
Abstract
Patients with systemic mastocytosis (SM) are at high risk of bone deterioration. However, the evaluation of bone microarchitecture in this disease remains unclear. We aimed to assess bone microarchitecture in patients with SM. This was a cross-sectional study of 21 adult patients with SM conducted in a quaternary referral hospital in Sao Paulo, Brazil. A healthy, age-, weight-, and sex-matched cohort of 63 participants was used to provide reference values for bone microarchitecture, assessed by high resolution peripheral quantitative computed tomography (HR-pQCT). Total volumetric bone mineral density (vBMD), cortical vBMD, and cortical thickness at the radius were significantly lower in the control group compared with the SM group (all P < 0.001). Patients with aggressive SM had significantly lower trabecular number (Tb.N) (P = 0.035) and estimated failure load (F.load) (P = 0.032) at the tibia compared with those with indolent SM. Handgrip strength was significantly higher in patients who had more Tb.N at the radius (ρ, 0.46; P = 0.036) and tibia (ρ, 0.49; P = 0.002), and lower who had more trabecular separation at the radius (ρ, −0.46; P = 0.035) and tibia (ρ, −0.52; P = 0.016). Strong and positive associations between F.load (ρ, 0.75; P < 0.001) and stiffness (ρ, 0.70; P < 0.001) at the radius, and between F.load at the tibia (ρ, 0.45; P = 0.038) were observed with handgrip strength. In this cross-sectional study, aggressive SM was more susceptible to bone deterioration compared with indolent SM. In addition, the findings demonstrated that handgrip strength was associated with bone microarchitecture and bone strength.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Systemic mastocytosis (SM) is a rare hematological disease characterized by abnormal proliferation and accumulation of mast cells in various organs, mainly skin and bone marrow [1, 2]. Patients with SM are at high risk of bone deterioration and fragility fractures [3,4,5,6]. Although the mechanisms of bone loss in SM remain unknown [7, 8], it has been suggested that allergic mediators such as histamine and tryptase may act by increasing the activity of osteoclasts, leading to an increase in bone resorption [9, 10].
A comprehensive assessment of bone in SM is scarce, with dual-energy X-ray absorptiometry (DXA) being the most used method in previous studies [4,5,6]. In patients with SM, most fragility fractures may occur with normal bone mineral density (BMD), which requires assessment of bone-related quality parameters. DXA provides information on trabecular compartment based on lumbar spine textural index (Trabecular Bone Score, TBS) [11], bone deformation (Bone Strain Index) [12], and bone cross-sectional geometry (Hip Structural Analysis) [13]. However, volumetric evaluation of bone tissue is not possible by DXA. In this context, high resolution peripheral quantitative computed tomography (HR-pQCT) emerges as an important technology that allows performing in vivo assessment of three dimensions high-definition bone structural measures [14]. Furthermore, the use of finite element models can estimate biomechanical properties of the tissue [14].
The objective of this study was to evaluate bone microarchitecture and bone strength using HR-pQCT in patients with SM, and their associations with clinical and biochemical parameters of the disease.
Methods
This was a cross-sectional study in which patients with SM underwent a comprehensive evaluation of bone and were compared with a cohort of healthy individuals. The study was approved by the ethics committee of the Hospital das Clinicas of the School of Medicine of the University of Sao Paulo (#19821519.0.0000.0068, date of approval September 4, 2019) and all the patients provided written informed consent before participation.
Participants
Patients with SM who fulfilled the WHO 2016 criteria [15] were recruited from Outpatient Hematology Clinic of the Hospital das Clinicas of the University of Sao Paulo, and were referred to the Rheumatology Division of the same institution for evaluation of bone parameters. Our institution is a public quaternary referral teaching hospital responsible for high complexity care. Patients were enrolled from October 2020 to June 2022, and the final analysis was in June 2022. To provide reference values for all measurements, we included a group of healthy adult participants whose data were obtained from a cohort who have participated in studies by our research group aimed to establish age-related reference curves for bone microarchitecture and strength [16, 17]. The control group was matched by age, weight, and sex in a ratio of 1:3.
Outcomes
HR-pQCT
The primary outcome was bone microarchitecture assessed by HR-pQCT. The distal radius and distal tibia were scanned using a first-generation HR-pQCT scanner (XtremeCT I, Scanco Medical AG, Brüttisellen, Switzerland). The measurements included 110 slices, corresponding to a 9.02 mm scan area (voxel size of 82 μm), positioned 9.5 mm and 22.5 mm proximal to the reference line for the distal radius and distal tibia, respectively. The variables measured were volumetric BMD (vBMD), structural parameters, and cortical porosity.
Finite Element Models
Finite element models were performed to estimate bone strength from HR-pQCT measurements using a specific software (Finite Element software v. 1.13, Scanco Medical AG, Switzerland). Models of the distal radius and distal tibia were generated directly from the HR-pQCT images (Image Processing Language and Finite Element Extension (IPLFE), Scanco Medical AG, Switzerland). The parameters obtained were estimated failure load (F.Load) and stiffness.
DXA
BMD Z-score and T-score at the lumbar spine, total hip, and femoral neck were measured using a DXA device (Lunar iDXA, GE Healthcare, Madison, WI).
TBS was assessed by the software TBS iNsight® version 2.1 (Medimaps, Bordeaux, France). It was analyzed as the mean value of the measurements of the L1–L4 vertebrae in the same region as the DXA images of the lumbar spine.
Vertebral fracture assessment (VFA) was obtained by lateral DXA scanning of the T4–L4 vertebrae. Assessments of vertebral fractures were performed using the method described by Genant et al. [18].
Handgrip Strength
Handgrip strength was assessed to obtain the maximum isometric strength of the dominant hand using a hydraulic hand dynamometer (SAEHAN SH5001, Saehan Corp.). Measurements were obtained with the participants in the sitting position and elbow flexed at 90°, and all assessments were performed by the same trained technician.
Biochemical Disease-related Markers
Quantification of KIT D816V mutation was performed by digital polymerase chain reaction (dPCR) [19]. Genomic DNA was obtained from peripheral blood leukocyte buttons collected in an EDTA tube. DNA extraction was performed using the QIAamp DNA Midi Kit (Qiagen, Ger) using 5 × 106 cells, and the concentration of the obtained DNA was measured on the NanoDrop 2000 spectrophotometer (Thermo Fisher, USA). The search for the D816V mutation by dPCR was performed with 50 ng of genomic DNA using the QuantStudio™ 3D dPCR mastermix V2 (Thermo Fisher, USA), and the Kit_1314 assay (ID Hs000000039_rm), according to the manufacturer's protocol. QuantStudio™ 3D dPCR AnalysisSuit software was used for the analysis of the results.
Serum tryptase levels were measured by fluorimetric immunoassay, with reference values between 1 and 15 μg/L and values greater than 20 μg/L was considered as a minor criterion for systemic mastocytosis.
Mastocytosis Activity Score
Disease activity was measured using the Mastocytosis Activity Score [20]. This questionnaire was performed by the same trained physician.
Bone Turnover Markers
Serum C-terminal telopeptide of type 1 collagen (CTX) and Procollagen type 1 N-terminal propeptide (P1NP) concentrations were determined by an automated electrochemiluminescence system (E411; Roche Diagnostics, Mannheim, Germany). Serum CTX and P1NP limits of detection were 10 ng/L and 5 mg/L, respectively.
Statistical Analysis
Data are presented as mean ± SD or median (IQR) and estimated difference between groups with 95% CI for continuous variables and as percentages for categorical variables. We used mixed models assuming group as fixed factor and subjects as a random factor to compare patients with SM and healthy individuals. Subgroup analyses using the Mann–Whitney U test were performed to compare patients with aggressive SM (aSM) and indolent SM (iSM). Spearman rank correlation (ρ) was used to measure the associations between handgrip strength and disease-related markers with bone parameters. Percentages were compared between groups using Fisher's exact test. All tests were 2-sided and the significance level was set to α = 0.05. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Patients
Of 30 patients assessed for eligibility in the SM group, 21 were eligible and included in the study. Of the 9 patients not included, 3 died before the assessments, 2 had cutaneous mastocytosis, 2 refused to participate, 1 did not have a confirmed diagnosis, and 1 did not have personal contact in our medical record. Of the 21 patients, 3 (14.3%) were men (Table 1), 15 (71.4%) had iSM, 6 (28.6%) had aSM, 6 (28.6%) had low bone mass, and 3 (14.3%) had osteoporosis (Table 2). No significant differences between the control group and the SM group were observed for age, weight, body mass index, sex, and race (Table 1).
Primary Outcome
Total vBMD (difference, − 61.0 mgHA/cm3 [95% CI − 91.3 to − 30.7]; P < 0.001) and cortical vBMD (difference, − 76.0 mgHA/cm3 [95% CI − 110.1 to − 42.0]; P < 0.001) at the radius were significantly lower in the control group compared with the SM group (Table 1). In addition, cortical thickness at the same bone site significantly differed between the control group and the SM group (difference, –0.27 mm [95% CI − 0.36 to − 0.17]; P < 0.001) (Table 1). No significant differences between the groups were observed for any other bone microarchitecture parameters.
Secondary Outcomes
Stiffness and F.load at the radius and tibia did not significantly differ between the groups. BMD Z-score at the lumbar spine was significantly lower in the SM group compared with the control group (difference, − 0.68 [95% CI, − 1.36 to − 0.01]; P = 0.047) (Table 1). The SM group had significantly more vertebral fractures compared with the control group (14.3% vs. 0%, P = 0.014) (Table 1). No other significant differences were observed in BMD Z-score, T-score, and TBS (Table 1).
Subgroup Analyses and Associations Between Handgrip Strength and Disease-related Markers with Bone Parameters
Subgroup analyses demonstrated that aSM group had significantly lower trabecular number (Tb.N) (difference, − 0.56 1/mm [95% CI − 1.04 to − 0.07]; P = 0.035) (Fig. 1A) and F.load (difference, − 1269.0 N [95% CI − 3417.0 to − 173.0; P = 0.032) at the tibia compared with iSM group (Fig. 1B). No significant differences were observed for the other parameters of bone microarchitecture, bone strength, TBS, and VFA (Table 2). Handgrip strength, biochemical disease-related markers, disease activity, and serum bone turnover markers did not significantly differ between the aSM and the iSM (Table 2).

Subgroup analyses. A Trabecular number (Tb.N) at the tibia. B Estimated failure load (F.load) at the tibia. Boxes represent median and interquartile range with whiskers extending to the highest and lowest values within 1.5 IQR of the 25th and 75th percentiles. Outliers are represented with dots
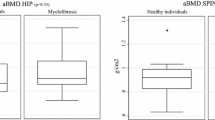
Handgrip strength was significantly higher in patients who had more Tb.N at the radius (ρ, 0.46, [95% CI 0.02–0.74]; P = 0.036) (Fig. 2A) and tibia (ρ, 0.49, [95% CI 0.06–0.76]; P = 0.002) (Fig. 2B), and lower who had more trabecular separation (Tb.Sp) at the radius (ρ, − 0.46, [95% CI − 0.74 to − 0.03]; P = 0.035) (Fig. 2C) and tibia (ρ, − 0.52, [95% CI − 0.77 to − 0.10]; P = 0.016) (Fig. 2D). Also, handgrip strength was strongly and positively associated with F.load (ρ, 0.75, [95% CI 0.46–0.89]; P < 0.001) (Fig. 3A) and stiffness (ρ, 0.70, [95% CI 0.37–0.87]; P < 0.001) (Fig. 3B) at the radius, and with F.load at the tibia (ρ, 0.45, [95% CI 0.02–0.74]; P = 0.038) (Fig. 3C).

Associations between handgrip strength and bone microarchitecture. A Trabecular number (Tb.N) at the radius. B Tb.N at the tibia. C Trabecular Separation (Tb.Sp) at the radius. D, Tb.Sp at the tibia

Associations between handgrip strength, serum tryptase levels and bone strength. A Estimated failure load (F.load) at the radius. B Stiffness at the radius. C F.load at the tibia. D F.load at the radius
Serum tryptase levels were significantly and negatively associated with F.load at the radius (ρ, − 0.46, [95% CI, − 0.74 to − 0.01]; P = 0.040) (Fig. 3D). No significant associations were observed between the age of the patients, the allele burden of the KIT D816V mutation, Mastocytosis Activity Score, and TBS with bone parameters and with handgrip strength.
Discussion
In this cross-sectional study, we found that SM group significantly differ in some bone structural measurements when compared with healthy individuals. Trabecular compartments of the tibia were lower in the aSM, possibly causing a reduction in bone strength. In addition, handgrip strength was associated with trabecular parameters and bone strength of the radius and tibia. To our knowledge, this is the first study to comprehensively assess bone using HR-pQCT in SM.
In SM, the accumulation of mast cells increases the levels of histamine, tryptase and cytokines, which may have a role in bone impairment. Approximately 0.5% of all causes of osteoporosis are derived from SM [10]. However, in young males, SM is responsible for 6% of secondary osteoporosis. Cohort studies show that patients with SM have 20–28% osteoporosis and 28–37% fragility fracture [5,6,7,8, 21].
Degboé et al. showed that bone marrow tryptase levels are associated with fragility fractures [6]. Our study did not show this relationship, but we observed an inverse association between serum tryptase levels and F.load at the radius.
Studies with knockout rodents of the enzyme histamine decarboxylase showed a lower number of osteoclasts and an increase in bone formation, indicating the role of this mediator on bone metabolism [22]. Moreover, histamine is involved in activating the RANK-RANKL system, which stimulates osteoclastogenesis [23]. Finally, in vitro studies using H1 and H2 histamine receptor antagonists showed a reduction in the number of osteoclasts [24].
In our study, although some cortical compartments of the radius were higher in SM, lumbar spine Z-score were lower compared with the control group, suggesting that SM may decrease the trabecular bone to a greater extent. Subgroup analyses may support this observation, as the Tb.N at the tibia was more affected in the aSM, possibly leading to a reduction in the F.load. Our findings corroborate with other studies that show impaired BMD at the lumbar spine and vertebral fractures in patients with SM when compared with healthy individuals [8, 10, 25].
Handgrip strength is a low-cost, easy-to-implement method for accurately measuring muscle strength. A recent study demonstrated that handgrip strength was associated with bone erosion assessed by HR-pQCT in patients with rheumatoid arthritis [26]. Our findings showed associations between handgrip strength and Tb.N and Tb.Sp at both radius and tibia, in addition to strong correlations with biomechanical parameters, suggesting that this method may be useful for estimating bone deterioration in SM.
The limitations of this study include the small sample size and single-center observational design. Although the SM is a rare disease, with about one case in sixty thousand, all patients treated at our referral hospital were included in the sample. In addition, the high mortality rate due to the poor prognosis of aSM resulted in the death of many patients before enrollment in the study, which limited the sample size of this subgroup and precluded the use of multiple regression analysis models to investigate the relationships between outcomes and variables that could represent a bias, particularly for the handgrip findings. Furthermore, we were unable to use bone marrow biopsies for histomorphometric analysis, which could elucidate mechanisms of bone loss.
Despite the challenges of conducting a study on a rare disease, our findings will contribute to the understanding of this disease and potential treatment options. The findings should be considered exploratory and hypothesis-generating. Further studies should confirm our results.
Conclusion
Among patients with SM, bone microarchitecture and bone strength were more affected in aSM compared with iSM. Associations between handgrip strength and parameters of bone microarchitecture and bone biomechanical were also observed, suggesting that handgrip strength may be a feasible method to estimate bone deterioration in the SM.
References
Pardanani A (2021) Systemic mastocytosis in adults: 2021 Update on diagnosis, risk stratification and management. Am J Hematol 96:508–525
Theoharides TC, Valent P, Akin C (2015) Mast cells, mastocytosis, and related disorders. N Engl J Med 373:163–172
Broesby-Olsen S, Farkas DK, Vestergaard H, Hermann AP, Møller MB, Mortz CG, Kristensen TK, Bindslev-Jensen C, Sørensen HT, Frederiksen H (2016) Risk of solid cancer, cardiovascular disease, anaphylaxis, osteoporosis and fractures in patients with systemic mastocytosis: a nationwide population-based study. Am J Hematol 91:1069–1075
Rossini M, Zanotti R, Bonadonna P, Artuso A, Caruso B, Schena D, Vecchiato D, Bonifacio M, Viapiana O, Gatti D, Senna G, Riccio A, Passalacqua G, Pizzolo G, Adami S (2011) Bone mineral density, bone turnover markers and fractures in patients with indolent systemic mastocytosis. Bone 49:880–885
van der Veer E, van der Goot W, de Monchy JG, Kluin-Nelemans HC, van Doormaal JJ (2012) High prevalence of fractures and osteoporosis in patients with indolent systemic mastocytosis. Allergy 67:431–438
Degboé Y, Eischen M, Nigon D, Apoil PA, Mailhol C, Tournier E, Laurent C, Hanssens K, Hermine O, Paul C, Laroche M, Bulai-Livideanu C (2017) Prevalence and risk factors for fragility fracture in systemic mastocytosis. Bone 105:219–225
Orsolini G, Viapiana O, Rossini M, Bonifacio M, Zanotti R (2018) Bone disease in mastocytosis. Immunol Allergy Clin North Am 38:443–454
Rossini M, Zanotti R, Viapiana O, Tripi G, Orsolini G, Idolazzi L, Bonadonna P, Schena D, Escribano L, Adami S, Gatti D (2014) Bone involvement and osteoporosis in mastocytosis. Immunol Allergy Clin North Am 34:383–396
Seitz S, Barvencik F, Koehne T, Priemel M, Pogoda P, Semler J, Minne H, Pfeiffer M, Zustin J, Püschel K, Eulenburg C, Schinke T, Amling M (2013) Increased osteoblast and osteoclast indices in individuals with systemic mastocytosis. Osteoporos Int 24:2325–2334
Gehlen M, Schmidt N, Pfeifer M, Balasingam S, Schwarz-Eywill M, Maier A, Werner M, Siggelkow H (2021) Osteoporosis caused by systemic mastocytosis: prevalence in a Cohort of 8392 patients with osteoporosis. Calcif Tissue Int 109:685–695
Hans D, Barthe N, Boutroy S, Pothuaud L, Winzenrieth R, Krieg MA (2011) Correlations between trabecular bone score, measured using anteroposterior dual-energy X-ray absorptiometry acquisition, and 3-dimensional parameters of bone microarchitecture: an experimental study on human cadaver vertebrae. J Clin Densitom 14:302–312
Ulivieri FM, Rinaudo L (2022) The bone strain index: an innovative dual X-ray absorptiometry bone strength index and its helpfulness in clinical medicine. J Clin Med 11:2284–2296
Ulivieri FM, Rinaudo L, Piodi LP, Barbieri V, Marotta G, Sciumè M, Grifoni FI, Cesana BM (2020) Usefulness of dual X-ray absorptiometry-derived bone geometry and structural indexes in mastocytosis. Calcif Tissue Int 107:551–558
Fuller H, Fuller R, Pereira RM (2015) High resolution peripheral quantitative computed tomography for the assessment of morphological and mechanical bone parameters. Rev Bras Reumatol 55:352–362
Valent P, Akin C, Metcalfe DD (2017) Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood 129:1420–1427
Alvarenga JC, Fuller H, Pasoto SG, Pereira RM (2017) Age-related reference curves of volumetric bone density, structure, and biomechanical parameters adjusted for weight and height in a population of healthy women: an HR-pQCT study. Osteoporos Int 28:1335–1346
Alvarenga JC, Caparbo VF, Domiciano DS, Pereira RMR (2022) Age-related reference data of bone microarchitecture, volumetric bone density, and bone strength parameters in a population of healthy Brazilian men: an HR-pQCT study. Osteoporos Int 33:1309–1321
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148
Greiner G, Gurbisz M, Ratzinger F, Witzeneder N, Simonitsch-Klupp I, Mitterbauer-Hohendanner G, Mayerhofer M, Müllauer L, Sperr WR, Valent P, Hoermann G (2018) Digital PCR: a sensitive and precise method for KIT D816V quantification in mastocytosis. Clin Chem 64:547–555
Siebenhaar F, Sander B, Ho LHT, Ellrich A, Maurer M, Weller K (2018) Development and validation of the mastocytosis activity score. Allergy 73:1489–1496
Guillaume N, Desoutter J, Chandesris O, Merlusca L, Henry I, Georgin-Lavialle S, Barete S, Hirsch I, Bouredji D, Royer B, Gruson B, Lok C, Sevestre H, Mentaverri R, Brazier M, Meynier J, Hermine O, Marolleau JP, Kamel S, Damaj G (2013) Bone complications of mastocytosis: a link between clinical and biological characteristics. Am J Med 126:75.e71-77
Fitzpatrick LA, Buzas E, Gagne TJ, Nagy A, Horvath C, Ferencz V, Mester A, Kari B, Ruan M, Falus A, Barsony J (2003) Targeted deletion of histidine decarboxylase gene in mice increases bone formation and protects against ovariectomy-induced bone loss. Proc Natl Acad Sci USA 100:6027–6032
Biosse-Duplan M, Baroukh B, Dy M, de Vernejoul MC, Saffar JL (2009) Histamine promotes osteoclastogenesis through the differential expression of histamine receptors on osteoclasts and osteoblasts. Am J Pathol 174:1426–1434
Dobigny C, Saffar JL (1997) H1 and H2 histamine receptors modulate osteoclastic resorption by different pathways: evidence obtained by using receptor antagonists in a rat synchronized resorption model. J Cell Physiol 173:10–18
Degboé Y, Eischen M, Apoil PA, Mailhol C, Dubreuil P, Hermine O, Paul C, Bulai Livideanu C, Laroche M (2019) Higher prevalence of vertebral fractures in systemic mastocytosis, but not in cutaneous mastocytosis and idiopathic mast cell activation syndrome. Osteoporos Int 30:1235–1241
Figueiredo CP, Perez MO, Sales LP, Domiciano DS, Sampaio-Barros MM, Caparbo VF, Pereira RMR (2022) Lower hand grip in rheumatoid arthritis patients is associated with low finite element analysis using high resolution peripheral quantitative computed tomography scan of the 2nd metacarpophalangeal joint. Int J Rheum Dis 25:1038–1045
Funding
This study was supported by Sao Paulo Research Foundation (FAPESP) (grants 19/24782-4).
Author information
Authors and Affiliations
Contributions
ASF had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: ASF, IHM, EDRPV, RMRP.Acquisition, analysis, and interpretation: All authors. Drafting of the manuscript: ASF, IHM. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: ASF, IHM, EDRPV. Obtained funding: EDRPV, RMRP. Supervision: EDRPV, RMRP. Administrative, technical, or material support: LT, VFC. Dra Luciana Nardinelli (Laboratory of Tumor Biology of Hospital das Clínicas da FMUSP for performing the dPCR KIT D816V studies) and Dr. Elaine Aparecida Rosseto (Clinical Laboratory of Hospital Israelita Albert Einstein) for performing tryptase tests. The authors are thankful to all the patients who participated in this study. All the individuals described in this section received no compensation for their participation in the study.
Corresponding author
Ethics declarations
Conflict of interest
Andre S. Franco, Igor H. Murai, Liliam Takayama, Valeria F. Caparbo, Luan L. Marchi, Elvira D. R. P. Velloso, and Rosa M. R. Pereira declare that they have no conflict of interest.
Role of the Funder/Sponsor
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Human and Animal Rights and Informed Consent
The study was approved by the ethics committee of the Hospital das Clinicas of the School of Medicine of the University of Sao Paulo (#19821519.0.0000.0068, date of approval September 4, 2019) and all the patients provided written informed consent before participation.
Additional information
Rosa M. R. Pereira in memoriam.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Franco, A.S., Murai, I.H., Takayama, L. et al. Assessment of Bone Microarchitecture in Patients with Systemic Mastocytosis and its Association with Clinical and Biochemical Parameters of the Disease. Calcif Tissue Int 113, 276–285 (2023). https://doi.org/10.1007/s00223-023-01107-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-023-01107-x