
Abstract
Although there still is conflicting evidence whether schizophrenia is a neurodegenerative disease, cognitive changes in schizophrenia resemble those observed during normal aging. In contrast to extensively demonstrated deficits in explicit learning, it remains unclear whether implicit sequence learning is impaired in schizophrenia and normal aging. Implicit sequence learning was investigated using a computerized drawing task, the ‘implicit pattern learning task (IPLT)’ in 30 stable patients with schizophrenia, 30 age-matched controls and 30 elderly subjects on two consecutive days and after 1 week (sessions 1, 2 and 3). Fixed sequence trials were intermixed with random trials, and sequence learning was assessed by subtraction of the response time in fixed sequence trials from random trials. Separate analyses of response times and movement accuracy (i.e., directional errors) were performed. Explicit sequence knowledge was assessed using three different awareness tasks. All groups learned equally during sessions 1 and 2. In session 3, control subjects showed significantly larger learning scores than patients with schizophrenia (p = .012) and elderly subjects (p = .021). This group difference is mainly expressed in movement time and directional errors. Patients with schizophrenia demonstrated less subjective sequence awareness, and both patients with schizophrenia and elderly subjects had less explicit sequence recall. Explicit recall was positively correlated with task performance in all groups. After a short 24 h interval, all subjects showed similar improvements in implicit sequence learning. However, no benefit of prior task exposure 1 week later was observed in patients with schizophrenia and elderly subjects compared to controls. As patients with schizophrenia and elderly both display less explicit sequence recall, the control group superiority after 1 week could be explained by an explicit learning component. The few patients with schizophrenia and elderly subjects who had some sequence recall could possibly utilize this explicit knowledge to improve their task performance but did this by distinct mechanisms.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The functional outcome of schizophrenia is substantially correlated with the severity of the cognitive symptoms (Green and Heaton 2004). The fast and progressive cognitive decline led initially to the conceptualization of schizophrenia as a disorder of chronic brain deterioration (Kraepelin 1971). Although the neurodegenerative nature of schizophrenia is currently under debate, there is evidence supporting the hypothesis that schizophrenia is associated with accelerated aging at a genetic and neuroanatomical level (Tang et al. 2009). On a clinical level, both patients with schizophrenia and normal aging subjects show a decline in cognitive functioning. However, patients with schizophrenia experience the greatest cognitive decline over a shorter period of time (mainly during the premorbid and prodromal stage of the illness) (Heaton et al. 1994) compared to normal aging-associated changes. For this reason, Kirkpatrick et al. (2008) argued that the early stage of schizophrenia can be considered as a period of ‘compressed aging.’ Importantly, there is a strong overlap between the cognitive domains that are affected in schizophrenia and those that are also vulnerable to decline in normal aging with processing speed, high-load information processing and explicit learning being the cognitive domains that are most consistently demonstrated to be affected (Bowie and Harvey 2006). Even though both groups seem to display similar deficits on identical neurocognitive tasks, to our knowledge, the performance between healthy elderly volunteers and patients with schizophrenia has never been directly compared on exactly the same tasks.
While deficits in explicit learning have been extensively demonstrated (Horan et al. 2008; Kalkstein et al. 2010), the literature is still inconclusive whether implicit learning is impaired in both schizophrenia (Remillard 2014; Siegert et al. 2008) and normal aging (Howard et al. 2013; Verneau et al. 2014). Implicit learning refers to the automatic and unconscious learning of information in contrast to explicit learning which involves the deliberate purpose to learn and requires conscious awareness (Horan et al. 2008). Implicit learning is a complex cognitive domain covering different learning paradigms (Seger 1994) which can be separately investigated by distinct neuropsychological tasks. While probabilistic classification, rotor pursuit, artificial grammar learning and word-stem completion tasks have been typically found to be preserved in schizophrenia (Baddeley 2002; Horan et al. 2008), implicit sequence learning (ISL), which refers to unconscious incremental acquisition of sequential information, has been reported to be impaired (Pedersen et al. 2008; Siegert et al. 2008). ISL involves primarily the dorsolateral striatum, the primary (pre)motor cortex and cerebellum (Ashe et al. 2006; King et al. 2013) and is considered to be unrelated and fundamentally different from explicit sequence learning, which involves the anterior striatum and the prefrontal cortex (Marvel et al. 2005).
The serial reaction time task (SRTT) (Nissen and Bullemer 1987) has proven to be a relevant instrument to study motor sequence learning in many human populations. In the implicit SRTT version, unknown to the participants, a fixed sequence of visual targets is usually presented repeatedly on a computer screen. Participants are instructed to react as fast as possible to these targets by pressing on a spatially corresponding button on a keyboard. Two main implicit learning components contribute to test results, namely sequence-specific learning and task-specific learning. Participants learn the sequence based upon the order in which the fixed targets appear on the screen (a form of visuospatial learning) and upon the order in which associated movements (such as key presses) are made (a form of sensorimotor learning). These two sequence learning mechanisms derive from distinct brain areas and circuits (Hikosaka et al. 1999). Task-specific learning (a form of procedural learning) encompasses all task-related information such as feedback signals, timing and location of stimulus presentation, or the position of the hand and fingers.
Up until to date, it remains unclear whether ISL as measured by the SRTT is impaired in schizophrenia (Gold et al. 2009; Remillard 2014) and during aging (Brown et al. 2009; Howard et al. 2013; Verneau et al. 2014). These inconsistent findings may be explained by methodological limitations in previous SRTT studies in both populations. Firstly, studies used small numbers of sequence repetitions (5–10 fixed sequence repetitions and only one session) (Adini et al. 2015). However, it has been shown that the amount of online ISL depends on the number of sequence repetitions per session (Marvel et al. 2007). In addition, as few longitudinal studies are available, there is no clear understanding about retention and offline consolidation effects (Janacsek and Nemeth 2013). Secondly, most SRTT studies use little visuospatial variation in their tasks and might be too simple to detect visuospatial deficits. However, it has also been shown that there are specific visuospatial deficits in schizophrenia (Hardoy et al. 2004; Khosravani and Goodarzi 2013; Kravariti et al. 2006) and aging (Alescio-Lautier et al. 2007) that influence implicit learning. For example, studies using non-visuospatial versions of the SRTT in schizophrenia found only accuracy (i.e., error-related) deficits, whereas a visuospatial version demonstrated larger impairments on both accuracy and response times (Marvel et al. 2005). Using the implicit pattern learning task (IPLT), a task with more visuospatial demands, learning deficits which were not detected by the SRTT were found in patients with mild cognitive impairment, Parkinson’s disease (Van Tilborg and Hulstijn 2010) and Korsakoff’s syndrome (Van Tilborg et al. 2011); however, this task has not been used in schizophrenia. Finally, explicit learning is well known to be impaired in schizophrenia and normal aging, but its presence in an implicit learning task cannot be excluded (Destrebecqz and Peigneux 2005). In order to further investigate implicit learning in schizophrenia and elderly, it is essential to overcome these methodological limitations.
This paper is part of a larger study that aims to compare the performance of patients with schizophrenia, elderly volunteers and healthy controls on a battery of different explicit and implicit psychomotor learning tasks. The aim of the current study is to understand better whether implicit sequence learning, a skill that is indispensable in performing elementary activities such as tying shoes, is impaired in patients with schizophrenia and healthy aging. Given the arguments for a visuospatial deficit in schizophrenia and aging, the IPLT was used, in which pen movements toward a larger number of possible targets are recorded on a digital writing tablet. Multiple test repetitions over several days allowed a detection of possible learning deficits on later learning phases. The hypothesis of the study was that patients with schizophrenia and older subjects would show less ISL improvement across sessions than controls since it has been demonstrated that both groups display deficits in motor sequence memory consolidation (Brown et al. 2009; King et al. 2013). Lastly, the presence and role of an explicit learning component was explored using three different awareness tasks, which were compared with each other and related to the task performance: a non-suggestive oral questionnaire, a sequence recognition task and an explicit recall task. It was expected that both patients with schizophrenia and elderly would demonstrate explicit learning deficits (Horan et al. 2008; Kalkstein et al. 2010).
Methods
Participants
Our study group consisted of 30 stably treated patients with schizophrenia (aged 18–55 years) who had not experienced a psychotic relapse in the past 2 months, 30 age- and gender-matched control participants, and 30 gender-matched elderly volunteers (aged 65–85 years). The patients were recruited from psychiatric hospitals in the area of Antwerp, Belgium and the healthy controls were recruited from the local community. All candidates provided a written informed consent. Participants receiving treatment with benzodiazepines and anticholinergics (including tricyclic antidepressant drugs) were excluded from participating in the study because of their documented negative effects on cognition. The inclusion and exclusion criteria for the three groups are described in detail in our previously published papers where the same groups of participants were studied (Cornelis et al. 2014; De Picker et al. 2014). The test was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki and that are consistent with Good Clinical Practices, applicable regulatory requirements, and in compliance with the study protocol. This study was conducted at the University Psychiatric Hospital Duffel, Belgium, and the study protocol was reviewed and approved by the institute’s Ethics Committee. The study is registered at ClinicalTrials.gov: NCT01788436.
Implicit pattern learning task (IPLT)
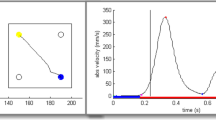
Participants were seated in front of a laptop computer and performed the IPLT writing task on a sheet of plastic that was fixed on a digitizing (WACOM) writing tablet. In order to control the cursor movements to different targets on the computer screen, subjects used a normal-looking, non-inking pen to move across the plastic sheet. The position of the pen tip was recorded on and up to 5 mm above the tablet. Sixteen 10-mm-diameter target circles were continuously displayed on the computer screen, positioned in a rhombus of four-by-four targets on equal distances from each other (see Fig. 1).

Target display on the computer screen during the IPLT. Turquoise circle starting position, i.e., the previous target after being hit by the cursor. Dark blue target the next target. Dark blue trajectory the trajectory of the twelve consecutive fixed sequence targets starting from target 11: 15, 14, 10, 13, 9, 10, 5, 6, 1, 5, 2, and 7. Black bold trajectory an example of pen movements on the fixed sequence targets. Black trajectory possible pen movements on eight random targets. A target error is shown on the pen trajectory on fixed trial 6, and five movement errors in which the movement started in the wrong direction (directional errors, DE) are marked. The display seen by the participants consisted solely of the turquoise pen cursor, the sixteen circles (without the numbers), the turquoise starting position and one target circle being filled dark blue (color figure online)
Each trial consisted of one target turning dark blue. Participants were instructed to move the cursor (a turquoise dot with 4 mm diameter) toward the dark blue target as quickly as possible by moving the non-inking pen on the digitizing tablet. The cursor had to be held inside that target circle for 100 ms. A correct hit (and stay of 100 ms) of the target circle by the cursor was indicated by a beep and a color change of that target circle to turquoise. From the moment the beep sounded, there was a short intertrial interval lasting for 100–108 ms, which was needed to write the data of the previous trial away. After this, the next trial started with a new, adjacent target turning dark blue. The turquoise starting position remained visible until the dark blue target was reached. The trials were presented either in learning blocks, consisting of repetitions of a fixed 12-target sequence, or in pseudo-random blocks, consisting of eight random targets which did not contain a fixed sequence. The total duration of one IPLT session took on average in 15 min.
The IPLT task was assessed in three sessions, conducted on two consecutive days (sessions 1 and 2) and 7 days later (session 3). In session 1, a first 60-trial pseudo-random block (R1) was followed by five 100-trial learning blocks (L1–L5), where the eight random targets followed by the 12-target fixed sequence were repeated five times. The five learning blocks were followed by a seventh pseudo-random block (R2) of 60 trials at the end of the session. Sessions 2 and 3 were largely similar to session 1, but consisted of only three learning blocks (L1–L3) instead of the original five. In between the blocks, participants were given a short self-timed break of about 20 s to reduce fatigue. All participants were examined individually.
On each session, the IPLT was performed as the third task during a larger 120-min neuropsychological test battery, after having performed a symbol digit substitution task, of which the results have been published elsewhere (Cornelis et al. 2014). Before every IPLT session, a practice exercise was performed in order to get familiar with the use of a digital writing tablet, the non-inking pen and the connection/coordination between pen movements and cursor movements on the computer screen.
Awareness tasks
The participants were not informed about the repeated sequence. Yet, by debriefing following each IPLT assessment a subjective awareness test was performed. After this debriefing on session 3, participants were informed about the fixed sequence, after which two additional more objective tests, one recognition test and one recall test, were performed.
Subjective awareness test
After each IPLT session, participants were asked if they had noticed anything with respect to the task to probe whether they had become aware about the tasks’ fixed sequence. Because the participants needed to remain naïve with regard to the fixed sequence until the end of the session 3, this question was asked in a sensitive, non-suggestive fashion. A degree of explicit awareness was scored when participants were able to verbalize that there seemed to be a repeating pattern in the task or found the middle (learning) blocks went smoother.
Recognition test
Four blocks each consisting of twenty trials were performed with the third block containing the fixed sequence and the other three blocks being entirely different from the fixed sequence. The participant was asked to estimate how likely it was that this sequence appeared during the IPLT by scoring each block on a scale of 0–100 % with 0 % meaning absolute certainty that the sequence did not appear in the IPLT and 100 % indicating that the subject was entirely certain that the presented sequence was identical to the fixed sequence in the IPLT.
Recall test
Participants were asked to try to actively regenerate the pattern on two identical test blocks, consisting of the twelve sequence targets. The next target was not signaled automatically anymore, and as soon as the right circle was hit, a beep sounded and this circle colored turquoise as in the normal IPLT, after which the next target could be searched for.
Analysis
We considered the general decrease in response time and errors across learning block L1 to L5 to depend on the combination of task- and sequence-specific learning. The difference in response time on sequence trials from random block R2 to the preceding learning block L5 or L3 was regarded as a measure of sequence learning and the decrease across random trials to be caused by task-related learning. The averaged differences in response time between the fixed and random trials and their increase over consecutive learning blocks provide an estimate of the learning rate within one session. The mean total response time per target (TT) was separated into the time needed to initiate a movement (mean reaction time, RT) and the time needed to cross the distance between the two circles (mean movement time, MT). The RT is measured as the time between the onset of stimulus presentation and the time at which the pen left the starting circle and crossed its 0.4-cm periphery (total diameter 3.4 cm). The MT is the time taken to cross the distance between the start-circle’s periphery and the periphery of the target circle. The spatial nature of the writing task allowed an analysis of detailed pen movements in different correct and wrong directions. The increase of the amount of directional errors (DEs) from L5 to R2 was used as a measurement of accuracy and enabled a detection of potential learning strategies. DEs were movements that left the starting circle at the wrong angle, i.e., deviations of >22.5° from the most optimal angle. This movement toward a wrong target in the first stage of the movement could still be corrected during the later stages of the movement, in contrast to a target error where a wrong (blank) target had been hit after making a DE.
All data were analyzed with ANOVA (GLM) repeated measures in IBM SPSS version 22. The schizophrenia group was compared with the control group, and the elderly group was compared with the same control group for the measures of significance (planned comparisons). Bonferroni post hoc analysis was used to compare the schizophrenia with the elderly group. Alpha was set at 0.05 throughout the study analyses.
Results
The demographic features of the three study groups and the distribution and daily doses of the antipsychotic drugs in patients with schizophrenia are summarized elsewhere (De Picker et al. 2014). As the data of one schizophrenia patient were missing due to a computer error, the performance levels of 29 patients with schizophrenia, 30 healthy controls, and 30 elderly patients were analyzed. To assess the effect of antipsychotic medication on the amount of ISL in patients with schizophrenia, the mean doses of antipsychotics were converted to chlorpromazine equivalents (Ceq). Six patients taking a depot variant of paliperidol, olanzapine and bromperidol were excluded as it was not possible to find reliable Ceq values for these three depot antipsychotic agents. The amount of sequence learning of the remaining 23 patients did not significantly correlate with the Ceq values (Spearman’s ρ: session 1 ρ = 0.20; session 2 ρ = −0.34; session 3 ρ = 0.07). The median dosage (400 Ceq) and the Belgian Center for Pharmacotherapeutic Information (2016) were used to divide all 29 patients into two categories of a relatively high or a relatively low dosage. Analyses of variance (GLM) on the TT values of the random and on the fixed sequence trials did not reveal any significant difference (p > 0.20) between the high- and the low-dose groups in any of the three sessions. The main outcome measure of the IPLT is the TT needed to reach a target. Group means over sessions and trial blocks within sessions are presented in Fig. 2. The figure shows two lines per group: one for the eight random targets and one for the twelve targets that were presented in a fixed sequence during the learning blocks (L1–L5) and in a random order during blocks R1 and R2. Before analyzing the data on sequence learning, we will first describe the sensorimotor learning results as shown by the responses to random targets.

Mean TT to reach random (filled markers) or fixed sequence targets (open markers) per block and session for the three groups. R1 and R2 are the random blocks and L1–L5 are the learning blocks on sessions 1, 2 and 3
Sensorimotor learning
Figure 2 shows that in general the control group (C) was much faster than the schizophrenia (S) and the elderly (E) group. ANOVA (GLM) showed on the TT means of the eight random targets with session (3) and block (5; only the first five blocks in session 1) as within-subject factors and group (3) as between-subject variable a significant group effect (F (2,86) = 26.99, p < .0001). Contrasts of group C (423 ms) with group S (531 ms) and with group E (541 ms) were significant (both p < .0001), whereas groups S and E were not different (p = .564).
ANOVA also showed considerable sensorimotor learning (TT reduction) over the three sessions (F (2,85) = 157.42, p < .0001) and over the blocks within the sessions (F (4,83) = 50.88, p < .0001). In addition, group differences in sensorimotor learning rate were found, as shown in the block by group interaction (F (8,166) = 5.25, p < .0001) and the session by group interaction (F (4,170) = 4.04, p = .004), while the highest order interaction (session by block by group) was not significant (p = .416). The block by group interaction is due to a larger TT decrease from block R1 to block L3 in the elderly (C: 31 ms, S: 38 ms and E: 75 ms; Group S vs. E, block × group: F (4,54) = 7.52, p < .0001). This must have been the result of the relatively large TT of group E in the random trials of block R1, because an analysis only over blocks L1 till L3 did not produce a significant block by group interaction any more (F (3,55) = 2.09, p = .112). Elderly persons seemed to have had much more problems with the very first trials of the task, at least in sessions 1 and 2 (see Fig. 2).
The elderly also differed in the amount of learning over sessions from the other groups. The significant session by group interaction is caused by the larger decrease in TT of the elderly (sessions 1–3: 592–532–499 ms) compared to the session reductions of group S (567–527–499 ms) and group C (453–416–399 ms). Even when only four blocks were averaged (omitting R1) and when only groups S and E were compared, the decrease over sessions was larger in the elderly (F (2,56) = 3.57, p = .035). In Fig. 2, this is shown by the larger TT of group E compared to group S in the random targets on session 1 (particularly on blocks L2–L4) and the disappearance of this difference in sessions 2 and 3.
Sequence learning per session
The amount of sequence learning can be determined by comparing targets in a fixed sequence with a control condition in which the order of targets is random. In the present study, this was done first in the traditional way by calculating for each session the difference in mean TT of random block R2 and the preceding learning block (L5 in session 1 and L3 in sessions 2 and 3). Figure 2 shows marked increases in TT from the last learning block to the subsequent random block (R2) for all groups in all sessions. ANOVA (GLM) on session (3 levels) and block (2 levels: last learning block vs. R2) as within-subject variables and group (3 levels) as between-subject factor showed a strong effect of sequence learning (block: F (1,86) = 313.08, p < .0001). In this analysis, the effect of session was also significant (F (2,85) = 75.99, p < .0001) as well as the block by session interaction (F (2,85) = 8.84, p = .0003).
To illustrate the amount of learning in the three sessions, the differences in TT between the final random blocks and the preceding learning blocks are displayed in Fig. 3 (left panel). The figure shows that in session 1 the degree of sequence learning was substantial (F (1,86) = 159.64, p < .0001) and equal for the three groups (F (2,86) = 0.28, p = .754). Session 2, compared to session 1, showed a higher degree of sequence learning in the three groups (F (1,86) = 8.42, p = .005). The lack of an interaction between session (sessions 1 and 2) and group (F (2,86) = 0.20, p = .816) demonstrates that this increase was about equal for the three groups. However, in session 3 the learning score of the control group improved again, while the other two groups remained on the same level as in session 2. The group by session (3 levels) interaction showed a significant linear contrast (F (2,86) = 3.61, p = .031) and simple contrasts on TT differences in session 3 yielded significant group differences between the control group and the other two groups (C–S: p = .012; C–E: p = .021).

Amount of learning at the end of the three sessions revealed by the differences between the final random block (R2) and the preceding learning block (L5 in session 1 or L3 in sessions 2 and 3)
More information on this control group superiority in the third session is gained by inspection of the RT and MT components of the TT (see Fig. 3). The shortening of RT with sequence learning was substantial (F (1,86) = 246.38, p < .0001), but did not improve over sessions (F (2,85) = 0.24, p = .784). It was equal for the three groups (F (2,86) = 1.53, p = .224) and did not show any group by session interaction (F (4,170) = 1.10, p = .360). However, MT offered a different picture. Like RT, the overall reduction in MT as a result of learning the sequence was large (F (1,86) = 82.56, p < .0001), but now the effects of session (F (2,85) = 12.51, p < .0001) and group by session (F (4,170) = 5.30, p = .0005) were significant. These effects were mainly caused by the control group. A reduction in MT can be obtained by increasing movement speed, but the main factor was probably avoiding the detours caused by starting the movement in the wrong direction. The fourth panel of Fig. 3 shows that the difference in percentage of DEs between blocks R2 and L5/L3 shows a similar picture as the differences in MT (group × session: F (4,170) = 3.20, p = .015). On random trials, the percentage of DEs increased over blocks within each session from 15 to 28 % (averaged over groups; not displayed in Fig. 3). This is possibly due to an increase in the tendency to start before the proper target has been identified. On fixed sequence targets, however, DEs decrease over learning blocks (in session 2 from 21 to 18 % and in session 3 from 20 to 16 %). When the fixed sequence turns into a random order, in the R2 blocks, large increases in percentage of DEs occur (shown in Fig. 3) which result in higher numbers of corrected trajectories with large detours from a straight path. This effect proved to be stronger for the control group in session 3 (simple contrasts C–S: p = .015; C–E: p = .021).
Sequence learning per block
The design of the present study, by including random trials in the learning blocks with fixed sequence trials, made it possible to test whether the groups differed in their learning speed already in the first learning blocks and not only at the final block in a session. However, as can be seen in Fig. 2, the TT to move to the 8 random targets was higher in block R1 than the TT to the 12 future fixed sequence targets (535 vs. 514 ms, F (1,86) = 53.81, p < .0001). Therefore, to test whether the measure of learning, i.e., the difference between random and fixed trials, is larger in blocks L2 till L5 compared with the first learning block, the differences at L1 were subtracted from the differences at L2, L3, L4 and L5. The resulting group means are displayed in Fig. 4. ANOVA on these data showed no group effect (F (2,86) = 0.11, p = .89), the block effect was significant (F (3,84) = 11.85, p < .0001), the significant block by group interaction (F (6,168) = 2.16, p = .049) was only caused by a cubic contrast (p = .007), and the linear and quadratic contrasts (p = .293 and p = .793) were not significant. Figure 4 also shows that sequence learning could be observed already in block L2. An analysis on these corrected L2 differences demonstrated a substantial improvement in L2 (F (1,86) = 42.06, p < .0001), which was equal for the three groups (F (2,86) = 1.04, p = .359). This means that significant sequence learning appeared already after 5 repetitions of the 12-target sequence (in L1) in all three groups alike.

Difference in TT per group between random and fixed sequence trials per block (L1–L5) in session 1 corrected for differences in L1. For comparison, the R2–L5 TT differences of session 1 (presented earlier in Fig. 3) are also shown
Awareness
The three different awareness tasks are significantly different from each other, but these tasks also correlated with each other. The subjective awareness task differed significantly from the recognition task (χ 2 = 8.45, p = .004) and from the recall task (χ 2 = 4.93, p = .026), and the recognition task differed significantly from the recall task (χ 2 = 8.99, p = .003). The subjective awareness task correlated significantly with the recognition task (r = .30, p = .004) and with the recall task (r = .23, p = .026) and the recognition task correlated significantly with the recall task (r = .31, p = .003).
The degree to which explicit knowledge had developed over the ISL task was assessed after each session by a subjective awareness questionnaire and—only after session 3—by a recognition test and a recall test. In order to split the data of the three awareness tasks into the dichotomous categories ‘explicit knowledge’ and ‘no explicit knowledge,’ the participants that scored higher than a criterion were counted. This criterion was set to a positive answer to the first question for subjective awareness and to the median score over all 89 participants for the recognition and recall tests. The percentage of participants who scored higher than these criteria is presented in Table 1. The schizophrenia group, as compared to the control group, was significantly lower on subjective awareness in session 1 (\(\chi_{(1)}^{2}\) = 4.39, p(2-sided) = .036) and session 3 (\(\chi_{(1)}^{2}\) = 7.04, p = .008) and on the recall test (\(\chi_{(1)}^{2}\) = 8.96, p = .003). The elderly group was significantly higher than the schizophrenia group on subjective awareness in session 3 (\(\chi_{(1)}^{2}\) = 5.15, p = .023) and on the recognition test (\(\chi_{(1)}^{2}\) = 4.88, p = .027). It differed significantly from the control group only in the recall test (\(\chi_{(1)}^{2}\) = 6.70, p = .010).
The relation between explicit knowledge and the amount of sequence learning (assessed by the TT difference between blocks R2 and L5/L3) was explored by calculating correlations (Spearman’s ρ and for recall Pearson r). These correlations are presented in Table 1. Correlations higher than or equal to 0.31 are significant (without correcting for multiple testing). The first and most striking result is that subjective awareness correlated significantly with amount of sequence learning only in the elderly and control groups. For the schizophrenia group, this correlation was even close to zero at the first session. This is in agreement with the finding that the amount of sequence learning of the 12 patients with schizophrenia without subjective awareness was equal to that of the 17 patients with schizophrenia who expressed some amount of subjective awareness (TT difference R2–L5: 50 vs. 51 ms; t (27) = −0.07, p = .949).
The second finding that emerges from these correlations is that the Recognition test scores had no significant relation with sequence learning in contrast with the recall test scores. On this latter test, the median score amounted to eight of the twelve targets that were pointed out without any error. This seems to suggest a substantial amount of explicit knowledge, but it must be recognized that it took a considerable amount of time to express this knowledge. The mean TT in the recall test was 1793 ms (2197, 1958 and 1223 ms for groups E, S and C), while the mean TT in block L3 of session 3 was more than four times faster, i.e., 392 ms (424, 436 and 316 ms for groups E, S and C).
The recall task shows that in patients with schizophrenia and in elderly there is a different contribution of explicit knowledge. In Table 2 is demonstrated that there is a significant correlation between awareness on recall and the performance on RTs in patients with schizophrenia. In the elderly, on the contrary, there is a significant correlation between the recall task and RTs and MTs and especially the amount of DEs. The elderly persons with awareness on recall (37 %) had significantly better MTs and DEs, while the aware persons in the control group (68 %) and schizophrenia group (32 %) showed the same performance levels on MT and DE.
The elderly might have profited from their explicit knowledge by making less DE. Importantly, while in patients with schizophrenia and the elderly the better performance levels can be partly attributed to explicit learning, this is not the case for the controls.
Discussion
This study investigated ISL in patients with schizophrenia, elderly subjects and young healthy controls. The main findings of the study were that all subjects showed an equally increasing amount of learning on two consecutive test days. However, when retested after 1 week, no further learning improvements were detected in patients with schizophrenia and the elderly in contrast to the controls who showed an ongoing linear improvement in their performance on the learning task. Explicit sequence recall was correlated with sequence learning in all subjects, indicating that the impaired performance in patients with schizophrenia and elderly subjects after 1 week might be related to explicit learning deficits.
In general, sensorimotor learning (on random trials) was found to be preserved in the elderly and in patients with schizophrenia. The elderly subjects were slower on the first random trials of each session, which might indicate difficulties to initiate the task or a poorer between-session sensorimotor skill consolidation in the elderly, although this group difference disappeared in the following learning blocks. The elderly showed more task-specific sensorimotor learning than patients with schizophrenia and controls during sessions 1 and 2, which is in line with previous SRTT findings in aging (Brown et al. 2009). This enhanced sensorimotor learning may be explained as a compensational mechanism for the explicit learning deficits in aging (Poldrack and Packard 2003) as compensatory increases in motor cortical and the cerebellar activation has been observed in older individuals (Mattay et al. 2002).
The control group superiority on session 3 might be explained by the combination of sequence-specific learning as their amount of DEs was only reduced on fixed trials, indicating that they anticipated the next target and moved the pen in the anticipated direction, and task-specific learning, as there was a general increase in movement speed. The elderly had also a lower amount of DEs only on fixed trials which might indicate that they were able to orient their attention to the next stimulus and learn the sequence, but they seemed not to benefit actively from this knowledge by increasing movement speed. Patients with schizophrenia had less DEs on both fixed and random trials, which suggests that their slower MTs enabled them to wait patiently until the next target appeared instead of actively searching for the next target. This result is in line with previous findings that patients with schizophrenia demonstrate greater difficulty to disengage their attention from attended stimuli (Remillard 2014) and show a delayed anticipatory orienting toward subsequent stimuli (Mushquash et al. 2012).
Although the elderly were found clinically healthy and free from disorders that might impair task performance, factors such as arthritis, sarcopenia, atrophy of the basal ganglia and a declining dopaminergic function which might have contributed to the slowing of their hand movements (Smith et al. 2005) could not be excluded. In schizophrenia, the slower MTs could be influenced by psychomotor slowing that is inherent to the illness (Morrens et al. 2006) and by extrapyramidal symptoms due to dopaminergic antagonist action of most antipsychotic drugs (Leucht et al. 1999; Morrens et al. 2008). All patients were stably treated with antipsychotic medication at the time of testing; however, we found no dose–response relationship between the used antipsychotic dosage (in chlorpromazine equivalents) and sensorimotor performance on the IPLT.
The 12-target sequence was learned already after 5 repetitions on the first learning block in all groups. This finding is similar to the findings of Nissen and Bullemer (1987) who found that sequence learning of a 10-trial sequence occurs after 6 sequence repetitions. The relatively fast learning of the sequence may be explained by the spatial character of our task as studies that used simpler but less spatial sequences reported that 25–40 sequence repetitions were needed (Oostwoud et al. 2016).
As most of the participants noticed that the targets were not random and the amount of aware persons increased across sessions, it can be argued that a variable amount of explicit sequence learning might have influenced the IPLT results.
As expected both patients with schizophrenia and elderly subjects demonstrated less explicit learning, but the nature of this deficit probably varied among both groups. Subjective awareness seemed to improve the IPLT performance in the controls and the elderly, but not in patients with schizophrenia. The recognition task did not correlate with the IPLT performance in any group, and recall was positively correlated with the IPLT performance in all groups. The apparently (but not significantly) smaller correlation of recall with IPLT performance in controls is counterintuitive but might be explained by the generally high score of recall in the controls. The higher amount of sequence learning in the controls on session 3 might be explained by more subjective awareness and the capacity to use this knowledge actively. The elderly showed a normal subjective awareness but had an impaired capacity to move the pen quickly in the anticipated direction, and the patients with schizophrenia demonstrated already deficits in the subjective knowledge of a fixed pattern. As the patients had a normal performance on session 1 and on this session there were no significant performance differences between aware and unaware patients, this supports our conclusion that ISL is preserved in schizophrenia. The few patients with schizophrenia who demonstrated explicit recall on session 3 might have used this knowledge to predict the next target’s location, while the elderly subjects used this knowledge mainly to improve their movement time.
In a recent study, the existence of ISL was altogether questioned as the authors found that only participants who did not learn the sequence explicitly did also not learn it implicitly and vice versa (Oostwoud et al. 2016). In contrast, our study demonstrates that the participants (2 controls, 3 elderly subjects and 10 patients with schizophrenia) without any awareness on session 3 nevertheless showed a significant amount of sequence learning (p = 0.003).
There are some limitations concerning the awareness tasks as the interpretation largely depends on the sensitivity of the utilized task. Verbal report by a subjective awareness questionnaire is the most frequently used task, but it is often influenced by the patient’s cooperativeness and self-confidence about the sequence. Subjects might be aware of parts of the sequence that are not addressed by the questions, and, alternatively, answering affirmatively might be the result of a positive response bias. To maximize the detection of explicit knowledge, more objective, forced-choice tasks have been developed (Perruchet and Amorim 1992). In our study, recall had the largest correlations with IPLT performance, but this task is not often used in other studies, not consistently conducted and prone to contamination by implicit sequence knowledge such as guessing based on a feeling of familiarity and sensorimotor practice effects (Gaillard et al. 2014).
Although it is difficult to rule out the effect of reduced motivation, we conclude based on our observations during the IPLT and other neurocognitive tasks that it was unlikely that a lack of motivation accounts for the drop in performance on session 3. As only patients who were able to complete the test batteries were included, our results cannot be generalized to the whole population of schizophrenic patients.
Finally, we remark that the positive correlation between the awareness and IPLT performance does not automatically imply a causal relation: it remains uncertain whether sequence awareness facilitates the performance on the IPLT. It is possible that the IPLT score improved due to explicit knowledge as our observation of DEs in controls shows that they must have moved the pen anticipatorily. However, it is equally possible that participants who learned better implicitly had a better awareness at the end due to active searching based on an implicit feeling of familiarity. The next target might also have appeared so quickly that participants did not have adequate time to benefit from their explicit knowledge: TTs during recall were generally fourfold higher than during the IPLT because here participants were instructed to actively find the next stimulus instead of working as fast as possible. It is most likely that both factors influenced each other.
The current study puts the cognitive capacities of patients with schizophrenia and healthy aging in an optimistic clinical perspective. Patients with schizophrenia and elderly subjects had a similar task performance in the first two sessions but seemed to utilize different working strategies. As patients with schizophrenia showed less subjective awareness and the elderly seemed to have rather problems in using this knowledge actively, it might be interesting whether rehabilitation programs focusing on increasing awareness and how to utilize it (e.g., improving the active verbalization of possible underlying task rules and structures) provide benefiting results in both groups.
Conclusion
On the short term, sequence learning is preserved in patients with schizophrenia and elderly controls and there seems to be no effect of awareness which endorses our hypothesis that implicit sequence learning is preserved in patients with schizophrenia and elderly subjects. Although our study methods do not allow us to conclude that the deficit which becomes apparent on session 2 and especially on session 3 is the result of crescent explicit sequence knowledge in the healthy controls, the correlations of IPLT performance with the measures of awareness make this assumption more plausible. Interestingly, both groups did utilize their smaller but existent amount of explicit awareness in order to improve their task performance, seemingly by employing different strategies.
The current study underlines that there continues to be a bias in the interpretation of implicit sequence learning studies. Further research which aims at disentangling the explicit learning component in these studies might bring to the proof whether ISL performance deficits in schizophrenia can be attributed to a deficit in explicit learning.
References
Adini Y, Bonneh YS, Komm S, Deutsch L, Israeli D (2015) The time course and characteristics of procedural learning in schizophrenia patients and healthy individuals. Front Hum Neurosci 9:1–16. doi:10.3389/fnhum.2015.00475
Alescio-Lautier B, Michel BF, Herrera C, Elahmadi A, Chambon C, Touzet C, Paban V (2007) Visual and visuospatial short-term memory in mild cognitive impairment and Alzheimer disease: role of attention. Neuropsychologia 45(8):1948–1960. doi:10.1016/j.neuropsychologia.2006.04.033
Ashe J, Lungu OV, Basford AT, Lu X (2006) Cortical control of motor sequences. Curr Opin Neurobiol 16:213–221. doi:10.1016/j.conb.2006.03.008
Baddeley A (2002) The handbook of memory disorders, 2nd edn. Wiley, Hoboken
Belgian Center for Pharmacotherapeutic Information (2016) Antipsychotics. Commented Drug Repertory 312–321
Bowie CR, Harvey PD (2006) Treatment of cognitive deficits in schizophrenia. Curr Opin Investig Drugs 7(7):608–613
Brown RM, Robertson EM, Press DZ (2009) Sequence skill acquisition and off-line learning in normal aging. PLoS One 4(8):e6683. doi:10.1371/journal.pone.0006683
Cornelis C, De Picker LJ, Hulstijn W, Dumont G, Timmers M, Janssens L, Sabbe BGC, Morrens M (2014) Preserved learning during the symbol digit substitution test in patients with schizophrenia, age-matched controls and elderly. Front Psychiatry. doi:10.3389/fpsyt.2014.00189
De Picker LJ, Cornelis C, Hulstijn W, Dumont G, Fransen E, Timmers M, Morrens M, Sabbe BGC (2014) Stable schizophrenia patients learn equally well as age-matched controls and better than elderly controls in two sensorimotor rotary pursuit tasks. Front Psychiatry 5(165):1–12. doi:10.3389/fpsyt.2014.00165
Destrebecqz A, Peigneux P (2005) Methods for studying unconscious learning. Prog Brain Res 150(6):69–80. doi:10.1016/S0079-6123(05)50006-2
Gaillard V, Cleeremans A, Destrebecqz A (2014) Dissociating conscious and unconscious learning with objective and subjective measures. Clin EEG Neurosci 45(1):50–56. doi:10.1177/1550059413516757
Gold JM, Hahn B, Strauss GP, Waltz J (2009) Turning it upside down: areas of preserved cognitive function in schizophrenia. Neuropsychol Rev 19(3):294–311. doi:10.1007/s11065-009-9098-x
Green MF, Heaton RK (2004) Longitudinal studies of cognition and functional outcome in schizophrenia: implications for MATRICS. Schizophr Res 72:41–51. doi:10.1016/j.schres.2004.09.009
Hardoy MC, Carta MG, Catena M, Hardoy MJ, Cadeddu M, Dell’Osso L, Carpiniello B (2004) Impairment in visual and spatial perception in schizophrenia and delusional disorder. Psychiatry Res 127(1–2):163–166. doi:10.1016/j.psychres.2004.03.002
Heaton R, Paulsen JS, McAdams LA, Kuck J, Zisook S, Braff D, Jeste DV (1994) Neuropsychological deficits in schizophrenics. Relationship to age, chronicity, and dementia. Arch Gen Psychiatry 51(6):469–476
Hikosaka O, Nakahara H, Rand MK, Sakai K, Lu X, Nakamura K, Doya K (1999) Parallel neural networks for learning. Trends Cogn Sci 22(10):464–471. doi:10.1016/S0166-2236(99)01439-3
Horan WP, Green MF, Knowlton BJ, Wynn JK, Mintz J, Nuechterlein KH (2008) Impaired implicit learning in schizophrenia. Neuropsychology 22(5):606–617. doi:10.1037/a0012602
Howard J, James H, Howard DV (2013) Aging mind and brain: is implicit learning spared in healthy aging? Front Psychol 4:1–6. doi:10.3389/fpsyg.2013.00817
Janacsek K, Nemeth D (2013) Implicit sequence learning and working memory: correlated or complicated? Cortex 49(8):2001–2006. doi:10.1016/j.cortex.2013.02.012
Kalkstein S, Hurford I, Gur RC (2010) Neurocognition in schizophrenia. Curr Top Behav Neurosci 4:373–390
Khosravani N, Goodarzi MA (2013) Patients with schizophrenia show deficits on spatial frequency doubling. Vis Res 93:49–53. doi:10.1016/j.visres.2013.10.007
King BR, Fogel SM, Albouy G, Doyon J (2013) Neural correlates of the age-related changes in motor sequence learning and motor adaptation in older adults. Front Hum Neurosci 7:1–13. doi:10.3389/fnhum.2013.00142
Kirkpatrick B, Messias E, Harvey PD, Fernandez-Egea E, Bowie CR (2008) Is schizophrenia a syndrome of accelerated aging? Schizophr Bull 34(6):1024–1032. doi:10.1093/schbul/sbm140
Kraepelin E (1971) Dementia praecox and paraphrenia. Robert E. Krieger Publishing Co., Inc., Huntington
Kravariti E, Toulopoulou T, Mapua-Filbey F, Schulze K, Walshe M, Sham P, McDonald C (2006) Intellectual asymmetry and genetic liability in first-degree relatives of probands with schizophrenia. Br J Psychiatry 188:186–187. doi:10.1192/bjp.bp.104.008177
Leucht S, Pitschel-Walz G, Abraham D, Kissling W (1999) Efficacy and extrapyramidal side-effects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res 35(1):51–68. doi:10.1016/S0920-9964(98)00105-4
Marvel CL, Schwartz BL, Howard DV, Howard J (2005) Implicit learning of non-spatial sequences in schizophrenia. J Int Neuropsychol Soc 11(6):659–667
Marvel C, Turner BM, O’Leary DS, Johnson HJ, Pierson RK, Boles Ponto LL, Andreasen NC (2007) The neural correlates of implicit sequence learning in schizophrenia. Neuropsychology 21(6):761–777. doi:10.1037/0894-4105.21.6.761
Mattay VS, Fera F, Tessitore A, Hariri AR, Das S, Callicott JH, Weinberger DR (2002) Neurophysiological correlates of age-related changes in human motor function. Neurology 58(4):630–635
Morrens M, Hulstijn W, Sabbe B (2006) Psychomotor slowing in schizophrenia. Schizophr Bull 33(4):1038–1053. doi:10.1093/schbul/sbl051
Morrens M, Hulstijn W, Sabbe B (2008) The effects of atypical and conventional antipsychotics on reduced processing speed and psychomotor slowing in schizophrenia: a cross-sectional exploratory study. Clin Ther 30(4):684–692. doi:10.1016/j.clinthera.2008.04.012
Mushquash AR, Fawcett JM, Klein RM (2012) Inhibition of return and schizophrenia: a meta-analysis. Schizophr Res 135(1–3):55–61. doi:10.1016/j.schres.2011.11.034
Nissen MJ, Bullemer P (1987) Attentional requirements of learning: evidence from performance measures. Cogn Psychol 19:1–32
Oostwoud WL, Brenner E, Smeets JBJ (2016) Exposing sequence learning in a double-step task. Exp Brain Res. doi:10.1007/s00221-016-4566-z
Pedersen A, Siegmund A, Ohrmann P, Rist F, Rothermundt M, Suslow T, Arolt V (2008) Reduced implicit and explicit sequence learning in first-episode schizophrenia. Neuropsychologia 46:186–195. doi:10.1016/j.neuropsychologia.2007.07.021
Perruchet P, Amorim MA (1992) Conscious knowledge and changes in performance in sequence learning: evidence against dissociation. J Exp Psychol Learn Mem Cogn 18(4):785–800
Poldrack RA, Packard MG (2003) Competition among multiple memory systems: converging evidence from animal and human brain studies. Neuropsychologia 41(3):245–251. doi:10.1016/S0028-3932(02)00157-4
Remillard G (2014) The study of sequence learning in individuals with schizophrenia: a critical review of the literature. J Neuropsychol 8:231–245. doi:10.1111/jnp.12022
Seger CA (1994) Implicit learning. Psychol Bull 115(2):163–196. doi:10.1037/0033-2909.115.2.163
Siegert RJ, Weatherall M, Bell EM (2008) Is implicit sequence learning impaired in schizophrenia? A meta-analysis. Brain Cogn 67(3):351–359. doi:10.1016/j.bandc.2008.02.005
Smith CD, Walton A, Loveland AD, Umberger GH, Kryscio RJ, Gash DM (2005) Memories that last in old age: motor skill learning and memory preservation. Neurobiol Aging 26(6):883–890. doi:10.1016/j.neurobiolaging.2004.08.014
Tang BCW, Lanigan CM, Dean B, Sutcliffe JG, Thomas EA (2009) Normal human aging and early-stage schizophrenia share common molecular profiles. Aging Cell 8(3):339–342. doi:10.1111/j.1474-9726.2009.00468.x
Van Tilborg IADA, Hulstijn W (2010) Implicit motor learning in patients with Parkinson’s and Alzheimer’s disease: differences in learning abilities? Mot Control 14:344–361
Van Tilborg IADA, Kessels RPC, Kruijt P, Wester AJ, Hulstijn W (2011) Spatial and nonspatial implicit motor learning in Korsakoff’s amnesia: evidence for selective deficits. Exp Brain Res 214(3):427–435. doi:10.1007/s00221-011-2841-6
Verneau M, van der Kamp J, Savelsbergh GJP, de Looze MP (2014) Age and time effects on implicit and explicit learning. Exp Aging Res 40(4):477–511. doi:10.1080/0361073X.2014.926778
Acknowledgments
The authors would like to thank Ms. Apers and Ms. Laureys for their support in the testing of the study participants. The authors also thank the study participants, without whom the study would never have been accomplished. This clinical trial was funded by Janssen Research & Development, a division of Janssen Pharmaceutica N.V., Beerse, Belgium. Co-authors P. de Boer, L. Janssens and M. Timmers are employees of Janssen Research and Development, A Division of Janssen Pharmaceutica N.V., Beerse, Belgium, and own shares in the company.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cornelis, C., De Picker, L.J., De Boer, P. et al. Implicit motor sequence learning in schizophrenia and in old age: reduced performance only in the third session. Exp Brain Res 234, 3531–3542 (2016). https://doi.org/10.1007/s00221-016-4751-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-016-4751-0