance doses and the maintenance dose-adjusted concentrations (CDR) of CBZ in GA and AA genotypes were lower than those in the GG genotype [28]. Conversely, a British study suggested that the maximum doses or serum levels of CBZ or PHT in AA genotype carriers were higher than those in GG genotype carriers [29]. Another study on a Taiwanese cohort reproduced these results, which indicated that PHT maintenance dose for the GG genotype was lower than that for the AA genotype [30]. An adequate drug concentration is required for antiepileptic efficacy. Therapeutic drug monitoring is recommended in epilepsy treatment to ensure that AED plasma concentration lies within the therapeutic window [31]. In our population, patients in the responsive group had a significantly lower VPA trough concentration than those in the resistant group. Therefore, the response of a patient may be the best evaluation criteria for efficacy.
Located at the 5′ splice donor site of a highly conserved region of SCN1A exon 5, rs3812718 (namely IVS5N+5, IVS5-91) G>A is a common functional intronic variant. It modulates the proportion of human brain SCN1A transcripts incorporating the canonical (5A) or alternative (5N) exon 5 [32]. The α subunit of Nav channel contains voltage sensors and an ion-conducting pore in four internally repeated domains (I–IV), each of which consists of six transmembrane α-helical segments (S1–S6) and a pore loop connecting S5 and S6 [9]. Exon 5 encodes the S4 transmembrane segment or voltage sensor in the first domain (DI) of NaV1.1. Investigators have demonstrated that NaV1.1-5N is primarily expressed during the neonatal periods and NaV1.1-5A is the adult form [29, 33]. However, strict developmental regulation of this splicing event may be relaxed as evidenced by the detection of NaV1.1 transcripts (up to 50% of transcripts) consisting of exon 5N in the adult human brain [29, 33]. Exon 5N makes up 50% GG genotype transcripts, while it only makes up 1% of transcripts in the AA genotype. Of note, the A allele can disrupt the consensus splice donor sequence immediately following exon 5N, therefore completely blocking Nova2-mediated (a specific nervous system splicing factor) incorporation of exon 5N into mature SCN1A mRNA transcripts and affecting the translating protein [33]. As a result, a three-amino-acid difference between channels containing 5N-(Phe, Asn, and Phe) and 5A-(Tyr, Asp, and Val) may alter the sensitivity to AEDs [34].
Our study provides evidence that rs3812718 may affect VPA response. However, the results in our cohort and the Malay IGE cohort were contrary to previous studies. Generally, drugs exert their pharmacological action through binding to their specific targets, and changes in those targets alter drug effects. Severe myoclonic epilepsy of infancy (SMEI) is caused by haplo insufficiency of Nav1.1 channel. Clinical practice suggests that sodium channel blockers should be avoided in these SMEI patients, which could worsen the disease [35]. Studies have shown that OXC and LTG exacerbate symptoms of some patients with Dravet syndrome, while VPA therapy is effective [36]. Dravet syndrome is also caused by SCN1A mutation. CBZ, PHT, and OXC mainly block sodium channels to create an antiepileptic effect. The multiplicity of cellular targets of VPA action, ranging from channels and receptors to pathways involved in gene expression regulation, makes the identification of antiseizure mechanisms a particularly difficult task. In addition, VPA is an inhibitor of histone deacetylase and displays antiepileptogenesis and neuroprotection activity in some animal models [37]. In view of the multiple extra- and intra-cellular targets of VPA, it could play an antiepileptic role through other pathway when something is wrong with the sodium channels. To some extent, this may explain why CBZ and PHT perform better in rs3812718 GG carriers while VPA performs better in the A allele carriers. For this reason, we need more studies with large samples to confirm our results.
Evidence has shown that SCN1A IVS5-91 G>A polymorphism is associated with a susceptibility to epilepsy but not with drug responsiveness [38]. A meta-analysis reported that the A allele was a risk factor of epilepsy both in North Indian and Caucasian populations [39]. Without a healthy control, we are not sure if this polymorphism is related to the susceptibility to epilepsy in our population.
Given Nav1.2 plays a vital role in epileptogenesis, we also tried to find the association between SCN2A gene polymorphisms and VPA resistance in our cohort. The result suggested that SCN2A rs2304016 A>G is a possible marker for VPA resistance, and G allele carriers seem more likely to be resistant to VPA therapy. However, this result is contrary to work done by Li and colleagues. They found that the AA genotype was a risk factor for VPA monotherapy resistance in Chinese epilepsy patients [18]. Furthermore, a multicenter study from Hong Kong in epileptics treated with AEDs revealed that rs2304016 did not affect the response of sodium channel blocker AEDs [40]. The SNP rs2304016 is located in the putative branch site for splicing exons 7 and 8, and a functional study demonstrated that this locus polymorphism did not affect splicing, nor did it influence mRNA expression [40]. It is possible that rs2304016 A>G polymorphism has no effect on drug response itself but is in linkage disequilibrium with a functional genetic variant that influences drug efficacy. In future studies, differences among genotypes at the protein level are worthwhile to explore.
Our study has the following limitations: (1) types of epilepsy were only roughly divided into primary and secondary seizures according to etiologies as it was not easy to select homogeneous individuals in this clinical study. However, a logistic regression analysis indicated that seizure type was not a confounder; (2) the study follow-up was only 1 year, and therapeutic effect of VPA therapy could be delayed; (3) the study sample size was relatively small which was not suitable for the Bonferroni correction to counteract the problem of multiple comparisons; and (4) the study population should be better defined with regard to age. It is necessary in future studies to investigate the molecular mechanism of how an IVS5-91 G>A splice-site polymorphism influencing treatment efficacies of VPA and other AEDs.
In conclusion, we have shown that SCN1A IVS5-91 G>A polymorphism was not only associated with VPA monotherapy response but also with VPA polytherapy response. Furthermore, the AA and GA genotypes were protective factors for a better antiepileptic response. SCN2A rs2304016 polymorphism also affected VPA efficacy. Pharmacogenomics diagnostics is an important part of precision medicine. If the above associations are confirmed in a prospective trial with a large population, the determination of SCN1A rs3812718 genotype and SCN2A rs2304016 genotype may help to identify epileptic patients who will benefit the most from VPA therapy.
References
Moshé SL, Perucca E, Ryvlin P, Tomson T (2015) Epilepsy: new advances. Lancet 385:884–898
Verrotti A, Mazzocchetti C (2016) Epilepsy: beyond seizures-the importance of comorbidities in epilepsy. Nat Rev Neurol 12:559–560
Brodie MJ, Besag F, Ettinger AB, Mula M, Gobbi G, Comai S, Aldenkamp AP, Steinhoff BJ (2016) Epilepsy, antiepileptic drugs, and aggression: an evidence-based review. Pharmacol Rev 68:563–602
Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen Hauser W, Mathern G, Moshé SL, Perucca E, Wiebe S, French J (2010) Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 51:1069–1077
Zhu MM, Li HL, Shi LH, Chen XP, Luo J, Zhang ZL (2017) The pharmacogenomics of valproic acid. J Hum Genet 62:1009–1014
Chateauvieux S, Morceau F, Dicato M, Diederich M (2010) Molecular and therapeutic potential and toxicity of valproic acid. J Biomed Biotechnol 2010
Marson AG, Al-Kharusi AM, Alwaidh M et al (2007) The SANAD study of effectiveness of valproate, lamotrigine, or topiramate for generalised and unclassifiable epilepsy: an unblinded randomised controlled trial. Lancet 369:1016–1026
Oyrer J, Maljevic S, Scheffer IE, Berkovic SF, Petrou S, Reid CA (2018) Ion channels in genetic epilepsy: from genes and mechanisms to disease-targeted therapies. Pharmacol Rev 70:142–173
Catterall WA, Kalume F, Oakley JC (2010) NaV1.1 channels and epilepsy. J Physiol 588:1849–1859
Szulczyk B, Nurowska E (2017) Valproic acid inhibits TTX-resistant sodium currents in prefrontal cortex pyramidal neurons. Biochem Biophys Res Commun 491:291–295
Löscher W (1999) Valproate: a reappraisal of its pharmacodynamic properties and mechanisms of action. Prog Neurobiol 58:31–59
Johannessen CU (2000) Mechanisms of action of valproate: a commentatory. Neurochem Int 37:103–110
Zuliani V, Fantini M, Rivara M (2012) Voltage-gated sodium channels as therapeutic targets in epilepsy and other neurological disorders. Curr Top Med Chem 12:962–970
Catterall WA (2014) Sodium channels, inherited epilepsy, and antiepileptic drugs. Annu Rev Pharmacol Toxicol 54:317–338
Yu FH, Mantegazza M, Westenbroek RE, Robbins CA, Kalume F, Burton KA, Spain WJ, McKnight GS, Scheuer T, Catterall WA (2006) Reduced sodium current in GABAergic interneurons in a mouse model of severe myoclonic epilepsy in infancy. Nat Neurosci 9:1142–1149
Haerian BS, Baum L, Tan HJ, Kwan P, Raymond AA, Saruwatari J, Nakagawa K, Mohamed Z (2012) SCN1AIVS5N+5 polymorphism and response to sodium valproate: a multicenter study. Pharmacogenomics 13:1477–1485
Yip TS, O'Doherty C, Tan NC, Dibbens LM, Suppiah V (2014) SCN1A variations and response to multiple antiepileptic drugs. Pharmacogenomics J 14:385–389
Li X, Zhang J, Wu X, Yan H, Zhang Y, He RH, Tang YJ, He YJ, Tan D, Mao XY, Yin JY, Liu ZQ, Zhou HH, Liu J (2016) Polymorphisms of ABAT, SCN2A and ALDH5A1 may affect valproic acid responses in the treatment of epilepsy in Chinese. Pharmacogenomics 17:2007–2014
Duan SH, Ma JL, Yang XL, Guo YF (2017) Simultaneous multigene mutation screening using SNPscan in patients from ethnic minorities with nonsyndromic hearingimpairment in Northwest China. Mol Med Rep 16:6722–6728
Ma CL, Wu XY, Jiao Z, Hong Z, Wu ZY, Zhong MK (2014) Association of SCN1A, SCN2A and ABCC2 gene polymorphisms with the response to antiepileptic drugs in Chinese Han patients with epilepsy. Pharmacogenomics 15:1323–1336
Zhou BT, Zhou QH, Yin JY, Li GL, Qu J, Xu XJ, Liu D, Zhou HH, Liu ZQ (2012) Effects of SCN1A and GABA receptor genetic polymorphisms on carbamazepine tolerability and efficacy in Chinese patients with partial seizures: 2-year longitudinal clinical follow-up. CNS Neurosci Ther 18:566–572
Zhou BT, Zhou QH, Yin JY, Li GL, Xu XJ, Qu J, Liu D, Zhou HH, Liu ZQ (2012) Comprehensive analysis of the association of SCN1A gene polymorphisms with the retention rate of carbamazepine following monotherapy for new-onset focal seizures in the Chinese Han population. Clin Exp Pharmacol Physiol 39:379–384
Manna I, Gambardella A, Bianchi A, Striano P, Tozzi R, Aguglia U, Beccaria F, Benna P, Campostrini R, Canevini MP, Condino F, Durisotti C, Elia M, Giallonardo AT, Iudice A, Labate A, la Neve A, Michelucci R, Muscas GC, Paravidino R, Zaccara G, Zucca C, Zara F, Perucca E (2011) A functional polymorphism in the SCN1A gene does not influence antiepileptic drug responsiveness in Italian patients with focal epilepsy. Epilepsia 52:e40–e44
Zhou L, Cao Y, Long H, Long L, Xu L, Liu Z, Zhang Y, Xiao B (2015) ABCB1, ABCC2, SCN1A, SCN2A, GABRA1 gene polymorphisms and drug resistant epilepsy in the Chinese Han population. Pharmazie 70:416–420
Sánchez MB, Herranz JL, Leno C, Arteaga R, Oterino A, Valdizán EM, Nicolás JM, Adín J, Armijo JA (2010) Genetic factors associated with drug-resistance of epilepsy: relevance of stratification by patient age and aetiology of epilepsy. Seizure 19:93–101
Yun W, Zhang F, Hu C, Luo X, Xue P, Wang J, Ge Y, Meng H, Guo Y (2013) Effects of EPHX1, SCN1A and CYP3A4 genetic polymorphisms on plasma carbamazepine concentrations and pharmacoresistance in Chinese patients with epilepsy. Epilepsy Res 107:231–237
Haerian BS, Baum L, Kwan P, Tan HJ, Raymond AA, Mohamed Z (2013) SCN1A, SCN2A and SCN3A gene polymorphisms and responsiveness to antiepileptic drugs: a multicenter cohort study and meta-analysis. Pharmacogenomics 14:1153–1166
Hung CC, Chang WL, Ho JL, Tai JJ, Hsieh TJ, Huang HC, Hsieh YW, Liou HH (2012) Association of polymorphisms in EPHX1, UGT2B7, ABCB1, ABCC2, SCN1A and SCN2A genes with carbamazepine therapy optimization. Pharmacogenomics 13:159–169
Tate SK, Depondt C, Sisodiya SM, Cavalleri GL, Schorge S, Soranzo N, Thom M, Sen A, Shorvon SD, Sander JW, Wood NW, Goldstein DB (2005) Genetic predictors of the maximum doses patients receive during clinical use of the anti-epileptic drugs carbamazepine and phenytoin. Proc Natl Acad Sci U S A 102:5507–5512
Tate SK, Singh R, Hung CC, Tai JJ, Depondt C, Cavalleri GL, Sisodiya SM, Goldstein DB, Liou HH (2006) A common polymorphism in the SCN1A gene associates with phenytoin serum levels at maintenance dose. Pharmacogenet Genomics 16:721–726
Eliasson E, Lindh JD, Malmström RE, Beck O, Dahl ML (2013) Therapeutic drug monitoring for tomorrow. Eur J Clin Pharmacol 69(Suppl 1):25–32
Copley RR (2004) Evolutionary convergence of alternative splicing in ion channels. Trends Genet 20:171–176
Heinzen EL, Yoon W, Tate SK, Sen A, Wood NW, Sisodiya SM, Goldstein DB (2007) Nova2 interacts with a cis-acting polymorphism to influence the proportions of drug-responsive splice variants of SCN1A. Am J Hum Genet 80:876–883
Fletcher EV, Kullmann DM, Schorge S (2011) Alternative splicing modulates inactivation of type 1 voltage-gated sodium channels by toggling an amino acid in the first S3-S4 linker. J Biol Chem 286:36700–36708
Anderson LL, Hawkins NA, Thompson CH, Kearney JA, George AL Jr (2017) Unexpected efficacy of a novel sodium channel modulator in Dravet syndrome. Sci Rep 7:1682
Brunklaus A, Ellis R, Reavey E, Forbes GH, Zuberi SM (2012) Prognostic, clinical and demographic features in SCN1A mutation-positive Dravet syndrome. Brain 135:2329–2336
Younus I, Reddy DS (2017) Epigenetic interventions for epileptogenesis: a new frontier for curing epilepsy. Pharmacol Ther 177:108–122
Kumari R, Lakhan R, Kumar S, Garg RK, Misra UK, Kalita J, Mittal B (2013) SCN1AIVS5-91G>A polymorphism is associated with susceptibility to epilepsy but not with drug responsiveness. Biochimie 95:1350–1353
Tang L, Lu X, Tao Y, Zheng J, Zhao P, Li K, Li L (2014) SCN1A rs3812718 polymorphism and susceptibility to epilepsy with febrile seizures: a meta-analysis. Gene 533:26–31
Kwan P, Poon WS, Ng HK, Kang DE, Wong V, Ng PW, Lui CH, Sin NC, Wong KS, Baum L (2008) Multidrug resistance in epilepsy and polymorphisms in the voltage-gated sodium channel genes SCN1A, SCN2A, and SCN3A: correlation among phenotype, genotype, and mRNA expression. Pharmacogenet Genomics 18:989–998
Acknowledgments
We thank all patients and their family members who contributed to this work. We thank Professor Shusen Sun from College of Pharmacy and Health Sciences at Western New England University, USA, for his valuable advice.
Contributions of authors
Zanling Zhang designed the study. Lihong Shi performed the data analysis and wrote the manuscript. Miaomiao Zhu, Huilan Li, and Zhipeng Wen recruited patients and conducted patients’ follow-up. Jia Luo and Cong Lin extracted the DNA. Xiaoping Chen reviewed the manuscript and critically revised the intellectual content of the manuscript.
Funding
This work was supported by a grant from the Natural Science Foundation of Hunan Province (no. 2017JJ2398).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of Xiangya Hospital Central South University Medical Ethics Committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 19 kb)
Rights and permissions
About this article

Cite this article
Shi, L., Zhu, M., Li, H. et al. SCN1A and SCN2A polymorphisms are associated with response to valproic acid in Chinese epilepsy patients. Eur J Clin Pharmacol 75, 655–663 (2019). https://doi.org/10.1007/s00228-019-02633-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-019-02633-0