
Abstract
Raman optical activity (ROA) is inherently sensitive to the secondary structure of biomolecules, which makes it a method of interest for finding new approaches to clinical applications based on blood plasma analysis, for instance the diagnostics of several protein-misfolding diseases. Unfortunately, real blood plasma exhibits strong background fluorescence when excited at 532 nm; hence, measuring the ROA spectra appears to be impossible. Therefore, we established a suitable method using a combination of kinetic quenchers, filtering, photobleaching, and a mathematical correction of residual fluorescence. Our method reduced the background fluorescence approximately by 90 %, which allowed speedup for each measurement by an average of 50 %. In addition, the signal-to-noise ratio was significantly increased, while the baseline distortion remained low. We assume that our method is suitable for the investigation of human blood plasma by ROA and may lead to the development of a new tool for clinical diagnostics.

The effect of a newly developed fluorescence quenching method for the ROA measurements of human blood plasma
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chiroptical methods are among the few methods inherently sensitive to the 3D structure of chiral biomolecules [1, 2]. Thus, the sensitivity of chiroptical methods to the structure of chiral molecules is much higher than in the case of conventional Raman and infrared (IR) spectroscopies, as has been many times proved and published in literature [3, 2]. This is most evident, for example, in determining the absolute configuration of small molecules [3, 4], in assessing the enantiomeric excess in pharmaceuticals [5–7], and in the spectra of biomolecules such as peptides, proteins, nucleic acids, carbohydrates, and even more complicated structures such as membranes, protein fibrils, viruses, and bacteria [3, 2]. Compared to conventional methods, the main disadvantages of chiroptical spectroscopy (especially of vibrational optical activity) are a more complex theory and instrumentation requirements, the need of a higher analyte concentration for the analyses, and more time-consuming measurements. To the best of our knowledge, they have never been used to study real biological samples such as human blood plasma and other biofluids (except our previous preliminary studies [8–10]). We suppose that chiroptical methods have a potential for the detection of slight conformational and stereochemical changes in the secondary and tertiary structure of biomolecules caused by pathological processes occurring during several diseases [11, 12]. For example, the diagnostics of some neurodegenerative (Alzheimer’s) and cancer (pancreatic, colon, etc.) diseases is complicated, mostly unreliable, invasive, or may be too late [13–15]. On the other hand, the diagnosis based on the analysis of human blood plasma would be minimally invasive and more tolerable for patients. Therefore, we use chiroptical spectroscopy, as electronic circular dichroism (ECD) and Raman optical activity (ROA), as a promising tool for the investigation of blood plasma samples and identification of disease-specific molecular fingerprints based on specific spectral pattern recognition. The ECD measurements of blood plasma are relatively uncomplicated [8, 9]. On the other hand, due to the presence of broad bands, ECD is not as sensitive to the secondary structure of biomolecules as ROA and VCD [1, 16, 8]. Therefore, by allowing a relatively simple measurement of aqueous solutions, ROA seems to be a more promising method for the analysis of blood plasma. However, the commercial equipment is limited to a 532-nm laser, which is the most widespread hardware version [17]. Unfortunately, excitation in the visible region represents an obstacle because it causes a strong fluorescence of real biological samples. In our study, we propose a methodology for the ROA measurements of human blood plasma to obtain reliable spectra.
Materials and methods
Blood plasma samples
Whole blood from 46 volunteers was collected by venipuncture, anticoagulant treated (ethylenediaminetetraacetic acid tripotassium salt—K3EDTA) using 9-ml sterile blood collection tubes (BD Vacutainer Systems, Plymouth, UK), and centrifuged at 1500g and 25 °C for 10 min at the Department of Oncology, First Faculty of Medicine, Charles University and General University Hospital in Prague [9]. The plasma fractions were collected, immediately frozen, and stored at −75 °C. Before each analysis, the frozen plasma samples were thawed at room temperature and filtered by centrifugation in centrifugal tubes with a polyvinylidene fluoride (PVDF) filter with a pore size of 0.45 μm (Grace, Chicago, IL, USA) at 13,000g and 15 °C for 10 min.
All optical cells were cleaned prior to and after the spectral measurements using Starna CellClean solution (Starna Scientific Ltd., Essex, UK), rinsed with demineralized water and methanol, and dried. In addition, the pH of the blood samples was monitored by a PHB-213 pH meter (Omega, Stanford, CA, USA) equipped with a pH microelectrode (Z113441, Sigma-Aldrich, Milwaukee, WI, USA).
The study was carried out according to the principles expressed in the Declaration of Helsinki and approved by the Ethics Committee of the First Faculty of Medicine and the General University Hospital, Prague. A written informed consent was secured from all subjects.
Human serum albumin sample
Human serum albumin (HSA, >99 %, fatty acid free, globulin free, Sigma-Aldrich, Saint Louis, MO, USA) was chosen as a model sample, which was prepared by dissolving 45 mg in 1.0 ml phosphate buffer (pH = 7.4, NaCl 137 mM, KCl 2.7 mM, KH2PO4 1.5 mM, Na2HPO4 8 mM). This buffer is commercially available and used to dilute blood plasma in medical routine. Prior to the spectral analysis, the sample was filtered by a syringe filter with a 0.45-μm PVDF membrane.
Raman optical activity and Raman spectroscopy
Raman optical activity/Raman spectra were measured on the ChiralRAMAN-2XTM spectrometer (BioTools Inc., Jupiter, FL, USA) equipped with a Laser Quantum (Stockport, UK) Opus 2W/MPC6000 system (exCitation at 532 nm) and a homemade Peltier cell holder to control the sample temperature. The filtered plasma (100 μl) was measured with a resolution of about 7 cm−1 in a 4 × 4 × 10 mm ROA quartz cell with an antireflective coating (BioTools Inc., Jupiter, FL, USA) at a temperature set to 15 °C. Real laser power on the sample was monitored by an Optical power meter 1916-R with 818-P sensor (Newport Corporation, Irvine, CA, USA). To correct a residual distorted baseline in raw ROA/Raman spectra, we modified the procedure described in the literature [18] and used a filtering by a fast Fourier transform (FFT) filter. The measured spectra were highly smoothed to create a virtual baseline, which was then subtracted from the raw ROA/Raman spectrum of the sample. Finally, the ROA spectra were smoothed by the FFT filter (period of ~10 cm−1).
We performed two different sets of experiments focusing on the reduction of the undesired background fluorescence of human blood plasma. Firstly, we tested sodium iodide (analytical grade, Penta a.s., Chrudim, Czech Republic) and acrylamide (Department of Organic Chemistry, ICT Prague, Czech Republic) as potential fluorescence quenchers [19, 20]. The procedure was as follows: 5 mg of acrylamide or 5, 10, and 15 mg of NaI were dissolved in 100 μl thawed and filtered plasma samples. After 5 min, a Raman spectrum was collected (280 mW real power on the sample and 0.147 s as the illumination period of the charge coupled device (CCD) detector, “time 0”) and the level of background fluorescence was evaluated from the signal at discrete wavenumbers: 671, 1242, 1569, and 1815 cm−1 (positions without any bands and covering the whole spectral region of interest). The measurement was repeated after 1, 2, 4, 6, 8, 10, and 12 h.
Secondly, we tested the practical efficiency of NaI as a fluorescence quencher for human blood plasma. At the start, a quartz cuvette was filled with 100 μl of thawed and filtered plasma and measured. The real power on the sample was set to 280 mW, and the illumination period of the CCD detector was 0.147 s. Furthermore, 10 mg of solid NaI was added to the sample as a kinetic fluorescence quencher. After 5 min, the samples were measured again (280 mW, 0.147 s). Subsequently, the sample was photobleached, which means the background fluorescence was quenched by leaving the sample in the laser beam for 12 h (280 mW). Finally, after the photobleaching, the samples were measured once more (280 mW, 0.147 s). The level of fluorescence background was evaluated by the same procedure as in the first experiment (calculated for signals at four discrete wavenumbers mentioned above).
The ROA spectra were collected after the aforementioned treatment by 10 mg of NaI and after photobleaching the sample for 12 h. The laser was set to 250 mW, and the illumination period was chosen according to the optimal working range of the CCD detector (from 1 to 2.5 s depending on individual samples). Total exposure time for the ROA spectra was kept at 24 h.
Signal-to-noise ratio (SNR) was calculated as the ratio of the ROA signal in the amide I region (intensity difference of a positive ~1675 cm−1 and a negative ~1642 cm−1 band) and root mean square (RMS) noise determined in the 2100–2200 cm−1 region, where no signals attributable to plasma biomolecules are found.
NIR-FT-Raman spectroscopy
NIR-FT-Raman spectra of raw blood plasma, blood plasma with sodium iodide (10 mg/100 μl) before and after light exposition during the ROA experiments, were recorded on an FT-Raman system consisting of an FRA 106/S module attached to an FT-IR spectrometer Equinox 55/S (Bruker, Ettlingen, Germany). The system was equipped with a quartz beam splitter, a Ge detector cooled with liquid N2, and a 1064-nm laser (Coherent, Santa Clara, CA, USA). The Raman spectra of the samples were recorded in a glass cell at 250 mW of laser power and the sample temperature of 22 °C. One thousand and twenty-four independent scans were co-added to generate each individual spectrum with a resolution of 2 cm−1. The averaged spectra were obtained from five independent experiments.
Results and discussion
Methodology of measurements and fluorescence quenchers
In the Raman spectra of raw blood plasma, we observed a high background with a strong fluorescence (Fig. 1), which caused two problems. Firstly, to avoid the saturation of the CCD detector, it was necessary to use a very short illumination period. Because of a delay time (0.93 s) between the laser pulses (CCD readout, changing the half-wave plates, setting liquid crystals to different polarity), the collection of the 24 h exposure time after pulses with 0.29–0.54 s takes 100–74 h real time of the measurement. Secondly, the fluorescence caused a strong distortion of the raw Raman and ROA spectra.

Raman spectra of unfiltered raw plasma (dotted line) and plasma filtered by a 0.45-μm PVDF filter (solid line)
We found that filtration had a positive effect on the undesirable background fluorescence (Fig. 1), which decreased with the decreasing pore size in the filters [9]. On the other hand, when the pores were too small, the high molecular weight proteins in plasma were removed and the signals were very low [9]. We examined two different pore sizes: 0.22 and 0.45 μm. By means of our observation, the ideal pore size for ROA/Raman experiments was established at 0.45 μm. According to Millipore, the producer of PVDF filters, the pore size of 0.45 μm is much larger than most plasma proteins. These filters are able to retain particles with sizes comparable to cells or larger. This means that only a small part of chylomicrons (lipoproteins) [21], possible insoluble protein aggregates, or residual blood cells can be removed from blood plasma samples. The aforementioned particles can cause unspecific scattering or exhibit intrinsic fluorescence [22, 23]. After removing them by filtration, the background fluorescence was reduced by approximately 20–50 % (depending on the sample; see Fig. 1).
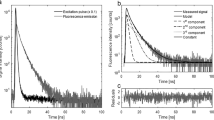
Forasmuch as the fluorescence background reduction was not sufficient enough, in the next step, we used the combination of photobleaching in a laser beam and the addition of sodium iodide or acrylamide as fluorescence quenchers [19, 20]. The effect of the kinetic quencher on the undesirable background was immediate and persistent during photobleaching in the laser beam (Fig. 2). After the addition of sodium iodide, the level of fluorescence decreased immediately (compare upper spectra in Fig. 2a, b). On the other hand, after the addition of acrylamide, the fluorescence increased temporarily due to intrinsic fluorescence of the used acrylamide (compare upper spectra in Fig. 2a, c, and Supplementary materials Fig. S1). After 12 h, the fluorescence level decreased by about 64 % (compared to the start of photobleaching/“time 0”) in the case of raw blood plasma (Fig. 2a), by 80 % after the addition of acrylamide (Fig. 2c), and even by 91 % after adding sodium iodide (Fig. 2b). The time-dependence experiment (0, 1, 2, 4, 6, 8, 10, and 12 h) was repeated with two samples. In both cases, the results showed the similar effect and trends in the fluorescence reduction (Fig. 3) although the initial level of fluorescence was different.

The time dependence of the fluoresce level of blood plasma in Raman spectra during photobleaching: raw blood plasma (a), plasma with 10 mg of sodium iodide (b), and 5 mg of acrylamide (c) per 100 μl. Spectra were measured after 0 (upper spectrum), 1, 2, 4, 6, 8, 10, and 12 h

The effect of kinetic quenchers on the reduction of fluorescence background in the Raman spectra during photobleaching; raw blood plasma (a), plasma with 5 mg of acrylamide (b), and 10 mg of sodium iodide (c) per 100 μl; the inset shows the average signal decrease with its standard deviation (the initial levels were normalized to 100 % for clarity)
Figure 3 shows averaged Raman signals at wavenumbers 671, 1242, 1569, and 1815 cm−1 (see “Materials and methods”). The inset represents the percentage of average signal decrease, where the initial fluorescence values were normalized to 100 % for clarity and their decrease was observed at the aforementioned discrete wavenumbers. Due to experiment variability, the error bars were added. Sodium iodide exhibited higher efficiency to reduce the undesirable fluorescence than acrylamide at the same molar concentration (10 mg of sodium iodide or 5 mg of acrylamide per 100 μl of blood plasma). Acrylamide also provided several Raman bands (1673, 1635, 1601, 1140, 1290, 1125, 1057, 978, 838, 626, 496, and 304 cm−1, Fig. S1 in Supplementary materials) [24] that cause spectral interference with substances in human blood plasma (for instance, 1673 and 1635 cm−1 with amide I of proteins [1]). Because of the stronger effect, no toxicity, and no significant spectral interferences, sodium iodide was finally chosen as the suitable kinetic quencher. Consequently, we tested the optimal amount of sodium iodide (see Supplementary materials Fig. S2). We observed that 10 and 15 mg of sodium iodide had a stronger effect in the reduction of fluorescence (the fluorescence level decreased approximately by 90 %) than 5 mg (approximately 80 % decrease; see the inset of Fig. S2 in Supplementary materials). The effect of 10 and 15 mg was almost the same after several hours; therefore, for our further experiments, we used the lowest amount having maximum efficiency, i.e., 10 mg.
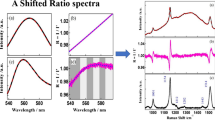
Due to the addition of a foreign substance (NaI) to the plasma samples, we tested its influence on the ROA spectra. Human serum albumin is a protein with the highest content in human blood plasma [25]. Therefore, HSA was chosen as a model sample and used for testing together with raw human blood plasma. The spectral pattern and detailed band interpretations of HSA can be found in literature [1, 8, 26]. Figure 4a, b shows negligible changes in the pair comparison of Raman/ROA spectra of HSA with/without NaI and spectra of raw blood plasma with/without NaI (Fig. 5). Some other differences shown in Figs. 4 and 5 originated mainly from residual background fluorescence after its mathematical correction.

Raman spectra of HSA (a): raw HSA (dotted line), HSA with 10 mg of sodium iodide (solid line) and ROA spectra of HSA (b): raw HSA (dotted line), HSA with 10 mg of sodium iodide (solid line) per 100 μl

ROA spectra of blood plasma: raw blood plasma (dotted line), plasma with 10 mg of sodium iodide (solid line) per 100 μl
Moreover, the ROA spectrum of raw blood plasma (without NaI) had a noticeably higher level of noise, especially in the region of 1800–2000 cm−1 (Fig. 5). The pH values were not influenced by adding either acrylamide or sodium iodide. Due to the natural buffer capacity of blood plasma (the system of bicarbonate [25, 27] and phosphate buffers [27]), the obtained values were stable.
As the second type of experiment focusing on the undesirable fluorescence, we tested the practical efficiency of sodium iodide on 46 real human blood plasma samples. After the addition of 10 mg of NaI per 100 μl of blood plasma, the fluorescence background was reduced with an average efficiency of about 31 % in 41 samples (calculated from signals at 671, 1242, 1569, 1815 cm−1). Negligible effect was observed only in five cases. Additional photobleaching of the samples in a laser beam (12 h) had an average reduction efficiency of about 76 % in comparison to the sample with NaI and about 89 % in comparison to the sample without NaI.
Figure 6 shows how NaI reduced the fluorescence background within one sample. The measurement conditions were equal (except the addition of NaI). The baseline distortion in ROA is significantly lower; compare Fig. 6e, d. In addition, while SNR achieved for raw blood plasma (Fig. 6d) was equal to 8.3, significant improvement to 20.9 was observed for plasma with sodium iodide (Fig. 6e) and to 34.4 after applying our methodology (filtration through a 0.45-μm PVDF filter, addition of sodium iodide, photobleaching, baseline correction, and FFT filtration; Fig. 6f). Thus, SNR was improved by a factor of 4.1. In the case of Raman, the spectrum in Fig. 6b has a significantly lower level of fluorescence than in Fig. 6a, which means longer acquisition time can be used, so the real time of the measurement of 24 h exposure time can be shorter. In this case, the measurement with a 1.83-s illumination period takes 36 h instead 64.5 h with a 0.55-s illumination period.

The Raman (top frames) and ROA (bottom frames) spectra of blood plasma: raw blood plasma (a, d), plasma with 10 mg of sodium iodide (b, e) per 100 μl, and plasma with 10 mg of sodium iodide per 100 μl after baseline correction and FFT filtering (c + its inset and f); 24 h of acquisition time
For 12 samples, we tested our procedure consisting of filtering combined with the addition of a kinetic quencher and photobleaching. The real time of the measurements was reduced from 70–100 h to 44–48 h (depending on the sample, for a 24-h acquisition period). Another very important benefit of our methodology was a better quality of the ROA spectra with an average increase of SNR by a factor of 3.3 (Table 1) and even in some cases allowing the ROA measurement in general.
Testing the methodology
Based on the abovementioned experiments, we established the following procedure for the Raman/ROA measurements of blood plasma-based samples and spectral data processing to suppress the undesirable fluorescence. Sodium iodide (10 mg) was added into 100 μl filtered sample of blood plasma (0.45 μm PVDF) and photobleached in a laser beam (280 mW) for 12 h. Then, the laser was set to 250 mW, the illumination period was selected according to the optimal working range of the CCD detector (from 1 to 2.5 s depending on the individual sample), and the ROA spectrum of the sample was collected. Total exposure time for the ROA/Raman spectra was kept at 24 h to achieve high SNR.
Figure 7 shows the two most different examples of the Raman and ROA spectra of human blood plasma treated with the abovementioned procedure. Three intense Raman bands at 1007, 1158, and 1519 cm−1 (Fig. 7a) can be assigned to carotenoids [8, 28–32]. Their concentration in blood plasma is low [33, 34]; however, they probably attend such intensities due to the resonance enhancement at 532-nm laser excitation. This interpretation was supported by the fact that carotenoids disappeared in the spectra with the excitation at 1064 nm (shown later in Fig. 8). Other bands localized at 1657 and 1285 cm−1 arose from the amide I and amide III vibrations of the peptide bond, respectively [1]. Other bands associated with proteins, 879 cm−1 and partly 1450 cm−1 (due to aliphatic side chains), overlap with phospholipids [8]. Phenylalanine and tryptophan show specific bands at 1588 and 1196 cm−1, and also a band at 1007 cm−1 (phenylalanine, overlapped by carotenoids). Lastly, the spectra show a band of carbohydrates at 961 cm−1. A more detailed interpretation of the particular spectral features in Raman/ROA was published previously in our work [8].

An example of the final Raman (a) and ROA (b) spectra of the two most different human blood plasma samples

FT-Raman spectra of blood plasma; raw plasma (dotted line, a), plasma with 10 mg NaI (solid line, a), plasma with 10 mg NaI and photobleached for 24 h by a 532-nm laser (dash-dotted line, a); difference of plasma with/without NaI (dotted line, b), difference of plasma with NaI and non-bleached/photobleached by a 532-nm laser (solid line, b); spectra are offset for clarity
Figure 7b shows the examples of ROA spectra of human blood plasma. The overall spectral pattern is typical for predominant α-helical proteins represented by a negative-positive couplet at (−)1645 and (+)1675 cm−1 (amide I) [1, 35, 36] and also positive bands at 1295, 1311, and 1342 cm−1 (amide III and the extended region of amide III) [1, 36]. A band for a higher contribution of β-sheets (1232 cm−1) can also be observed.
FT-Raman spectroscopy
NIR-FT-Raman spectroscopy (exCitation at 1064 nm) was chosen as an alternative method to VIS-Raman spectroscopy to estimate the sodium iodide influence on the main biomolecules of blood plasma (proteins, lipids, carbohydrates, etc.) during the ROA experiment. As VIS-Raman, NIR-FT-Raman spectroscopy provides important information about structural and environmental changes in blood plasma components. Moreover, because most biological molecules do not absorb near 1064 nm, undesirable intrinsic fluorescence is commonly suppressed or even eliminated at this excitation wavelength. Also, at an excitation over 600 nm, degradation processes rarely occur [37]; therefore, we used Raman with the excitation at 1064 nm to follow spectral changes and fluorescence of the samples if compared to excitation at a 532-nm laser.
The average NIR-FT-Raman spectra of raw blood plasma, blood plasma with sodium iodide before and after laser exposition, and their differences are shown in Fig. 8. The spectrum of raw plasma demonstrates the characteristic bands of main blood plasma components. The bands of carotenoids (1007, 1158, and 1519 cm−1; Fig. 7a) disappeared, which is the experimental verification of their resonance enhancement with the 532-nm laser. A weak negative band at 1633 cm−1 was found in the difference spectrum between raw blood plasma and the plasma with the addition of sodium iodide. However, its intensity is less than two times higher than the peak-to-peak spectral noise. The attained results demonstrate that the presence of NaI does not significantly affect the spectral response of human blood plasma even at the 1064-nm excitation, and the samples are stable during the whole measurement. After the ROA experiment, any other significant spectral changes were not observed in the plasma containing sodium iodide (data not shown).
Conclusion
We analyzed real human blood plasma samples using Raman optical activity supplemented by Raman spectroscopy while suppressing the influence of the undesired background fluorescence. To the best of our knowledge, this is the first study describing an entire experimental procedure that enables the analysis of highly fluorescent blood-based samples by ROA with the excitation at 532 nm.
Because the filtration of the samples prior to the measurements did not sufficiently reduce the fluorescence, kinetic fluorescence quenchers were added and the samples subjected to a laser treatment (photobleaching). Due to its higher efficiency, lack of toxicity, and lack of spectral interference, sodium iodide was chosen as a suitable fluorescence quencher. The combination of sodium iodide with laser photobleaching of the sample led to a satisfactory reduction of the spectral background approximately by 90 %. In addition, the signal-to-noise ratio was significantly increased (in average by a factor of 3.3), while the baseline distortion remained low. Moreover, the decrease in fluorescence reduced the time required for each measurement by an average of 50 %. Indeed, without our method, it would not even have been possible to analyze some of the real human blood plasma samples, due to their strong intrinsic fluorescence.
References
Barron LD, Hecht L, Blanch EW, Bell AF (2000) Prog Biophys Mol Biol 73:1–49
Berova N, Polavarapu PL, Nakanishi K, Woody RW (2012) Comprehensive chiroptical spectroscopy. Wiley, New Jersey
Nafie LA (2011) Vibrational optical activity: principles and applications. Wiley, New York
He Y, Bo W, Dukor RK, Nafie LA (2011) Appl Spectrosc 65:699–723
Shah RD, Nafie LA (2001) Curr Opin Drug Discov Dev 4:764–775
Urbanová M, Setnička V, Volka K (2000) Chirality 12:199–203
Julínek O, Setnička V, Řezáčová A, Dohnal J, Vosátka V, Urbanová M (2010) J Pharm Biomed Anal 53:958–961
Synytsya A, Judexová M, Hrubý T, Tatarkovič M, Miškovičová M, Petruželka L, Setnička V (2013) Anal Bioanal Chem 405:5441–5453
Tatarkovič M, Fišar Z, Raboch J, Jirák R, Setnička V (2012) Chirality 24:951–955
Tatarkovič M, Kykal S, Synytsya A, Miškovičová M, Petruželka L, Setnička V (2013) Eur Biophys J 42:S107–S107
Minde DP, Anvarian Z, Rudiger SG, Maurice MM (2011) Mol Cancer 10:101
Querfurth HW, LaFerla FM (2010) N Engl J Med 362:329–344
Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen RC, Snyder PJ, Carrillo MC, Thies B, Phelps CH (2011) Alzheimers Dement 7:270–279
Chari ST (2007) Semin Oncol 34:284–294
Adelstein B-A, Macaskill P, Chan S, Katelaris P, Irwig L (2011) BMC Gastroenterol 11:65
Blanch EW, Hecht L, Syme CD, Volpetti V, Lomonossoff GP, Nielsen K, Barron LD (2002) J Gen Virol 83:2593–2600
Barron LD (2013) Raman optical activity studies of structure and behavior of biomolecules. In: Roberts GK (ed) Encyclopedia of biophysics. Springer, Berlin
Člupek M, Matějka P, Volka K (2007) J Raman Spectrosc 38:1174–1179
Bekhouche M, Blum LJ, Doumèche B (2011) J Phys Chem B 116:413–423
Chmyrov A, Sandén T, Widengren J (2010) J Phys Chem B 114:11282–11291
Murray RK, Granner DK, Mayes PA, Rodwell VW (2003) Harper’s illustrated biochemistry (26th edition). McGraw-Hill, New York
Engelsman J, Garidel P, Smulders R, Koll H, Smith B, Bassarab S, Seidl A, Hainzl O, Jiskoot W (2011) Pharm Res 28:920–933
Hug W (1981) Appl Spectrosc 35:115–124
Jonathan N (1961) J Mol Spectrosc 6:205–214
Garrett R, Grisham CM (1995) Biochemistry. Saunders College Pub, Belmont
Barron LD, Buckingham AD (2010) Chem Phys Lett 492:199–213
Hames BD, Hooper NM (2005) Instant notes in biochemistry. Taylor & Francis, Abingdon
Darvin ME, Gersonde I, Albrecht H, Sterry W, Lademann J (2007) Laser Phys Lett 4:452–456
Hata TR, Scholz TA, Ermakov IV, McClane RW, Khachik F, Gellermann W, Pershing LK (2000) J Investig Dermatol 115:441–448
Redd DCB, Feng ZC, Yue KT, Gansler TS (1993) Appl Spectrosc 47:787–791
Schulte F, Mäder J, Kroh LW, Panne U, Kneipp J (2009) Anal Chem 81:8426–8433
Stone N, Kendall C, Smith J, Crow P, Barr H (2004) Faraday Discuss 126:141–157
Ollberding NJ, Maskarinec G, Conroy SM, Morimoto Y, Franke AA, Cooney RV, Wilkens LR, Le Marchand L, Goodman MT, Hernandez BY, Henderson BE, Kolonel LN (2012) Blood 119:5817–5823
Parker RS (1989) J Nutr 119:101–104
Urbanová M (2009) Chirality 21:E215–E230
Kinalwa MN, Blanch EW, Doig AJ (2010) Anal Chem 82:6347–6349
Puppels GJ, Olminkhof JHF, Segers-Nolten GMJ, Otto C, Mul FFM, Greve J (1991) Exp Cell Res 195:361–367
Acknowledgments
The work was supported by the Ministry of Health of the Czech Republic (Grant No. NT13259-3) and partly by Specific University Research MSMT No. 20/2013 - A1_FCHI_2013_003 and A2_FCHI_2013_003.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 136 kb)
Rights and permissions
About this article

Cite this article
Tatarkovič, M., Synytsya, A., Šťovíčková, L. et al. The minimizing of fluorescence background in Raman optical activity and Raman spectra of human blood plasma. Anal Bioanal Chem 407, 1335–1342 (2015). https://doi.org/10.1007/s00216-014-8358-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-014-8358-7