
Abstract
Ultrafast affinity extraction and a two-dimensional high performance affinity chromatographic system were used to measure the free fractions for various drugs in serum and at typical therapeutic concentrations. Pooled samples of normal serum or serum from diabetic patients were utilized in this work. Several drug models (i.e., quinidine, diazepam, gliclazide, tolbutamide, and acetohexamide) were examined that represented a relatively wide range of therapeutic concentrations and affinities for human serum albumin (HSA). The two-dimensional system consisted of an HSA microcolumn for the extraction of a free drug fraction, followed by a larger HSA analytical column for the further separation and measurement of this fraction. Factors that were optimized in this method included the flow rates, column sizes, and column switching times that were employed. The final extraction times used for isolating the free drug fractions were 333–665 ms or less. The dissociation rate constants for several of the drugs with soluble HSA were measured during system optimization, giving results that agreed with reference values. In the final system, free drug fractions in the range of 0.7–9.5 % were measured and gave good agreement with values that were determined by ultrafiltration. Association equilibrium constants or global affinities were also estimated by this approach for the drugs with soluble HSA. The results for the two-dimensional system were obtained in 5–10 min or less and required only 1–5 μL of serum per injection. The same approach could be adapted for work with other drugs and proteins in clinical samples or for biomedical research.

General scheme for the analysis of free drug fractions in serum by ultrafast affinity chromatography and two-dimensional affinity chromatography. The circles represent the drug and the half-circles on the left are serum proteins that can undergo reversible binding with this drug. The rectangles represent (from left-to-right) a guard column, an affinity microcolumn, and an analytical affinity column that are used to isolate and measure the drug's free fraction in serum
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Human serum albumin (HSA) is the most abundant transport protein in blood, with a normal concentration of 30–50 g/L (or 450–750 μM) [1, 2]. This protein can bind to and transport many drugs through reversible interactions. These interactions, in turn, can affect such processes as drug metabolism, absorption, distribution, and excretion [3–5]. For instance, this binding leads to the creation of both a protein-bound fraction for a drug and a free (or non-bound) fraction. The free fraction for many drugs is generally considered to be the active form because it is this form that can cross cell membranes or bind to receptors [2, 3, 5].
These features make the measurement of free drug fractions and the study of drug–protein interactions in serum of interest when characterizing both existing drugs and new drug candidates [5–8]. However, the isolation and measurement of free drug fractions in serum can be difficult due to the many chemicals that are present in such a sample [5, 9–11]. In addition, the free fraction may be only a small part of the total amount of drug that is present. This means it must be possible to measure a relatively small concentration for this fraction in the presence of a much larger concentration of the corresponding protein and protein-bound drug fraction [5–11].
Two common methods that are used to measure free drug fractions are ultrafiltration and equilibrium dialysis [7, 8, 12, 13]. Unfortunately, these methods typically require relatively long separation or analysis times and need moderate-to-large amounts of sample. The adsorption of drugs to the membranes or other system components that are used in these methods also must be considered to avoid introducing errors into the final free fraction values [7, 8, 12, 13]. Many other analytical methods have been employed to study drug–protein interactions [14–29]. Examples are isothermal titration calorimetry, affinity chromatography, X-ray crystallography, surface plasmon resonance (SPR) spectroscopy, capillary electrophoresis, and nuclear magnetic resonance spectroscopy, as well as equilibrium dialysis and ultrafiltration [1, 7, 8, 11–29]. However, many of these techniques employ simple aqueous samples for drug–protein interaction studies and can be difficult to use directly with a complex sample such as serum [18–20, 24]. In addition, techniques such as SPR and traditional affinity chromatography, which make use of immobilized binding agents, need to first be validated when they are employed in studying an interaction that normally occurs in solution [17, 29].
Alternative techniques based on ultrafast affinity extraction have recently been developed to measure free drug fractions and to estimate binding parameters for solution-phase drug–protein interactions [3, 7, 8, 10, 11, 24, 30, 31]. In this approach, the free drug fraction is rapidly extracted from a sample (i.e., in few seconds or less) by using a small affinity column that contains an immobilized binding agent for the drug of interest. This free fraction is then measured directly as it elutes form the affinity microcolumn [3, 10, 24] or indirectly through the use of a method such as an on-line displacement immunoassay [7, 30, 31].
A number of recent applications have been reported for ultrafast affinity extraction. For instance, this method has been used in combination with a chiral separation to analyze the free fractions for the enantiomers of warfarin (i.e., a drug with strong binding to HSA at Sudlow site I) in aqueous solutions and in serum [10]. In addition, affinity microcolumns and ultrafast affinity extraction have been combined with longer affinity columns to measure the free fractions of sulfonylurea drugs in aqueous protein solutions and at therapeutic levels [11]. Ultrafast affinity extraction has also been used to examine the thermodynamics and kinetics of drug–protein interactions in aqueous solutions, through the use of immobilized HSA as a secondary binding agent to separate a free drug from its protein-bound form in these samples [3]. Some general advantages that have been noted for ultrafast affinity extraction in these applications are the ability of this method to provide results in a matter of minutes, its ease of automation, and its need for only a small amount of sample per injection [3, 10, 11].
In this study, ultrafast affinity extraction will be further developed and adapted for use in a two-dimensional high performance affinity system to measure the free fractions for various drugs at therapeutic concentrations in human serum and to directly study drug–protein binding in these biological samples. The samples to be examined will include pooled serum from both normal individuals and diabetic patents. Immobilized HSA will be used as the stationary phase in the affinity columns due to its relatively fast and reversible binding to a large number of drugs with a moderate affinity [1–4, 10, 32], as well as its ability to later elute these drugs under isocratic conditions and at a physiological pH [3, 10, 11]. Several factors will be considered when developing the two-dimensional affinity system. These factors will include the flow rate and column size that are used to isolate the free drug fraction, as well as the conditions that are employed to couple ultrafast affinity extraction with a second affinity column for further separation and measurement of the free fraction [3, 11]. Several model drugs with various binding sites for HSA, as well as a relatively wide range of therapeutic concentrations and affinities for this protein, will be used to evaluate this approach. The results should provide important information on the relative advantages or potential limitations of using ultrafast affinity extraction for measuring free drug fractions and for examining drug–protein binding directly in biological samples. This information should also provide general guidelines that can be used in the future to adapt this technique for work with other drugs, proteins, or samples of interest in clinical chemistry, pharmaceutical science, or biomedical research [1–6].
Experimental
Reagents
The HSA (Cohn fraction V, essentially fatty acid free, ≥96 % pure), human serum (from male AB plasma, H4522, lots 039 K0728 and SLBJ1038V, HSA concentrations of 42 and 33 g/L, glucose concentrations of 4.3 and 5.4 mM; sterile filtered and tested negative for HIV-1/2 and hepatitis B/C), tolbutamide, acetohexamide, gliclazide, diazepam, quinidine, and racemic warfarin were from Sigma-Aldrich (St. Louis, MO, USA). The pooled serum was prepared using de-identified and pre-existing samples from diabetic patients who had HbA1c levels ranging from 8.1 to 12.6 %, with this pooled serum having an HSA content of 44 g/L (provided by W. Clarke, Johns Hopkins University School of Medicine, Baltimore, MD, USA; this work was determined to be exempt from IRB review by the Johns Hopkins School of Medicine, according to the Code of Federal Regulations—45 CFR 46.101 b). Based on their HbA1c levels, the clinical samples that were used to prepare this pooled serum had estimated glycated HSA levels in the range of 21–38 % and glucose concentrations of 10–20 mM [33, 34]. The commercial samples of normal human serum were estimated through a similar approach and from their glucose concentrations to have HbA1c levels of 4–5 % and glycated HSA levels of 6–9 %. All of the serum samples were kept in BSL-2 facilities and handled according to standard procedures for dealing with materials that may contain blood-borne pathogens. The reagents for the bicinchoninic acid (BCA) protein assay were purchased from Pierce (Rockford, IL, USA). The Nucleosil Si-300 silica (300 Å pore size, 7 μm particle diameter) was from Macherey Nagel (Dűren, Germany). All buffers and aqueous solutions were prepared using water from a Milli-Q Advantage A 10 system (EMD Millipore Corporation, Billerica, MA, USA) and were passed through Osmonics 0.22 μm nylon filters from Fisher (Pittsburgh, PA, USA).
Apparatus
A Prep 24 pump from ChromTech (Apple Valley, MN, USA) was used to pack the columns that were used in this study. The chromatographic system included a PU-2080 Plus pump, an AS-2057 autosampler, and a UV-2075 absorbance detector from Jasco (Easton, MD, USA), plus a six-port LabPro valve from Rheodyne (Cotati, CA, USA). This system was controlled by ChromNAV v1.18.04 software and LCNet from Jasco. A CHM column heater and a TCM column heater controller from Waters (Milford, MA, USA) were used to maintain a temperature of 37.0 (±0.1) °C for the columns during all experiments. Chromatograms were analyzed by utilizing PeakFit v4.12 software (Jandel Scientific, San Rafael, CA, USA). A temperature-controlled 5702RH centrifuge from Fisher was used in the ultrafiltration studies, along with Ultracel YM-T cellulose membranes (30 kDa, cutoff) from EMD Millipore.
Column preparation
In the ultrafiltration and ultrafast affinity extraction studies, the support and stationary phase consisted of Nucleosil Si-300 silica that had been converted into a diol-bonded form and used to immobilize HSA by the Schiff base method, as described in ref. [35]. A control support, in which no HSA was added during the immobilization step, was prepared by the same process. The protein content of the final HSA support was determined in quadruplicate through a BCA assay by using HSA as the standard and the control support as the blank [36–40]. This assay gave a content of 59 (±1) mg HSA/g silica.
HSA affinity columns with sizes of 5 × 2.1 mm i.d., 10 × 2.1 mm i.d., 20 mm × 2.1 mm i.d., and 25 mm × 2.1 mm i.d. were packed into standard stainless steel housings using pH 7.4, 0.067 M potassium phosphate buffer as the packing solution. Guard columns with a size of 1 mm × 2.1 mm i.d. were packed in a similar manner with the control support but using a frit-in-column design, as described in ref. [40]. The packing pressure was 3,000 psi (20 MPa) for the 1- and 5-mm-long columns and 4,000 psi (28 MPa) for the 10-, 20-, and 25-mm-long columns. Each of these columns was stored at 4 °C in pH 7.4, 0.067 M phosphate buffer when not in use. The affinity microcolumns that were used for free drug extractions were stable for at least 150 injections, and the longer analytical affinity columns could be used for at least 250 injections. For instance, no significant changes in retention (at the 95 % confidence level) were noted on the HSA microcolumns for injections of racemic warfarin (used as a control) or acetohexamide that were made over the course of 150–200 sample injections and during the free drug fraction measurements. In addition, no significant carryover effects (at the 95 % confidence level) were noted, with only random variations of ±0.35–19 % in the peak areas being seen over the course of four replicate injections for each drug/serum sample that was examined in this study.
Chromatographic studies
The two-dimensional affinity system that was used in this study is illustrated in Fig. 1. A 1 mm × 2.1 mm i.d. guard column was used to protect the HSA microcolumn from particulate matter in the serum samples. The HSA microcolumn was used to extract the free drug fractions. The second, longer HSA column was later placed on-line with the HSA microcolumn to further separate the extracted free drug fraction from other sample components, such as any drug that had dissociated from proteins in the sample during passage through the HSA microcolumn [11]. The wavelengths that were employed for detection were tolbutamide, 227 nm; acetohexamide, 248 nm; diazepam, 230 nm; gliclazide, 226 nm; quinidine, 331 nm; and warfarin, 308 nm. The approximate molar absorptivities at these wavelengths and in pH 7.4, 0.067 M phosphate buffer for the drugs that were used in the free fraction measurements were as follows, in units of L/(mol cm): tolbutamide, 1.5 × 104; acetohexamide, 1.4 × 104; diazepam, 2.6 × 104; gliclazide, 1.4 × 104; and quinidine, 3.5 × 103.

General scheme used for the isolation of a free drug fraction from the drug’s protein-bound form and other components in serum through the use of ultrafast affinity extraction and a two-dimensional affinity system
The mobile phase used for all of these columns was pH 7.4, 0.067 M phosphate buffer. Most of the drugs were dissolved in this buffer to give working stock solutions which contained approximately 8,070 μM tolbutamide, 730 μM gliclazide, 123 μM diazepam, or 480 μM quinidine. These solutions were spiked into the commercial preparations of normal human serum or the pooled serum from diabetic patients. These spiked samples were prepared by dissolving approximately 10 μL of each drug solution into 300 μL of serum. Samples containing only the drug and no protein were prepared in the same manner but by combining the stock solution of the drug with pH 7.4, 0.067 M phosphate buffer instead of serum. The final samples that were made in this manner contained 275 μM tolbutamide, 23 μM gliclazide, 3.5 μM diazepam, or 10 μM quinidine, which were within the typical therapeutic ranges for these agents (i.e., 184–370 μM tolbutamide, 15–31 μM gliclazide, 0.7–7.0 μM diazepam, or 3–15 μM quinidine) [2, 41]. The HSA concentrations in these drug/serum mixtures ranged from 479 to 646 μM and were representative of the normal physiological levels for this protein [2].
An alternative approach was used to make the serum samples that contained acetohexamide. In this case, 1 mg of acetohexamide was dissolved directly in 14.28 mL of human serum, with 268 μL of this spiked mixture then being mixed with 150 μL of the original serum. The concentration of acetohexamide in this final spiked serum sample was 138 μM, which was within the normal therapeutic range for this drug (i.e., 61–216 μM) [41]. The concentration of HSA in the final spiked serum sample was the same as the original content of the serum. Samples containing acetohexamide alone were prepared in the same manner but with this drug being dissolved in and diluted with pH 7.4, 0.067 M phosphate buffer instead of serum.
The flow rates, column sizes, and valve switching times that were used to study the interactions of diazepam or quinidine with HSA were optimized as described in the “Results and discussion” section. The HSA microcolumns that were used in the final system to extract the free drug fractions had the following dimensions: 5 mm × 2.1 mm i.d. for tolbutamide, acetohexamide, and diazepam and 10 mm × 2.1 mm i.d. for gliclazide and quinidine. The flow rates that were employed to inject samples onto these HSA microcolumns were as follows: 2.25 mL/min, tolbutamide; 2.5 mL/min, acetohexamide or gliclazide; and 3.0 mL/min, diazepam or quinidine. The injection volume was 1 μL for tolbutamide, acetohexamide, and gliclazide and 5 μL for quinidine and diazepam.
The size of the second HSA column in the final system was 10 mm × 2.1 mm i.d. for tolbutamide, acetohexamide, and diazepam and 25 mm × 2.1 mm i.d. for gliclazide and quinidine. A six-port valve was used to control the time at which this second column was placed on-line with the first HSA microcolumn. The times for this switching event were 1.2 min after sample injection for tolbutamide, 1.5 min for acetohexamide, 0.6 min for diazepam, 0.7 min for gliclazide, and 0.4 min for quinidine. The flow rate was changed at this same time to 0.50 mL/min for tolbutamide, gliclazide, and quinidine and 0.75 mL/min for acetohexamide and diazepam during the second portion of the separation. The free drug concentration was determined by comparing the resulting peak area to that which was obtained for standards containing only the drug [10]. The free fraction was calculated by dividing the free drug concentration by the total concentration of the drug in the sample [3, 10, 24].
Ultrafiltration studies
Each ultrafiltration tube was washed three times with 1 mL of water, followed by three similar washing steps with pH 7.4, 0.067 M potassium phosphate buffer. The spinning speed and time used in these washing steps were 1,500×g and 5 min. After the last washing step, the buffer in the tube was decanted. The remaining buffer was removed by spinning the ultrafiltration device at 1,500×g for 15 min. One milliliter of a drug or drug/protein sample in pH 7.4, 0.067 M phosphate buffer or in serum and at the same concentrations as used in the chromatographic studies was placed into a washed ultrafiltration tube and spun at 1,500×g and 37 °C. The spinning time for a solution of the drug alone or a drug in serum was 1.5 or 10.0 min, respectively, based on data from previous ultrafiltration studies [10, 11].
The filtrates were injected onto a chromatographic system for measurement of the free drug fraction. The injection volume was 20 μL for the filtrates containing gliclazide, quinidine, or diazepam and 2 μL for the filtrates containing tolbutamide or acetohexamide. The columns used in these measurements contained the same immobilized HSA support as used in the affinity microcolumns but had the following dimensions: quinidine, 20 mm × 2.1 mm i.d.; gliclazide, 10–20 mm × 2.1 mm i.d.; and diazepam, tolbutamide, or acetohexamide, 5 mm × 2.1 mm i.d. Standards containing these drugs in pH 7.4, 0.067 M phosphate buffer were injected under the same conditions. The mobile phase was pH 7.4, 0.067 M phosphate buffer, which was applied at a flow rate of 0.5 mL/min for gliclazide, quinidine, and tolbutamide; 0.25 mL/min for diazepam; or 0.75 mL/min for acetohexamide. The detection wavelengths and system temperature were the same as described earlier for ultrafast affinity extraction. The concentration of the drug in each filtrate was found by comparing the peak areas obtained for both the filtrate samples and standard solutions. The free drug fraction was calculated in the same manner as described for ultrafast affinity extraction.
Results and discussion
Optimization of conditions for ultrafast affinity extraction
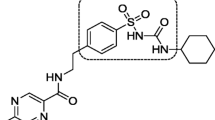
Several drugs with a relatively wide range of binding strengths for HSA and therapeutic concentrations were used as models to investigate the use of ultrafast affinity extraction to measure free drug fractions in serum. The structures of these drugs are given in Fig. 2. Quinidine is an antiarrhythmic drug that binds at Sudlow site II of HSA [1, 22]. Diazepam is a benzodiazepine that is generally believed to have one major binding region on HSA, which is located at Sudlow site II [1, 42]. Tolbutamide, acetohexamide, and gliclazide are sulfonylurea drugs that are used to treat type II diabetes and that interact with HSA at both Sudlow sites I and II [36–39]. These agents have previously reported affinities for HSA that range from 103 to 106 M−1 [1, 3, 11, 20, 42–44] and typical therapeutic concentrations that span from 0.7 to 7.0 μM for diazepam to 184–370 μM for tolbutamide [2, 41]. These features made this group of drugs useful as models for examining the performance of the ultrafast affinity extraction/two-dimensional affinity system as it was used to measure a variety of free fractions and free drug concentrations.

Structures of the model drugs that were examined in this report. The portion within the dashed box represents the core structure of a sulfonylurea drug
The residence time for the sample as it passes through an affinity extraction column is an important factor to consider during the isolation of a free drug fraction from its corresponding drug–protein complex. This time can be adjusted by changing the size of the affinity extraction column or by altering the flow rate [3, 7, 8]. For drugs such as tolbutamide and acetohexamide, which have relatively strong binding to serum proteins (i.e., association equilibrium constants or global affinities of ~105–106 M−1 for soluble HSA), it is known that an HSA microcolumn with a size of 5 mm × 2.1 mm i.d. can be used to extract and isolate their free fractions in aqueous samples [3, 11]. Diazepam has a similar affinity for soluble HSA, with a binding strength of roughly 2–12 × 105 M−1 [20, 43], so the free fraction of this drug was also isolated by using a 5 mm × 2.1 mm i.d. HSA microcolumn. Gliclazide, which has moderately strong binding to soluble HSA (~104–105 M−1), was analyzed by using a longer 10 mm × 2.1 mm i.d. HSA microcolumn. The same type of longer microcolumn was used with quinidine, which has an affinity for soluble HSA in the range of 0.1–5 × 104 M−1 [1, 44].
The effect of the injection flow rate on the measured free drug fractions was also considered. Figure 3 illustrates this effect. The data in this figure were obtained for injections of diazepam and quinidine or mixtures of these drugs with soluble HSA, as made onto 5 or 10 mm × 2.1 mm i.d. HSA microcolumns. It was found that low-to-moderate injection flow rates (i.e., 0.5–2.0 mL/min for diazepam and 0.25–2.50 mL/min for quinidine) resulted in high values for the apparent free drug fractions. However, when the flow rate was raised above 2.5 mL/min for diazepam or above 3.0 mL/min for quinidine, a consistent free drug fraction was obtained. The high values seen at low-to-moderate flow rates were caused by dissociation of these drugs from their complexes with soluble HSA while the samples were passing through the affinity extraction microcolumns [3, 7, 10, 24, 31]. This dissociation was minimized at high flow rates as the sample residence time in the column was decreased, which allowed the original free fraction of the drug to be determined at these higher flow rates. A consistent free fraction was obtained when the sample residence time was less than 333 millisecond (ms) for diazepam and 554 ms for quinidine. The maximum sample residence times that gave similar behavior for the other model drugs during the process of ultrafast affinity extraction were 415 ms for tolbutamide, 333 ms for acetohexamide, and 665 ms for gliclazide [11].

Measurement of free drug fractions at various injection flow rates. These plots were obtained for 1.0 μL injections of (a) 10 μM diazepam or a 10 μM diazepam/20 μM HSA mixture onto a 5 mm × 2.1 mm i.d. HSA microcolumn and (b) 10 μM quinidine or a 10 μM quinidine/20 μM HSA mixture onto a 10 mm × 2.1 mm i.d. HSA microcolumn. These results were measured at 37 °C in pH 7.4, 0.067 M phosphate buffer
These flow rate and residence time data were also used to estimate the dissociation rate constant (k d) for each drug with soluble HSA. This was done by using Eq. (1) and the apparent free drug fractions that were measured at low-to-moderate flow rates [3].
In Eq. (1), F 0 is the original free fraction of the drug in the sample, as is measured at or above a flow rate that provides minimal dissociation of this drug from soluble proteins in the sample during passage through the affinity extraction column. The term F t is the apparent free drug fraction that is measured at a given column residence time t. The value of t is also equal to the column void time, which can be calculated by using the flow rate and column void volume [3].
As is indicated by Eq. (1), a drug–protein system that undergoes essentially first-order dissociation as it passes through the affinity extraction column should provide a linear relationship with an intercept of zero when ln[(1 − F 0) / (1 − F t )] is plotted against t. Figure 4 shows examples of such linear relationships, as were obtained from the affinity extraction experiments that were conducted with quinidine or diazepam in the presence of soluble HSA. These particular plots gave correlation coefficients of 0.990–0.999 (n = 5–6) and intercepts that were equivalent to zero at the 95 % confidence level. Similar behavior has been noted for the other drugs that were considered in this study [3]. The dissociation rate constants for these systems were then determined from the slopes of the best-fit lines for these plots.

Determination of the dissociation rate constants for (a) quinidine and (b) diazepam with soluble HSA by using ultrafast affinity extraction and Eq. (1). The chromatographic conditions were the same as in Fig. 3. The equation for the best-fit lines were (a) y = 0.58 (±0.02) x + 0.01 (±0.03) and (b) y = 0.63 (±0.05) x + 0.02 (±0.05). The correlation coefficients for these plots were 0.990 (n = 5) and 0.999 (n = 6), respectively. The error bars represent a range of ±1 SD (n = 4)
Table 1 shows the dissociation rate constants that were estimated by using Eq. (1) and the ultrafast affinity extraction data. The k d values for quinidine and diazepam with HSA were 0.58 (±0.02) and 0.63 (±0.05) s−1, respectively, which had absolute differences of only 0.05–0.19 s−1 from values in the literature [22, 45]. The relative precisions of these k d values were ±3.4 to 7.9 %. The same approach, with similar relative precisions and agreement with the literature, has previously provided dissociation rate constant estimates of 0.59 (±0.03) s−1 for tolbutamide, 0.67 (±0.03) s−1 for acetohexamide, and 0.61 (±0.02) s−1 for gliclazide [3].
Optimization of conditions for two-dimensional affinity system
When working with a complex matrix such as serum, the large amount of proteins or other sample components that are present may make it difficult to obtain good resolution between the non-retained and retained peaks on an HSA microcolumn at high flow rates, such as those used in the previous section. To avoid this problem, ultrafast affinity extraction was carried out as part of a two-dimensional affinity system [10, 11]. This was achieved by placing a second and longer HSA column on-line after samples had passed through the microcolumn that was used for ultrafast affinity extraction. In this system, part of the free drug fraction that was retained by and later eluted from the affinity microcolumn was delivered to the second column for further separation and analysis. This technique has been shown in prior work to improve the separation of the retained free drug fraction from other sample components, including serum proteins or any protein-bound drug in the sample that had undergone dissociation during its passage through the affinity extraction column [10].
In this two-dimensional method, the time for switching the valve to place the second column on-line with the first is an important factor to consider, as it determines the amount of a drug and its free drug fraction that are transferred to the second column [10, 11]. This time was optimized by using samples that contained only the drug or a mixture of this drug plus soluble proteins, which were each present at typical therapeutic or physiological concentrations. In the case of quinidine, a sample containing 10 μM quinidine in the presence or absence of 600 μM soluble HSA was injected onto a 10 mm × 2.1 mm i.d. HSA column at an initial flow rate of 3.0 mL/min for ultrafast affinity extraction, as optimized in the previous section. The retained drug was then delivered to a 25 mm × 2.1 mm i.d. HSA column at various times after sample injection. Figure 5a provides examples of the retained drug peaks that were transferred to this second column for quinidine when the switching event occurred at 0.30, 0.35, 0.40, or 0.50 min after injection. The flow rate was also decreased to 0.50 mL/min as the second column was placed on-line. It was found in this two-dimensional system that the retained drug gave a peak maximum that occurred at 4.3–5.2 min after sample injection. Diazepam, tolbutamide, acetohexamide, and gliclazide provided similar chromatograms, in which peak maxima were observed at 7.5–7.9, 7.6–8.2, 9.6–10.0, or 7.6–7.8 min, respectively, under the final conditions that are given in the “Experimental” section. This allowed the use of ultrafast affinity extraction with the two-dimensional system to measure the free fractions for these drugs in serum with analysis times of only 5–10 min per injection.

Effect of valve switching time on (a) the recovery of quinidine at 0.5 mL/min on a 25 mm × 2.1 mm i.d. HSA column that was put on-line with a 10 mm × 2.1 mm i.d. HSA microcolumn after various times following the injection of a 5-μL sample of 10 μM quinidine onto the first column at 3.0 mL/min and (b) the apparent free drug fractions that were measured by using the same two-dimensional system and chromatographic conditions as in (a) with a sample that contained 10 μM quinidine and 600 μM HSA. All of the times shown are the elapsed interval after sample injection. The error bars represent a range of ±1 standard error of the mean (n = 4). All of these measurements were made at pH 7.4 and 37 °C
The timing of the switching event was important to consider in that it could create some changes in the apparent free drug fractions that were measured. This effect is illustrated in Fig. 5b for injections that were made onto the two-dimensional system for a sample of 10 μM quinidine or a mixture of this drug with 600 μM HSA. A time for the switching event that was too short caused an overestimation in the free drug fraction, due to contamination of this fraction by dissociation of the original drug–protein complex in the sample. When the time for the switching event was made longer (e.g., at least 0.40 min in Fig. 5), a consistent value in the measured free fraction was obtained. However, this increase in time also created a loss in precision for the measured free fraction as the overall peak area for the transferred drug was decreased. These combined effects led to the use of intermediate times for the switching event that provided both good accuracy and reasonable precisions for the measured free fractions [11]. For quinidine, the final switching time that was employed was 0.40 min. The switching times that were optimized and selected for the other drugs were 0.6 min for diazepam, 1.5 min for acetohexamide, 1.2 min for tolbutamide, and 0.7 min for gliclazide.
Measurement of free fractions and binding of drugs to HSA in serum
The use of ultrafast affinity extraction with the optimized two-dimensional system was next used to measure the free fractions for various drugs that were present at typical therapeutic concentrations in serum from various sources. The results are summarized in Table 2. These free fractions were in the general range of 0.7–9.5 % for all of the drugs and serum samples that were tested. The corresponding free drug concentrations that were measured ranged from 0.02–0.03 μM for diazepam to 6.7–10.8 μM for tolbutamide. The two-dimensional affinity method based on ultrafast affinity extraction gave good absolute precisions for its measured free fractions (±0.07–0.80 %), as well as reasonable relative precisions (±6.2–28 %). The limits of detection for the free drug concentrations in this method, as estimated at a signal-to-noise ratio of three and based on absorbance detection, were as follows: diazepam, 0.006–0.008 μM; quinidine, 0.11–0.16 μM; gliclazide, 0.04–0.19 μM; acetohexamide, 0.05 μM; and tolbutamide, 0.11 μM.
When the results of the system based on ultrafast affinity extraction were compared to those measured by ultrafiltration, an absolute difference of 0.5 % or less was obtained (average difference, 0.08 %). Most of the free fractions obtained by ultrafast affinity extraction were equivalent at the 95 % confidence level to those measured by ultrafiltration. The only exception was the result that was measured for acetohexamide with the sample of normal human serum 1; however, even in this case, the absolute difference in the values was only 0.29 %. Both methods gave similar trends in the free drug fractions when going from one sample to the next. For instance, as the HSA content in the normal serum samples decreased from 42 to 33 g/L, a 1.2- to 1.6-fold increase in the free drug fractions was observed with each of these two methods. Both methods also gave a decrease in the measured free fractions of the three sulfonylurea drugs (i.e., a change of 0.6- to 0.8-fold) when comparing the pooled serum from diabetic patients versus the normal serum sample with a similar HSA content (i.e., normal human serum 1). This latter trend agrees with previous studies which have found that glycation-related modifications on HSA, as occurs in diabetes, can lead to a change in the binding of sulfonylurea drugs with this protein and in the free fractions of these drugs [11, 32].
The free drug fractions that were measured with the two-dimensional affinity system were further used to estimate the binding constants for each drug with HSA in the serum samples. These binding constants were calculated by using Eq. (2), which can be used to provide the association equilibrium constant (K a) for a system with single-site binding or the global affinity constant (nK a ′) for a system with multiple but independent binding sites [3, 10, 24].
In this equation, F 0 is the free fraction for the drug that is measured in the absence of any appreciable drug–protein dissociation in the sample, while [D] and [P] are the concentrations of the drug and soluble protein in the original sample, respectively. For drugs such as diazepam and quinidine, which each have a single major binding site on HSA [1, 22, 42], Eq. (2) can be used to provide the value of K a for these interactions. For tolbutamide, acetohexamide, and gliclazide, which each have two major binding sites on HSA [36–39], Eq. (2) would instead provide an estimate of the global affinity constant for these drug–protein interactions.
Table 3 summarizes the values of K a or nK a ′ that were determined from the free drug fraction measurements. The relative precisions for these binding constants ranged from ±1.3 to 29 %. The values estimated for tolbutamide, acetohexamide, gliclazide, and quinidine and when using the normal serum samples were all consistent with previous binding constants that have been reported for these drugs with normal HSA and at the same temperature and pH [1, 36–39, 44]; these values were also consistent between the two normal serum samples. These particular results differed from the literature values by only 1.2–15.7 % (average difference, 7.2 %) or fell within the range of previously reported values (e.g., in the case of quinidine). The binding constants determined for diazepam with HSA in the two normal serum samples were also equivalent to each other and fell within the range of previous values that have been obtained with normal HSA at the same pH but at room temperature [20, 43]. In addition, all of the binding constants that were measured by ultrafast affinity extraction and the two-dimensional system agreed with the results that were obtained for the same samples of normal serum when using ultrafiltration (i.e., values that differed by 27 % or less, with an average difference of 5.2 %).
Table 3 also shows the global affinity constants that were estimated for the three sulfonylurea drugs when using the pooled clinical sample from diabetic patients. These values were compared to those obtained with the sample of normal human serum 1, which had a similar HSA content to that of the diabetic sample (i.e., 42 versus 44 g/L). It was found that the global affinity constants for the clinical sample increased by 1.4- to 1.6-fold for acetohexamide and gliclazide versus the values that were acquired for normal human serum 1. These differences were significant at the 95 % confidence level. For tolbutamide, going from the sample of normal human serum 1 to the clinical sample also gave an apparent increase of 1.2-fold in the global affinity constant; however, this change was not significant at the 95 % confidence level. These trends were consistent with those seen in previous studies that have been carried out with the same drugs and in vivo samples of glycated HSA, as isolated from diabetic patients [32]. In addition, each of these binding constants showed good agreement with the value that was obtained for the same clinical sample when using ultrafiltration (i.e., results that differed by 11 % or less and that had an average difference of 5.9 %).
Conclusion
This study used ultrafast affinity extraction and a two-dimensional affinity system to measure free drug fractions and to study drug–protein interactions in serum. Several model drugs, which represented a relatively wide range of therapeutic concentrations and affinities for HSA, were used to test and illustrate this approach. Various factors were considered when optimizing this system to measure free drug fractions in serum and at typical therapeutic concentrations. These factors included the flow rates and column sizes that were used for extraction of the free drug fraction and the times at which the affinity extraction column was placed on-line with a larger affinity column for use in further isolating and measuring the retained free fraction.
The free fractions that were estimated for each drug by this approach were in good agreement with the results measured by ultrafiltration. The binding constants that were determined from the same data also agreed with those obtained by ultrafiltration and with literature values. However, the approach based on ultrafast affinity extraction had several advantages over traditional methods for free drug measurements and for drug–protein binding studies. For instance, this method required much smaller sample volumes than ultrafiltration or equilibrium dialysis (i.e., 1–5 μL per injection versus at least 1 mL per analysis) [3, 10, 11, 24]. The use of HSA microcolumns in this method made it possible to examine a variety of drugs and to isolate the free fractions of these drugs in 333–665 ms or less. In addition, the use of these columns in a two-dimensional affinity system provided results within 5–10 min of sample injection. The limits of detection for the free drug concentrations were in the range of 0.006–3.8 μM (i.e., based on absorbance detection), and free fractions in serum could be measured at levels down to at least 0.7 %. It was also shown how these free fractions could be used to examine the binding by drugs with soluble proteins in serum samples.
This report indicated that a two-dimensional affinity system using HSA microcolumns could be used to measure the free fractions of the model drugs in various serum samples. Although this study involved optimization of the system for each drug that was examined, it should be possible in the future to employ the trends that were observed in this study to adapt this approach for use with other drugs or solutes. Examples of other possible candidates for this technique include low mass hormones and fatty acids which can bind to HSA [1, 16, 21]. It should be further possible to develop microcolumns for ultrafast affinity extraction that contain other types of immobilized binding agents (e.g., alpha1-acid glycoprotein), which would allow this approach to be extended to an even greater range of drugs and solutes [4, 32]. These developments, in turn, should continue to increase the flexibility and applications of ultrafast affinity extraction in such areas as clinical testing, pharmaceutical analysis, and biomedical research.
References
Peters T Jr (1996) All about albumin: biochemistry, genetics and medical applications. Academic, San Diego, CA
Burtis CA, Ashwood ER, Bruns DE (2006) Tietz textbook of clinical chemistry and molecular diagnostics. Saunders, St Louis, MO
Zheng X, Li Z, Podariu MI, Hage DS (2014) Anal Chem 86:6454–6460
Hage DS, Jackson A, Sobansky MR, Schiel JE, Yoo MJ, Joseph KS (2009) J Sep Sci 32:835–853
Kwong TC (1985) Clin Chim Acta 151:193–216
Herve F, Urien S, Albengres E, Duche JC, Tillement JP (1994) Clin Pharmacokinet 26:44–58
Clarke W, Schiel JE, Moser A, Hage DS (2005) Anal Chem 77:1859–1866
Clarke W, Chowdhuri AR, Hage DS (2001) Anal Chem 73:2157–2164
Krebs HA (1950) Annu Rev Biochem 19:409–430
Zheng X, Yoo MJ, Hage DS (2013) Analyst 138:6262–6265
Zheng X, Matsuda R, Hage DS (2014) J Chromatogr A 1371:82–89
Melten JW, Wittebrood AJ, Hubb JJ, Faber GH, Wemer J, Faber DB (1985) J Pharm Sci 74:692–694
Musteata FM (2011) Bioanalysis 3:1753–1768
Matsuda R, Bi C, Anguizola J, Sobansky M, Rodriquez E, Badilla JV, Zheng X, Hage B, Hage DS (2014) J Chromatogr B 966:48–58
Vuignier K, Schappler J, Veuthey J, Carrupt P, Martel S (2010) Anal Bioanal Chem 398:53–66
Zheng X, Li Z, Beeram S, Podariu M, Matsuda R, Pfaunmiller EL, White CJ II, Carter N, Hage DS (2014) J Chromatogr B 968:49–63
Rich LR, Day YS, Morton TA, Myszka DG (2001) Anal Biochem 296:197–207
Dings F, Zhao G, Chen S, Liu F, Sun Y, Zhang L (2009) J Mol Struct 929:159–166
Leis D, Barbosa S, Attwood D, Taboada P, Mosquera V (2002) Langmuir 18:8178–8185
Yuan H, Pawliszyn J (2001) Anal Chem 73:4410–4416
Schiel JE, Hage DS (2009) J Sep Sci 32:1507–1522
Yoo MJ, Hage DS (2011) J Chromatogr A 1218:2072–2078
Schiel JE, Hage DS (2009) J Sep Sci 32:1507–1522
Mallik R, Yoo MJ, Briscoe CJ, Hage DS (2010) J Chromatogr A 1217:2796–2803
Ahene AB (2011) Bioanalysis 3:1287–1295
Holm SS, Hansen SH, Faber J, Staun-Olsen P (2004) Clin Biochem 37:85–93
Soldin OP, Soldin SJ (2011) Clin Biochem 44:89–94
Weber PC, Salemme FR (2003) Curr Opin Struct Biol 13:115–121
Zheng X, Bi C, Li Z, Podariu M, Hage DS (2015) J Pharm Biomed Anal. doi:10.1016/j.jpba.2015.01.042
Schiel JE, Tong Z, Sakulthaew C, Hage DS (2011) Anal Chem 83:9384–9390
Ohnmacht CM, Schiel JE, Hage DS (2006) Anal Chem 78:7547–7556
Anguizola J, Joseph KS, Barnaby OS, Matsuda R, Alvarado G, Clarke W, Cerny RL, Hage DS (2013) Anal Chem 85:4453–4460
Lee JW, Kim HJ, Kwon YS, Jun YH, Kim SK, Choi JW, Lee JE (2003) Ann Pediatr Endocrinol Metab 18:208–213
Rohlfing CL, Wiedmeyer HM, Little RR, England JD, Tennill A, Goldstein DE (2002) Diabetes Care 25:275–278
Chen J, Hage DS (2006) Anal Chem 78:2672–2683
Joseph KS, Hage DS (2010) J Chromatogr B 878:1590–1598
Joseph KS, Anguizola J, Jackson AJ, Hage DS (2010) J Chromatogr B 878:2775–2781
Joseph KS, Anguizola J, Hage DS (2011) J Pharm Biomed Anal 54:426–432
Matsuda R, Anguizola J, Joseph KS, Hage DS (2011) Anal Bioanal Chem 401:2811–2819
Schiel JE (2009) Clinical and pharmaceutical applications of high-performance affinity chromatography. Ph.D. dissertation, University of Nebraska, Lincoln, NE
Regenthal R, Krueger M, Koeppel C, Preiss R (1999) J Clin Monit 15:529–544
Kratochwil NA, Huber W, Muller F, Kansy M, Gerber PR (2002) Biochem Pharmacol 64:1355–1374
Wilting J, Hart BJT, De Gier JJ (1980) Biochim Biophys Acta 626:291–298
Ueda CT, Makoid MC (1979) J Pharm Sci 68:448–450
Yoo MJ, Hage DS (2011) J Sep Sci 34:2255–2263
Acknowledgments
This work was supported by the National Institutes of Health under grants R01 GM044931 and R01 DK069629. M. Podariu was supported through a UCARE fellowship from the University of Nebraska-Lincoln. The concept of free fraction analysis by rapid affinity chromatography is the subject of U.S. Patent 6,720,193 (D.S. Hage and W.A. Clarke).
Conflict of interest
The authors declare that they have competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Zheng, X., Podariu, M., Matsuda, R. et al. Analysis of free drug fractions in human serum by ultrafast affinity extraction and two-dimensional affinity chromatography. Anal Bioanal Chem 408, 131–140 (2016). https://doi.org/10.1007/s00216-015-9082-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-015-9082-7