
Abstract
It remains an issue to directly quantify trace biologically important carboxyl compounds in body fluids. Herein we propose an innovative method to determine α-lipoic acid, 2-(β-carboxyethyl)-6-hydroxy-2,7,8-trimethylchroman, prostaglandin E2, cholic acid, and chenodeoxycholic acid in saliva. The method consists of two successive steps: fast and direct labeling of the target analytes with N-(3-dimethylaminopropyl)-N′-ethylcarbodiimide followed by ultrahigh-performance liquid chromatography–tandem mass spectrometry analysis. The method exhibited a wide linear range from 2.5 to 2500 pg/mL, with linear coefficients greater than 0.9963 and limits of detection and quantification as low as 0.10 and 0.33 pg/mL, respectively. The method precision was evaluated, with relative standard deviations ranging from 2.12% to 10.63% for intraday assays and from 2.98% to 12.88% for interday assays. The recoveries were measured by our spiking saliva samples with standards at three different levels, and ranged from 72.5% to 98.0%. Real applicability was validated by direct quantification of trace target analytes in human saliva, with simple pretreatment, use of a small sample volume, and a short analysis time.

Sequential steps to extract, label, and determine the ultratrace carboxylic acids in saliva. CDCA chenodeoxycholic acid, γ-CEHC 2-(β-carboxyethyl)-6-hydroxy-2,7,8-trimethylchroman, α-LA α-lipoic acid, PGE2 prostaglandin E2, UHPLC-MS/MS ultrahigh-performance liquid chromatography–tandem mass spectrometry
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In recent years, there has been increasing interest in research into saliva as a biological fluid for the analysis of related diseases because some trace and ultratrace potential biomarkers often appear in saliva. In addition, collection of saliva is noninvasive, painless, and acceptable to patients [1]. Like blood, saliva is a complex fluid, and most of the compounds found in blood are also present in saliva [2, 3]. Thus, saliva is functionally equivalent to serum in reflecting the physiological state of the body. However, although saliva contains diverse components with diagnostic properties, their low concentration compared with those in blood is a serious challenge for analytical chemistry, making salivary diagnostics not clinically practical [4]. The core issue is how to conveniently, quickly, and accurately determine the biologically and clinically important components in very complex saliva samples.
In assays of saliva samples, carboxylic acids (CAs) have been attracting more and more attention. CAs are widely distributed in saliva, and play important roles but function at only trace levels in regulating various physiological and biological functions [5]. For example, prostaglandin E2 (PGE2), an inflammatory mediator, stimulates alveolar resorption, causing the teeth to gradually loosen and eventually fall out [6]. Various methods have been described for the determination of these CAs, such as enzyme-linked immunosorbent assay [7], high-performance liquid chromatography (HPLC) [8, 9], capillary electrophoresis [10], and mass spectrometry (MS), which can also be coupled with gas chromatography or liquid chromatography (LC). LC–MS/MS in multiple reaction monitoring mode is becoming more and more popular because of its high selectivity and sensitivity. Even so, the sensitivity remains insufficient to directly analyze trace and ultratrace CAs in biofluids, especially in the case of negative ion mode electrospray ionization (ESI) [11]. Chemical derivatization has been considered and various approaches have been explored to introduce easily chargeable groups into the molecules of target analytes to increase ionization efficiency and in turn increase detection sensitivity. This has also led to increasing use of regents for labeling CAs; for example, 2-hydrazinopyridine, 2-picolylamine [5], (S)-1-(4,6-dimethoxy-1,3,5-triazin-2-yl)pyrrolidin-3-amine [12], (S)-anabasine [13], and 1-(3-aminopropyl)-3-bromoquinolinium bromide [14]. Unfortunately, they commonly need rigorous conditions and long reaction times [12, 14], and some of them have low recovery [13] and limited sensitivity enhancement [5]. An example is the use of a reaction newly developed by Mochizuki et al. [14] for the analysis of bile acids and free fatty acids in saliva. It takes a long time to prepurify the target analytes and to synthesize the labeling reagents. Higashi et al. [13] simplified the derivation of 2-(β-carboxyethyl)-6-hydroxy-2,7,8-trimethylchroman (γ-CEHC) in human saliva but the recovery rate was lowered to 55%. It is highly desired to have a more convenient, more sensitive, and faster labeling method to perform trace analysis of CAs in very complex saliva samples.
In the past 10 years, our research group has successfully established a sensitive derivatization technique used in the quantitative determination of ultratrace gibberellins [15], which are CAs but are normally found in plants. Our method uses N-(3-dimethylaminopropyl)-N′-ethylcarbodiimide (EDC) to directly label ultratrace gibberellins under mild conditions (avoiding the isomerization of some gibberellins at a high temperature), and is able to analyze the ultratrace gibberellins in only a floral organ of Arabidopsis thaliana. The method is in theory extendable to the determination of target trace or even ultratrace CAs in body fluids such as saliva. To demonstrate this, five CAs—α-lipoic acid (α-LA), γ-CEHC, PGE2, cholic acid, and chenodeoxycholic acid (CDCA)—were selected as target analytes. They are physiologically and biologically important; for example, α-LA is a natural cofactor serving as an acyl carrier in the oxidative decarboxylation of the α-keto acids (pyruvate and α-ketoglutarate) [16,17,18] and an aminomethyl carrier in the glycine-cleavage enzyme system [19, 20] to prevent free radicals in vitro and in vivo attacks [21,22,23,24], whereas γ-CEHC is a major metabolite of γ-tocopherol, and its S enantiomer functions as a potent natriuretic factor [25]; γ-tocopherol is thus often taken as a food supplement in the hope of an antioxidant effect. The target analytes were first labeled with EDC and then analyzed by ultrahigh-performance liquid chromatography (UHPLC)–MS/MS. The data revealed that direct transformation of the original method was not very ideal, with the labeling taking a long time. The labeling reaction was hence reinvestigated on the basis that CAs are more thermostable than gibberellins [15], and the results are worthy of discussion.
Materials and methods
Chemicals and reagents
α-LA, γ-CEHC, PGE2, cholic acid, CDCA, and EDC were purchased from Sigma (St Louis, MO, USA). Formic acid and HPLC grade methanol, ethanol, acetonitrile, and ethyl acetate were from Fisher Scientific (Waltham, MA, USA). Analytical grade hydrochloric acid was obtained from Beijing Chemical Works (Beijing, China). Pure water produced by a Milli-Q Academic system (Millipore, Billerica, MA, USA) was used throughout the study. Stock solutions of the CAs were prepared as 1 mg/mL solutions in methanol, and were stored at -20 °C. The working standard solutions at desired concentrations used in the analysis were prepared by dilution of the stock solutions with methanol. The EDC solutions were prepared freshly by our dissolving EDC powder in ethanol.
UHPLC–ESI-MS/MS analysis
All separation-based assays were performed with an LCMS-8040 instrument and controlled by LabSolutions LCMS version 5.6 (Shimadzu, Kyoto, Japan), which has a UHPLC unit consisting of a CBM-20A system controller, an LC-30AD pump, a DGU-20A5R degasser, a SIL-30AC autosampler, and a CTO-20AC column oven, and is coupled to a triple quadrupole mass spectrometer via an ESI interface.
A sample (10 μL) was injected into a reversed-phase packed column (XR-ODS, 50 mm × 3.0-mm inner diameter, 2.2 μm, Shimadzu) and eluted at a column temperature of 40 °C and a flow rate of 0.3 mL/min with binary solvents of 0.1% formic acid in water (solvent A) and 0.1% formic acid in acetonitrile (solvent B) with a programmed gradient from 99:1 (v/v) solvent A–solvent B to 40:60 (v/v) solvent A–solvent B over 14 min (Table 1). The eluates were sent to the MS unit via ESI to produce positive ion species, and were detected in multiple reaction monitoring mode (see Table S1). The MS parameters for the LCMS-8040 instrument were set as follows: nebulizing gas flow of 3 L/min, drying gas flow of 15 L/min, interface voltage of 4.5 kV, desolvation line temperature of 300 °C, heat block temperature of 450 °C, and collision-induced dissociation gas pressure of 230 kPa. The other parameters were tuned automatically.
Preparation of EDC-labeled CAs
Five microliters (the calibration curves) or 10 μL (the recovery experiments) of CA standard was transferred to a 0.6-mL Eppendorf tube. After this had been dried under a stream of nitrogen gas, 50 μL of 10 mM EDC in ethanol was added, and the mixture was sonicated for 1 min and incubated in a water bath at 70 °C for 15 min for all samples. The resulting solutions were vacuum-dried and redissolved in 50 μL acetonitrile–H2O (1:1, v/v) for UHPLC–ESI-MS/MS analysis.
Collection and pretreatment of saliva samples
The method of collecting saliva samples as previously reported by Higashi et al. [13] was slightly modified. Saliva (approximately 1.5 mL) was collected directly into a 5-mL tube (without a collection device) from healthy volunteers and stored at -20 °C until use. The volunteers ingested no food or beverages and did not stimulate or rinse their mouths in the 30 min before sample collection. They also did not brush their teeth in the 1 h before sample collection to avoid any blood contamination. The saliva samples were centrifuged at 1000g for 10 min before use. Informed consent for saliva analysis was obtained from all individual volunteers. The study was approved by the Ethics Committee of North China University of Science and Technology, and all procedures adhered to the guidelines in the Declaration of Helsinki.
Pretreatment for analysis of γ-CEHC in saliva
A saliva sample (200 μL) was added to acetonitrile (200 μL), and the mixture was sonicated for 1 min and centrifuged at 2000g for 5 min. After the sediment had been retreated with 200 μL acetonitrile, the supernatants were combined, dried to about one-third volume by a N2 gas stream, and extracted with ethyl acetate (200 μL, twice) under ultrasonication (KQ5200DE Kunshan Ultrasonic Instrument Co., Kunshan, China) for 5 min. The ethyl acetate layer was collected and dried for later derivatization. Gentler extraction was also performed with the same procedure except that the ultrasonication was replaced by shaking for 30 min on a shaker (MS 3 digital, IKA-Werke, Staufen, Germany) at 25 °C and 1000 rpm.
Pretreatment for analysis of α-LA, PGE2, cholic acid, and CDCA in saliva
Similarly, a saliva sample (200 μL) was added to 200 μL acetonitrile, and the mixture was sonicated for 1 min. It was centrifuged at 2000g for 5 min, and the sediment was retreated with 200 μL acetonitrile. The supernatants were combined (approximately 600 μL in total) and dried completely under a N2 gas stream. The dried residue was redissolved in 200 μL water at pH 2.5, and extracted twice with ethyl acetate (200 μL each time) under ultrasonication for 5 min. The ethyl acetate layer was collected and dried for later derivatization. The shaking extraction was performed in the same way except for the replacement of ultrasonication by shaking (see the previous section).
Method validation
To establish the calibration curves, ten solutions of CA standards were prepared in a concentration sequence of 0.00, 0.25, 1.25, 2.50, 12.50, 25.0, 125.0, 250.0, 1250.0, and 2500.0 pg/mL, and were subjected to labeling with EDC and analysis by UHPLC–ESI-MS/MS. The linear regression equations were obtained by our plotting the experimental peak area against CA concentration (n = 3). The relative standard deviations (RSDs) for all analytes were determined in three replicates on either 1 day or on three different days (see Table S2). The limit of detection (LOD) and limit of quantification (LOQ) were calculated as the concentration of CA standards corresponding to a signal of 3 and 10 times the baseline noise, respectively, which were theoretical levels and were not tested. The precision of the method was evaluated by our spiking saliva samples with CAs at three levels: 20, 250, and 2000 pg/mL. The intraday variation of peak areas of EDC-labeled CAs was determined by three replicates on 1 day, and the interday variation was determined on three different days. The recovery of each spiked CA and the 95% confidence interval of the RSDs for all recovery experiments was calculated on the basis of the peak areas.
Results and discussion
Reduction of sample pretreatment process
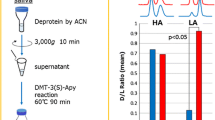
To reduce sample loss, the sample handling steps should be as few as possible on the basis of ensuring the elimination of interfering components. Herein we reduced the sample pretreatment to two steps: to precipitate protein from saliva with acetonitrile and to purify the CAs with ethyl acetate (Fig. 1). All the other steps were removed, such as solid-phase extraction and water cleanup. The two steps were both performed under ultrasonication. The first ultrasonication step is to prevent the inclusion of analytes from precipitating proteins, and the second step aims at speeding up the extraction and increasing the recovery. After this measure, the recovery of α-LA and γ-CEHC increased significantly (n = 3, P < 0.05, t test) from 12.5% to 74.3% and from 15.6% to 81.5%, respectively. It was reported that the recovery rate of γ-CEHC is commonly only around 55% [13]. This is too low to perform quantification. Nevertheless, after ultrasonication the recovery reached the quantification standards. The recoveries of the other target analytes were higher, ranging from 84.2% to 92.8%, with no statistically significant (n = 3, P > 0.05, t test) difference from the shaking extraction (Fig. 2).

Steps for extraction and purification of the target carboxylic acids from saliva samples. CDCA chenodeoxycholic acid, γ-CEHC 2-(β-carboxyethyl)-6-hydroxy-2,7,8-trimethylchroman, α-LA α-lipoic acid, PGE2 prostaglandin E2

Comparison of recovery between shaking extraction and ultrasonic extraction. The data were averaged over three independent analyses at carboxylic acid spiking levels of 20, 250, and 2000 pg/mL, respectively. The data were measured by ultrahigh-performance liquid chromatography–tandem mass spectrometry just after sample pretreatment and N-(3-dimethylaminopropyl)-N′-ethylcarbodiimide labeling. The error bars correspond to the standard deviation (n = 3). CDCA chenodeoxycholic acid, γ-CEHC 2-(β-carboxyethyl)-6-hydroxy-2,7,8-trimethylchroman, α-LA α-lipoic acid, PGE2 prostaglandin E2
Fast labeling of ultratrace CAs
Chemical derivatization is a general method for the analysis of CAs by HPLC–ESI-MS/MS to significantly increase the ionization efficiency. Although various reagents are available to label CAs, our method is convenient to quickly analyze the target analytes. We thus considered a very sensitive chemical labeling approach explored in our laboratory aiming at the quantification of ultratrace plant hormones. That approach used EDC and is able to directly (one manipulation step) label some gibberellins at a concentration as low as 1 pM [15]. On the basis of our previous research, ethanol was used as the reaction solvent to increase the reactivity and lower solvent toxicity. In this case, the mechanism of the reaction is very simple (Fig. 3): The EDC is first protonated and then reacts with monocarboxylic cholic acid to form an unstable O-acylurea intermediate, which subsequently becomes a stable N-acylurea product through O→N migration.

Chemical structure of the analyzed carboxylic acids and their N-(3-dimethylaminopropyl)-N′-ethylcarbodiimide labeling reaction
The preliminary studies revealed that the original protocol was transferable but the labeling took a long time (more than 40 min), much the same as for other reported methods. To reduce the time, the labeling reaction was reinvestigated with the use of five biologically and clinically important CAs as target analytes (Fig. 3). After a systematic inspection, it was found that the reaction temperature impacts seriously on the reaction time. As shown in Fig. 4, on increase of the temperature from 25 to 70 °C, the reaction time at which a plateau was reached was reduced from about 120 min to only 15 min. The final peak intensity (i.e., at the time of reaction saturation) increased with the reaction temperature (e.g., by more than twofold as measured for PGE2; 2.3-fold as shown in Fig. S1). Thus, a high reaction temperature (if allowed but dependent on solvent and analytes) is suggested in the labeling of CAs to increase both the labeling speed and the detection sensitivity. In the analysis of our five target analytes, the temperature was set to 70 °C, somewhat below the boiling point of ethanol of 78 °C, to avoid exorbitant temperature-induced excessive volatilization of reaction solvents.

Peak area versus reaction time at different temperatures (25, 35, 45, 60, and 70 °C) in the labeling of carboxylic acids (1 ng/mL) with 10 mM N-(3-dimethylaminopropyl)-N′-ethylcarbodiimide. CDCA chenodeoxycholic acid, γ-CEHC 2-(β-carboxyethyl)-6-hydroxy-2,7,8-trimethylchroman, α-LA α-lipoic acid, PGE2 prostaglandin E2
Quantification features of the method
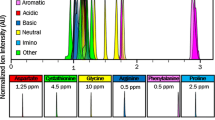
On the basis of the improved labeling approach in combination with UHPLC–ESI-MS/MS, a sensitive method was established and validated to be suitable for quantitative analysis of the target analytes. The calibration curves of the five analytes were plotted over the range from 2.5 to 2500 pg/mL, with linear coefficients greater than 0.9963. The LOQ was calculated to be 0.33–5.58 pg/mL, and the LOD was calculated to be 0.10–1.68 pg/mL (Table 2), which was comparable with the LOD of the enzyme-linked immunosorbent assay method for PGE2 measurement down to picograms per milliliter [7]. Moreover, the LOD was much lower than that of the method of Campos et al. [9] to quantify α-LA by HPLC, with a LOD at the microgram per milliliter level [9], and the LOQ was comparable with the LOQ of 25 pg/mL for detecting CDCA by HPLC–MS/MS with derivatization [26]. The precision of the method was evaluated by the peak area, giving RSDs of 10.63% or lower for intraday assays and 12.88% or lower for interday assays. The recovery measured by the spiking technique was 72.5–98.0% (Table 3), which was higher than the 55% reported for γ-CEHC in [13].
Quantitation of CAs in saliva
The real applicability of the method was validated by measurement of the content of CAs in saliva samples collected from ten healthy volunteers (24–27 years old). The measured content in saliva samples largely differed among the volunteers; for example, the α-LA content in samples from volunteers 3 and 6 was below the LOD but was 266 pg/mL in the sample from volunteer 8 (Table 4). This seems to be dependent on the antioxidant capacity of the volunteers. A similar variation was found for the concentration of γ-CEHC, between 49 and 328 pg/mL (Table 4). These results demonstrate that the new method has enough sensitivity and specificity for practical applications.
Impressive is the content of PGE2, an important inflammatory mediator closely related to periodontitis [6], which was at nearly the same level among the ten volunteers, 35–71 pg/mL (Table 4), much the same as the 73 ± 9 pg/mL reported in the literature [7]. This also suggests that our newly developed method is reliable in practice.
Determination of total bile acids is one of the more accurate and effective liver function tests because they are the most potent ligands for farnesoid X receptor and transcriptionally regulate its biosynthesis and enterohepatic transport [27]. In this validation, cholic acid and CDCA were determined because they are known important biomarkers of many liver diseases (e.g., hepatitis, cirrhosis, and liver cancer) [5, 26]. The data from the same ten volunteers showed that the amounts of cholic acid and CDCA were between 103 and 272 pg/mL and between 142 and 533 pg/mL, respectively (Table 4), consistent with the 53–457 pg/mL for CDCA reported in the literature [26].
Conclusions
To quickly and accurately determine carboxyl compounds of potentially physiological and biological importance, a convenient, fast, and sensitive method was established by innovative transfer of our previously developed EDC-based labeling approach and in combination with UHPLC–MS/MS. The method features high recovery, a fairly wide linear working range, and a low LOD and LOQ, reaching the low picogram per milliliter level. The method was validated to be applicable to the quantification of CA biomarkers such as γ-CEHC, α-LA, PGE2, cholic acid, and CDCA in saliva. The measured data are comparable with data from reported methods [12, 14].
References
Lee Y-H, Wong DT. Saliva: an emerging biofluid for early detection of diseases. Am J Dent. 2009;22(4):241.
Rehak NN, Cecco SA, Csako G. Biochemical composition and electrolyte balance of "unstimulated" whole human saliva. Clin Chem Lab Med. 2000;38(4):335–43.
Zelles T, Purushotham K, Macauley S, Oxford G, Humphreys-Beher M. Concise review: saliva and growth factors: the fountain of youth resides in us all. J Dent Res. 1995;74(12):1826–32.
Miller S. Saliva testing—a nontraditional diagnostic tool. Clin Lab Sci. 1994;7(1):39–44.
Higashi T, Ichikawa T, Inagaki S, Min JZ, Fukushima T, Toyo’oka T. Simple and practical derivatization procedure for enhanced detection of carboxylic acids in liquid chromatography–electrospray ionization-tandem mass spectrometry. J Pharm Biomed Anal. 2010;52(5):809–18.
Page RC. The role of inflammatory mediators in the pathogenesis of periodontal disease. J Periodontal Res. 1991;26(3):230–42.
Sánchez GA, Miozza VA, Delgado A, Busch L. Salivary IL-1β and PGE2 as biomarkers of periodontal status, before and after periodontal treatment. J Clin Periodontol. 2013;40(12):1112–7.
Steijger O, Lingeman H, Brinkman UT, Holthuis J, Smilde A, Doornbos D. Liquid chromatographic analysis of carboxylic acids using N-(4-aminobutyl)-N-ethylisoluminol as chemiluminescent label: determination of ibuprofen in saliva. J Chromatogr B. 1993;615(1):97–110.
Campos PM, Praça FSG, Bentley MVLB. Quantification of lipoic acid from skin samples by HPLC using ultraviolet, electrochemical and evaporative light scattering detectors. J Chromatogr B. 2016;1019:66–71.
Guan Y, Wu T, Ye J. Determination of uric acid and p-aminohippuric acid in human saliva and urine using capillary electrophoresis with electrochemical detection: potential application in fast diagnosis of renal disease. J Chromatogr B. 2005;821(2):229–34.
Deng T, Wu D, Duan C, Yan X, Du Y, Zou J, et al. Spatial profiling of gibberellins in a single leaf based on microscale matrix solid-phase dispersion and precolumn derivatization coupled with ultraperformance liquid chromatography-tandem mass spectrometry. Anal Chem. 2017;89(17):9537–43.
Takayama T, Kuwabara T, Maeda T, Noge I, Kitagawa Y, Inoue K, et al. Profiling of chiral and achiral carboxylic acid metabolomics: synthesis and evaluation of triazine-type chiral derivatization reagents for carboxylic acids by LC-ESI-MS/MS and the application to saliva of healthy volunteers and diabetic patients. Anal Bioanal Chem. 2015;407(3):1003–14.
Higashi T, Kawasaki M, Tadokoro H, Ogawa S, Tsutsui H, Fukushima T, et al. Derivatization of chiral carboxylic acids with (S)-anabasine for increasing detectability and enantiomeric separation in LC/ESI-MS/MS. J Sep Sci. 2012;35(21):2840–6.
Mochizuki Y, Inagaki S, Suzuki M, Min JZ, Inoue K, Todoroki K, et al. A novel derivatization reagent possessing a bromoquinolinium structure for biological carboxylic acids in HPLC-ESI-MS/MS. J Sep Sci. 2013;36(12):1883–9.
Li D, Guo Z, Chen Y. Direct derivatization and quantitation of ultra-trace gibberellins in sub-milligram fresh plant organs. Mol Plant. 2016;9(1):175–7.
Reed LJ. Multienzyme complexes. Acc Chem Res. 1974;7(2):40–6.
Pettit FH, Yeaman SJ, Reed LJ. Purification and characterization of branched chain α-keto acid dehydrogenase complex of bovine kidney. Proc Natl Acad Sci U S A. 1978;75(10):4881–5.
Reed LJ, Hackert ML. Structure-function relationships in dihydrolipoamide acyltransferases. J Biol Chem. 1990;265(16):8971–4.
Kikuchi G, Hiraga K. The mitochondrial glycine cleavage system. Mol Cell Biochem. 1982;45(3):137–49.
Fujiwara K, Okamura K, Motokawa Y. Hydrogen carrier protein from chicken liver: purification, characterization, and role of its prosthetic group, lipoic acid, in the glycine cleavage reaction. Arch Biochem Biophys. 1979;197(2):454–62.
Fuchs J, Milbradt R, Zimmer G. Dihydrolipoate inhibits reactive oxygen species mediated skin inflammation. Free Radic Biol Med. 1990;9:189.
Kagan V, Khan S, Swanson C, Shvedova A, Serbinova E, Packer L. Antioxidant action of thioctic and dihydrolipoic acid. Free Radic Biol Med. 1990;9:15.
Ramakrishnan N, Wolfe WW, Catravas GN. Radioprotection of hematopoietic tissues in mice by lipoic acid. Radiat Res. 1992;130(3):360–5.
Suzuki YJ, Tsuchiya M, Packer L. Thioctic acid and dihydrolipoic acid are novel antioxidants which interact with reactive oxygen species. Free Radic Res Commun. 1991;15(5):255–63.
Murray ED, Wechter WJ, Kantoci D, Wang W-H, Pham T, Quiggle DD, et al. Endogenous natriuretic factors 7: biospecificity of a natriuretic γ-tocopherol metabolite LLU-α. J Pharmacol Exp Ther. 1997;282(2):657–62.
Higashi T, Shibayama Y, Ichikawa T, Ito K, Toyo’oka T, Shimada K, et al. Salivary chenodeoxycholic acid and its glycine-conjugate: their determination method using LC–MS/MS and variation of their concentrations with increased saliva flow rate. Steroids. 2010;75(4):338–45.
Makishima M, Okamoto AY, Repa JJ, Tu H, Learned RM, Luk A, et al. Identification of a nuclear receptor for bile acids. Science. 1999;284(5418):1362–5.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (nos. 21235007, 21727809, and 21621062) and the Chinese Academy of Sciences (QYZDJ-SSW-SLH034).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Informed consent was obtained from all participants who provided saliva samples.
Conflict of interest
The authors declare that they have no competing interests.
Electronic supplementary material
ESM 1
(PDF 522 kb)
Rights and permissions
About this article

Cite this article
Guo, C., Li, D., Liu, C. et al. Facile derivatization of ultratrace carboxylic acids in saliva for quantification by HPLC–MS/MS. Anal Bioanal Chem 410, 4293–4300 (2018). https://doi.org/10.1007/s00216-018-1078-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-018-1078-7