
Abstract
Afferent somatosensory information is modulated before the afferent input arrives at the primary somatosensory cortex during voluntary movement. The aim of the present study was to clarify the effect of muscular contraction strength on somatosensory evoked fields (SEFs) during voluntary movement. In addition, we examined the differences in gating between innervated and non-innervated muscle during contraction. We investigated the changes in gating effect by muscular contraction strength and innervated and non-innervated muscles in human using 306-channel magnetoencephalography. SEFs were recorded following the right median nerve stimulation in a resting condition and during isometric muscular contractions from 10 % electromyographic activity (EMG), 20 and 30 % EMG of the right extensor indicis muscle and abductor pollicis brevis muscle. Our results showed that the equivalent current dipole (ECD) strength for P35m decreased with increasing strength of muscular contraction of the right abductor pollicis brevis muscle. However, changes were observed only at 30 % EMG contraction level of the right extensor indicis muscle, which was not innervated by the median nerve. There were no significant changes in the peak latencies and ECD locations of each component in all conditions. The ECD strength did not differ significantly for N20m and P60m regardless of the strength of muscular contraction and innervation. Therefore, we suggest that the gating of SEF waveforms following peripheral nerve stimulation was affected by the strength of muscular contraction and innervation of the contracting muscle.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Somatosensory information is processed in various ways at different stages of movement in humans. Many studies have reported that somatosensory evoked potentials (SEPs) are attenuated during voluntary movement compared with a resting state (Kirimoto et al. 2014; Nakata et al. 2003; Ogata et al. 2009; Wasaka et al. 2005). In rat and monkey studies, the excitability of pyramidal cells in the primary somatosensory area (S1) was attenuated during voluntary movement of limbs; therefore, it was suggested that afferent somatosensory information is modulated before the afferent input arrives at the S1 during voluntary movement (Courtemanche et al. 1997; Fanselow and Nicolelis 1999).
In somatosensory evoked magnetic fields (SEFs) studies in humans, N20m and P35m deflections of SEFs were attenuated by electrical stimulation of the peripheral nerve during voluntary movement compared with those during the resting condition, as detected by magnetoencephalography (MEG) as well as SEP studies (Huttunen and Lauronen 2012; Kakigi et al. 1995; Kida et al. 2006; Schnitzler et al. 1995; Wasaka et al. 2003). SEF deflections after stimulation of the median nerve consist of three main components, the N20m, the P35m, and the P60m deflection. Previous studies have reported that N20m deflection reflects excitatory postsynaptic potentials (EPSPs) in the pyramidal neurons of Brodmann’s area 3b, and P35m deflections reflect inhibitory postsynaptic potentials (IPSPs) in 3b or the activation of area 4 (Huttunen et al. 2001; Kawamura et al. 1996; Sugawara et al. 2014; Wikström et al. 1996). The response of S1 neurons to cutaneous stimulus in monkeys was modulated during movement compared with that to only an air-puff stimulus (Courtemanche et al. 1997). Jiang et al. (1990a) reported that higher intensities of intracortical microstimulation (ICMS) in area 4 decreased the response of the S1 in awake monkeys. Therefore, we predicted that changes in the strength of voluntary movement altered the processing of somatosensory information in the S1 in humans also.
Previous studies have demonstrated that the amplitude of P35m deflection decreases during or prior to voluntary movement; this is known as gating (Huttunen and Lauronen 2012; Kida et al. 2006). N20m deflections are the first SEF waveform deflections, and Kakigi et al. (1995) reported the attenuation of N20m deflections following median nerve stimulation during movement of four fingers. Conversely, Huttunen and Lauronen (2012) reported attenuated P35m deflections during ipsilateral median nerve stimulation in a continuous finger opposition task compared with resting conditions, whereas no difference was observed in N20m deflections. Forss and Jousmaki (1998) investigated the effects of muscular contraction on SEF gating and reported that the deflection of P35m decreased during isometric contraction of the thenar muscle. Although there was a consensus that P35m deflections were attenuated during or prior to voluntary movement compared with those during a resting condition (Huttunen and Lauronen 2012; Kida et al. 2006; Wasaka et al. 2003), there is still a degree of controversy among previous studies in terms of N20m deflections. This may be explained by differences in the manner and strength of muscle contractions used among these studies. P60m deflections observed from 50 to 100 ms after peripheral stimulation reflect activation within areas 1 and 2 (Huttunen et al. 2006; Sugawara et al. 2014). However, there are few reports of P60m deflection gating in middle-latency SEFs.
The aim of the present study was to clarify the effect of muscular contraction strength on SEFs during voluntary movement. In addition, we examined the differences in gating between innervated and non-innervated muscle during contraction. Many studies have reported that N20m is unchanged during voluntary movement (Huttunen and Lauronen 2012; Kida et al. 2006; Kristeva-Feige et al. 1996a). Wasaka et al. (2003) reported gating of P35m deflections prior to voluntary movement, indicating that SMA activity participates in the attenuation of P35m. Therefore, we predicted that N20m deflections would be unchanged similar to those observed in previous studies and P35m deflections would be attenuated in proportion to the increase in strength of muscular contractions because the activity of the movement-related cortical area (including the M1 and SMA) increases according to muscular strength, according to functional magnetic resonance imaging (fMRI) studies (Dai et al. 2001; Post et al. 2009). In addition, we predicted that SEFs are selectively attenuated and that gating occurs in innervated but not non-innervated areas, as demonstrated previously (Cohen and Starr 1987; Kristeva-Feige et al. 1996a; Nishihira et al. 1997).
Materials and methods
Participants
Twelve healthy volunteers (age range 21–27 years; mean ± standard deviation (SD), 22.9 ± 2.2 years; 11 right-handed and one left-handed) participated in this study. None of the participants had engaged in recreational drug use or used medications affecting the central nervous system. All participants provided written informed consent. The study conformed to the Declaration of Helsinki and the Code of Ethics of the World Medical Association and was approved by the ethics committee of Niigata University of Health and Welfare.
Experimental procedures
Voluntary movement task
We used isometric contraction of the right extensor indicis muscle and the right abductor pollicis brevis muscle as voluntary movement tasks. We measured the 100 % electromyographic activity (EMG) of the right extensor indicis muscle and abductor pollicis brevis muscle of all participants and calculated the 10, 20, and 30 % EMG of each participant before MEG measurements. The muscular contraction strength was adjusted using an elastic band for each participant. The right forearm was placed comfortably on a table, with the elbow joint flexed at 70°–80° in the pronated position, with fingers and thumbs flexed naturally (Sugawara et al. 2013a, b). We observed that fingers did not move together with the right index finger in all participants. Contraction strengths of the right extensor indicis muscle from 10 to 30 % EMG were adjusted using a plastic band fixed to the proximal phalange (Fig. 1a). When the contraction of the right abductor pollicis brevis muscle was recorded, the forearm was in the supinated position, with all fingers relaxed. Contraction strengths of the right abductor pollicis brevis muscle from 10 to 30 % EMG were adjusted using a plastic band fixed to the proximal phalanx of the thumb (Fig. 1b). Participants performed a total of eight trials (rest, 10, 20, and 30 % EMG for the right extensor indicis muscle innervated by the radial nerve and the right abductor pollicis brevis muscle innervated by the median nerve), and muscular contraction was performed for 5 s, separated by 5 s of rest to avoid fatigue in each trial. We measured SEF during a contraction condition with a finger in a trial, and all trials were conducted in a pseudorandom order on the same day. By measuring and observing EMG, we monitored whether participants could resume the isometric contraction strength after rest in a trial during MEG measurements. SEF was measured by stimulating the median nerve during muscular contractions and resting. To minimize the influence of fatigue, each condition was performed after 5 min of rest. Participants were required to extend the index finger and abduct the thumb of the right hand approximately 4 cm above the horizontal surface and keep this point of extension (Fig. 1a, b). SEFs were successively recorded in the rest and muscle contraction conditions in a pseudorandom order on the same day. The peak latencies, equivalent current dipole (ECD) locations, and ECD strengths for the N20m, P35m, and P60m SEF deflections were measured, and comparisons were made between resting and muscular contractions (10, 20, and 30 % EMG). Each component of the SEFs was used as a baseline measure during resting.

Appearance during contraction of the right extensor indicis muscle (a) and the right abductor pollicis brevis muscle (b). Fixation of plastic band to the proximal phalange of the right index finger and fixation of the plastic band to the proximal phalanx of the thumb
EMG recordings
When we measured EMG of the right extensor indicis muscle and abductor pollicis brevis muscle of all participants and calculated the 10, 20, and 30 % EMG of each participant before MEG measurements, the EMG was measured using a pair of Ag/AgCl electrodes (Blue-sensor NF-00; Ambu, Denmark) mounted over the right extensor indicis muscle and abductor pollicis brevis muscle to detect any voluntary movements. EMG signals (DL-140; 4 assist, Japan) were sampled at 1000 Hz (Power Lab; AD Instruments, CO) and band-pass filtered at 0.5–500 Hz. When we measured EMG as MEG recordings, Ag/AgCl disk electrodes with a paste were mounted in a bipolar arrangement over the right extensor indicis muscle and abductor pollicis brevis muscle at a distance of 2 cm.
SEF recordings
SEFs were recorded following electrical stimulation of the right median nerve stimulated at the wrist with randomized inter-stimulus intervals from 0.5 to 1.5 s and an electrical pulse width of 0.2 ms (NeuropackΣ; Nihon Kohden, Japan). Stimulation intensity was fixed at the motor threshold and was monitored throughout the experiment. The motor thresholds were decided for each test of the right extensor indicis muscle and the right abductor pollicis brevis muscle. The mean intensity for the SEF during muscular contraction of the right extensor indicis muscle was 5.3 ± 1.9 mA (mean ± SD) (range 3.3–10 mA) and 5.0 ± 2.0 mA (2.1–10 mA) with contraction of the abductor pollicis brevis muscle. Since previous studies reported that SEP changes differ by the phase of isometric contraction and during articular movement (Gantchev et al. 1994; Rushton et al. 1981), we stimulated median nerves 1 s after the onset of isometric contraction.
Data acquisition
Neuromagnetic signals were recorded using a 306-channel whole-head MEG system (Vectorview; Elekta, Helsinki, Finland). This 306-channel device contains 102 identical triple sensors, each housing two orthogonal planar gradiometers and one magnetometer. This configuration of gradiometers specifically detects the signal just above the source current. Continuous MEG signals were sampled at 1000 Hz using a band-pass filter ranging between 0.03 and 330 Hz. The participants were comfortably seated inside a magnetically shielded room (Tokin Ltd., Sendai, Japan). MEG recordings were acquired from 50 ms before to 300 ms after median nerve stimulation to analyze SEFs. An average value from more than 150 recordings (155.0 ± 4.1 recordings) was calculated during each session. Before MEG measurements were made, three anatomical fiducial points (nasion and bilateral preauricular points) and four indicator coil locations (bilateral mastoids and bilateral hairlines superior to temple) on the scalp were digitized using a three-dimensional digitizer (Polhemus, Colchester, VT, USA). We set up to automatically reject MEG artifacts more than 3000 fT/cm during MEG measurements in this study, but few waveforms were observed. All MEG measurements were taken at Nishi-Niigata Chuo National Hospital.
Data analysis
For analysis of SEFs, the band-pass filter was set between 0.5 and 100 Hz. The 20-ms period preceding stimulation was used as the baseline. The ECDs, best describing the measured data, were determined by a least-squares search using subsets of 16–22 channels, including a gradiometer and magnetometer, over the maximum response area for the left hemisphere (Kida et al. 2006; Lin et al. 2000; Sugawara et al. 2014). These calculations resulted in the three-dimensional location, orientations, and strength of the ECDs in a spherical conductor model, and we used source modeling software (Elekta) to estimate the sources. We accepted ECDs corresponding to peak amplitudes from sensor levels and a goodness-of-fit (g) of >90 % for analysis and the ECD strengths which were calculated from each ECDs during each muscular strength or finger movement were expressed as a percentage of the SEF recorded during resting.
All data were expressed as the mean ± standard error of the mean (SE). The muscular contraction strengths (%EMG) were statistically analyzed using one-way repeated-measures analysis of variance (ANOVA), and the latencies for the N20m, P35m, and P60m deflections during resting and muscular contraction were compared using two-way ANOVA with finger movement versus strength of contraction as factors. The ECD locations were compared using three-way ANOVA with finger movement (index finger and thumb) versus strength of contraction (rest, 10, 20, and 30 % EMG) vs. SEF component (N20m, P35m, and P60m) as factors. Post hoc analyses with Bonferroni correction were used for multiple comparisons. The Friedman test with post hoc analysis using the Wilcoxon signed-rank test for N20m, P35m, and P60m ECD strengths was used to test for significant differences between the muscular contraction and finger movement conditions. The statistical significance was set at P < 0.05.
Results
The responses to stimulation of the right median nerve consisted of three main deflections in the left primary sensorimotor cortex: N20m, P35m, and P60m. Clear response deflections were found in all participants. Figure 2a, b presents SEF grand averaged waveforms during each condition (rest, 10, 20, 30 % EMG) of the right extensor indicis muscle and abductor pollicis brevis muscle. We used the largest amplitude for each waveform within the sensors of interest in the SEF over the sensorimotor area and calculated the grand averaged waveforms for all participants. For the present analyses, the source was modelled at the peak latencies of the waveforms.

We used the largest amplitude for each waveform within the sensors of interest in the SEF over the sensorimotor area and calculated the grand averaged waveforms in all participants. a The grand averaged waveforms from a channel showing maximum signals from the left sensorimotor area after stimulation of the right median nerve during contraction of the right extensor indicis muscle. The responses consisted of three deflections peaking at N20m, P35m, and P60m, respectively, after stimulus onset. Dotted line rest. Dashed line 10 % EMG condition. Gray line 20 % EMG condition. Black line 30 % EMG condition. b The grand averaged waveforms from a channel showing maximum signals from the left sensorimotor area after stimulation of the right median nerve during contraction of the abductor pollicis brevis muscle. The responses consisted of three deflections peaking at N20m, P35m, and P60m after stimulus onset. Dotted line rest condition. Dashed line 10 % EMG condition. Gray line 20 % EMG condition. Black line 30 % EMG condition
Table 1 shows the EMG (%) from the right extensor indicis muscle and abductor pollicis brevis muscle during rest, 10, 20, and 30 % EMG. One-way ANOVA showed significant differences between the four conditions for each muscle (extensor indicis muscle, F (3,48) = 442.402, P < 0.001, partial η 2 = 0.976; abductor pollicis brevis muscle, F (3,48) = 584.042, P < 0.001, partial η 2 = 0.982), and post hoc analysis revealed significant differences between all conditions (rest vs. 10 % EMG, P < 0.001; rest vs. 20 % EMG, P < 0.001; rest vs. 30 % EMG, P < 0.001; 10 % EMG vs. 20 % EMG, P < 0.001; 10 % EMG vs. 30 % EMG, P < 0.001; 20 % EMG vs. 30 % EMG, P < 0.001 for the extensor indicis muscle and abductor pollicis brevis muscle).
Table 2 shows the peak latencies of N20m, P35m, and P60m during the four conditions in both muscles. There was no significant main effect of finger movement or strength of isometric contraction for all SEF components (P > 0.05) and also no significant interaction between finger movement and strength of contraction (P > 0.05). These results indicate that finger movement and strength of contraction did not effect on the peak latencies of SEF waveforms.
Table 3 shows the ECD locations of N20m, P35m, and P60m during four conditions in both muscles. There was a significant main effect of all SEF components in the X-axis (medial–lateral), Y-axis (anterior-posterior), and Z-axis (superior-inferior) (X-axis, F (2,264) = 15.038, P < 0.001, partial η 2 = 0.102; Y-axis, F (2,264) = 6.743, P = 0.001, partial η 2 = 0.049; Z-axis, F (2,264) = 3.391, P = 0.033, partial η 2 = 0.025), but there was no significant effect of finger movement (X-axis, F (1,264) = 2.00, P = 0.158, partial η 2 = 0.008; Y-axis, F (1,264) = 0.173, P = 0.678, partial η 2 = 0.001; Z-axis, F (1,264) = 0.582, P = 0.446, partial η 2 = 0.002) or strength of contraction (X-axis, F (3,264) = 0.792, P = 0.499, partial η 2 = 0.009; Y-axis, F (3,264) = 0.342, P = 0.795, partial η 2 = 0.009; Z-axis, F (3,264) = 0.336, P = 0.799, partial η 2 = 0.004). In all ECD locations (X-axis, Y-axis, and Z-axis), there were no significant interactions among finger movement, strength of contraction, and SEF component (finger movement vs. strength of contraction vs. SEF component: X-axis, F (6,264) = 0.067, P = 0.999, partial η 2 = 0.002; Y-axis, F (6,264) = 0.002, P = 1.000, partial η 2 = 0.002; Z-axis, F (6,264) = 0.006, P = 1.000, partial η 2 = 0.002); (strength of contraction vs. finger movement: X-axis, F (3,264) = 0.075, P = 0.974, partial η 2 = 0.001; Y-axis, F (3,264) = 0.278, P = 0.841, partial η 2 = 0.003; Z-axis, F (3,264) = 1.171, P = 0.321, partial η 2 = 0.013); (finger movement vs. SEF component: X-axis, F (2,264) = 0.058, P = 0.943, partial η 2 < 0.001; Y-axis, F (2,264) = 0.026, P = 0.974, partial η 2 < 0.001; Z-axis, F (2,264) = 0.023, P = 0.978, partial η 2 < 0.001); (strength of contraction vs. SEF component: X-axis, F (6,264) = 0.095, P = 0.997, partial η 2 = 0.002; Y-axis, F (6,264) = 0.018, P = 1.000, partial η 2 < 0.001; Z-axis, F (6,264) = 0.022, P = 1.000, partial η 2 < 0.001).
Concerning the SEF component, the mean ECD locations for P35m were significantly more medial than N20m and P60m in the X-axis (P35m vs. N20m, P < 0.001, r = 0.94; P35m vs. P60m, P = 0.029, r = 0.94), and the mean ECD location for P60m was significantly more medial than N20m (P = 0.011, r = 0.94). Although the mean ECD locations for P35m were significantly more anterior than P60m in the Y-axis (P = 0.001, r = 0.88), there were no significant differences between P35 and N20m, and P60m and N20m (P35m vs. N20m, P = 0.210, r = 0.88; P60m vs. N20m, P = 0.178, r = 0.88). In the Z-axis, the mean ECD location for P35m was significantly more superior than N20m (P35m vs. N20m, P = 0.045, r = 0.79), but there were no significant differences between P35 and P60m (P = 0.796, r = 0.79), N20m and P60m (P = 0.084, r = 0.79).
Figure 3 shows the ECD strength of each contraction of the right extensor indicis muscle and abductor pollicis brevis muscle. The Friedman test revealed a significant main effect on P35m (P < 0.001, r = 0.92), but no significant main effects were observed for N20m and P60m (N20m, P = 0.958, r = 0.59; P60m, P = 0.839, r = 0.98). During contraction of the right extensor indicis muscle, the ECD strengths for P35m significantly decreased during 30 % EMG compared with the resting condition (P = 0.021, r = 0.98). The ECD strengths for P35m during 20 and 30 % EMG significantly decreased during contraction of the right abductor pollicis brevis muscle compared with the resting condition (rest vs. 30 % EMG, P = 0.008, r = 0.98; rest vs. 20 % EMG, P = 0.043, r = 0.92).

ECD strengths for N20m, P35m, and P60m with 10, 20, and 30 % EMG compared to resting baseline. The upper panel is a graphical representation during contraction of the extensor indicis muscle, and the lower panel is a graphical representation during contraction of the abductor pollicis brevis muscle. *P < 0.05, **P < 0.01
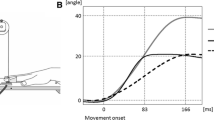
Figure 4 shows the source waveforms at the ECD calculated from the peak latencies of P35m during all conditions calculated from all participants. Strength of only 30 % EMG was observed in the extensor indicis muscle, which was not innervated by the median nerve (Fig. 4a). The ECD strength of P35m during muscular contraction of the abductor pollicis brevis innervated by the median nerve decreased as the contraction strength of the muscle increased (Fig. 4b).

a The source waveforms at the ECD calculated from the peak latencies of P35m during contraction of the abductor pollicis brevis muscle. b The source waveforms at the ECD calculated from the peak latencies of P35m during contraction of the right extensor indicis muscle. Dotted line rest. Dashed line 10 % EMG condition. Gray line 20 % EMG condition. Black line 30 % EMG condition
Discussion
We investigated whether changes in SEF following stimulation of the right median nerve were affected by the strength of muscular contractions and by innervated or non-innervated muscular contraction. Our results showed that the ECD strength for P35m decreased with increasing strength of muscular contraction of the right abductor pollicis brevis muscle. However, changes were observed at only 30 % EMG contraction level in the contraction of the right extensor indicis muscle, which was not innervated by the median nerve. There were no significant changes in the latencies and ECD locations of each component in all conditions. ECD strength did not differ significantly for N20m and P60m regardless of the strength of muscular contraction and innervation.
Gating in voluntary movement is caused by two main factors. One is SEF or SEP gating before and at the onset of contraction. This gating is generated by a central mechanism (centrifugal gating); outputs from movement-related cortical areas such as M1 and the supplementary motor area (SMA) inhibit afferent impulses originating from peripheral nerves that were stimulated at the cortical or subcortical stages. The other factor is gating during voluntary or passive movement, which is due to competition between the input from the presented stimulus and the afferent proprioceptive feedback caused by the movement itself (centripetal gating) (Cheron and Borenstein 1992; Jones et al. 1989; Kakigi and Jones 1985; Kida et al. 2004; Kirimoto et al. 2014; Starr and Cohen 1985). Our results were caused by both centrifugal and centripetal gating mechanisms since we stimulated median nerves during voluntary muscular contraction.
Gantchev et al. (1994) investigated the attenuation of SEP amplitude during muscular contraction and reported that attenuation occurred as muscular force increased (dynamic phases) and not during maintained muscular force (hold contraction phases). The authors suggested that the modulation of SEP differed according to the phase (dynamic or hold contraction) of muscular contraction. In the present study, we stimulated median nerves after 1 s at the onset of voluntary muscular contraction, and we used isometric contraction as a voluntary movement task for investigating the relation between the strength of muscular contraction and gating effects in detail because the gating occurred in prior to movement onset and the gating effect was changed by the change of velocity of movement (Kida et al. 2006; Rauch et al. 1985; Wasaka et al. 2003, 2005).
Many previous studies have reported that the N20m component of SEFs following median nerve stimulation reflects a response in area 3b (Forss et al. 1994; Huttunen et al. 1987, 1992, 2006; Kakigi 1994; Kakigi et al. 2000; Lin et al. 2005) and reported that the amplitude was not attenuated during voluntary movement (Huttunen and Lauronen 2012; Kida et al. 2006; Kristeva-Feige et al. 1996a; Wasaka et al. 2003). However, Gantchev et al. (1994) reported that suppression of the early components was caused by fatigue during muscular contraction. In the present study, fatigue may have been avoided because the duration of isometric contraction was short and rests were taken among contraction tasks. We found that N20m was unchanged by increasing muscular contraction strength, in agreement with previous studies.
The current source for P35m is still debated, but previous studies have reported as a response activation in areas 3b or 4 (Huttunen et al. 2001; Kawamura et al. 1996; Sugawara et al. 2014; Wikström et al. 1996). Previous studies have indicated differential activation of N20m and P35m; the ECD for P35m was located medial to the N20m source (Ishibashi et al. 2000; Lin et al. 2005; Sugawara et al. 2014). These results suggested that N20m, P35m, and P60m reflect differential activation as ECD for P35m was located medial and superior to that for N20m and anterior to that for P60m in all conditions. Our results showed that the ECD strength for P35m was attenuated during 20 and 30 % EMG contractions in the right abductor brevis muscle innervated by the median nerve compared to a resting condition, but N20m and P60m were unchanged. It has been reported that SMA activation or reduced IPSP in area 3b is involved in attenuation of P35m (Huttunen and Lauronen 2012; Wasaka et al. 2003). Several factors have been implicated in the attenuation of P35m in response to increasing strength of isometric contraction in this study. First, an increase in SMA activity in response to the increasing strength of muscular contraction affected IPSP in area 3b, resulting in an attenuation of the ECD strength for P35m. Many studies reported that activation of M1 was not only observed during voluntary movement but also during activation of several cortical areas, including S1 and SMA (Kristeva-Feige et al. 1995, 1996b; Kristeva et al. 1990, 1991; Mima et al. 1999; Onishi et al. 2011, 2013; Sugawara et al. 2013a, b). It has been reported in fMRI studies that SMA activity also increases with the increase in strength of voluntary movement (Dai et al. 2001; Liu et al. 2003; Post et al. 2009; Siemionow et al. 2000). Second, the ECD direction of P35m was countervailed by the increase in activation in area 4 because the ECD direction of P35m was posterior (Sugawara et al. 2014), whereas that of area 4 during voluntary movement was anterior (Onishi et al. 2006), resulting in an attenuation of P35m. Finally, input from Ia afferents may have increased due to the increasing contraction strength of the abductor pollicis brevis muscle (increase in centripetal gating). Afferent input following muscle contraction and proprioceptive feedback during conservation of muscular activity (Harrison and Jankowska 1984; Kirimoto et al. 2014; Rushton et al. 1981) attenuated the ECD strength for P35m because of competition between median nerve stimulation and afferent input as the strength of muscular contraction increased.
Selectivity in gating has been reported (Cohen and Starr 1987; Kristeva-Feige et al. 1996a; Nishihira et al. 1997). Tapia et al. (1987) reported that attenuation of SEP amplitude by median nerve stimulation was accompanied by movement of the thumb but not the little finger, whereas attenuation of SEP amplitude by stimulation of the ulnar nerve stimulation was accompanied by movement of the little finger but not the thumb. A muscular contraction of 30 % EMG (but not 10 and 20 % EMG) significantly attenuated the ECD strength for P35m in the extensor indicis muscle. These results suggest that the attenuation of P35m occurs during contraction of non-innervated muscle, at least when the strength of the muscular contraction is above a certain threshold. It is possible that the attenuation of P35m during isometric contraction of the extensor indicis muscle (which is not innervated by the median nerve) occurred because the ECD direction of P35m was countervailed by that of area 4 as the anterior direction involving in contraction of the extensor indicis muscle. However, gating is caused by several factors (Morita et al. 1998), and the selective mechanism of gating is not known (Nishihira et al. 1997). Our findings cannot fully explain gating in non-innervated muscles. Further investigation is required into the relationship between increased contraction strength and gating in non-innervated domains.
In the present study, the ECD for P60m was located posterior to P35m and medial to N20m and P35m, which was consistent with findings from previous studies (Ishibashi et al. 2000; Sugawara et al. 2014). The current source for P60m is still being debated, but some studies have suggested activation in areas 1/2 or late IPSPs originating from gamma-amino-butyric acid b (GABAb) (Huttunen et al. 2003, 2006; Sugawara et al. 2014). Kristeva-Feige et al. (1996a) reported that the attenuation of SEF amplitude during voluntary movement was observed until 100 ms after median nerve stimulation. However, although we stimulated the median nerve during isometric contraction as muscle activation, changes in the ECD strength for P60m were not observed in this study. It was believed that the findings from the current study did not agree with those of previous studies on P60m since previous studies reported that the effect of gating differed in phase of muscular contraction and contraction manner (Gantchev et al. 1994; Jiang et al. 1990b; Rushton et al. 1981). For these results, isometric contraction did not affect late IPSP or area 1/2 regardless of the innervation or the strength of muscular contraction as the peripheral nerve was stimulated by electric stimulation.
We investigated the effect of isometric muscle contraction strength on the gating of SEF as manners of muscular contraction were different among previous studies investigating gating and there were no studies investigating the relation between gating and the strength of muscular contraction. In the present study, we observed attenuated ECD strength for P35m as the contraction strength of the abductor pollicis brevis (which was innervated by the median nerve) increased. In previous studies investigating selectivity in gating, it has been reported that gating did not occur in non-innervated muscles (Kristeva-Feige et al. 1996a; Tapia et al. 1987) but that strength of only 30 % EMG was found in the extensor indicis muscle, which was not innervated by the median nerve in the present study. The ECD strengths for N20m and P60m were not affected by innervation and the strength of muscular contractions. Therefore, we could clarify that the gating of SEF waveforms following peripheral nerve stimulation was affected by the strength of muscular contraction and by the innervation of the contracting muscle by analyzing ECD strengths and ECD directions obtained from the present study.
References
Cheron G, Borenstein S (1992) Mental movement simulation affects the N30 frontal component of the somatosensory evoked potential. Electroencephalogr Clin Neurophysiol 84:288–292
Cohen LG, Starr A (1987) Localization, timing and specificity of gating of somatosensory evoked potentials during active movement in man. Brain J Neurol 110:451–467
Courtemanche R, Sun GD, Lamarre Y (1997) Movement-related modulation across the receptive field of neurons in the primary somatosensory cortex of the monkey. Brain Res 777:170–178
Dai TH, Liu JZ, Sahgal V, Brown RW, Yue GH (2001) Relationship between muscle output and functional MRI-measured brain activation. Exp Brain Res 140:290–300
Fanselow EE, Nicolelis MA (1999) Behavioral modulation of tactile responses in the rat somatosensory system. J Neurosci Off J Soc Neurosci 19:7603–7616
Forss N, Jousmaki V (1998) Sensorimotor integration in human primary and secondary somatosensory cortices. Brain Res 781:259–267
Forss N, Hari R, Salmelin R, Ahonen A, Hämäläinen M, Kajola M, Knuutila J, Simola J (1994) Activation of the human posterior parietal cortex by median nerve stimulation. Exp Brain Res 99:309–315
Gantchev G, Gavrilenko T, Concek V (1994) Somatosensory evoked potentials modification related to isometric voluntary contraction. Int J Psychophysiol 17:191–196
Harrison PJ, Jankowska E (1984) Do interneurones in lower lumbar segments contribute to the presynaptic depolarization of group I muscle afferents in Clarke’s column? Brain Res 295:203–210
Huttunen J, Lauronen L (2012) Intracortical modulation of somatosensory evoked fields during movement: evidence for selective suppression of postsynaptic inhibition. Brain Res 1459:43–51. doi:10.1016/j.brainres.2012.04.023
Huttunen J, Hari R, Leinonen L (1987) Cerebral magnetic responses to stimulation of ulnar and median nerves. Electroencephalogr Clin Neurophysiol 66:391–400
Huttunen J, Ahlfors S, Hari R (1992) Interaction of afferent impulses in the human primary sensorimotor cortex. Electroencephalogr Clin Neurophysiol 82:176–181
Huttunen J, Jääskeläinen IP, Hirvonen J, Kaakkola S, Ilmoniemi RJ, Pekkonen E (2001) Scopolamine reduces the P35m and P60m deflections of the human somatosensory evoked magnetic fields. NeuroReport 12:619–623
Huttunen J, Kähkönen S, Kaakkola S, Ahveninen J, Pekkonen E (2003) Effects of an acute D2-dopaminergic blockade on the somatosensory cortical responses in healthy humans: evidence from evoked magnetic fields. NeuroReport 14:1609–1612. doi:10.1097/01.wnr.0000085689.46774.53
Huttunen J, Komssi S, Lauronen L (2006) Spatial dynamics of population activities at S1 after median and ulnar nerve stimulation revisited: an MEG study. NeuroImage 32:1024–1031. doi:10.1016/j.neuroimage.2006.04.196
Ishibashi H, Tobimatsu S, Shigeto H, Morioka T, Yamamoto T, Fukui M (2000) Differential interaction of somatosensory inputs in the human primary sensory cortex: a magnetoencephalographic study. Clin Neurophysiol Off J Int Fed Clin Neurophysiol 111:1095–1102
Jiang W, Chapman CE, Lamarre Y (1990a) Modulation of somatosensory evoked responses in the primary somatosensory cortex produced by intracortical microstimulation of the motor cortex in the monkey. Exp Brain Res 80:333–344
Jiang W, Lamarre Y, Chapman CE (1990b) Modulation of cutaneous cortical evoked potentials during isometric and isotonic contractions in the monkey. Brain Res 536:69–78
Jones SJ, Halonen JP, Shawkat F (1989) Centrifugal and centripetal mechanisms involved in the ‘gating’ of cortical SEPs during movement. Electroencephalogr Clin Neurophysiol 74:36–45
Kakigi R (1994) Somatosensory evoked magnetic fields following median nerve stimulation. Neurosci Res 20:165–174
Kakigi R, Jones SJ (1985) Effects on median nerve SEPs of tactile stimulation applied to adjacent and remote areas of the body surface. Electroencephalogr Clin Neurophysiol 62:252–265
Kakigi R, Koyama S, Hoshiyama M, Watanabe S, Shimojo M, Kitamura Y (1995) Gating of somatosensory evoked responses during active finger movements magnetoencephalographic studies. J Neurol Sci 128:195–204
Kakigi R, Hoshiyama M, Shimojo M, Naka D, Yamasaki H, Watanabe S, Xiang J, Maeda K, Lam K, Itomi K, Nakamura A (2000) The somatosensory evoked magnetic fields. Prog Neurobiol 61:495–523
Kawamura T, Nakasato N, Seki K, Kanno A, Fujita S, Fujiwara S, Yoshimoto T (1996) Neuromagnetic evidence of pre- and post-central cortical sources of somatosensory evoked responses. Electroencephalogr Clin Neurophysiol 100:44–50
Kida T, Nishihira Y, Wasaka T, Sakajiri Y, Tazoe T (2004) Differential modulation of the short- and long-latency somatosensory evoked potentials in a forewarned reaction time task. Clin Neurophysiol Off J Int Fed Clin Neurophysiol 115:2223–2230. doi:10.1016/j.clinph.2004.04.017
Kida T, Wasaka T, Inui K, Akatsuka K, Nakata H, Kakigi R (2006) Centrifugal regulation of human cortical responses to a task-relevant somatosensory signal triggering voluntary movement. NeuroImage 32:1355–1364. doi:10.1016/j.neuroimage.2006.05.015
Kirimoto H, Tamaki H, Suzuki M, Matsumoto T, Sugawara K, Kojima S, Onishi H (2014) Sensorimotor modulation differs with load type during constant finger force or position. PLoS one 9:e108058. doi:10.1371/journal.pone.0108058
Kristeva R, Cheyne D, Lang W, Lindinger G, Deecke L (1990) Movement-related potentials accompanying unilateral and bilateral finger movements with different inertial loads. Electroencephalogr Clin Neurophysiol 75:410–418
Kristeva R, Cheyne D, Deecke L (1991) Neuromagnetic fields accompanying unilateral and bilateral voluntary movements: topography and analysis of cortical sources. Electroencephalogr Clin Neurophysiol 81:284–298
Kristeva-Feige R, Rossi S, Pizzella V, Tecchio F, Romani GL, Erne S, Edrich J, Orlacchio A, Rossini PM (1995) Neuromagnetic fields of the brain evoked by voluntary movement and electrical stimulation of the index finger. Brain Res 682:22–28
Kristeva-Feige R, Rossi S, Pizzella V, Lopez L, Erne SN, Edrich J, Rossini PM (1996a) A neuromagnetic study of movement-related somatosensory gating in the human brain. Exp Brain Res 107:504–514
Kristeva-Feige R, Rossi S, Pizzella V, Tecchio F, Romani GL, Edrich J, Rossini PM (1996b) Functional organization of the primary sensory cortex in humans: a neuromagnetic study. Electroencephalogr Clin Neurophysiol Suppl 46:215–220
Lin YY, Simoes C, Forss N, Hari R (2000) Differential effects of muscle contraction from various body parts on neuromagnetic somatosensory responses. NeuroImage 11:334–340. doi:10.1006/nimg.1999.0536
Lin YY, Chen WT, Liao KK, Yeh TC, Wu ZA, Ho LT, Lee LS (2005) Differential generators for N20m and P35m responses to median nerve stimulation. NeuroImage 25:1090–1099. doi:10.1016/j.neuroimage.2004.12.047
Liu JZ, Shan ZY, Zhang LD, Sahgal V, Brown RW, Yue GH (2003) Human brain activation during sustained and intermittent submaximal fatigue muscle contractions: an FMRI study. J Neurophysiol 90:300–312. doi:10.1152/jn.00821.2002
Mima T, Sadato N, Yazawa S, Hanakawa T, Fukuyama H, Yonekura Y, Shibasaki H (1999) Brain structures related to active and passive finger movements in man. Brain J Neurol 122:1989–1997
Morita H, Petersen N, Nielsen J (1998) Gating of somatosensory evoked potentials during voluntary movement of the lower limb in man. Exp Brain Res 120:143–152
Nakata H, Inui K, Wasaka T, Nishihira Y, Kakigi R (2003) Mechanisms of differences in gating effects on short-and long-latency somatosensory evoked potentials relating to movement. Brain Topogr 15:211–222
Nishihira Y, Araki H, Funase K, Imanaka K (1997) Selective modification of somatosensory evoked potential during voluntary finger movement in humans. Percept Mot Skills 85:259–266. doi:10.2466/pms.1997.85.1.259
Ogata K, Okamoto T, Yamasaki T, Shigeto H, Tobimatsu S (2009) Pre-movement gating of somatosensory-evoked potentials by self-initiated movements: the effects of ageing and its implication. Clin Neurophys Off J Int Fed Clin Neurophys 120:1143–1148. doi:10.1016/j.clinph.2009.01.020
Onishi H, Soma T, Kameyama S, Oishi M, Fuijmoto A, Oyama M, Furusawa AA, Kurokawa Y (2006) Cortical neuromagnetic activation accompanying two types of voluntary finger extension. Brain Res 1123:112–118. doi:10.1016/j.brainres.2006.09.033
Onishi H, Oyama M, Soma T, Kirimoto H, Sugawara K, Murakami H, Kameyama S (2011) Muscle-afferent projection to the sensorimotor cortex after voluntary movement and motor-point stimulation: an MEG study. Clin Neurophys Off J Int Fed Clin Neurophys 122:605–610. doi:10.1016/j.clinph.2010.07.027
Onishi H, Sugawara K, Yamashiro K, Sato D, Suzuki M, Kirimoto H, Tamaki H, Murakami H, Kameyama S (2013) Neuromagnetic activation following active and passive finger movements. Brain and behavior 3:178–192. doi:10.1002/brb3.126
Post M, Steens A, Renken R, Maurits NM, Zijdewind I (2009) Voluntary activation and cortical activity during a sustained maximal contraction: an fMRI study. Hum Brain Mapp 30:1014–1027. doi:10.1002/hbm.20562
Rauch R, Angel RW, Boylls CC (1985) Velocity-dependent suppression of somatosensory evoked potentials during movement. Electroencephalogr Clin Neurophysiol 62:421–425
Rushton DN, Rothwell JC, Craggs MD (1981) Gating of somatosensory evoked potentials during different kinds of movement in man. Brain J Neurol 104:465–491
Schnitzler A, Witte OW, Cheyne D, Haid G, Vrba J, Freund HJ (1995) Modulation of somatosensory evoked magnetic fields by sensory and motor interferences. NeuroReport 6:1653–1658
Siemionow V, Yue GH, Ranganathan VK, Liu JZ, Sahgal V (2000) Relationship between motor activity-related cortical potential and voluntary muscle activation. Exp Brain Res 133:303–311
Starr A, Cohen LG (1985) ‘Gating’ of somatosensory evoked potentials begins before the onset of voluntary movement in man. Brain Res 348:183–186
Sugawara K, Onishi H, Yamashiro K, Kirimoto H, Tsubaki A, Suzuki M, Tamaki H, Murakami H, Kameyama S (2013a) Activation of the human premotor cortex during motor preparation in visuomotor tasks. Brain Topogr 26:581–590. doi:10.1007/s10548-013-0299-5
Sugawara K, Onishi H, Yamashiro K, Soma T, Oyama M, Kirimoto H, Tamaki H, Murakami H, Kameyama S (2013b) Repeated practice of a Go/NoGo visuomotor task induces neuroplastic change in the human posterior parietal cortex: an MEG study. Exp Brain Res. doi:10.1007/s00221-013-3461-0
Sugawara K, Onishi H, Yamashiro K, Kojima S, Miyaguchi S, Kirimoto H, Tsubaki A, Tamaki H, Shirozu H, Kameyama S (2014) The effect of anodal transcranial direct current stimulation over the primary motor or somatosensory cortices on somatosensory evoked magnetic fields. Clin Neurophysiol Off J Int Fed Clin Neurophysiol. doi:10.1016/j.clinph.2014.04.014
Tapia MC, Cohen LG, Starr A (1987) Selectivity of attenuation (i.e., gating) of somatosensory potentials during voluntary movement in humans. Electroencephalogr Clin Neurophysiol 68:226–230
Wasaka T, Hoshiyama M, Nakata H, Nishihira Y, Kakigi R (2003) Gating of somatosensory evoked magnetic fields during the preparatory period of self-initiated finger movement. NeuroImage 20:1830–1838
Wasaka T, Nakata H, Kida T, Kakigi R (2005) Gating of SEPs by contraction of the contralateral homologous muscle during the preparatory period of self-initiated plantar flexion. Brain Res Cogn Brain Res 23:354–360. doi:10.1016/j.cogbrainres.2004.11.002
Wikström H, Huttunen J, Korvenoja A, Virtanen J, Salonen O, Aronen H, Ilmoniemi RJ (1996) Effects of interstimulus interval on somatosensory evoked magnetic fields (SEFs): a hypothesis concerning SEF generation at the primary sensorimotor cortex. Electroencephalogr Clin Neurophysiol 100:479–487
Acknowledgments
This study was supported by Grant-in-Aid for Scientific Research (B) 25282162 and 16H03207 from the Japan Society for the Promotion of Science (JSPS).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Sugawara, K., Onishi, H., Yamashiro, K. et al. Effect of muscle contraction strength on gating of somatosensory magnetic fields. Exp Brain Res 234, 3389–3398 (2016). https://doi.org/10.1007/s00221-016-4736-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-016-4736-z