
Abstract
The aim of this study was to analyze the efficacy of using rhBMP-2 (recombinant human morphogenetic protein-2) in the treatment of patients with cleft lip and palate defects (CLPD). Seven databases were screened: PubMed (Medline), Lilacs, Ibecs, Web of Science, BBO, Scopus, and The Cochrane Library. Clinical trials that evaluated the use of bioactive treatment with rhBMP-2 in the treatment of patients with CLPD were included. Statistical analyses were performed by comparing the standardized mean difference of bone formation volume and bone filling percentage (p = 0.05). Ten studies compared the use of rhBMP-2 and iliac crest bone graft (ICBG). The global analysis for bone formation volume and bone filling percentage showed that bioactive materials were similar to ICBG with a standardized mean difference of respectively 0.07 (95% CI − 0.41 to 0.56) and 0.24 (95% CI − 0.32 to 0.80). The available literature suggested that use of rhBMP-2 presented similar bone formation results to those of ICBG in secondary alveolar bone grafting for patients with CLPD.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cleft lip and cleft palate are the most common congenital facial malformations that occur during the fourth to tenth week of gestation in 0.36–0.83 of 1000 live-born infants as a result of deficient union of the oropalatal shelves and nasal process [1,2,3,4]. Over half of the cases present cleft of the alveolus [4]. The treatment may involve a multidisciplinary approach with a long-term follow-up and multiple surgeries [5]. Usually children face several surgical stages such as lip closure within the first 3 months of birth, and palate around 2 years of age [6]. Currently, secondary alveolar bone grafting is considered the mainstay of treatment, being recommended during the mixed dentition period and before permanent canine eruption, between 7 and 12 years of age, to provide adequate periodontal support with no detrimental effect on maxillary growth [5,6,7]. This procedure aims to stabilize the maxillary dental arch; close the residual oronasal fistula; provide support for the lip and nose, and bone support for the teeth adjacent to the cleft area [5, 6].
Despite recent advances in regenerative dentistry, reconstruction of maxillofacial defects remains a challenge. In some patients with alveolar cleft and cleft lip, it is difficult to augment the bone defect adequately because of the width of the gap, or as a result of bone resorption [8,9,10]. Grafting of the defective site can be performed with different biomaterials, with autologous bone grafts being the gold standard, because they provide osteogenic cells, as well as essential osteoinductive factors needed for bone healing and regeneration, stimulating bone regeneration through osteoinduction while avoiding an immunologic reaction [4, 11]. These bone grafts can be taken from the patient’s iliac crest, mandibular symphysis, rib, tibia, and calvarium [4]. Among them, the illiac crest bone graft (ICBG) obtained from the anterior iliac bone was first reported for alveolar repair by Boyne and Sands [8]. Nowadays, ICBG is the standard procedure, with success rates higher than 88% [3, 8, 9, 12]. However, ICBG is associated with significant donor-site morbidity and potential for serious complications, (such as infection, pain, hemorrhage, and nerve injury) [3, 13,14,15,16]. These complications are reported in approximately 8% of patients [17]. Although ICBG provides one of the most biocompatible options for alveolar and palate cleft defects, its disadvantages have driven the search for better alternatives such as the use of bioactive materials containing proteins.
Bone morphogenetic proteins (BMPs) are a group of bioactive proteins with osteoinductive properties that are part of the transforming growth factor superfamily [3, 18, 19]. They were first described by Urist and Strates [20, 21] as a factor within the bone matrix that has the capability of inducing bone formation through bone-forming cells. Wozney et al. [22] sequenced recombinant human bone morphogenetic protein (rhBMP) in 1989 and cloned it, which allowed the production of large and pure quantities of this bioactive protein. In the early 1990s, it became possible to produce rhBMP synthetically by using recombinant technology [23]. From there, clinical studies involving spine fusions and nonunion of long bones were performed, especially using rhBMP-2 associated with absorbable collagen sponge (ACS), which demonstrated efficacy and safety for human application [23, 24]. The use of these novel biological treatments is an example of formation of the tissue engineering triangle, in an attempt to develop more biocompatible materials that induce the best tissue response with the least damaging response from the patient [25, 26].
Alveolar and palate cleft defect reconstruction continues to pose a significant challenge to maxillofacial surgeons, and although ICBG has been routinely used, its limitations have driven the search for and development of alternative treatments using bioactive proteins for bone repair and regeneration. Therefore, the aim of this study was to analyze the efficacy of using rhBMP-2 (recombinant human morphogenetic protein-2) in secondary alveolar bone grafting for patients with cleft lip and palate defects. Our hypothesis was that the use of bioactive proteins would present similar performance relative to bone formation in cleft lip and palate defects when compared with iliac crest bone graft (ICBG).
Materials and Methods
The protocol of this review was registered in the PROSPERO (CRD42017057169) and it was reported according to the PRISMA Statement [27].
Focused Question
To formulate the focused question from evidence-based practice, the following PICO was stated: Population patients with cleft lip and palate defects; Intervention use of rhBMP-2 in biomaterials for bone graft; Comparison use of iliac crest bone graft (ICBG); and Outcome bone formation volume and bone filling percentage. The focused research question was: Would the use of rhBMP-2 show similar outcomes regarding bone formation in cleft lip and palate defects when compared with iliac crest bone graft (ICBG)?
Search Strategies
Two independent reviewers (WLOR and TMS) screened seven databases in search of appropriate papers that satisfied the study purpose as follows: PubMed (Medline), Web of Science, Lilacs, Ibecs, BBO, Scopus and The Cochrane Library, until 14th February 2018. The reviewers also searched the references cited in the articles included. The structured search strategy used in PubMed (Medline) is described in Table 1, which was customized for other databases. Duplicates were removed by using Endnote X7 software (Thompson Reuters, Philadelphia, PA, USA).
Screening and Selection
The titles and abstracts of all of the papers were assessed by two reviewers independently (WLOR and TMS). The following inclusion criteria were used: retrospective or prospective clinical trials; and studies that evaluated the use of bioactive proteins in the treatment of patients with cleft lip and palate defects. Furthermore, only studies published in English were accepted. Review articles, in vitro studies, case series or case reports, and clinical trials without a control group were excluded. Studies that apparently met the inclusion criteria, or for which there were insufficient data in the title and abstract to make a clear decision, were selected for full analysis. Only studies that fulfilled all of the eligibility criteria were included. Any disagreement was resolved by discussion between the reviewers or by a third reviewer (AS).
Data Extraction
The following data were tabulated from all papers included using data extraction sheets: demographic data, study design, number of patients, gender, age, and follow-up of included studies (Table 2). Additionally, the main characteristics of the included papers, such as selection criteria and groups evaluated, were analyzed (Table 3). Moreover, the evaluation methods, main findings, and adverse events reported were also tabulated (Table 4). If there was any information missing, the authors were contacted via e-mail to retrieve any missing data.
Assessment of Risk of Bias
Two reviewers (WLOR and TMS) scored the methodological quality independently according to the Cochrane guidelines [28] within the following parameters: bias due to incomplete data; as well as selection, performance, detection, and reporting bias. Other bias, such as industry sponsorship bias, was also analyzed.
Statistical Analysis
The statistical analyses were performed using Review Manager Software version 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). Thus, the global analysis was carried out using a random-effects model, and pooled-effect estimates were obtained by comparing the standardized mean difference of bone formation volume and bone filling percentage after using bioactive materials containing proteins or autogenous bone graft for cleft lip and palate defects. A p value < 0.05 was considered statistically significant.
Subgroup analysis for outcomes in an evaluation period of up to 6 months, and of at least 12 months was also performed. Multiple groups from the same study were analyzed according to the Cochrane guidelines for combining groups [28]. In addition, sensitivity analyses considering only studies with low risk of bias were performed. Statistical heterogeneity was analyzed using the Cochran’s Q test and the inconsistency I2 test, in which values higher than 50% were considered indicative of substantial heterogeneity [28].
Results
Search Strategy
The article selection process according to the PRISMA Statement is showed in Fig. 1 [27]. Initially, 132 potentially relevant records were identified from all databases. No additional studies were identified after a manual search of the reference lists. After examining the title and abstract, 58 studies were excluded because they did not meet the selection criteria. Of the 13 studies retained for detailed review, 3 were not included because one was a review article [3]; one was an animal experiment [29] and one was a case series [30]. A total of 10 studies fulfilled all of the selection criteria and were included in the qualitative analysis.

Search flow (as described in the PRISMA statement)
Descriptive Analysis
All clinical trials included were published after 2007 (Table 2). Four studies were randomized clinical trials, and five were retrospective studies. A total of 653 subjects were evaluated. All clinical studies had a minimum period of 4 months of follow-up and used ICBG as control. The dose of rhBMP-2 mainly used was 3.2–4.2 mg (1.5 mg/ml). Furthermore, the majority of included studies used an absorbable collagen sponge (Infuse Bone Graft, Medtronic, Memphis, USA) as the protein carrier. Only one study [31] evaluated a hyaluronan-based hydrogel with bioactive protein.
In general, biomaterials containing rhBMP-2 were able to promote bone formation in the majority of included studies. One study reported that a low BMP-2 concentration of 50 mg/ml hydrogel did not induce bone formation after 6 months, but when the concentration was raised to 250 mg/ml, the bone formation increased [31].
Among complications reported for rhBMP-2, the studies reported significant swelling [32,33,34], as well as prolonged wound healing and granulation tissue in one subject [35] who received rhBMP-2. One study [31] also reported a severe gingival swelling during the first week in patients treated with BMP-2 in doses of 250 mg/ml. Furthermore, for ICBG the postoperative intraoral infection rate was significantly higher in one study [7]. Another study reported 3 patients experienced syncopal episodes, and seven cases of post-operatory wound infection [32]. Three clinical trials [32,33,34] also reported significant donor-site pain in ICBG patients, and another study [35] reported that five out of 12 patients presented partial loss of bone graft; one with nearly complete loss of bone graft secondary to wound breakdown and problematic healing.
Meta-analysis
A meta-analysis was performed for eight of the clinical trials included. The subgroup analysis in the evaluation period of up to 6 months and of at least 12 months showed that rhBMP-2 and ICBG were similar with regard to bone formation volume (Figs. 1a, 2b) and bone filling percentage (Fig. 3a, b) (p > 0.05). In addition, the global analysis for bone formation volume (Fig. 2c) and bone filling percentage (Fig. 3c) showed that results obtained with bioactive materials were similar to those of ICBG with a standardized mean difference of 0.07 [95% CI − 0.41 to 0.56] and 0.24 [95% CI − 0.32 to 0.80] respectively. When only randomized clinical trials were considered, the results for bioactive materials were also similar to those of ICBG for bone formation volume and bone filling percentage, with a standardized mean difference of − 0.51 [95% CI − 1.19 to 0.16; I2 = 74%], and 0.57 [95% CI − 0.08 to 1.22; I2 = 40%] respectively. Sensitivity analysis considering only studies with low risk of bias also demonstrated no differences between rhBMP-2 and ICBG, with a standardized mean difference of 0.28 [95% CI − 0.24 to 0.80; I2 = 0%] for bone filling percentage (p = 0.29) and 0.51 [95% CI − 0.80 to 1.81; I2 = 49%] for bone formation volume (p = 0.45).

Forest plot for the bone formation volume analysis with use of bioactive materials containing proteins when compared with iliac crest bone graft (ICBG) for cleft lip and palate treatment. Both treatments were similar in evaluation periods of: up to 6 months (a); at least 12-months (b) and in the global analysis (c)

Forest plot for the bone filling percentage analysis with use of bioactive materials containing proteins when compared with iliac crest bone graft (ICBG) for cleft lip and palate treatment. Both treatments were similar in evaluation periods of: up to 6 months (a), at least 12 months (b) and in the global analysis (c)
Risk of Bias of Included Studies
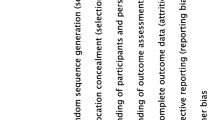
Concerning the quality assessment (Fig. 4), the included studies presented a low risk of bias for incomplete outcome data and other biases. Relative to selection bias (sequence generation, allocation concealment), reporting bias (selective reporting), performance and detection bias (blinding of operators) a low risk of bias was observed in over half of the studies.

Review authors’ judgments about each risk of bias item for each included study
Discussion
The hypothesis tested was accepted, because our meta-analysis demonstrated that bioactive materials with rhBMP-2 in the treatment of cleft lip and palate patients showed similar results to those of ICBG in all analyses performed. The evidence available in the literature suggested that the use of rhBMP-2 presented a performance similar to that of ICBG. The subgroup analysis after 6-month and 12-month periods of follow-up also showed no difference between the two treatment options. It is also important to emphasize that the majority of clinical trials included were randomized and had low risk of bias relative to the parameters analyzed. However, they showed heterogeneity regarding the type; concentration and delivery system of the protein evaluated; evaluation methods; follow-up periods, and outcomes assessed. Despite this evidence of benefits gained by using bioactive materials for bone regeneration and repair of cleft lip and palate defects, further knowledge still needs to be gained about the ideal type of protein and dosage, the interactions of bioactive materials with other proteins, the time course, and their release kinetics [17, 25].
Regeneration of any type of tissue demands the presence of the classical tissue engineering triangle: a signal for bone formation, a source of cells, and a matrix. The U.S. Food and Drug Administration approved the use of rhBMP-2 in human spine fusion procedures, and the introduction of bone morphogenetic proteins in clinical use occurred in cases of spinal fusion and nonunion fractures by orthopedic applications [14, 36]. Studies have reported that the use of rhBMP-2/ACS provided an appropriate signal for induction of bone formation in both tibial and lumbar vertebral fractures, as well as in alveolar ridge preservation and augmentation of the maxillary sinus [22, 23]. Indeed, it seems that the effect of this bioactive material is due the chemoattraction of rhBMP-2/ACS towards osteoprogenitor and stem cells, which serve as sources of bone-forming cells [22].
Regarding scaffolding matrices used for delivering rhBMP-2, the only type at present approved by U.S. Food and Drug Administration is an absorbable collagen sponge (ACS), which the majority of included clinical trials used as the protein carrier for alveolar and cleft defects. This delivery system seems to be ideal for bone tissue engineering, serving as a site for osteoblast attachment, and being reabsorbed within 4–12 weeks [34, 37]. Furthermore, ACSs have good biocompatibility, as they degrade into physiologically compatible products and are suitable for interaction with cells and other macromolecules. In addition, after 15 min of soaking, ACS retain 95% of the rhBMP-2 originally made available [37]. However, ACS showed little structural stability, which can lead to the collapse of soft-tissue walls in the grafted area [34]. One of the disadvantages of using the reported delivery systems evaluated by the clinical trials included in this review was that they did not present controlled BMP-2 release kinetics. Therefore, higher doses of bioactive proteins were needed to obtain therapeutic results. Thus, the development of carriers with greater structural stability and release-controlled system could improve bone induction and ensure the controlled availability of these proteins to local osteoprogenitor cells during new bone formation [17]. To enhance the efficacy of BMP-2, one study [31] evaluated the use of a hyaluronan-based hydrogel, which has been reported to enhance the release of BMP-2, when compared with type I collagen, probably because of the electrostatic interaction between hyaluronan and bioactive molecules [38]. Retention of intact BMP-2 in the grafted area and the appropriate release kinetics may influence the chemotaxis and proliferation of mesenchymal stem cells (MSCs) and subsequent differentiation into osteoblasts, leading to enhanced bone formation [31]. The included study that evaluated rhBMP-2 with hyaluronan-based hydrogel showed that a low BMP-2 concentration of 50 mg/ml hydrogel did not induce bone formation after 6 months, but when this concentration was increased to 250 mg/ml the bone formation increased, and the result was comparable with those of autologous bone grafts [31].
One of the advantages of using bioactive materials in young patients is that they may present high capacity to promote tissue repair and regeneration. The majority of the subjects evaluated in the studies included in this review were in the age-range between 7 and 12 years. At this age, bone graft healing may be highly successful [8], as showed by our review. Older patients may present problems of wound healing, recurrent fistula, and graft exposure [14, 39,40,41]. Furthermore, the risk of graft failure would increase if the patient were a smoker, had poor oral hygiene, or presented a systemic condition such as diabetes [9]. Additionally, the adverse events, such as hematoma, swallowing/breathing difficulties, or dramatic swelling without hematoma in anterior cervical spine fusion, reported with the use of recombinant protein in biological treatments have been questioned [42]. An estimated 10–50% of adverse events have been reported in spine-fusion surgery with rhBMP-2, depending on the approach used [43]. For alveolar and palate cleft defects, only one clinical trial [31] needed to end the study prematurely due to severe gingival swelling during the first week, in patients treated with doses of 250 mg/ml of rhBMP-2. This may be a dose-dependent phenomenon that still needs to be investigated [23, 44]. None of the other studies evaluated such high doses of BMP-2, as they mainly used doses of 3.2–4.2 mg. The studies reported adverse events such as swelling [32,33,34], prolonged wound healing and granulation tissue [35] that were, in general, restricted to few subjects evaluated, and did not impair treatment and further bone formation. Whereas for ICBG, postoperative intraoral infection [7], donor-site pain [32,33,34], partial loss of bone graft, and problematic healing were reported [35].
Two included clinical trials [7, 35] also compared the costs of surgery between the use of rhBMP-2 and ICBG. The mean overall cost of the procedure for alveolar cleft was reported to be higher with ICBG ($21,800) when compared with BMP-2 treatment ($11,100) [35]. One study also analyzed the costs associated with surgery time, and showed that the cost of rhBMP-2 materials ($2600) was balanced by cost savings associated with a reduction in operative time of nearly 1 h and 45 min [7]. A decreased operative time can improve operating room use and limit the patient’s exposure to anesthesia, which are of advantage to both the clinician and patient. Due to these factors, the costs of using both BMP-2 and ICBG were similar [7].
Different methods were used to perform bone formation analysis in the studies, such as only qualitative and quantitative evaluation using radiographs or computed tomography (CT) scans. Although surgeons may use two-dimensional radiographs to evaluate secondary bone grafting for clefts, the exam might sometimes contain inherent distortion factors [23]. The majority of included studies used CT scans [5, 14, 16, 31, 33,34,35] and measured the difference between preoperative and postoperative defect volume, which was defined as bone filling volume, and the percentage ratio between the bone filling volume and the preoperative defect volume was defined as bone filling percentage. Computed tomography (CT) may be a better alternative to provide a more accurate assessment; however, it may present higher cost, increased radiation exposure, patient inconvenience, and lack of accessibility [33]. A limited number of identifiable landmarks and positioning problems could affect the quality of the images, and consequently, the evaluation of bone formation. On the other hand, the use of CT has the advantage of excluding image enlargement and distortion, and also superimposition of adjacent structures [23, 33]. Furthermore, some included studies [14, 33] used Cone Beam CT images. It is important to standardize the evaluation methods for bone formation analysis, and Cone Beam in comparison with conventional fan beam CT is faster, more cost effective, and capable of obtaining images at one-tenth the radiation dose as that of standard CT [33].
The standard procedure for closure of alveolar cleft is the use of autogenous marrow from iliac crest graft; however, this treatment may be followed by notable morbidity and complication. The iliac bone harvesting procedure involves a second surgical step performed in parallel. Consequently, there is the resultant scar in the iliac crest region, longer duration of anesthesia, pain on mobility in the iliac area, loss of blood, risk of infection, and many other potential complications resulting from this clinical procedure [3, 13,14,15,16]. Although the clinical trials available in the literature showed heterogeneity regarding type and doses of bioactive molecules used, the present evidence showed that rhBMP-2 provided similar results to those obtained with ICBG in younger patients. It is important to consider the limitations of the evidence available at present, considering that some included studies presented small sample sizes; no power analysis; variability in time point measurements; and the lack of differences between the use of rhBMP-2 and ICBG could be due to limited power of the studies. However, the largest and most recent study [32] included was a retrospective clinical trial that evaluated 414 subjects, and demonstrated a clinical graft success of 88.4% in the ICBG group and 90% in the rhBMP-2 group. Taking into consideration the complications and high cost associated with ICBG, the use of bioactive proteins in cleft lip and palate patients seemed to be a suitable treatment option for bone repair and regeneration.
References
Pradel W, Tausche E, Gollogly J, Lauer G (2008) Spontaneous tooth eruption after alveolar cleft osteoplasty using tissue-engineered bone: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol 105:440–444. https://doi.org/10.1016/j.tripleo.2007.07.042
Vecchiatini R, Mobilio N, Raimondi F et al (2009) Implant-prosthetic rehabilitation for a patient with monolateral cleft lip and palate: a clinical report. Quintessence Int 40:445–447
Khojasteh A, Behnia H, Naghdi N et al (2013) Effects of different growth factors and carriers on bone regeneration: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol 116:e405–e423. https://doi.org/10.1016/j.oooo.2012.01.044
van Hout WMMT, van der Molen ABM, Breugem CC et al (2011) Reconstruction of the alveolar cleft: can growth factor-aided tissue engineering replace autologous bone grafting? A literature review and systematic review of results obtained with bone morphogenetic protein-2. Clin Oral Invest 15:297–303. https://doi.org/10.1007/s00784-011-0547-6
Canan LW, Da Silva Freitas R, Alonso N et al (2012) Human bone morphogenetic protein-2 use for maxillary reconstruction in cleft lip and palate patients. J Craniofac Surg 23:1627–1633. https://doi.org/10.1097/SCS.0b013e31825c75ba
Gupta C, Mehrotra D, Mohammad S et al (2013) Alveolar bone graft with platelet rich plasma in cleft alveolus. J Oral Biol Craniofac Res 3:3–8. https://doi.org/10.1016/j.jobcr.2013.02.002
Francis CS, Mobin SSN, Lypka MA et al (2013) RhBMP-2 with a demineralized bone matrix scaffold versus autologous iliac crest bone graft for alveolar cleft reconstruction. Plast Reconstr Surg 131:1107–1115. https://doi.org/10.1097/PRS.0b013e3182865dfb
Hibi H, Yamada Y, Ueda M, Endo Y (2006) Alveolar cleft osteoplasty using tissue-engineered osteogenic material. Int J Oral Maxillofac Surg 35:551–555. https://doi.org/10.1016/j.ijom.2005.12.007
Behnia H, Khojasteh A, Soleimani M et al (2012) Repair of alveolar cleft defect with mesenchymal stem cells and platelet derived growth factors: a preliminary report. J Cranio-Maxillofac Surg 40:2–7. https://doi.org/10.1016/j.jcms.2011.02.003
Janssen NG, Weijs WLJ, Koole R et al (2014) Tissue engineering strategies for alveolar cleft reconstruction: a systematic review of the literature. Clin Oral Invest 18:219–226. https://doi.org/10.1007/s00784-013-0947-x
Herford AS, Miller M, Signorino F (2017) Maxillofacial defects and the use of growth factors. Oral Maxillofac Surg Clin North Am 29:75–88. https://doi.org/10.1016/j.coms.2016.08.006
Janssen NG, Weijs WL, Koole R et al (2014) Tissue engineering strategies for alveolar cleft reconstruction: a systematic review of the literature. Clin Oral Invest 18:219–226. https://doi.org/10.1007/s00784-013-0947-x
Laurie SW, Kaban LB, Mulliken JB, Murray JE (1984) Donor-site morbidity after harvesting rib and iliac bone. Plast Reconstr Surg 73:933–938. https://doi.org/10.1097/00006534-198406000-00014
Dickinson BP, Ashley RK, Wasson KL et al (2008) Reduced morbidity and improved healing with bone morphogenic protein-2 in older patients with alveolar cleft defects. Plast Reconstr Surg 121:209–217
Francis CS, Mobin SSN, Lypka M et al (2013) rhBMP-2 with a demineralized bone matrix scaffold versus autologous iliac crest bone graft for alveolar cleft reconstruction. Plast Reconstr Surg 131:1107–1115. https://doi.org/10.1097/PRS.0b013e3182865dfb
Alonso N, Risso GH, Denadai R, Raposo-Amaral CE (2014) Effect of maxillary alveolar reconstruction on nasal symmetry of cleft lip and palate patients: a study comparing iliac crest bone graft and recombinant human bone morphogenetic protein-2. J Plast Reconstr Aesthetic Surg 67:1201–1208. https://doi.org/10.1016/j.bjps.2014.05.014
Marukawa E, Oshina H, Iino G et al (2011) Reduction of bone resorption by the application of platelet-rich plasma (PRP) in bone grafting of the alveolar cleft. J Cranio-Maxillofac Surg 39:278–283. https://doi.org/10.1016/j.jcms.2010.04.017
Sailer HF, Kolb E (1994) Application of purified bone morphogenetic protein (BMP) in cranio-maxillo-facial surgery. BMP in compromised surgical reconstructions using titanium implants. J Cranio-Maxillofac Surg 22:2–11. https://doi.org/10.1016/S1010-5182(05)80289-6
Azari K, Doctor JS, Doll BA, Hollinger JO (2002) Bone morphogenetic proteins. A review for cranial and maxillofacial surgery. Oral Maxillofac Surg Clin North Am 14:1–14. https://doi.org/10.1016/s1042-3699(02)00011-0
Urist MR, Strates BS (1971) Bone morphogenetic protein. J Dent Res 50:1392
Urist MR (1965) Bone: formation by autoinduction. Science 150:1893
Wozney J (1989) Bone morphogenetic proteins. Prog Growth Factor Res 1:267–280
Balaji SM (2009) Use of recombinant human bone morphogenetic protein (rhBMP-2) in reconstruction of maxillary alveolar clefts. J Maxillofac Oral Surg 8:211–217. https://doi.org/10.1007/s12663-009-0052-5
Gomes-Ferreira PHS, Okamoto R, Ferreira S et al (2016) Scientific evidence on the use of recombinant human bone morphogenetic protein-2 (rhBMP-2) in oral and maxillofacial surgery. Oral Maxillofac Surg 20:223–232. https://doi.org/10.1007/s10006-016-0563-4
da Rosa WL de O, da Silva TM, da Silva AF, Piva E (2017) Bioactive treatments in bone grafts for implant-based rehabilitation: systematic review and meta-analysis. Clin Implant Dent Relat Res 1–10. https://doi.org/10.1111/cid.12552
da Rosa WL, Piva E, Silva AF (2018) Disclosing the physiology of dental pulp for vital pulp therapy. Int Endod J. https://doi.org/10.1111/iej.12906
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 62:1006–1012. https://doi.org/10.1016/j.jclinepi.2009.06.005
Higgins JP, Green S (2008) Cochrane handbook for systematic reviews of interventions: cochrane book series. Wiley: Hoboken
da Lima AFM, Rahal SC, dos Volpi RS et al (2007) Effect of bovine bone morphogenetic proteins on radius fracture healing in rabbits. Acta Cir Bras 22:259–264
Clokie CML, Sándor GKB (2008) Reconstruction of 10 major mandibular defects using bioimplants containing BMP-7. J Can Dent Assoc 74:67–72
Neovius E, Lemberger M, Docherty Skogh AC et al (2013) Alveolar bone healing accompanied by severe swelling in cleft children treated with bone morphogenetic protein-2 delivered by hydrogel. J Plast Reconstr Aesthet Surg 66:37–42
Hammoudeh JA, Fahradyan A, Gould DJ et al (2017) A comparative analysis of recombinant human bone morphogenetic protein-2 with a demineralized bone matrix versus iliac crest bone graft for secondary alveolar bone grafts in patients with cleft lip and palate: review of 501 cases. Plast Reconstr Surg 140:318–325. https://doi.org/10.1097/PRS.0000000000003519
Liang F, Yen SLK, Imahiyerobo T et al (2017) Three-dimensional cone beam computed tomography volumetric outcomes of rhBMP-2/demineralized bone matrix versus iliac crest bone graft for alveolar cleft reconstruction. Plast Reconstr Surg 140:767–774. https://doi.org/10.1097/PRS.0000000000003686
Alonso N, Tanikawa DYS, Freitas R da S, et al (2010) Evaluation of maxillary alveolar reconstruction using a resorbable collagen sponge with recombinant human bone morphogenetic protein-2 in cleft lip and palate patients. Tissue Eng C Methods 16:1183–1189. https://doi.org/10.1089/ten.tec.2009.0824
Herford AS, Boyne PJ, Rawson R, Williams RP (2007) Bone morphogenetic protein-induced repair of the premaxillary cleft. J Oral Maxillofac Surg 65:2136–2141. https://doi.org/10.1016/j.joms.2007.06.670
Zhang H, Sucato DJ, Welch RD (2005) Recombinant human bone morphogenic protein-2-enhanced anterior spine fusion without bone encroachment into the spinal canal: a histomorphometric study in a thoracoscopically instrumented porcine model. Spine 30:512–518. https://doi.org/10.1097/01.brs.0000154651.62088.e3
Bessa PC, Casal M, Reis RL (2008) Bone morphogenetic proteins in tissue engineering: the road from laboratory to clinic, part II (BMP delivery). J Tissue Eng Regen Med 2:81–96
Bergman K, Engstrand T, Hilborn J et al (2009) Injectable cell-free template for bone-tissue formation. J Biomed Mater Res A 91:1111–1118. https://doi.org/10.1002/jbm.a.32289
Cohen M, Figueroa AA, Haviv Y et al (1991) Iliac versus cranial bone for secondary grafting of residual alveolar clefts. Plast Reconstr Surg 87:423–427. https://doi.org/10.1097/00006534-199103000-00004
Harsha BC, Turvey TA, Powers SK (1986) Use of autogenous cranial bone grafts in maxillofacial surgery: a preliminary report. J Oral Maxillofac Surg 44:11–15. https://doi.org/10.1016/0278-2391(86)90008-X
Denny AD, Talisman R, Bonawitz SC (1999) Secondary alveolar bone grafting using milled cranial bone graft: a retrospective study of a consecutive series of 100 patients. Cleft Palate Craniofacial J 36:144–153. https://doi.org/10.1597/1545-1569
Shields LBE, Raque GH, Glassman SD et al (2006) Adverse effects associated with high-dose recombinant human bone morphogenetic protein-2 use in anterior. Cervical Spine Fusion 31:542–547
Carragee EJ, Hurwitz EL, Weiner BK (2011) A critical review of recombinant human bone morphogenetic protein-2 trials in spinal surgery: emerging safety concerns and lessons learned. Spine J 11:471–491. https://doi.org/10.1016/j.spinee.2011.04.023
Balaji SM (2009) Mandibular cystic defect: a composite approach with rhBMP-2 and rib graft. J Maxillofac Oral Surg 8:27–30. https://doi.org/10.1007/s12663-009-0007-x
Acknowledgements
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001 and DOCFIX #88887.195037/2018-00. The present research was also supported by the Fundação de Amparo à Pesquisa do Rio Grande do Sul (Pronex FAPERGS #16.0471-4) and by National Council of Technological and Scientific Development (CNPq - grant Technological Development).
Author information
Authors and Affiliations
Contributions
WLOR, TMS, and AFS designed the study. WLOR and TMS prepared the first draft of the paper. WLOR was responsible for statistical analysis of the data. WLOR, ADG, and EP prepared the final draft of the manuscript. All authors revised the paper critically for intellectual content and approved the final version. All authors agree to be accountable for the work and to ensure that any questions relating to the accuracy and integrity of the paper are investigated and properly resolved.
Corresponding author
Ethics declarations
Conflict of interest
Wellington Luiz de Oliveira da Rosa, Tiago Machado da Silva, Arthur Dias Galarça, Evandro Piva, and Adriana Fernandes da Silva have no conflicts of interest related to this work.
Research Involving Human and Animal Participants
There were no human or animal studies conducted by the authors who were described in this review.
Informed consent
The study is with secondary data from other papers. Informed consent was obtained from all individual participants in each included study for whom identifying information is included in this article.
Rights and permissions
About this article

Cite this article
da Rosa, W.L.d.O., da Silva, T.M., Galarça, A.D. et al. Efficacy of rhBMP-2 in Cleft Lip and Palate Defects: Systematic Review and Meta-analysis. Calcif Tissue Int 104, 115–129 (2019). https://doi.org/10.1007/s00223-018-0486-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-018-0486-1