
Abstract
Age- and sex-related alterations in the control of multiple muscles during contractions are not well understood. The purpose of the present study was to examine the age and sex differences in force steadiness and intermuscular coherence (IMC), and thereby to clarify the functional role of IMC during plantar flexion. Twenty-six young (YNG, 23–34 years), thirty middle-aged (MID, 35–64 years) and twenty-four older adults (OLD, 65–82 years) performed submaximal isometric contractions of plantar flexion, while electromyography was recorded from the soleus (SOL), gastrocnemius lateralis/medialis (GL/GM) and tibialis anterior (TA) muscles. Coefficient of variation (CV) of torque and IMC in the alpha, beta and gamma bands was calculated. We found that OLD demonstrated significantly higher torque CV than YNG and MID, and males demonstrated significantly higher torque CV than females (both p < 0.05). The IMC in the gamma band (five out of the six pairs) was significantly higher in YNG than MID and/or OLD (p < 0.05), while the gamma band IMC between GL and SOL was significantly higher in females. However, age or sex differences were not detected in the alpha or beta band. Moreover, the gamma band IMC between SOL and TA had a weak (r = − 0.229) but significant (p < 0.05) negative correlation with torque CV. These results suggest that force steadiness differs with age and sex, and that the higher gamma band IMC may contribute to more stable force control during plantar flexion.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Maintaining healthy skeletal muscles is critical for functional activities of daily living. It is well recognized that skeletal muscle mass and strength change dramatically as we get older (Goodpaster et al. 2006; Mitchell et al. 2012). Also, aging has been shown to influence the ability of an individual to sustain a target force level stably (Galganski et al. 1993). This ability is termed “force steadiness” and can be quantified as the coefficient of variation (CV) of muscle force or joint torque during submaximal isometric contraction. Many previous studies have confirmed that force steadiness declines with age, in various muscle groups under low- and high-intensity contractions (Oomen and van Dieën 2017). The decline in force steadiness aggravates postural stability in older adults (Kouzaki and Shinohara 2010; Hirono et al. 2020). In fact, older adults who had a history of falling have shown less steady contractions in the quadriceps femoris muscles than those without a falls history (Carville et al. 2007).
Along with age, sex is also an important determinant of force steadiness. Although there are few studies focusing on sex difference in force steadiness, some previous studies have found that males are steadier than females (Brown et al. 2010; Vanden Noven et al. 2014).
However, the understanding of the age and sex differences in force steadiness is limited. For example, as most previous studies have only compared force steadiness of young (typically less than 30 years old) and older (aged 65 years or older) adults, it is not clear at what age the change in force steadiness begins. In addition, it remains unknown whether the age-related change in force steadiness differs between males and females.
According to previous research, a potential neurophysiological determinant of force steadiness is the variability in common synaptic input from the motor cortex to motor neurons (Feeney et al. 2018). In fact, CV of force during isometric contraction was strongly correlated with the variance in the common modulation of the motor unit discharge rate in the abductor digiti minimi and the tibialis anterior because these muscles produce a large fraction of net joint torque (Negro et al. 2009; Castronovo et al. 2018). However, the association of force steadiness with the variability in common synaptic input is expected to be different when multiple muscles are coordinated in joint torque production. For example, ankle plantar flexion is a movement that involves multiple muscles, including antagonist muscles such as the tibialis anterior (Kouzaki and Shinohara 2010). Each of these muscles receives a relatively low proportion of shared synaptic input (Hug et al. 2021), resulting in weak correlations between the steadiness of ankle joint torque and common modulation of motor unit discharge rate in each muscle (Davis et al. 2020). It is therefore speculated that not only the common synaptic input into each muscle but the coordinated activities of lower leg muscles are important to stabilize the ankle joint torque.
One potential method to assess the coordination of multiple muscles is coherence analysis. Coherence represents the magnitude of association between two biological signals in a frequency domain (Halliday et al. 1995). There are two types of typical coherence associated with skeletal muscle. One is cortico-muscular coherence (CMC), which is the coherence between electroencephalography (EEG) or magnetoencephalography in the cortical motor cortex and electromyography (EMG) in the muscles. The other one is the intermuscular coherence (IMC), which shows the correlation between two EMG signals. While CMC represents a functional association between the motor cortex and a single skeletal muscle (Liu et al. 2019), IMC has been considered to represent a common synaptic input to a motor neuron pool in multiple skeletal muscles (Dideriksen et al. 2018). In fact, previous studies have demonstrated that IMC represents the shared neural drive and the pattern of coordination between muscles (Laine and Valero-Cuevas 2017; Watanabe et al. 2018). Therefore, IMC of lower leg muscles will provide valuable insights into force steadiness of the plantar flexion.
While IMC analysis is a promising means to elucidate neural mechanisms of force steadiness, it is unclear whether age and sex may influence IMC because of inconsistent findings and limited investigations. For example, some studies found that IMC decreased with age (Walker et al. 2019), while others reported that IMC remained unchanged (Jaiser et al. 2016). Moreover, sex difference in IMC and its relation to age have yet to be explored. Investigating the influence of age and sex on IMC is critical to understanding the role of these factors in force steadiness.
The purpose of the present study was to examine the age and sex differences in force steadiness and IMC during plantar flexion torque-matching tasks, and further to determine if there is an association between force steadiness and IMC. For this purpose, we recorded EMGs of the soleus (SOL), gastrocnemius medialis (GM), gastrocnemius lateralis (GL) and tibialis anterior (TA) muscles to calculate IMC between them. We did not examine the activities of deep plantar flexors, considering the spectral properties are substantially different between surface and fine-wire EMGs. Nevertheless, the activation of deep plantar flexors varies between individuals, but the mechanical contribution to plantar flexion torque can be assumed to be small compared to that of the triceps surae muscles (Finni et al. 2006).
Methods
Participants
Eighty adults (36 males and 44 females, determined by self-report) participated in this study. Inclusion criteria were apparently healthy males and females aged 20 years or older and able to carry out the activities of daily living independently. Exclusion criteria were a self-reported history of heart attack, stroke, uncontrolled hypertension (systolic blood pressure of more than 200 mmHg and/or diastolic blood pressure of more than 110 mmHg), complicated type 2 diabetes, acute or chronic liver disease, limited range of motion in the lower extremities due to musculoskeletal pain, and/or osteoporosis with compression fractures. Prior to the measurement, all participants signed a written, informed consent. This study was approved by the Ethics Committee for Human Experiments, the University of Tokyo.
Participants were divided into the following three groups, according to their age: YNG (age range: 23–34 years, n = 26), MID (age range: 35–64 years, n = 30) and OLD (age range: 65–82 years, n = 24). The age stratification was performed so that each age group contained 20 or more participants, on the basis of previous studies on the age differences in force steadiness (Kouzaki and Shinohara 2010; Davis et al. 2020) and intermuscular coherence (Jaiser et al. 2016; Walker et al. 2019). Participants’ characteristics are shown in Table 1.
Experimental protocol
Participants were seated on a chair, with their right knee extended and their ankle firmly strapped on a custom-designed ankle dynamometer at 90° (Fig. 1A). After a warm-up session, participants performed two trials of maximum voluntary isometric contraction (MVC) of plantar flexors for 6 s. If the difference in the averaged torque, calculated over 3 s in the middle of contraction, between the two trials, was > 5%, another trial was performed. The highest torque in the two or three trials was defined as MVC.

Experimental setup (A) and placement of electrodes for surface electromyography (B). SOL soleus, GM gastrocnemius medialis, GL gastrocnemius lateralis, TA tibialis anterior
Participants then performed a submaximal isometric plantar flexion at a constant torque level. The contraction intensity was targeted at 10–90% of MVC in 10% increments, where participants performed one trial for each intensity. The contraction intensities were set widely because the large difference in the absolute joint torque (i.e., expressed in N m) across participants with different age and sex may influence force steadiness and muscle activities. To avoid the effect of preceding high-intensity contractions, which can cause a post-activation potentiation or fatigue, on the following low-intensity contraction tasks, the torque level was arranged in an ascending order (Sasaki et al. 2012).
The target torque level and participants’ real-time torque production were displayed as a horizontal line on an oscilloscope screen. Participants tried to match the two lines as closely as possible for 6 s, which was considered close to the maximum time to correctly perform the task at high intensities. A rest of at least 1 min was given between each contraction.
Recordings
The plantar flexion torque was measured by a load cell (LMB-A, Kyowa electronic instruments, Japan) firmly attached to the edge of a rotor of the dynamometer. The output signal from the load cell was calibrated by applying a constant torque to the rotor using a self-made lever-weight system. The signal was amplified with a strain amplifier (6M84, NEC San-ei, Japan) and sampled at 4000 Hz by an A/D converter (PowerLab/16SP, ADInstruments, New Zealand).
Surface electromyography (EMG) was recorded during the isometric contraction task using bipolar Ag/AgCl electrodes (F-150 M, Nihon Kohden, Japan) with an inter-electrode distance of 25 mm. Participants’ skin was shaved and cleaned with alcohol before placing electrodes. The electrodes were positioned on SOL, GM, GL and TA of the right leg (Fig. 1B). With regard to the electrode location, we followed the SENIAM recommendations (Hermens et al. 2000) except for SOL, in which the electrodes were placed on the lateral part as opposed to the medial part recommended by SENIAM. This is because the SOL electrodes placed medially tend to suffer from cross-talk (Bogey et al. 2000). EMG signals were amplified (gain 500–1000; 5–1000 Hz) with an amplifier (AB-610 J, Nihon Kohden) and sampled concurrently with the torque signal.
Data analysis
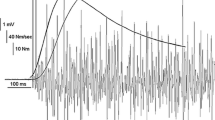
Force steadiness was analyzed for 5.120 s (the window length suitable for the calculation of IMC) in the middle of isometric contraction (Fig. 2). If the plateau phase of ankle joint torque in the middle of contraction was shorter than 5.120 s, the data were reduced to a 4.608 s or 4.096 s. Before the analysis, the recorded torque signals were digitally low-pass filtered (cut-off 50 Hz) and de-trended by fitting a 2nd-order polynomial to the torque–time curve (Spencer et al. 2020). CV of the joint torque, which is a reciprocal measure of force steadiness (i.e., higher CV represents lower steadiness), was calculated using the following equation:

Raw torque and full-wave rectified EMG traces during a submaximal isometric voluntary contraction (at 50% MVC). The signals between the two dashed lines were used for the calculation of the coefficient of variation of the torque and intermuscular coherence. SOL: soleus, GM: gastrocnemius medialis, GL: gastrocnemius lateralis, TA: tibialis anterior
IMC between two EMG signals was calculated for the same time period as used for the calculation of torque CV. EMG signals were de-trended and full-wave rectified prior to analyses because full-wave rectification of EMG is known to provide the temporal pattern of grouped firing of motor units (Halliday et al. 1995).
IMC was calculated using 2048-point (512-ms) fast Fourier transforms with 50% overlap, which gave the frequency resolution of 1.95 Hz. Coherence of two EMG signals was defined as the absolute square of cross-spectrum normalized by the two auto-spectra (Grosse et al. 2002):
where \({f}_{\mathrm{1,1}}\) and \({f}_{\mathrm{2,2}}\) denote the auto-spectrum of each signal, and \({f}_{\mathrm{1,2}}\) denotes the cross-spectrum. Coherence ranges from 0 to 1, where higher value indicates that the two signals are highly correlated. IMC was calculated between all six pairs of four muscles (SOL, GM, GL and TA).
Statistical analysis
A three-way analysis of variance (ANOVA) was used to test main effects and interactions of age (between-participants factor), sex (between-participants factor) and contraction intensity (within-participants factor) on torque CV. An unequal variance t test and a paired t test were used as post hoc multiple comparison tests for the main effects of age and contraction intensity, respectively. If the interaction between age and sex was significant, the unequal variance t test was performed to determine the age differences in the same sex and the sex difference within the same age categories. The significance level for the multiple comparisons was adjusted according to the false discovery rate procedure. This procedure is a method of controlling the false discovery rate (the expected fraction of null hypotheses rejected mistakenly) instead of the familywise error rate (for details, see Curran-Everett 2000).
Coherence is considered to be significant if it exceeds a confidence limit S (Rosenberg et al. 1989):
where \(\alpha =0.05\) and \(L\) denotes the number of sections used for the calculation of coherence. The confidence limit was adjusted to account for overlaps of the segments (Gallet and Julien 2011). The percentage of IMC that exceeded the confidence limit was calculated for each frequency and compared among six groups with different age and sex combinations.
Prior to statistical analysis of IMC, z-transformation was applied to the raw coherence values (Semmler et al. 2004). IMC z scores were then averaged in the alpha band (5–15 Hz), beta band (15–30 Hz) and gamma band (30–60 Hz). A range of frequency in each band was determined based on the neural origins suggested in previous studies (Grosse et al. 2002; Weersink et al. 2021) and the percentage of significant coherence (see below) observed (Hansen et al. 2002). Recent studies have indicated that alpha band IMC has subcortical origins including the reticulospinal pathway (Grosse and Brown 2003; Weersink et al. 2021), while both beta and gamma band IMCs originate from motor cortex oscillations (Grosse et al. 2002; Kenville et al. 2020). In each band, a three-way ANOVA and post hoc multiple comparison tests (the same procedure as used for the analysis of torque CV) were used to test the effect of age, sex and contraction intensity on IMC.
To test the association between force steadiness and the magnitude of muscle coordination, both torque CV and IMC z score were averaged across nine contraction intensities and analyzed with correlation analysis. In all statistical analyses, p < 0.05 was considered significant.
Results
Force steadiness
The three-way ANOVA on torque CV revealed a significant main effect of contraction intensity (F(8,592) = 6.73, p < 0.001), a significant main effect of age (F(2,74) = 11.67, p < 0.001) and a significant main effect of sex (F(1,74) = 8.68, p = 0.004). No interaction was found among these factors. Torque CV was the highest at 10% MVC, gradually decreased as the contraction intensity increased, and remained almost constant from 40 to 90% MVC (Fig. 3A). Although the difference was small, torque CVs at 10 and 20% MVC were significantly higher than those at 40–90% MVC except 80% MVC. As no interaction was detected between age, sex and contraction intensity, the individual average of torque CV over nine contraction intensities was calculated for further analysis to examine the age and sex differences. The averaged torque CV was significantly higher (p = 0.015) in MID (1.88 ± 0.32%) than in YNG (1.67 ± 0.30%), and significantly higher (p = 0.013) in OLD (2.25 ± 0.64%) than in MID (Fig. 3B). Males (2.09 ± 0.56%) demonstrated significantly higher (p = 0.007) torque CV than females (1.78 ± 0.38%, Fig. 3C).

Changes in coefficient of variation (CV) of torque with contraction intensity (A), age (B), and sex (C). Torque CV was averaged for all participants at each contraction intensity (A). Torque CV was averaged over nine contraction intensities and compared between age groups (B) and sexes (C). Data are mean and standard deviation. YNG young adults, MID middle-aged adults, OLD older adults. (a) p < 0.05 vs. 10%MVC, (b) p < 0.05 vs. 20%MVC, * p < 0.05 between groups
Intermuscular coherence
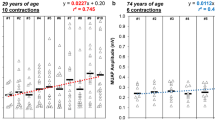
The percentage of IMC above the confidence limit was calculated for the three age groups of males (Fig. 4A) and females (Fig. 4B). A relatively high percentage of significant IMC was observed around 10 Hz and 35 Hz compared to other frequencies, regardless of age, sex, and the pair of EMGs analyzed. The effects of age, sex and contraction intensity on IMC were determined in each frequency band using the three-way ANOVA, the results of which are summarized in Table 2.

Percentages of intermuscular coherence (IMC) exceeding the confidence limit in three age groups of males (A) and females (B). IMC was calculated at each frequency and analyzed separately in the alpha (5–15 Hz), beta (15–30 Hz) and gamma (30–60 Hz) bands. The percentage was calculated in each group using all IMC data, with six pairs of EMGs and nine contraction intensities
Alpha band
The interactions between contraction intensity and age/sex were not significant in any muscle pair. The main effect of intensity was significant only in GL–TA pair. The interaction between age and sex was significant in GM–GL pair, whereas the main effect of age was significant in GL–TA pair. However, a post hoc multiple comparison test failed to detect a significant difference between the groups. No main effect of sex was found in any muscle pair.
Beta band
The three-way interaction of age, sex and contraction intensity was only significant in SOL–GM pair. However, no significant interaction between contraction intensity and age/sex was found in any muscle pair. The main effect of intensity was significant in SOL–GL, GM–GL and GL–TA pairs. The interaction of age and sex was significant in SOL–GL, SOL–TA and GM–GL pairs, but a post hoc multiple comparison test failed to detect a significant difference between the groups. No main effect of age or sex was found in any muscle pair.
Gamma band
The interaction between contraction intensity and sex was significant in GM–TA pair, but no significant interaction between contraction intensity and age/sex was found in any other muscle pair. The main effect of intensity was significant in all muscle pairs. Post hoc multiple comparison tests revealed that the gamma band IMC (averaged for all muscle pairs) was almost constant from 10 to 60% MVC, but slightly increased as the contraction intensity increased further where the gamma band IMC of 70 to 90% MVC was significantly higher than that of 10 to 60% MVC (Fig. 5A). The significant interaction between age and sex was found in SOL–TA pair, where young females showed higher IMC than did middle-aged and older females (both p < 0.001). The significant main effect of age was detected in all the six pairs, where YNG demonstrated significantly higher IMC than did MID and/or OLD except for SOL–GM pair (p < 0.05, Fig. 5B). The significant main effect of sex was demonstrated only in SOL–GL pair, where females demonstrated significantly higher IMC than males.

Differences in intermuscular coherence (IMC) z scores in the gamma band across nine submaximal contraction intensities (A) and three age groups (B). The IMC z score was averaged over six pairs of EMGs in each participant and compared between nine contraction intensities (A). The IMC z score was averaged over nine contraction intensities in each participant and compared among the three age groups in each pair of EMGs (B). Data are mean and standard deviation. YNG young adults, MID middle-aged adults, OLD older adults, SOL soleus, GM gastrocnemius medialis, GL gastrocnemius lateralis, TA tibialis anterior. a p < 0.05 vs. 70% MVC, b vs. 80% MVC, and c vs. 90% MVC. * p < 0.05 between age groups
As described above, the significant age and sex differences in IMC were detected only in the gamma band, except that the main effect of age was significant in the alpha band IMC of GL–TA pair. Thus, we examined associations of the gamma band IMC z scores with torque CV. We found that the gamma band IMC of SOL–TA pair was significantly correlated with torque CV (r = − 0.229, p = 0.041, Fig. 6) and that of GL–TA pair tended to be correlated with CV (r = − 0.210, p = 0.062). No such correlation was found in the alpha or beta band IMC.

Correlation between coefficient of variation (CV) of torque and gamma band (30–60 Hz) intermuscular coherence (IMC) z score of soleus (SOL) and tibialis anterior (TA) muscles (r = − 0.229, p = 0.041). Note that the CV and the gamma band IMC shown were averaged over nine contraction intensities in each participant
Discussion
The purpose of the present study was to examine the age and sex differences in force steadiness (represented by CV of ankle joint torque) and IMC during isometric plantar flexions with various contraction intensities. We found that older participants showed significantly higher torque CV than did the other groups, while young adults showed significantly higher gamma band IMC. As to the sex difference, males showed significantly higher torque CV but lower gamma band IMC than females. There was a weak but significant negative correlation between the torque CV and the gamma band IMC of SOL–TA pair.
Force steadiness
In the present study, the age difference in force steadiness was studied by comparing CV of plantar flexion torque across three age groups. We categorized the individuals aged 35–64 years as a single age group (MID) so that the number of participants was comparable to those of young (YNG) and old (OLD) counterparts, ensuring statistical power to detect a significant age difference. The torque CV was significantly higher in OLD than YNG, which agrees well with previous studies (e.g.,Tracy 2007; Kouzaki and Shinohara 2010). MID had a torque CV significantly higher than YNG but significantly lower than OLD. To our knowledge, this is the first study to detect the difference in force steadiness between young (28.0 ± 4.2 years) and middle-aged adults (53.5 ± 8.4 years). These findings suggest that the age-related decline in the ability to control plantar flexion torque does not start at the later life, but rather at the middle age.
Compared to the age difference, there have been limited attempts to investigate the sex difference in force steadiness. To our knowledge, no study has so far examined the sex difference in force steadiness of isometric plantar flexion. Contrary to earlier observations on other joint movements, we found that the fluctuations of ankle joint torque during submaximal plantar flexion were significantly larger in males than in females. Moreover, there was no significant interaction between age and sex, suggesting that the decline in force steadiness with age is similar between males and females.
The difference in absolute muscle strength is likely to be a factor for sex difference in force steadiness. In fact, there was a significant negative correlation between elbow flexors MVC and the magnitude of torque CV (Brown et al. 2010). We found, however, that females showed weaker strength but greater force steadiness than males and that torque CV was not significantly correlated with MVC or MVC per body weight. These results imply no direct link between the sex differences in absolute strength and force steadiness. Likewise, other proposed mechanisms underlying the sex difference (e.g., the difference in muscle fiber and motor unit types) are suitable for greater steadiness in males but not in females. Thus, we cannot provide a clear explanation of why females were steadier than males, although the sex difference in IMC may play a role, as discussed later.
A recent meta-analysis suggests that the magnitude of sex difference in force steadiness differs among muscles (Jakobi et al. 2018). Generally, force steadiness is greater in males than in females, but the difference tends to be small in the lower limb (e.g., knee extensors and dorsiflexors) compared to upper limb (e.g., elbow flexors and wrist extensors) muscles. Moreover, a previous study on knee extensors (Clark et al. 2005) demonstrated that males showed significantly higher torque CV than females. Therefore, our results may provide a support for the idea that the sex difference in force steadiness is dependent on the muscles, although further study is needed to elucidate the physiological mechanisms of this muscle specificity.
In relation to the contraction intensity, torque CV was the highest at 10% MVC and decreased with increasing contraction intensity, resulting in a nearly constant value at more than 40% MVC. These results are in good agreement with those previously reported (Taylor et al. 2003; Moritz et al. 2005). Despite the intensity dependence of torque CV, we combined the data from different contraction intensities to test the age and sex differences. This was not only because the influence of contraction intensity on torque CV was small, but also because no influence of contraction intensity was observed on the age or sex difference in force steadiness.
Intermuscular coherence
Since IMC reflects shared neural input from the motor neuron pool into each muscle, it might have some associations with the steadiness of joint torque production where multiple muscles are involved. In the present study, we investigated the age and sex differences in IMC of lower leg muscles in three major frequency bands. As a result, IMC exceeded the significance level at a relatively high rate in the alpha and gamma bands compared to the beta band. The main effect of age was significant in the gamma band IMC of all the muscle pairs studied, where YNG showed higher values than MID and/or OLD except for SOL–GM pair. In contrast, such an age difference was not found in the alpha or beta band, with the exception of the significant main effect of age in the alpha band IMC of GL–TA pair. Although the neural origin of IMC in each band is not completely understood, recent studies have indicated that alpha band IMC has subcortical origins, while both beta and gamma band IMCs originate from motor cortex oscillations (Grosse et al. 2002; Kenville et al. 2020). Considering that the gamma band IMC was significantly different with age, but the alpha band IMC was not, the cortico-muscular connection may change more severely with aging than the subcortical afferent function.
With regard to the sex difference, the gamma band IMC between SOL and GL was significantly higher in females than in males, but no such difference was observed in the alpha or beta band. Because there have been very few studies examining the sex difference in IMC, we could not specify why females showed higher IMC only in the gamma band. Nevertheless, this result suggests that the cortical control of plantar flexion is more enhanced in females than in males. In fact, a previous study (Lissek et al. 2007) found that females showed significantly higher activation in the cortical area than males during motor tasks.
These age and sex differences are generally consistent with those in force steadiness. We found that YNG and females showed lower torque CV but higher gamma band IMC than did OLD and males, respectively. These relationships raise the possibility that the gamma band IMC is associated with the ability of an individual to coordinate multiple muscles around a joint and to stably control the net joint torque. In fact, the contribution of beta and gamma oscillations to force control has been reported recently in both simulation (Watanabe and Kohn 2015) and experimental models (Castronovo et al. 2018). In the present study, we found a weak but significant negative correlation between CV of plantar flexion torque and the gamma band IMC of SOL–TA pair and a similar trend was detected in the gamma band IMC of GL–TA pair. As both SOL–TA and GL–TA pairs are agonist–antagonist muscle relationships, the loss of cooperative activities between agonist and antagonist muscles may be responsible for the decline in force steadiness. These findings are in agreement with the fact that co-contractions of TA and gastrocnemius muscles stabilize the ankle joint during standing (Vette et al. 2017).
Taken together, the decline in the gamma band IMC observed in OLD suggests the age-related deterioration in the cortical ability to control multiple muscles. As the gamma band IMC was significantly different between YNG and MID for five of the six muscle pairs, the degradation in the coordinated activities of synergistic and antagonistic muscles may start around middle age. Furthermore, the present study provides a support for the notion that the sex difference in the cortical control of multiple muscles, reflected by the gamma band IMC, is one of the determinants of the sex difference in force steadiness.
Limitations and future directions
There are several limitations to be mentioned. First, the time period (typically 5.120 s) used for calculating force steadiness and IMC was relatively short compared with those in previous studies. We chose this duration for the direct comparison of force steadiness and IMC among different contraction intensities (up to near maximal effort) while minimizing the fatigue. As a result, the magnitude of torque CV in this study (approximately 2%) is in good agreement with the findings in previous studies examining 5- to 40-s isometric contractions (Tracy 2007; Kouzaki and Shinohara 2010; Kallio et al. 2012). For IMC analysis, such a short duration would lead to a relatively high confidence limit, with which the percentage of significant coherence will decrease. Nevertheless, we could find significant coherence in a wide range of frequencies, the percentage of which is comparable with those reported in previous studies (Walker et al. 2020).
Second, IMC between adjacent muscles has the potential risk of cross-talk, which cannot be eliminated completely with available methods (Farina et al. 2014). The EMG-EMG cross-talk can result in high levels of coherence across a wide range of frequencies (Farmer et al. 2007). However, we did not find such unnaturally high IMC even in older adults who tended to have a thinner leg (due to muscle atrophy) and have a higher potential risk of cross-talk. It is thus reasonable to assume that the influence of cross-talk was minimal in this study.
Third, our results suggest that the force steadiness and the gamma band IMC decrease in middle-aged compared to young individuals, but the age range of MID was relatively wide (35–64 years) with its mean (53.5 years) trending toward the older range. Future research should use a narrower age range to identify a more specific estimate for the age at which these changes occur.
Finally, although we detected negative correlations between the gamma band IMC and the torque CV, it remains uncertain how the gamma band IMC is related to force steadiness. As surface EMG is just a summation of motor unit action potentials within the recording volume of the electrode, it is difficult to analyze the activity of individual motor units and its relation to the common neural drive. To overcome this limitation, some studies have used high-density multichannel surface EMG, which is a powerful tool for determining motor unit discharge timings (e.g., Hug et al. 2021). In the present study, coordinated activities of agonist and antagonist muscles were related to the steadiness of ankle joint torque. Further studies combining IMC analysis including antagonist muscles and the coherence analysis of motor unit spike trains within each muscle might improve our understanding in the neurophysiological determinants of force steadiness.
Conclusion
We aimed to investigate the age and sex differences in force steadiness of plantar flexion and intermuscular coherence of lower leg muscles. Consequently, older adults and males showed significantly larger torque fluctuations and lower IMC in the gamma band, compared to young adults and females, respectively. We found a significant negative correlation between torque fluctuations and the gamma band IMC of an agonist–antagonist muscle pair. Therefore, we conclude that force steadiness differs with both age and sex, which is partly explained by the difference in the gamma band IMC, a measure of muscle coordination achieved by the motor cortex.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
Bogey RA, Perry J, Bontrager EL, Gronley JK (2000) Comparison of across-subject EMG profiles using surface and multiple indwelling wire electrodes during gait. J Electromyogr Kinesiol 10:255–259. https://doi.org/10.1016/S1050-6411(00)00015-8
Brown RE, Edwards DL, Jakobi JM (2010) Sex differences in force steadiness in three positions of the forearm. Eur J Appl Physiol 110:1251–1257. https://doi.org/10.1007/s00421-010-1600-x
Carville SF, Perry MC, Rutherford OM, Smith IC, Newham DJ (2007) Steadiness of quadriceps contractions in young and older adults with and without a history of falling. Eur J Appl Physiol 100:527–533. https://doi.org/10.1007/s00421-006-0245-2
Castronovo AM, Mrachacz-Kersting N, Stevenson AJT, Holobar A, Enoka RM, Farina D (2018) Decrease in force steadiness with aging is associated with increased power of the common but not independent input to motor neurons. J Neurophysiol 120:1616–1624. https://doi.org/10.1152/jn.00093.2018
Clark BC, Collier SR, Manini TM, Ploutz-Snyder LL (2005) Sex differences in muscle fatigability and activation patterns of the human quadriceps femoris. Eur J Appl Physiol 94:196–206. https://doi.org/10.1007/s00421-004-1293-0
Curran-Everett D (2000) Multiple comparisons: philosophies and illustrations. Am J Physiol Regul Integr Comp Physiol 279:R1–R8. https://doi.org/10.1152/ajpregu.2000.279.1.R1
Davis LA, Alenazy MS, Almuklass AM, Feeney DF, Vieira T, Botter A, Enoka RM (2020) Force control during submaximal isometric contractions is associated with walking performance in persons with multiple sclerosis. J Neurophysiol 123:2191–2200. https://doi.org/10.1152/jn.00085.2020
Dideriksen JL, Negro F, Falla D, Kristensen SR, Mrachacz-Kersting N, Farina D (2018) Coherence of the surface EMG and common synaptic input to motor neurons. Front Hum Neurosci 12:207. https://doi.org/10.3389/fnhum.2018.00207
Farina D, Merletti R, Enoka RM (2014) The extraction of neural strategies from the surface EMG: an update. J Appl Physiol 117:1215–1230. https://doi.org/10.1152/japplphysiol.00162.2014
Farmer SF, Gibbs J, Halliday DM, Harrison LM, James LM, Mayston MJ, Stephens JA (2007) Changes in EMG coherence between long and short thumb abductor muscles during human development. J Physiol 579:389–402. https://doi.org/10.1113/jphysiol.2006.123174
Feeney DF, Mani D, Enoka RM (2018) Variability in common synaptic input to motor neurons modulates both force steadiness and pegboard time in young and older adults. J Physiol 596:3793–3806. https://doi.org/10.1113/jp275658
Finni T, Hodgson JA, Lai AM, Edgerton VR, Sinha S (2006) Muscle synergism during isometric plantarflexion in achilles tendon rupture patients and in normal subjects revealed by velocity-encoded cine phase-contrast MRI. Clin Biomech 21:67–74. https://doi.org/10.1016/j.clinbiomech.2005.08.007
Galganski ME, Fuglevand AJ, Enoka RM (1993) Reduced control of motor output in a human hand muscle of elderly subjects during submaximal contractions. J Neurophysiol 69:2108–2115. https://doi.org/10.1152/jn.1993.69.6.2108
Gallet C, Julien C (2011) The significance threshold for coherence when using the Welch’s periodogram method: Effect of overlapping segments. Biomed Signal Process Control 6:405–409. https://doi.org/10.1016/j.bspc.2010.11.004
Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, Simonsick EM, Tylavsky FA, Visser M, Newman AB (2006) The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci 61:1059–1064. https://doi.org/10.1093/gerona/61.10.1059
Grosse P, Brown P (2003) Acoustic startle evokes bilaterally synchronous oscillatory EMG activity in the healthy human. J Neurophysiol 90:1654–1661. https://doi.org/10.1152/jn.00125.2003
Grosse P, Cassidy MJ, Brown P (2002) EEG-EMG, MEG-EMG and EMG-EMG frequency analysis: physiological principles and clinical applications. Clin Neurophysiol 113:1523–1531. https://doi.org/10.1016/s1388-2457(02)00223-7
Halliday DM, Rosenberg JR, Amjad AM, Breeze P, Conway BA, Farmer SF (1995) A framework for the analysis of mixed time series/point process data–theory and application to the study of physiological tremor, single motor unit discharges and electromyograms. Prog Biophys Mol Biol 64:237–278. https://doi.org/10.1016/s0079-6107(96)00009-0
Hansen S, Hansen NL, Christensen LOD, Petersen NT, Nielsen JB (2002) Coupling of antagonistic ankle muscles during co-contraction in humans. Exp Brain Res 146:282–292. https://doi.org/10.1007/s00221-002-1152-3
Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G (2000) Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 10:361–374. https://doi.org/10.1016/s1050-6411(00)00027-4
Hirono T, Ikezoe T, Taniguchi M, Yamagata M, Miyakoshi K, Umehara J, Ichihashi N (2020) Relationship between ankle plantar flexor force steadiness and postural stability on stable and unstable platforms. Eur J Appl Physiol 120:1075–1082. https://doi.org/10.1007/s00421-020-04346-0
Hug F, Del Vecchio A, Avrillon S, Farina D, Tucker K (2021) Muscles from the same muscle group do not necessarily share common drive: evidence from the human triceps surae. J Appl Physiol 130:342–354. https://doi.org/10.1152/japplphysiol.00635.2020
Jaiser SR, Baker MR, Baker SN (2016) Intermuscular coherence in normal adults: variability and changes with age. PLoS ONE 11:e0149029. https://doi.org/10.1371/journal.pone.0149029
Jakobi JM, Haynes EMK, Smart RR (2018) Is there sufficient evidence to explain the cause of sexually dimorphic behaviour in force steadiness? Appl Physiol Nutr Metab 43:1207–1214. https://doi.org/10.1139/apnm-2018-0196
Kallio J, Søgaard K, Avela J, Komi P, Selänne H, Linnamo V (2012) Age-related decreases in motor unit discharge rate and force control during isometric plantar flexion. J Electromyogr Kinesiol 22:983–989. https://doi.org/10.1016/j.jelekin.2012.05.009
Kenville R, Maudrich T, Vidaurre C, Maudrich D, Villringer A, Ragert P, Nikulin VV (2020) Intermuscular coherence between homologous muscles during dynamic and static movement periods of bipedal squatting. J Neurophysiol 124:1045–1055. https://doi.org/10.1152/jn.00231.2020
Kouzaki M, Shinohara M (2010) Steadiness in plantar flexor muscles and its relation to postural sway in young and elderly adults. Muscle Nerve 42:78–87. https://doi.org/10.1002/mus.21599
Laine CM, Valero-Cuevas FJ (2017) Intermuscular coherence reflects functional coordination. J Neurophysiol 118:1775–1783. https://doi.org/10.1152/jn.00204.2017
Lissek S, Hausmann M, Knossalla F, Peters S, Nicolas V, Güntürkün O, Tegenthoff M (2007) Sex differences in cortical and subcortical recruitment during simple and complex motor control: an fMRI study. Neuroimage 37:912–926. https://doi.org/10.1016/j.neuroimage.2007.05.037
Liu J, Sheng Y, Liu H (2019) Corticomuscular coherence and its applications: a review. Front Hum Neurosci 13:100. https://doi.org/10.3389/fnhum.2019.00100
Mitchell WK, Williams J, Atherton P, Larvin M, Lund J, Narici M (2012) Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front Physiol 3:260. https://doi.org/10.3389/fphys.2012.00260
Moritz CT, Barry BK, Pascoe MA, Enoka RM (2005) Discharge rate variability influences the variation in force fluctuations across the working range of a hand muscle. J Neurophysiol 93:2449–2459. https://doi.org/10.1152/jn.01122.2004
Negro F, Holobar A, Farina D (2009) Fluctuations in isometric muscle force can be described by one linear projection of low-frequency components of motor unit discharge rates. J Physiol 587:5925–5938. https://doi.org/10.1113/jphysiol.2009.178509
Oomen NM, van Dieën JH (2017) Effects of age on force steadiness: a literature review and meta-analysis. Ageing Res Rev 35:312–321. https://doi.org/10.1016/j.arr.2016.11.004
Rosenberg JR, Amjad AM, Breeze P, Brillinger DR, Halliday DM (1989) The Fourier approach to the identification of functional coupling between neuronal spike trains. Prog Biophys Mol Biol 53:1–31. https://doi.org/10.1016/0079-6107(89)90004-7
Sasaki K, Tomioka Y, Ishii N (2012) Activation of fast-twitch fibers assessed with twitch potentiation. Muscle Nerve 46:218–227. https://doi.org/10.1002/mus.23290
Semmler JG, Sale MV, Meyer FG, Nordstrom MA (2004) Motor-unit coherence and its relation with synchrony are influenced by training. J Neurophysiol 92:3320–3331. https://doi.org/10.1152/jn.00316.2004
Spencer A, Davis K, Jacobs C, Johnson D, Ireland ML, Noehren B (2020) Decreased quadriceps force steadiness following anterior cruciate ligament reconstruction is associated with altered running kinematics. Clin Biomech 72:58–62. https://doi.org/10.1016/j.clinbiomech.2019.11.021
Taylor AM, Christou EA, Enoka RM (2003) Multiple features of motor-unit activity influence force fluctuations during isometric contractions. J Neurophysiol 90:1350–1361. https://doi.org/10.1152/jn.00056.2003
Tracy BL (2007) Force control is impaired in the ankle plantarflexors of elderly adults. Eur J Appl Physiol 101:629–636. https://doi.org/10.1007/s00421-007-0538-0
Vanden Noven ML, Pereira HM, Yoon T, Stevens AA, Nielson KA, Hunter SK (2014) Motor variability during sustained contractions increases with cognitive demand in older adults. Front Aging Neurosci 6:97. https://doi.org/10.3389/fnagi.2014.00097
Vette AH, Sayenko DG, Jones M, Abe MO, Nakazawa K, Masani K (2017) Ankle muscle co-contractions during quiet standing are associated with decreased postural steadiness in the elderly. Gait Posture 55:31–36. https://doi.org/10.1016/j.gaitpost.2017.03.032
Walker S, Avela J, Wikgren J, Meeusen R, Piitulainen H, Baker SN, Parviainen TM (2019) Aging and strength training influence knee extensor intermuscular coherence during low- and high-force isometric contractions. Front Physiol 9:1933. https://doi.org/10.3389/fphys.2018.01933
Walker S, Piitulainen H, Manlangit T, Avela J, Baker SN (2020) Older adults show elevated intermuscular coherence in eyes-open standing but only young adults increase coherence in response to closing the eyes. Exp Physiol 105:1000–1011. https://doi.org/10.1113/EP088468
Watanabe RN, Kohn AF (2015) Fast oscillatory commands from the motor cortex can be decoded by the spinal cord for force control. J Neurosci 35:13687–13697. https://doi.org/10.1523/jneurosci.1950-15.2015
Watanabe T, Saito K, Ishida K, Tanabe S, Nojima I (2018) Coordination of plantar flexor muscles during bipedal and unipedal stances in young and elderly adults. Exp Brain Res 236:1229–1239. https://doi.org/10.1007/s00221-018-5217-3
Weersink JB, de Jong BM, Halliday DM, Maurits NM (2021) Intermuscular coherence analysis in older adults reveals that gait-related arm swing drives lower limb muscles via subcortical and cortical pathways. J Physiol 599:2283–2298. https://doi.org/10.1113/jp281094
Acknowledgements
The authors thank Prof. Naokata Ishii and Ms. Yukie Aoki (Graduate School of Arts and Sciences, The University of Tokyo) for their help in conducting the experiment. This work was supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan (No. 21700651 to K.S.).
Funding
This work was supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan (No. 21700651 to K.S.).
Author information
Authors and Affiliations
Contributions
Conceptualization, KS; Methodology, KS; Software, KS, JX; Validation, JX; Formal analysis, TY, JX, KS; Data curation, TY; Investigation, KS; Writing original draft, TY, JX, KS; Visualization, TY, JX; Supervision, KS; Funding acquisition, KS.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Approval was obtained from the Ethics Committee for Human Experiments, the University of Tokyo. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from the participants.
Additional information
Communicated by Bill J Yates.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yamaguchi, T., Xu, J. & Sasaki, K. Age and sex differences in force steadiness and intermuscular coherence of lower leg muscles during isometric plantar flexion. Exp Brain Res 241, 277–288 (2023). https://doi.org/10.1007/s00221-022-06517-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-022-06517-1