
Abstract
Immunoglobin E (IgE)-related allergy constitutes a high proportion in allergic diseases. The production of specific IgE is key to evoking serial cascades and pathological reactions. Thus, targeting IgE is a different therapeutic approach from symptomatic treatments. Monoclonal antibodies (mAbs) against IgE were developed and a humanized antibody, omalizumab, was approved by five countries. It could inhibit the binding of IgE with epsilon receptor I of crystallizable fragment (FcεRI), thus preventing anaphylactic reactions. However, no bioactivity assay, which is the critical quality attribute and should thoroughly reflect the clinical mechanism, has been established to date. In commercial lot release, only the enzyme-linked immunosorbent assay (ELISA) method was applied, which only reflects the binding of omalizumab to IgE but not the subsequent reaction. In scientific research works, human FcεRI-transfected RBL-2H3 cells were used to indicate degranulation based on the detection of β-hexosaminidase. Nevertheless, this method needs much work to stabilize the response and, hence, is not suitable for routine usage in commercial production and control of antibodies. To evaluate the bioactivity of anti-IgE antibodies including omalizumab using a simple assay that reflects the following mechanism of actions (MOA) after binding, we established an RBL-2H3 cell line transfected with both the α subunit of human FcεRI and nuclear factor-activated T cell (NFAT) response elements, the latter is conjugated with a luciferase gene, which could shed luminescence when substrates exist. The method was proven to possess good specificity, accuracy, linearity, and precision and may be utilized as a supplement to anti-IgE antibody bioactivity assays in terms of development, lot release, stability, and comparability studies.

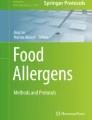
The mechanism sketch of reporter gene assay for bioactivity determination of anti-IgE antibodies by RBL-2H3/FcεRIα/NFAT-Luc cells (left) and representative curves generated by the reporter gene assay (right).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Allergen-specific IgE plays a pivotal role in type I hypersensitivity diseases [1,2,3,5] that affect individuals of all ages, with children accounting for the unneglectable portion of cases [6,6,7,9]. IgE could bind to high affinity receptor FcεRI on effector cells such as mast cells and basophils. Crosslinking of these cell-bound IgE molecules by the corresponding allergen results in the release of pro-inflammatory mediators such as histamine, prostaglandins, leukotrienes, chemokines, and cytokines which then evoke a pathological reaction [1, 10]. Thus, IgE was not only utilized as a diagnostic biomarker but also employed as a potential therapeutic target [3, 11,11,12,14].
Anti-IgE mAbs were developed to target IgE as potent therapeutics. Omalizumab is a recombinant DNA-derived humanized monoclonal antibody that selectively binds to human IgE. Hence, it prevents binding of IgE to the high affinity FcεRI receptor, thereby reducing the amount of free IgE, which triggers the allergic cascade and is proportional to FcεRI expression that could induce the activation of effector cells. Omalizumab was successively approved in Australia, the USA, the European Union, and Japan in 2002, 2003, 2005, and 2009, respectively, for the treatment of moderate to severe persistent asthma. Omalizumab was approved for use in China in 2014. In March of the same year, it was approved in Europe and the USA for adult and adolescent patients with chronic idiopathic urticaria after treatment with histamine H1 antagonists. Studies also demonstrated that omalizumab can be used in allergen-specific immunotherapy to reduce signs of anaphylaxis associated with allergy shots and to accelerate the immunization schedule and dosing [15, 16].
Although there are other treatments to alleviate allergic symptoms, such as inhaled corticosteroids and a β2 agonist for the primary treatment of asthma, the use of β2 agonist could result in side effects such as increased heart rate and headaches. Furthermore, it is not suitable for the treatment of severe asthma. As a treatment with a different mechanism, i.e., interrupting the allergic cascades, omalizumab possesses its own advantages. It can be administrated for moderate to severe persistent asthma and reduce asthma exacerbations, emergency room visits, and use of systemic corticosteroids and bronchodilators, thus improving patients’ quality of life [17,17,18].
In the antibody quality control (QC) system, biological activity is no doubt the most important test because it cannot be proven using other detection methods. An ideal activity method should, first, reflect the mechanism of action (MOA) of the drug; second, be stable enough for lot release; and third, sensitive enough for quality variation. Currently, the main activity assay for omalizumab is enzyme-linked immunosorbent assay (ELISA), which can only indicate the binding of omalizumab and IgE, but not the subsequent effects after binding. A basophilic leukemia cell-based assay was developed to reflect the bioactivity of anti-IgE antibody by detecting the β-hexosaminidase release or other markers after degranulation of cells [19, 20]. This method is highly relevant to the MOA and often used in relevant research. However, it is not suitable for lot release of anti-IgE antibodies owing to its tedious operation procedures and relatively large variation.
Considering the promising development of anti-IgE antibodies and similar biotherapeutic products, a reporter gene assay (RGA) stably indicating the biological activity was developed in this study. Rat basophilic leukemia RBL-2H3 cells were selected as targets because there is no human cell line that naturally expresses enough FcεRI. Αs previously reported, the α subunit of FcεRI plays the fundamental role in IgE binding and signal transduction, indicating that the α subunit is enough for the pathway [19, 21]. In the subsequent signaling, Ca2+ serves as the crosspoint for degranulation and NFAT transcription [22, 23], so the RBL-2H3 cells were stably transfected with FcεRIα and NFAT-RE-luc reporter gene to indicate the biological response of degranulation. Binding of allergic IgE to FcεRI is not sufficient to evoke degranulation, and thus, crosslinking of IgE is required. In vivo, allergens could crosslink with FcεRIα-bound IgE. In view of the poor accessibility of homogeneous allergic IgE and allergen in in vitro assays, a biotin and streptavidin system was introduced. Once IgE-biotin binds to the membrane FcεRIα and is stimulated by streptavidin, signaling is initiated, which includes Ca2+ influx, NFAT promotion, and luciferase gene expression that could be detected by a relative luminescence unit (RLU) after adding the luciferase substrate. When an anti-IgE antibody exists in the system, the response could be inhibited, which reflects the bioactivity of the antibody (Fig. 1b). This assay has satisfactory performance, including high specificity, accuracy, precision, robustness, and stability, and thus may be utilized as a supplement for an anti-IgE bioactivity assay.

The scheme showing the generation of the RBL-2H3/FcεRIα/NFAT-Luc cells and the RGA processes. a The RBL-2H3 cell was sequentially transfected with pcDNA3.1[FcεRIα/G418] and pGL4.30[luc2P/NFAT-RE/Puro]. Transfection of RBL-2H3 with pcDNA3.1[FcεRIα/G418] by Lipofectamine 3000 was followed by the addition of 1 mg/mL of G418 24 h later to select those successfully transfected. Then, limited dilution was applied to screen single clones, and the one with the highest expression was selected. This selected clone was further transfected with pGL4.30[luc2P/NFAT-RE/Puro] by transfection reagent PEI, followed by screening with 1.5 μg/mL puromycin and limited dilution. The clone with intense responses to stimulation of IgE was named RBL-2H3/FcεRIα/NFAT-Luc. b Streptavidin could activate RBL-2H3/FcεRIα/NFAT-Luc after binding of IgE-biotin to human FcεRIα on cell membrane. The binding could be inhibited by anti-IgE mAbs. Following cascades including the signal transduction, Ca2+ influx, NFAT promotion, and luciferase gene expression were hence inhibited. The luminescence signals then decreased when substrate existed, which was in line with the amount of anti-IgE mAbs
Materials and methods
Reagents and cell lines
MEM was purchased from Corning (Corning, NY, USA). Fetal bovine serum (FBS), G418, puromycin, phosphate-buffered saline (PBS), and trypsin were purchased from Gibco (Grand Island, CA, USA). Biotinylated IgE (IgE-biotin) and FITC-labeled IgE (IgE-FITC) were from Shanghai Taiyin Biotechnology Co., Ltd. (Shanghai, China). Two plasmids, namely, pcDNA3.1[FcεRIα/G418] and pGL4.30[luc2P/NFAT-RE/Puro], were constructed by SuZhou Genewiz Biotechnology Co., Ltd. (Suzhou, Jiangsu, China). Lipofectamine 3000 and PEI transfection reagents were from Invitrogen (Carlsbad, CA, USA) and Sigma (St. Louis, MO, USA). Omalizumab was obtained from Novartis (Basel, Switzerland), whereas rituximab, pertuzumab, and tocilizumab were from Roche (Basel, Switzerland). Streptavidin was from Yeasen (Shanghai, China). Bright-Glo Luciferase Assay System was purchased from Promega (Madison, WI, USA). Bovine serum album (BSA) and 4-methylumbelliferyl-N-acetyl-b-d-glucosaminide were purchased from Sigma (St. Louis, MO, USA). NaCl, KCl, NaH2PO4, NaHCO3, MgCl2, CaCl2, glucose, citrate, and glycine were all from Sinopharm Chemical Reagent Co., Ltd. (Shanghai, China).
Generation of the RBL-2H3/FcεRIα/NFAT-Luc cell line
RBL-2H3 cells (ATCC CRL-2256) were sequentially transfected with pcDNA3.1[FcεRIα/G418] and pGL4.30[luc2P/NFAT-RE/Puro]. The streamline can be referred to in Fig. 1a. RBL-2H3 cell clones transfected with pcDNA3.1[FcεRIα/G418] were screened by flow cytometry (see the method below) for the one with the highest expression. RBL-2H3 cell clones transfected with both pcDNA3.1[FcεRIα/G418] and pGL4.30[luc2P/NFAT-RE/Puro] were detected to select the clone with intense luminescence signal (see the method below). The selected clone was named RBL-2H3/FcεRIα/NFAT-Luc and saved for subsequent experiments after culturing in MEM medium with 1 mg/mL G418, 1.5 μg/mL puromycin, and 15% FBS.
Flow cytometry analysis
Cells (1 × 106) were digested with 0.25% trypsin and washed twice with PBS, then cells were resuspended with 200 μL of 2% BSA/PBS containing 10 μg of IgE-FITC and incubated at 4 °C for 1 h. After washing with 2% BSA/PBS for 2 times, the cells were detected by a flow cytometer (BD FACSCalibur).
Selection of RBL-2H3/FcεRIα/NFAT-Luc cell clone
Cells (2 × 105) were seeded in 96-well white plate with 100 μL assay medium (MEM medium with 15% fetal bovine serum) containing 100 ng/mL of IgE-biotin and incubated at 37 °C with 5% CO2 overnight. The cells served as negative control were cultured in assay medium without adding of IgE-biotin. Streptavidin (20 μg/mL, 100 μL each well) was added the next day after discarding the previous liquid. After 3 h of incubation, 100 μL of Bright-Glo Luciferase Assay Reagent was added into each well, and the RLU was recorded with a plate reader (SpectraMax M5).
RGA procedure
RBL-2H3/FcεRIα/NFAT-Luc was seeded into a 96-cell white plate at a density of 1 × 106 cells /mL in 100 μL and incubated at 37 °C with 5% CO2 for 2 h. In the time interval, omalizumab was serially diluted at a 1:4 ratio with the assay medium at an initial concentration of 1000 μg/mL. Then, the diluted omalizumab with 10 gradients was mixed with an equal volume of 400 ng/mL IgE-biotin, which was also diluted with the assay medium. The mixture was incubated at 37 °C with 5% CO2 for 1 h. Then, 100 μL of the mixture was transferred to each well of the 96-cell white plate. The final concentrations of omalizumab were 250.000, 62.500, 15.625, 3.906, 0.977, 0.244, 0.061, 0.015, 0.0038, and 0.001 μg/mL, while the final concentration of IgE-biotin was 100 ng/mL. The plate was incubated at 37 °C with 5% CO2 overnight. The following procedures were the same with those in “Selection of RBL-2H3/FcεRIα/NFAT-Luc cell clone.”
Optimization of RGA
The established RGA was optimized from reagent concentration, dilution ratio, cell number, incubation time, and degranulation time. The optimization of experiment conditions was implemented one by one. When optimizing one condition, other conditions were kept constant.
Validation and application of RGA
The optimized conditions were applied in RGA validation. Specificity of RGA was observed by applying three antibodies targeting moleculars other than IgE in the assay. As to accuracy and linearity, omalizumab was diluted to a final concentration of 1.5, 1.25, 1, 0.75, and 0.5 times of 250 μg/mL, with 250 μg/mL as reference. The expected potencies of the five dilutions were 150, 125, 100, 75, and 50%. All samples were tested 12 times. The agreement of measured potencies and expected potencies represents the accuracy and linearity of the bioassay. In regard to precision, the relative standard derivations (RSDs) of assays at the five levels (150, 125, 100, 75, and 50%) were calculated. For repeatability, the assays performed in 1 day by one analyst was used; for intermediate precision, those finished by two analysts on different days were calculated; for reproducibility, the data from another lab was incorporated. Robustness was observed by slightly altering several conditions from the optimized set points (pre-incubation time, luciferase substrate volume, detection time point). The universality of RGA application was observed by utilizing omalizumab SBP candidates, another source of IgE-biotin and other types of luciferase substrates.
Cell line stability
RBL-2H3/FcεRIα/NFAT-Luc was continuously cultured to passages 9, 18, 30, 40, 45, and 50 and then frozen with culture medium supplemented with 10% DMSO. Then, the cells from different passages were thawed simultaneously and passaged for one generation before bioactivity assay, which was run 3 times to observe the stability of the cell line.
β-Hexosaminidase assay
The RBL-2H3/FcεRIα cell clone with the highest FcεRIα expression (RBL-2H3/FcεRIα-18) was used in the β-hexosaminidase assay. The process of cell seeding, serial dilution of omalizumab, pre-incubation with IgE-biotin, and overnight incubation was the same as the RGA procedure. After that, the liquid in the 96-well plate was discarded and the wells were washed thrice with Tyrode’s solution (140 mM NaCl, 5 mM KCl, 0.64 mM NaH2PO4, 23.8 mM NaHCO3 0.6 mM MgCl2, 1.8 mM CaCl2, 5.5 mM glucose). Then streptavidin was diluted to 20 μg/mL in Tyrode’s solution and was added to the plate with the volume of 100 μL. Besides, 100 μL of 1% Triton X-100 or Tyrode’s solution was added for total degranulation and blank. After incubation at 37 °C with 5% CO2 for 1 h, the activity of β-hexosaminidase was determined by mixing 20 μL of the supernatant with 50 μL of the substrate 4-methylumbelliferyl-N-acetyl-b-d-glucosaminide (0.1 mM in 100 mM citrate, pH 4.5). After incubation at 37 °C for 30 min, 100 μL of glycine (0.02 M, pH 10.7) was added to stop the reaction. The fluorescent value was recorded using an excitation wavelength of 380 nm and an emission wavelength of 440 nm. The data was shown by relative fluorescent units (RFU) in order to compare with RGA.
Generation of heat-treated antibodies
Omalizumab was heated in a water bath of 80 °C for 5 min. The stressed antibody was immediately diluted for the bioactivity assay, which was run 3 times.
Statistical analysis
The inhibition curve was fitted by a four-parameter logistic model, namely, the upper asymptote, lower asymptote, slope, and 50% inhibitive concentration (IC50). The relative potency of a sample was expressed as the IC50 ratio of the reference to the sample. The assay window was represented by the ratio of the upper asymptote to the lower asymptote, named signal-to-noise (S/N) ratio. Analysis was conducted using GraphPad Prism software.
Results
Generation of the RBL-2H3/FcεRIα/NFAT-Luc cell line
RBL-2H3 cells were sequentially transfected with pcDNA3.1[FcεRIα/G418] and pGL4.30[luc2P/NFAT-RE/Puro] for the bioassay of the anti-IgE antibodies. The single transfected and subcloned cell RBL-2H3/FcεRIα was selected by flow cytometry for the highest expression. As shown in Fig. 2a, the four clones expressed FcεRIα with different intensities, whereas clone 18 showed the most intense signals, which was then selected for the subsequent step. After transfection of the second plasmids, the clones were assessed by luminescence response to stimulation of IgE-biotin and streptavidin. The one that exhibited the highest S/N was the final choice for the subsequent experiment, which was designated as RBL-2H3/FcεRIα/NFAT-Luc (Fig. 2b, clone 93). Furthermore, we also demonstrated that the RGA was dependent on the constructed cell line. Figure 2c shows the sole presence of an inhibitory dose–response curve for omalizumab on RBL-2H3/FcεRIα/NFAT-Luc cells but not on RBL-2H3 and RBL-2H3/FcεRIα.

Clone selection of RBL-2H3/FcεRIα/NFAT-Luc cells. RBL-2H3 cells were sequentially transfected with genes of FcεRIα and NFAT-luc. After the transfection of pcDNA3.1[FcεRIα/G418], the clone with the highest expression (RBL-2H3/FcεRIα-18) was screened by flow cytometry (a). The clone was further transfected with pGL4.30[luc2P/NFAT-RE/Puro]. The clones transfected with the two genes were stimulated with IgE-biotin (100 ng/mL) and streptavidin (20 μg/mL) the next day, and the signal-to-noise ratio of luminescence response was recorded as b. Those not stimulated with IgE-biotin were used as negative controls. Each test was repeated thrice. t test was done to compare the difference between the selected clone (clone 93) with other clones. When serial diluted omalizumab exists (250 μg/mL as initial concentration, 1:5 as dilution ratio), only the cell clone of RBL-2H3/FcεRIα/NFAT-Luc (1 × 105/well) showed the inhibition curve after stimulation with IgE-biotin (100 ng/mL) and streptavidin (20 μg/mL), whereas RBL-2H3 and RBL-2H3/FcεRIα were not (c). The points on the curves are average of duplicates with standard derivation (SD). The data in c is a representative of one from three experiments
Optimization of the reagent concentration in the RGA
There are several reagents that affect the assay performance, including the concentration of IgE-biotin, anti-IgE concentration ladder, and cell density.
The function of IgE-biotin in this assay is to occupy the FcεRIα receptor on RBL-2H3/FcεRIα/NFAT-Luc cell, which is the basis for the stimulation of streptavidin. Thus, the more IgE-biotin that was applied, the more intense signals that were obtained, as shown in Fig. 3a. To select a proper concentration of IgE-biotin for anti-IgE antibody inhibition, 90–50% of the maximal effect concentration (EC90 to EC50) of the stimulation curve was observed, i.e., 150, 100, 50, and 25 ng/mL. Under different concentrations of IgE-biotin, serially diluted omalizumab was added, and dose–response curves were all obtained (Fig. 3b). The main difference among these curves was the S/N ratios. As the concentration of IgE-biotin increased, the S/N ratio increased. When 100 ng/mL of IgE-biotin was applied, the S/N ratio was about 10 (Fig. 3c), which could adequately meet the demand of the subsequent assay. To attain a balance between satisfactory S/N ratio and minimizing the use of reagents, 100 ng/mL of IgE-biotin was selected.

Optimization of the reagent concentration in the RGA. A wide concentration range of IgE-biotin (10–6.1 × 10−4 μg/mL) with a dilution ratio of 1:2 was adopted to stimulate RBL-2H3/FcεRIα/NFAT-Luc cell (1 × 105/well) after the addition of streptavidin (20 μg/mL) the next day. The dose–response curve was shown as a. According to the curve, four IgE-biotin concentrations were prepared to be inhibited by serial diluted omalizumab (initial concentration 250 μg/mL, dilution ratio 1:5). The inhibitory curves of omalizumab and S/N ratios under different IgE-biotin concentrations were shown as b and c. A wide concentration range of omalizumab (250–6.92 × 10−6 μg/mL with a dilution ratio of 1:2.5 was applied to obtain the proper concentration range of inhibitory curve (d). Under the concentration range of 250–1.28 × 10−4 μg/mL, four dilution ratios of omalizumab were tried (e). Different numbers of RBL-2H3/FcεRIα/NFAT-Luc cell (f) were seeded and serial diluted omalizumab (initial concentration 250 μg/mL, dilution ratio 1:5) mixed with 100 ng/mL of IgE-biotin was added. After overnight incubation, streptavidin (20 μg/mL) was added to obtain luciferase activity curve. Comparison was done by t test. All of the experiments were tested in triplicate. The points on the curves are average of duplicates with SD
After fixing the concentration of IgE-biotin, the dilution series of omalizumab was developed to obtain a rational distribution of the dots on the inhibition curve, i.e., enough dots on the linear section, with at least two dots on the upper and lower asymptotes. First, a wide range of omalizumab concentrations was implemented to obtain a curve with enough points (Fig. 3d). To ensure the integrity of the curve, 250 μg/mL was set as the first point, and dilution ratios of 1:3, 1:4, 1:5, and 1:6 were then employed (Fig. 3e). Finally, the dilution of 1:4 was selected.
Cell density was another factor that influenced the inhibition curve because it indicated how many FcεRIα receptors were incorporated in the assay. We initially assessed the effects of using cell densities of 2.5 × 104, 5 × 104, 1 × 105, and 2 × 105 cells/well. Figure 3f shows that the densities of 1 × 105 and 2 × 105 cells/well generated comparable curves and S/N ratios, which indicated that under the fixed concentration of IgE-biotin, 1 × 105 cells/well was sufficient.
Optimization of the incubation time in the RGA
The incubation time of IgE-biotin and anti-IgE with cells as well as the stimulation time of streptavidin was also explored. To achieve equal degrees of binding among IgE-biotin, anti-IgE, and the FcεRIα receptor on cells, different incubation times of the three components were explored, namely, 3, 6, 15, 18, 21, and 24 h (Fig. 4a). The S/N ratios could adequately met the demand of experiment window when incubated for 15 h (9.485 ± 0.698) though the S/N ratios increased with elongation of incubation time, and a significant difference was seen in the S/N ratios of 18 and 21 h incubation (Fig. 4b). In order to obtain the results in the next morning no matter the experiment was started in the morning or in the afternoon (according to the cell status) the day before, incubation time of 15–21 h was accepted in view of operational convenience and time effectiveness.

Optimization of incubation time in the RGA. RBL-2H3/FcεRIα/NFAT-Luc cells (1 × 105/well) were seeded and serial diluted omalizumab (initial concentration 250 μg/mL, dilution ratio 1:5) mixed with 100 ng/mL of IgE-biotin was added. After different incubation times (3, 6, 15, 18, 21, 24 h), streptavidin (20 μg/mL) was added and incubated for 3 h to obtain luciferase activity curves. Inhibition curves and corresponding S/N ratios under different incubation times were shown as a and b. Five streptavidin (20 μg/mL) stimulation times (1, 3, 6, 9, 12 h) were tried. Corresponding inhibition curves and S/N ratios were shown as c and d. Comparison was done by t test. All of the experiments were tested in triplicate. The points on the curves are average of duplicates with SD
Stimulation time of streptavidin indicates the crosslinking of IgE-biotin and ensuing signal transduction. An increase followed by a decrease in S/N ratio were observed across the stimulation time span of 1–12 h, which represented the degranulation process, i.e., the RLU signal rapidly increased and peaked in 3 h, then slowly decreased to baseline (Fig. 4c, d). Based on the results, stimulation for 3 h was adopted. Table 1 shows the summary of the parameters derived from the optimization procedure, which was applied to the subsequent experiments. The concentrations listed are the final concentrations when all components were added.
RGA validation including specificity, accuracy, linearity, precision, and robustness
Specificity indicates the ability of an assay to exclusively assess the analyte of interest. As can be seen in Fig. 5a, no dose–response curve of rituximab, pertuzumab, and tocilizumab was shown except omalizumab, indicating the assay only detected the bioactivity of omalizumab as intended, which indicates specificity.

The validation of specificity, accuracy, and linearity of the optimized RGA. Different mAbs were subjected to the RGA and only omalizumab showed dose–response curve (a). Curves in a were repeated twice. The levels of 50, 75, 100, 125, and 150%, that is, the initial concentration of omalizumab was 50, 75, 100, 125, and 150% of the optimized value, were used to detect their bioactivity relative to the optimized curve. Relative bioactivity (average with SD) obtained from IC50 was shown in b. The correlation of expected and measured bioactivity between the range of 50 and 150% was shown in c. Data in b and c were repeated for 12 times
Accuracy, sometimes also termed as trueness, expresses the closeness of agreement between the measured value and the expected true value of an analytical procedure. We implemented the accuracy test within the range of 50–150%. The starting concentrations of omalizumab were 50, 75, 100, 125, and 150% of the optimized first point, while other conditions such as dilution ratio were kept constant. Another omalizumab sample was simultaneously operated by the optimized concentration, which was used as a reference. The samples with five levels were tested by RGA against the reference. Thus, the IC50 values of the five sample levels were expected to be 50, 75, 100, 125, and 150% of those of the reference. The samples were analyzed for 12 replicates, each containing five levels. Figure 5b shows that the means of recovery rates of the five sample levels ranged within 93 to 103%, indicating good agreement between the measured and expected values.
The linear curve between the measured and expected values also showed excellent linearity with R2 of up to 0.9966 (Fig. 5c). The working range of a bioassay was the linearity section of the four-parameter curve, where the IC50 fell on. Although we observed five concentrations in linearity assessment, the range was not limited to 50–150%. From the dose–response curve, we could define the working concentration to range from 0.05 to 1 μg/mL by visual evaluation.
The assay was also investigated in terms of repeatability, intermediate precision, and reproducibility. For repeatability, the RGA was simultaneously performed 6 times under the same operating conditions. For intermediate precision, two operators performed the RGA on different days while each of the operators run 6 times. For reproducibility, the assay was implemented in two laboratories in parallel. Satisfactory precision was achieved for all three aspects. Table 2 shows the summarized validation results, including precision.
Robustness testing evaluates the influence of deliberate variations in procedure-related method parameters. In fact, some major factors were assessed in method optimization, e.g., cell density, dilution ratio, and incubation time. The results have shown acceptable design space other than the defined parameter values that were determined for the sake of comprehensive consideration. We further inspected some other factors that may disturb the assay, including pre-incubation time of IgE-biotin and omalizumab, the volume of luciferase substrate, and the luminescence time before reading. Figure 6a and b show that there were no changes observed between 30 and 60 min pre-incubation or between 90 and 100 μL of the luciferase substrate (Fig. 6c, d). With longer luminescence time, the S/N ratio decreased, although no effect on IC50 was observed (Fig. 6e, f). These assays illustrated that the parameters could be slightly moved from the set points without influencing the results.

Robustness of the RGA. When RBL-2H3/FcεRIα/NFAT-Luc cells (1 × 105/well) were seeded, 30 and 60 min (a) was tried for pre-incubation of serial diluted omalizumab (initial concentration 250 μg/mL, dilution ratio 1:4) with 100 ng/mL of IgE-biotin, corresponding S/N ratios were shown as b. After overnight incubation, streptavidin (20 μg/mL) was added and incubated for 3 h; 90 and 100 μL luciferase substrate (c) was tried to obtain luciferase activity curves and the time intervals of 0, 15, and 30 min (e) were also tried. Corresponding S/N ratios were shown as d and f. The points on the figures are average of duplicates with SD. All of the experiments were tested in triplicate. Comparison was done by t test
Stability of the RBL-2H3/FcεRIα/NFAT-Luc cell line
RBL-2H3/FcεRIα/NFAT-Luc cell line is the key material for the RGA, and it was expected to be stable for a period of time, i.e., the anti-IgE antibody exploring or releasing period. Continuously cultured RBL-2H3/FcεRIα/NFAT-Luc cells were frozen at different passages and thawed at the same time. The cells from different passages were cultured for one generation and then subjected to RGA. Figure 7a shows that the curves derived from six different cell passages exhibited good parallelism. In addition, the S/N ratios of the curves showed an increase followed by a decrease. Nevertheless, the S/N ratio of passage 51 was comparable with that of passage 10 and all the S/N ratios could meet the demand of test window (Fig. 7b). This assay well indicated that the results acquired from RBL-2H3/FcεRIα/NFAT-Luc cells were highly stable even up to passage 51.

Stability of RBL-2H3/FcεRIα/NFAT-Luc cells under different passages. The RBL-2H3/FcεRIα/NFAT-Luc cells at passages 10, 19, 31, 41, 46, and 51 were tested simultaneously by the established RAG (a). Corresponding S/N ratios were shown as b. All the points on the curves are average of replicates with SD. The curves shown are one representative data out of three experiments. Comparison was done by t test
Universality of the RGA
We employed omalizumab as the subject in our assay development and method validation. In addition, two similar biotherapeutic product (SBP) candidates were also subjected to RGA, both of which showed similar fitting curves as omalizumab (Fig. 8a). Besides, the IgE-biotin adopted in this assay was not irreplaceable. The fitting curve was well established even when the source of IgE-biotin was changed (Fig. 8b), despite the fact that it is the key reagent in the assay. Furthermore, four different luciferase substrates were tested. All of these displayed similar fitting curves and IC50, although with differed intensities (Fig. 8c). This section demonstrated the wide applications of the RGA.

Universality of the RGA. The established RGA could detect bioactivity of omalizumab SBP candidates (a). It could also work after changing the source of IgE-biotin (b) and types of luciferase substrates (c). The curves shown are one representative data out of three experiments
Comparison of RGA with the β-hexosaminidase assay
Rituximab, pertuzumab, and tocilizumab were applied in the β-hexosaminidase assay for specificity evaluation. No dose–response curve was seen for the three mAbs except omalizumab (Fig. 9a), which was the same with RGA (Fig. 5a), Furthermore, we performed the β-hexosaminidase assay at the level of 100% and compared its performance to RGA. At the 100% level, the recovery rate of the β-hexosaminidase assay was 82% with RSD of 23%, while RGA was 102% with RSD of 7% (Fig. 9b). The significant difference of recovery rates between the two methods was due to relatively lower accuracy of β-hexosaminidase assay, which also showed much larger variation. Additionally, heat-treated omalizumab (80 °C for 5 min) [24] was also detected by both the β-hexosaminidase assay and RGA. The result (Fig. 9c, d) demonstrated the consistence of the two methods to discriminate the change in the activity of heat-treated omalizumab though the curve of β-hexosaminidase assay showed higher variation. These findings indicate that the β-hexosaminidase assay and RGA generate results with same trends but with differed variation. Table 3 shows the detailed comparison of the two methods.

Comparison of RGA with β-hexosaminidase assay. Different mAbs were subjected to β-hexosaminidase assay and only omalizumab showed a dose–response curve (a). Curves in a were repeated thrice. Independently diluted omalizumab was subjected to both RGA (repeated for 12 times) and β-hexosaminidase assay (repeated for 10 times) with one curve as reference. Average bioactivities with SD were shown as b. Heat-treated omalizumab (80 °C for 5 min) was applied both in RGA and β-hexosaminidase assay (c, d). All the points on the curves are average of replicates with SD. The curves shown are one representative data out of three experiments. Comparison was done by t test
Discussion
Here, we have constructed an RBL-2H3 cell clone stably expressing FcεRIα and harboring the luciferase reporter gene as a basis of an RGA for assessing the bioactivity of anti-IgE antibodies. Previously, RBL-2H3 expressing FcεRIα was already applied in either the supplemental test for allergy or the standardization and batch control of allergen extracts [12, 19, 21], but not in the area of anti-IgE antibody bioactivity control after thorough optimization and validation. Furthermore, tedious procedures were needed to obtain considerable response under the risk of evoking background signals in the assay. NFAT was shown to play an important role in FcεRI crosslinking-induced gene expression in RBL-2H3 cells. Nakamura has taken advantage of this method to evaluate binding between IgE and allergens [25]. However, the specific IgEs used in these studies were pooled sera including IgE. To be universally known, the substances in the sera are extremely complex and may contribute to matrix effects or toxicity to cells. Furthermore, the consistency of sera was another concern because the pooled sera were from different individuals, and the composition was not constant from lot to lot. Thus, we introduced a biotin–streptavidin system instead of a sera–antigen system, which was much more consistent to fit the demand of therapeutic antibody QC.
Taking omalizumab as an example, the RGA was optimized for the concentration of IgE-biotin, serial dilution ladder of omalizumab, and cell density, as well as incubation time and degranulation time. The optimized conditions contributed to a perfect sigmoid curve, which was the solid basis for application. Then, the RGA was validated according to the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH)-Q2 guidelines, including specificity, accuracy, linearity, precision, and robustness. Only the anti-IgE antibody, omalizumab, but not antibodies targeting CD20, HER2, and IL-6R showed dose–response curves. These data indicated that the assay has good specificity. The recovery rates were within the range of 93–103%, while the linearity was up to 0.9966, which showed satisfactory accuracy and linearity. In terms of precision, intermediate precision was controlled within 15%. In addition, the assay was reproducible and stable when some condition variations existed or corresponding reagent substitutes were used. All of the above demonstrated that the RGA could either meet the requirements for therapeutic anti-IgE antibody lot release or stability monitoring.
Apart from omalizumab, we also applied RGA in bioactivity determination for two SBP candidates in stages of clinical trials, both of which showed responses comparable to omalizumab. However, we did not validate other anti-IgE antibodies such as anti-IgE mAb QGE031, which binds to the same IgE site as omalizumab but with higher affinity [26] or a different antibody anti-IgE TNX-901 [27, 28] because these have no approval for distribution in China. We believe that the RGA could also work if the antibody could inhibit the binding of IgE to FcεRI. One point that should be noted was that omalizumab only binds to free IgE, but not FcεRI-bound IgE [29], so there is one step involving pre-incubation of IgE and omalizumab in the working scheme. If anti-IgE antibodies possess significantly higher affinity to IgE than FcεRI to IgE, then the pre-incubation step may not be needed. To further expand the application restrictions of anti-IgE antibodies, the bioactivity of other therapeutic molecules such as anti-FcεRI antibodies, which are proteins that accelerate the dissociation of IgE:FcεRI complexes, may also be controlled using the RGA. One concern that is related to the use of anti-FcεRI antibodies was the crosslinking of FcεRI, and further degranulation may be evoked by the antibody itself, but not the IgE-biotin–streptavidin system. Whether the design of the RGA could work without interference lies on the characteristics of the anti-FcεRI antibody used. Thus, the suitability of the RGA should thus be assessed in every case.
Various allergen screening bioassays are reported and reviewed and might potentially be extended to the bioactivity determination of anti-IgE mAbs [23, 30,31,32,33]. The mechanisms of these assays span from the initial binding between IgE and its receptors and the intermediate signaling to the end of point of degranulation. Binding assays are much less MOA-related, in terms of bioactivity determination of anti-IgE mAbs. Cytosolic Ca2+ influx, as one of the representative signaling events of IgE, is a feasible readout; however, neither real-time fluorescence nor flow cytometric analysis is seldom applied in QC labs. The classical β-hexosaminidase assay is already widely used in the evaluation of degranulation; however, the assay is highly variable, for example, Karen Knipping and colleagues demonstrated the high coefficient of variation up to 50% as for the results of intra- and interlaboratory validation [34], which renders the assay less favorable as the release control of anti-IgE mAbs. Another marker of degranulation is histamine; nevertheless, its half-life is as short as 1 min [31, 35], indicating that it is very unstable which thus restricts its usage. The basophil activation test (BAT) takes advantage of the upregulation of markers on cell surface as an indicator after the cell activation; however, the analytical performance is influenced by many experiment conditions and further validation is needed [36, 37]. Another novel strategy to indicate degranulation is by utilizing granule-labeling fluorescent dye [33]. It is convenient and promising yet needs quantitative correlation study with existing methods.
Biologic therapy in the treatment of IgE-related allergy is a promising field, although there are currently only a limited number of antibodies on the market except omalizumab [4, , 38,39,40]. QC, especially bioactivity evaluation, which is the indication of MOA that is linked to clinical efficacy, is crucial in the evaluation of anti-IgE antibodies because it could not be replaced by any other physiochemical characterization detections. Though there are many newly emerged methods that may possibly be applied in QC of anti-IgE antibodies, some points are still to be addressed. The potential method should be fully validated before application in QC because it is a mandatory requirement. Furthermore, the method should be easy to transfer because testing in laboratories worldwide may be needed in new drug application in different countries, including whether the required instrument is universally used. Additionally, the method should be QC-friendly from the aspect of method management. Under the global background, a serial of RGAs have been developed with compliance to these requirements [41,42,43,44]. As to the RGA here, NFAT-controlled luciferase was selected because its expression is highly dependent on and reliably indicative of Ca2+ influx, which represents the MOA of cell activation. The stability of the engineered cell line was demonstrated by comparison of the RGAs with different passages of the cells. The constructed RGA provides a stable and MOA-indicating bioassay that is a choice for anti-IgE antibody development, lot release, and stability assessment, as well as comparability study, which may promote the development of IgE-targeted antibody drugs.
References
Kalesnikoff J, Huber M, Lam V, Damen JE, Zhang J, Siraganian RP, et al. Monomeric IgE stimulates signaling pathways in mast cells that lead to cytokine production and cell survival. Immunity. 2001;14:801–11.
Walker SMM, Phelan K, Lasserson TJ, Walters EH. Anti-IgE for chronic asthma in adults and children. Cochrane Database Syst Rev. 2006;19(2):CD003559. https://doi.org/10.1002/14651858.CD003559.pub3.
Douglass JA, O’Hehir RE. Diagnosis, treatment and prevention of allergic disease: the basics. Med J Aust. 2006;185(4):228–33.
Kawakami T, Blank U. From IgE to omalizumab. J Immunol. 2016;197(11):4187–92.
Oettgen HC. Fifty years later: emerging functions of IgE antibodies in host defense, immune regulation, and allergic diseases. J Allergy Clin Immunol. 2016;137(6):1631–45.
Baena-Cagnani CE. The global burden of asthma and allergic diseases: the challenge for the new century. Curr Allergy Asthma Rep. 2001;1(4):297–8.
Braman SS. The global burden of asthma. Chest. 2006;130(1 Suppl):4S–12S.
Ehteshami-Afshar S, Fitzgerald JM, Doyle-Waters MM, Sadatsafavi M. The global economic burden of asthma and chronic obstructive pulmonary disease. Int J Tuberc Lung Dis. 2016;20(1):11–23.
Cruz AA, Stelmach R, Ponte EV. Asthma prevalence and severity in low-resource communities. Curr Opin Allergy Clin Immunol. 2017;17(3):188–93.
Anto JM, Pinart M, Akdis M, Auffray C, Bachert C, Basagana X, et al. Understanding the complexity of IgE-related phenotypes from childhood to young adulthood: a Mechanisms of the Development of Allergy (MeDALL) seminar. J Allergy Clin Immunol. 2012;129(4):943–54 e4.
Hoffmann A, Vieths S, Haustein D. Biologic allergen assay for in vivo test allergens with an in vitro model of the murine type I reaction. J Allergy Clin Immunol. 1997;99(2):227–32.
Vogel L, Luttkopf D, Hatahet L, Haustein D, Vieths S. Development of a functional in vitro assay as a novel tool for the standardization of allergen extracts in the human system. Allergy. 2005;60(8):1021–8.
Navines-Ferrer A, Serrano-Candelas E, Molina-Molina GJ, Martin M. IgE-related chronic diseases and anti-IgE-based treatments. J Immunol Res. 2016;2016:8163803.
Platts-Mills TAE, Schuyler AJ, Erwin EA, Commins SP, Woodfolk JA. IgE in the diagnosis and treatment of allergic disease. J Allergy Clin Immunol. 2016;137(6):1662–70.
Khodoun MV, Kucuk ZY, Strait RT, Krishnamurthy D, Janek K, Lewkowich I, et al. Rapid polyclonal desensitization with antibodies to IgE and FcepsilonRIalpha. J Allergy Clin Immunol. 2013;131(6):1555–64.
MacGinnitie AJ, Rachid R, Gragg H, Little SV, Lakin P, Cianferoni A, et al. Omalizumab facilitates rapid oral desensitization for peanut allergy. J Allergy Clin Immunol. 2017;139(3):873–81 e8.
Holgate S, Buhl R, Bousquet J, Smith N, Panahloo Z, Jimenez P. The use of omalizumab in the treatment of severe allergic asthma: a clinical experience update. Respir Med. 2009;103(8):1098–113.
D’Amato G, Stanziola A, Sanduzzi A, Liccardi G, Salzillo A, Vitale C, et al. Treating severe allergic asthma with anti-IgE monoclonal antibody (omalizumab): a review. Multidiscip Respir Med. 2014;9(1):23. https://doi.org/10.1186/2049-6958-9-23.
Palmer GW. RBL cells expressing human FcεRI are a sensitive tool for exploring functional IgE-allergen interactions: studies with sera from peanut-sensitive patients. J Immunol Methods. 2003;274(1):37–45.
Hoffmann HJ, Santos AF, Mayorga C, Nopp A, Eberlein B, Ferrer M, et al. The clinical utility of basophil activation testing in diagnosis and monitoring of allergic disease. Allergy. 2015;70(11):1393–405.
Takagi K, Nakamura R, Teshima R, Sawada J. Application of human FcεRI a-chain-transfected RBL-2H3 cells for estimation of active serum IgE. Biol Pharm Bull. 2003;26(2):252–5.
Rice LV, Bax HJ, Russell LJ, Barrett VJ, Walton SE, Deakin AM, et al. Characterization of selective calcium-release activated calcium channel blockers in mast cells and T-cells from human, rat, mouse and guinea-pig preparations. Eur J Pharmacol. 2013;704(1–3):49–57.
Sun R, Yang Y, Ran X, Yang T. Calcium influx of mast cells is inhibited by aptamers targeting the first extracellular domain of Orai1. PLoS One. 2016;11(7):e0158223.
Tomita S, Matsuda A, Nishinami S, Kurita R, Shiraki K. One-step identification of antibody degradation pathways using fluorescence signatures generated by cross-reactive DNA-based arrays. Anal Chem. 2017;89(15):7818–22.
Nakamura R, Uchida Y, Higuchi M, Nakamura R, Tsuge I, Urisu A, et al. A convenient and sensitive allergy test: IgE crosslinking-induced luciferase expression in cultured mast cells. Allergy. 2010;65(10):1266–73.
Gauvreau GM, Arm JP, Boulet LP, Leigh R, Cockcroft DW, Davis BE, et al. Efficacy and safety of multiple doses of QGE031 (ligelizumab) versus omalizumab and placebo in inhibiting allergen-induced early asthmatic responses. J Allergy Clin Immunol. 2016;138(4):1051–9.
Casale TB, Bernstein IL, Busse WW, CF LF, Tinkelman DG, Stoltz RR, et al. Use of an anti-IgE humanized monoclonal antibody in ragweed-induced allergic rhinitis. J Allergy Clin Immunol. 1997;100(1):110–21.
Adelroth E, Rak S, Haahtela T, Aasand G, Rosenhall L, Zetterstrom O, et al. Recombinant humanized mAb-E25, an anti-IgE mAb, in birch pollen-induced seasonal allergic rhinitis. J Allergy Clin Immunol. 2000;106(2):253–9.
Presta L, Shields R, O’Connell L, Lahr S, Porteri J, Goman C, et al. The binding site on human immunoglobulin E for its high affinity receptor. J Biol Chem. 1994;269(42):26368–73.
Larson D, Mitre E. Histamine release and surface CD200R1 staining as sensitive methods for assessing murine mast cell activation. J Immunol Methods. 2012;379(1–2):15–22.
Huang L, Pi J, Wu J, Zhou H, Cai J, Li T, et al. A rapid and sensitive assay based on particle analysis for cell degranulation detection in basophils and mast cells. Pharmacol Res. 2016;111:374–83.
Nyborg AC, Zacco A, Ettinger R, Jack Borrok M, Zhu J, Martin T, et al. Development of an antibody that neutralizes soluble IgE and eliminates IgE expressing B cells. Cell Mol Immunol. 2016;13(3):391–400.
Ho HP, Lau PM, Kwok HC, Wu SY, Gao M, Cheung AK, et al. Allergen screening bioassays: recent developments in lab-on-a-chip and lab-on-a-disc systems. Bioanalysis. 2014;6(14):2005–18.
Knipping K, van Roest M, Kruijssen L, Smits M, Teunis M, Cox L, et al. Intra- and inter-laboratory validation of an innovative huFcepsilonRIalpha-RBL-2H3 degranulation assay for in vitro allergenicity assessment of whey hydrolysates. Toxicol in Vitro. 2016;33:29–34.
Blott EJ, Griffiths GM. Secretory lysosomes. Nat Rev Mol Cell Biol. 2002;3(2):122–31.
Kleine-Tebbe J, Erdmann S, Knol EF, MacGlashan DW Jr, Poulsen LK, Gibbs BF. Diagnostic tests based on human basophils: potentials, pitfalls and perspectives. Int Arch Allergy Immunol. 2006;141(1):79–90.
Chirumbolo S. Basophil activation test in allergy: time for an update? Int Arch Allergy Immunol. 2012;158(2):99–114.
Anna N, Johansson SGO, Adédoyin J, Ankerst J, Palmqvist M, Oman H. After 6 years with Xolair; a 3-year withdrawal follow-up. Allergy. 2010;65(1):56–60.
Holgate ST. New strategies with anti-IgE in allergic diseases. World Allergy Organ J. 2014;7(1):17.
Incorvaia C, Mauro M, Russello M, Formigoni C, Riario-Sforza GG, Ridolo E. Omalizumab, an anti-immunoglobulin E antibody: state of the art. Drug Des Devel Ther. 2014;8:197–207.
Wang L, Yu C, Wang J. Development of reporter gene assays to determine the bioactivity of biopharmaceuticals. Biotechnol Adv. 2019:107466.
Wang L, Xu GL, Gao K, Wilkinson J, Zhang F, Yu L, et al. Development of a robust reporter-based assay for the bioactivity determination of anti-VEGF therapeutic antibodies. J Pharm Biomed Anal. 2016;125:212–8.
Yang Y, Zhou Y, Yu L, Li X, Shi X, Qin X, et al. A novel reporter gene assay for recombinant human erythropoietin (rHuEPO) pharmaceutical products. J Pharm Biomed Anal. 2014;100:316–21.
Yu L, Shi X, Han C, Rao C, Wang J. A rapid reporter assay for recombinant human brain natriuretic peptide (rhBNP) by GloSensor technology. J Pharm Anal. 2018;8(5):297–301.
Funding
This work was supported by the National Science and Technology Major Projects for Major New Drugs Innovation and Development (Grant number: 2018ZX09736-008).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Guo, S., Yu, C., Wang, Y. et al. A robust and stable reporter gene bioassay for anti-IgE antibodies. Anal Bioanal Chem 412, 1901–1914 (2020). https://doi.org/10.1007/s00216-020-02442-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-020-02442-w