
Abstract
Spinal cord edema is a quick-onset phenomenon with long-term effects. This complication is associated with inflammatory responses, as well as poor motor function. No effective treatment has been developed against spinal edema, which urges the need to provide novel therapies. Astaxanthin (AST) is a fat-soluble carotenoid with anti-inflammatory effects and a promising candidate for treating neurological disorders. This study aimed to investigate the underlying mechanism of AST on the inhibition of spinal cord edema, astrocyte activation, and reduction of inflammatory responsesin a rat compression spinal cord injury (SCI) model. Male rats underwent laminectomy at thoracic 8–9, and the SCI model was induced using an aneurysm clip. After SCI, rats received dimethyl sulfoxide or AST via intrathecal injection. The effects of AST were examined on the motor function, spinal cord edema, integrity of blood-spinal cord barrier (BSCB), and expression of high mobility group box 1 (HMGB1), toll-like receptor 4 (TLR4), nuclear factor-kappa B (NF-κB), glial fibrillary acidic protein (GFAP), and aquaporin-4 (AQP4), and matrix metallopeptidase- 9 (MMP-9) post-SCI. We showed that AST potentially improved the recovery of motor function and inhibited the spinal cord edema via maintaining the integrity of BSCB, reducing the expression of HMGB1, TLR4, and NF-κB, MMP-9 as well as downregulation of astrocyte activation (GFAP) and AQP4 expression. AST improves motor function and reduces edema and inflammatory responses in the spinal tissue. These effects are mediated by suppression of the HMGB1/TLR4/NF-κB signaling pathway, suppressing post-SCI astrocyte activation, and decreasing AQP4 and MMP-9 expression.
Graphical abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Spinal cord injury (SCI) is one of the most common causes of disability and mortality worldwide. SCI is composed of primary and secondary molecular phases. The primary mechanical events are usually followed by a number of secondary consequences, including electrolyte disturbances, neuroinflammation, functional impairment of the blood-spinal cord barrier (BSCB), and spinal cord edema (Anwar et al. 2016). Inflammatory responses initiate two main types of edema, cytotoxic and vasogenic following SCI (Huang et al. 2019). Extracellular high mobility group box-1 (HMGB1) induces this inflammatory response in neurons and astrocytes via activation of toll-like receptor-4 (TLR4)/receptor of advanced glycation end product (RAGE)/nuclear factor-kappa B (NF-κB) signaling pathway (Ohnishi et al. 2014). HMGB1 and its associated signaling pathways resulted in cytotoxic edema with a significant increase in astrocyte swelling, as well as aquaporin-4 (AQP4) expression after SCI (Sun et al. 2019). AQP4s are normally expressed in the perivascular membrane of astrocytes and provide the main pathway for water movement (Papadopoulos and Verkman 2013). Several experimental studies have shown that AQP4 expression is closely interconnected to spinal cord edema and BSCB which is occurred shortly following the primary injury (Oklinski et al. 2016, Pan et al. 2019). In the signaling pathways following SCI, it seems that matrix metalloproteinase-9 (MMP-9) is regulated by the NF-κB factor. MMP-9 matrix belongs to a family of zinc-binding proteolytic enzymes, and in pathological conditions, MMP-9 plays an important role in causing vasogenic edema by degradation of the main components of the extracellular matrix (Noble et al. 2002). Therefore, inhibition of such signaling can reduce the swelling of astrocytes and edema in rats, and improve motor function subsequently (Zhang et al. 2011; Sun et al. 2019).
There are limited numbers of alternative therapies that target specific molecules involved in spinal cord edema (Liu et al. 2015). Astaxanthin (AST) is a potent ketocarotenoid with strong antioxidant and anti-inflammatory properties. The notable effects of AST on targeting various signaling pathways have been reported in vivo and in vitro studies (Fakhri et al. 2018a). Previously, we reported the significant effects of AST on improving sensory and motor complications in rats after SCI (Masoudi et al. 2017; Fakhri et al. 2018b, 2019). In this study, we seek to investigate the underlying mechanisms of AST on spinal cord edema and inflammatory responses and during a compression SCI rat model.
Materials and methods
Animals
A total of 108 adult male Wistar rats (230–250 g) were purchased from the Neuroscience Research Center, Shahid Beheshti University of Medical Sciences, Iran. All animal experiments were approved by the institutional animal care and use committee at the Iran University of Medical Sciences (IR.IUMS.REC.1399.1007). The rats were randomly assigned to 3 groups sham, SCI + DMSO (vehicle/control), and SCI + AST (treatment) groups. AST was dissolved in 5% dimethyl sulfoxide (DMSO) just before use, and 30-min after SCI, 10 μl of 5% DMSO and 10 μl of 0.005 mg/kg AST were intrathecally injected into SCI + DMSO, and SCI + AST groups, respectively.
Compression SCI
The rat compression model was designed based on our previous experiment (Fakhri et al. 2019). Briefly, the male rats were anesthetized using ketamine/xylazine (80/20 mg/kg, intraperitoneal [i.p.]). After placement on a heating pad, the skin was cut in the thoracic 8–10 (T8-10), and a complete laminectomy was performed at the T9 level. Then, compression SCI was induced by an aneurysm clip (Aesculap, Tuttlingen, Germany) with a force of 90 g for 60 s. Finally, the muscles and skin were closed with thread. To prevent infection, cefazolin was i.p. administrated in a dose of 40 mg/kg for 3 consecutive days. For neurogenic bladder care, a hand massage of the hypogastric region was performed twice daily.
Evaluation of motor function
Motor function was assessed before (Day 0) and every week after SCI from 1st week to 4th week, using the Basso, Beattie, and Bresnahan scores (BBB) (Fakhri et al. 2019). In addition to BBB assessment, we used a beam walking test, including two parameters of foot-stepping angle (FSA) and rump height index (RHI) for complex and objective evaluation of motor recovery. FSA is the angular degree that the foot makes at the instant of ground contact. In intact rats, this angle is approximately 20 degrees. After SCI, this amount increases to 150 degrees. RHI is the height of the rump, the vertical distance from the dorsal of the rat's tail to the beam. Values for the right and left feet were averaged. Then, the distances and angles were obtained using Image Tool 2.0 software. The recovery index (RI) is an individual estimate for each specific parameter described above and is calculated as a percentage described below.
RI = [(Y7+n − Y7)/(Y0 − Y7)] × 100, where Y0, Y7, and Y7+n are experimental values before the injury (Day 0), 7 days after injury (Day 7), and a time-point (n) days after SCI (Days 14, 21, and 28), respectively. This measure estimates the increase in performance (Y7+n − Y7) as a fraction of the functional decline (Y0 − Y7) induced by SCI. The overall RI was calculated as means of RI for all the three parameters, BBB, FSA and RHI (Saini et al. 2016).
Determination of tissue water content
The water content of spinal cord was estimated by wet/dry method. On the 12 h and 1st, 3rd and 7th days after surgery, 1 cm of the spinal cord, including lesion epicenter, was weighed on digital scales. Afterward, tissues were heated at 80 °C for 48 h and re-weighed.
The percentage water content was calculated via the formula below:
Magnetic resonance imaging (MRI) scanning
The spinal edema was assessed by MRI (Sandner et al. 2009). MRI was performed on a 3 T clinical MR scanner (GE Discovery MR750w) with a Flex coil. On day 7, Rats were anesthetized using an i.p. injection of ketamine/xylazine (80/20 mg/kg) and were placed in a supine position. Two-dimensional axial and sagittal images of the spine were obtained.
Spin echo pulse sequence was used for acquiring T2-weighted images in sagittal and axial planes. The following parameters of the spin echo sequence were applied: repetition time of 2902 ms, echo time of 85 ms, image matrix 224 × 224, field of view of 6 × 6 cm, and a number of acquisitions of 12. The acquired images had an in-plane resolution of 268 lm with a section thickness of 1.5 mm and spacing is 0.1 mm between sections. The total volume of the spinal cord was measured at 1 cm of the site of injury, and also the volume of hyperintensity in T2 images was measured over one slice at the epicenter of the lesion in the axial plan. Data were processed using 3D Slicer (http://www.slicer.org).
Assessment of evans blue extravasation
The BSCB disruption was assessed using Evans blue (EB) dye (Sigma-Aldrich, 314–13-6). One day after SCI, rats received 5 mL of Evans blue 2% and then perfused with 0.1 M phosphate-buffered saline (PBS) 3 h later. About 1 cm of spinal cord centered at the lesion site was separated and macroscopic photographs were obtained. Then, tissues were homogenized in PBS, and an equal volume of 50% trichloroacetic acid (Sigma-Aldrich, T0699) was added to each sample. After centrifugation, supernatants were diluted to 1:3 with ethanol. Finally, EB absorbance was measured at 610 nm using a spectrophotometer (Cabrera-Aldana et al. 2017; Park et al. 2020).
Western blot assay
On the 12 h, 1st, 3rd, and 7th days after surgery, 1 cm of spinal cord injury site (T8-9) was collected and homogenized in RIPA lysis buffer and protease inhibitor 1% (Roche, 11836153001). Tissues were centrifugated at 12.000 rpm for 30 min. Protein concentration was assessed using Bradford assay and bovine serum albumin (BSA) as the standard. Proteins were loaded and separated by 10% SDS-PAGE and transferred to a polyvinylidene difluoride (PVDF) membrane (Millipore, IPVH00010). PVDF paper was cut depending on the molecular weight proteins of the proteins. Then, membranes were blocked in 2% nonfat dry milk. After 2 h, blots were incubated overnight at 4 °C with primary antibodies: anti-GFAP (1:10000, Cell Signaling, 3670), anti-AQP4 (1:1000, Novus Biologicals, NBP2-92886), anti-HMGB1(1:1000, Novus Biologicals, NB100-2322SS), anti-MMP-9 (1:1000, Novus Biologicals, NBP2-13173), anti-TLR4 (1:1000, Novus Biologicals, NB100-56723), anti-NF-κB (1:500 Santa Cruz, sc-8008), and anti-β-Actin (1:1000, Cell Signaling, 3700). Afterward, the membranes were washed in Tris-buffered saline with Tween-80 (TBST), and incubated for 120 min with anti-rabbit (1:8000, Cell Signaling, 7074) and anti-mouse secondary (1:8000, Cell Signaling, 7076) antibody for three times. Immunoreactive proteins were visualized via ECL chemiluminescence kit (Amersham, GE HealthCare, RPN2232). Eventually, the protein levels were densitometry by Image J software.
Statistical analysis
Graph pad Prism software (Version 8.0) was used for statistical analyses. All values were expressed as mean ± standard error of the mean (SEM), and statistical significance was p value of < 0.05. One-way and two-way analyses of variance (ANOVA) with Tukey or Bonferroni post-hoc test were used to compare the differences among the three groups in all tests. The correlation between HMGB1, GFAP, AQP4, and MMP-9 levels in spinal cord tissue and BBB score (motor activity) was assessed by correlation Pearson analysis in SCI + DMSO and SCI + AST groups.
Results
AST ameliorated motor function after SCI
Compression SCI caused severe motor disabilities that were estimated by the BBB scores 4 weeks after injury. Rats treated with AST showed increased mean BBB scores from the first week (Groups: F 2, 90 = 569.6, p < 0.0001; times: F 4, 90 = 142.5, p < 0.0001; interaction: F 8, 90 = 47.74, p < 0.0001; Fig. 1a, b). In addition, we analyzed the plantar stepping ability of the rats by measuring the FSA, which was in agreement with the BBB scores (Groups: F 2, 90 = 1381, p < 0.0001; times: F 4, 90 = 393, p < 0.0001; interaction: F 8, 90 = 114.1, p < 0.0001; Fig. 1c, d). Superior motor function was observed in the SCI + AST group compared to the SCI + DMSO group from the first week. Furthermore, RHI was analyzed as a parameter to evaluate the ability to support body weight during ground movement (Groups: F 2, 90 = 593.8, p < 0.0001; times: F 4, 90 = 151.2, p < 0.0001; interaction: F 8, 90 = 44.65, p < 0.0001; Fig. 1e, f). The results showed that rats treated with AST had a higher RHI and smaller FSA than the SCI + DMSO group. Overall recovery indices for each rat displayed a better overall result in the SCI + AST group compared to the SCI + DMSO group (Groups: F 1, 36 = 169.9, p < 0.0001; times: F 2, 36 = 91.51, p < 0.0001; interaction: F 2, 36 = 19.62, p < 0.0001; Fig. 1g).

Effects of AST on motor function after SCI. Time course and degree of motor recovery in rats treated with AST during 4 weeks post-SCI. (a) BBB scores, (c) FSA, (e) RHI, (b, d, f) recovery indices, and (g) the overall recovery index. Data are shown as mean ± SEM (n = 6). *** p < 0.001 versus sham group and + p < 0.05,++ p < 0.01, +++ p < 0.001 versus SCI + DMSO group. Statistical comparisons were made using a two-way analysis of variance with the Bonferroni post-hoc test. AST: Astaxanthin (10 μl of 0.005 mg/kg), BBB: Basso, Beattie and Bresnahan scores, DMSO: 5% Dimethylsulfoxide (vehicle, 10 µl), FSA: Foot-stepping angle, RHI: Rump height index, SCI: Spinal cord injury
AST decreased spinal cord edema after SCI
Water content was detected in the injured spinal cord by wet/dry method on the 12 h, 1st, 3rd, and 7th days after surgery. As shown in Fig. 2a, the water content of the SCI group was obviously increased compared with the sham group. Treatment with AST significantly alleviated the amount of water content after SCI from day 1 to day 7 (Groups: F 2, 24 = 86.24, p < 0.0001; times: F 3, 24 = 1.358, p = 0.2793; interaction: F 6, 24 = 1.627, p = 0.1830; Fig. 2a).

Effects of AST on the spinal cord edema of SCI rats. (a) Changes in spinal cord water content on the 12 h and 1st, 3rd, and 7th days after surgery. The sagittal (b) and axial (c) T2-weighted MRI showed no edema in the sham group, whereas extensive edema was observed in the SCI groups seven days after SCI. Treatment with AST was associated with reduced edema. Analysis of edema (volume hyperintense) at 1 cm of the injury site (d) and in one slice in the epicenter of the injury (e) revealed a significantly reduced edema in AST-treated rats on day 7 after SCI. Data are shown as mean ± SEM (n = 3). *** p < 0.001 versus sham group and ++ p < 0.01, +++ p < 0.001 versus SCI + DMSO group. Statistical comparisons were made using one-way and two-way analysis of variance with Tukey or Bonferroni post-hoc test. AST: Astaxanthin (10 μl of 0.005 mg/kg), DMSO: 5% Dimethylsulfoxide (vehicle, 10 µl), MRI: Magnetic resonance imaging, SCI: Spinal cord injury
We examined the spinal edema after SCI using the MRI method on day 7. Both the sagittal and axial T2-weighted MRI showed no spinal edema in the sham group, whereas extensive edema was observed in the spinal cord of rats seven days after SCI. Treatment with AST significantly decreased spinal edema in rats (Fig. 2b, c).
As expected, T2-weighted imaging revealed no hyperintense pixel in sham-operated rats. But the volume hyperintense in 1 cm of the spinal cord tissue (T8-9), and the volume hyperintense in one slice in the epicenter of the injury in T2-weighted MRI was significantly increased in SCI + DMSO group seven days after SCI (F 2, 6 = 141.1, p < 0.0001; Fig. 2d). These enhanced volumes were significantly attenuated by AST compared with the SCI + DMSO group (F 2, 6 = 368.3, p < 0.0001, Fig. 2e).
AST ameliorated BSCB disruption and reduced MMP-9 activation after SCI
The integrity of BSCB after SCI was determined based on the permeability of EB dye (Fig. 3a). As shown in Fig. 3b, the SCI led to more BSCB extravasation into the spinal cord tissues on day 1. The BSCB influx of EB dye was significantly reduced in the SCI + AST group (F 2, 6 = 203.3, p < 0.0001; Fig. 3b).

Effects of AST on the integrity of BSCB and expression of MMP-9 after SCI. (a, b) Representative spinal cords and quantification of BSCB permeability data at 1 day after SCI. (c, d) Representative western blots and quantification data of MMP-9 on the 12 h and 1st, 3rd, and 7th days after surgery. (e) the correlation n between MMP9 level in spinal cord tissue and BBB score (motor activity). Data are shown as mean ± SEM (n = 3). * p < 0.05, *** p < 0.001 versus sham group and + p < 0.05,+++ p < 0.001 versus SCI + DMSO group. Statistical comparisons were made using one-way and two-way analysis of variance with Tukey or Bonferroni post-hoc test. AST: Astaxanthin (10 μl of 0.005 mg/kg), DMSO: 5% Dimethylsulfoxide (vehicle, 10 µl), MMP-9: Matrix Metalloproteinase-9, SCI: Spinal cord injury
On the other hand, MMP-9 plays an important role in BSCB dysfunction (Noble et al. 2002). In this regard, the MMP-9 expression was detected by western blot on the 12 h, 1st, 3rd, and 7th days after surgery. The level of MMP-9 in the SCI + DMSO group was significantly higher, compared with that in the sham group. AST led to a reduction in the level of MMP-9 compared with the SCI + DMSO group (Groups: F 2, 24 = 76.14, p < 0.0001; times: F 3, 24 = 10.05, p = 0.0002; interaction: F 6, 24 = 1.361, p = 0.2700; Fig. 3c, d). A significant negative correlation was observed between the BBB score and HMGB1 spinal level (r = -0.8889, p = 0.0048, Fig. 3e).
Effects of AST on HMGB1/TLR4/ NF-κB pathway after SCI
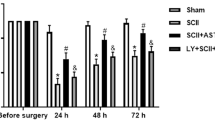
Expression levels of HMGB1, TLR4, and NF-κB after SCI were determined by Western blot analyses (Fig. 4a). HMGB1, TLR4, and NF-κB protein levels were significantly increased compared with the sham group on the 12 h, 1st, 3rd and 7th days after SCI, while the level of HMGB1(Groups: F 2, 24 = 147.8, p < 0.0001; times: F 3, 24 = 11.28, p < 0.0001; interaction: F 6, 24 = 2.469, p = 0.0529; Fig. 4b), TLR4 (Groups: F 2, 24 = 226.6, p < 0.0001; times: F 3, 24 = 5.658, p = 0.0045; interaction: F 6, 24 = 2.568, p = 0.0458; Fig. 4c) and NF-κB (Groups: F 2, 24 = 380.4, p < 0.0001; times: F 3, 24 = 3.847, p = 0.0222; interaction: F 6, 24 = 7.202, p = 0.0002; Fig. 4d) was significantly lower in the SCI + AST group at the same time points. A significant negative correlation was observed between the BBB score and HMGB1 spinal level (r = -0.8712, p = 0.0065, Fig. 4e).

Effects of AST on HMGB1/TLR4/ NF-κB pathway after SCI. (a) western blot analysis and Optical density ratio of (b) HMGB1, (c) TLR4, (d) NF-κB to β-actin on the 12 h and 1st, 3rd, and 7th days after SCI, and (e) the correlation n between HMGB1level in spinal cord tissue and BBB score (motor activity). Data are shown as mean ± SEM (n = 3). * p < 0.05, *** p < 0.001 versus sham and + p < 0.05, ++ p < 0.01, +++ p < 0.001 versus SCI + DMSO group. Statistical comparisons were made using a two-way analysis of variance with the Bonferroni post-hoc test. AST: Astaxanthin (10 μl of 0.005 mg/kg), BBB: Basso, Beattie, and Bresnahan scores, DMSO: 5% Dimethylsulfoxide (vehicle, 10 µl), GFAP: Glial fibrillary acidic protein, NF-κB: nuclear factor-kappa B, SCI: Spinal cord injury, TLR4: Toll-like receptor-4
Effects of AST on GFAP and AQP4 expression after SCI
The changes in the spinal cord GFAP and AQP4 levels of, the three groups were observed using Western blot (Fig. 5a). GFAP and AQP4 expression significantly increased on the 12 h, 1st, 3rd, and 7th days after SCI. Compared with the SCI + DMSO group, the level of GFAP (Groups: F 2, 24 = 147.6, p < 0.0001; times: F 3, 24 = 7.333, p = 0.0012; interaction: F 6, 24 = 1.309, p = 0.2910; Fig. 5b) and AQP4 (Groups: F 2, 24 = 162.6, p < 0.0001; times: F 3, 24 = 5.430, p = 0.0054; interaction: F 6, 24 = 1.238, p = 0.3224; Fig. 5c). was significantly lower in the SCI + AST group at the same time points A significant negative correlation was observed between the BBB score and GFAP spinal level (r = -0.9226, p = 0.0023, Fig. 5d) and AQP4 spinal level (r = -0.9245, p = 0.0022, Fig. 5e).

Effects of AST on GFAP and AQP4 expression after SCI. (a) western blot analysis and Optical density ratio of (b) GFAP, and (c) AQP4 to β-actin on the 12 h and 1st, 3rd and 7th days after SCI, the correlation between (d) GFAP and (e) AQP4 level in spinal cord tissue and BBB score (motor activity). Data are shown as mean ± SEM (n = 3). * p < 0.05, ** p < 0.01, *** p < 0.001 versus sham and + p < 0.05, ++ p < 0.01, +++ p < 0.001 versus SCI + DMSO group. Statistical comparisions were made using two-way analysis of variance with Bonferroni post-hoc test. AST: Astaxanthin (10 μl of 0.005 mg/kg), AQP4: Aquapurin-4, BBB: Basso, Beattie and Bresnahan scores, DMSO: 5% Dimethylsulfoxide (vehicle, 10 µl), GFAP: Glial fibrillary acidic protein, SCI: Spinal cord injury
Discussion
The present study showed that intrathecal administration of a single dose of AST (10 μl of 0.005 mg/kg) improved motor outcomes by reducing inflammatory responses and spinal cord edema that coccur following the primary injury. At the molecular level, AST suppressed the HMGB1/TLR4/NF-κB signaling pathway and downregulated the astrocytes activation, AQP4, and MMP-9 expression toward such therapeutic effects.
Among the different models of SCI, the compression SCI model is more suitable for studying pressure and edema on the surface of the spinal cord, because, in this model, pressure is applied equally and simultaneously on both the dorsal and ventral surfaces of the spinal cord (Poon et al. 2007). Wagner and Stewart reported that the extension of spinal cord edema is directly related to the amount of initial trauma (Wagner and Stewart 1981). SCI-induced motor dysfunction is closely related to the degree of edema and the magnitude of neuroprotective (Sharma et al. 2005). In this study, we induced the severe compression SCI model in rats.
Following SCI, the inflammatory response causes edema in the acute stage of injury, which is strongly connected to the activation of the secondary signaling cascade and motor dysfunction of SCI (Oshio et al. 2004). Following early edema, intrathecal pressure increases lead to decreased blood flow and inadequate nutrition of spinal cord tissue. These conditions result in spinal ischemia, cell death, and motor dysfunction. The symptoms of edema appear within 5 min after the injury and peak over 1 week. It generally resolves within 14 days, when the astrocytes form the glial scar and the BSCB regenerates (Cho et al. 2017, Pan et al. 2019).
The initiator of this inflammatory response is the HMGB1 protein, which increases the expression of AQP4 and the activity of astrocytes. The breakdown of the BSCB also causes the process of cell death and impaired motor function. HMGB1 is an inflammatory cytokine released from activated astrocytes and microglia in the CNS as well as from necrotic cells after pathogenic or tissue damage (Agalave and Svensson 2014). The effects of HMGB1 are mediated through TLRs. The interaction between HMGB1 and TLR4 resulted in the activation of NF-κB, which increases the production and release of cytokines (Sun et al. 2017).
It has been reported that inhibition of HMGB1-TLR4 signaling decreased cerebral edema in a TBI injury model by reducing neurovascular disorders and AQP4 expression (Laird et al. 2014). Activation of NF-κB in astrocytes has been reported to be a key factor in the process of cerebral edema after TBI in rats (Wang et al. 2016). It has been shown that the inhibition of HMGB1 in models of brain and spinal cord injury led to the improvement of motor performance by reducing inflammatory factors (Ieong et al. 2018), spinal fluid content, and spinal cord edema (Sun et al. 2019). Zhang et al. showed that AST treatment reduced cerebral inflammation and cerebral edema, and improved neurological function by inhibiting the TLR4 signaling following subarachnoid hemorrhage (SAH) (Zhang et al. 2019). An in vivo study reported that pretreatment with AST significantly prevented the trauma-induced initiation of NF-κB, and expressions of pro-inflammatory cytokines (Zhang et al. 2017). In agreement with other studies, our results also showed that AST could significantly reduce the increased expression level of HMGB1, TLR4, and NF-κB after SCI and improve motor function in rats.
There are two types of spinal edema, vasogenic edema, and cytotoxic edema (Huang et al. 2019). Vasogenic edema is caused by a disturbance in the integrity of the BSCB. The BSCB consists of endothelial cells, pericytes, astrocytes, and basal layers at the cellular level. which is an obstacle against the entry of pathogens and blood-derived cells into the spinal cord parenchyma. Following SCI and inflammatory conditions, MMP-9 s are produced by activated microglia and astrocytes. They cause the breakdown of the BSCB and the development of vasogenic edema by destroying the basal layer and loosening the connections between endothelial cells (Kumar et al. 2017). Moreover, AQP4s lead to more damage to endothelial cells with the entry of water and an increase in hydrostatic pressure and thus intensify vasogenic edema. Therefore, excess water, ions, inflammatory factors, and immune cells (neutrophils, lymphocytes, etc.) penetrate into the spinal cord parenchyma, and the entry of these substances intensifies the inflammation (Jin et al. 2021). These reciprocal events lead to edema, the release of glutamate, an increase in continuous calcium flux, and ultimately neuronal death and motor dysfunction (Nishibori et al. 2020). It has been reported that 24 h after SCI, MMP-9 activity is increased, which is associated with a significant reduction in BSCB disruption and improved motor performance (Noble et al. 2002), and maximal BSCB disruption has been reported 24 h after the SCI (Figley et al. 2014).
Inhibition of the NF-κB/MMP-9 pathway has been able to improve motor function by reducing the blood–brain barrier (Teng et al. 2017) and BSCB (Lee et al. 2012) disruption. Zhang et al. showed that intraventricular injection of AST reduced the expression and activity of MMP-9 in the brain of male rats 30 min after the SAH model (Zhang et al. 2015). Consistent with other studies, our results also showed that AST maintained BSCB integrity after injury by reducing MMP-9 expression.
Cytotoxic edema is caused by swelling of astrocytes and increased expression of AQP4s. In the astrocyte end feet, AQP4s are in the vicinity of Na + /K + -ATPase pumps and Na + -K + -Cl- cotransporter (NKCC) and metabotropic glutamate receptor subtype 5 (mGluR5) receptors. In the conditions of SCI and ATP deprivation, the function of Na + /K + -ATPase pumps is disrupted, which moves Na + against its concentration gradient and causes ionic imbalance. To counteract this ionic imbalance, Cl- ions are transported into the cell through NKCC cotransporter to electrically neutralize it, which results in excessive water entering the cell through AQP4s and causing cytotoxic edema. On the other hand, the activity of AQP4 causes the activation and migration of astrocytes. Activated astrocytes increase the flow of calcium (Huang et al. 2021). AQP4 can facilitate the influx of calcium ions through the activation of autocrine purinergic signaling (P2 purinergic receptor) and transient receptor potential vanilloid 4 (TRPV 4) into astrocytes. Calcium ions activate calmodulin (CaM). CaM can also promote protein kinase A (PKA) activation. Finally, the activation of PKA causes the activation of AQP4 and the entry of more water into astrocytes (Kitchen et al. 2015; Huang et al. 2021). In addition, the activation of astrocytes through mGluR5 receptors causes the accumulation of glutamate inside the cell. Accumulation of glutamate leads to the swelling of astrocytes, and the exacerbation of cytotoxic edema (Illarionova et al. 2010). It has been reported that AQP4 deficiency or knock-down in mice was associated with reduced brain edema, inhibition of glial scar formation, and improved neurological function (Verkman et al. 2006). Liu et al. suggested that a decrease in AQP4 leads to an anti-inflammatory response that alleviates brain edema (Liu et al. 2017). Down-regulation of AQP4 expression reduced the SCI secondary phase caused by the formation of glial scar and enhanced inflammation (Pan et al. 2022). In 2016, Zhang et al. showed that intraperitoneal administration of 100 mg/kg of AST alleviates cerebral edema by modulating AQP4 and NKCC expression after TBI in mice. Our results also showed that AST could significantly prevent the increase in the expression of GFAP and AQP4 after spinal cord injury and reduce the edema and water content of the spinal cord.
We note a suggestion for this study. Although AST reduced early spinal cord edema and improved locomotor function after spinal cord injury in rats, the observation period was relatively short. In future experiments, a longer observation period (over 7 days after SCI) may be needed.
Taken together, our results demonstrated that AST treatment could reduce both cytotoxic and vasogenic edema and improve motor function. These effects were associated with the inhibition of the HMGB1/TLR4/NF-κB pathway, prevention of astrocyte activation, downregulation of the expression of AQP4 and MMP-9, and maintaining the integrity of the BSCB in the SCI rat model. Given the early and prominent effects of AST, it may be possible to suggest it as a novel potential therapeutic agent for SCI.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AQP4:
-
Aquapurin-4
- AST:
-
Astaxanthin
- BBB:
-
Basso, Beattie and Bresnahan
- BSA:
-
Bovine serum albumin
- BSCB:
-
Blood-spinal cord barrier
- CAM:
-
Calmodulin
- DMSO:
-
Dimethyl sulfoxide
- EB:
-
Evans blue
- FSA:
-
Foot-stepping angle
- GFAP:
-
Glial fibrillary acidic protein
- HMGB1:
-
High mobility group box-1
- MMP-9:
-
Matrix metalloproteinase-9
- MRI:
-
Magnetic Resonance Imaging
- NF-Κb:
-
Nuclear factor-kappa B
- PBS:
-
Phosphate-buffered saline
- PKA:
-
Protein kinase A
- PVDF:
-
Polyvinylidene difluoride
- RAGE:
-
Receptor of advanced glycation end product
- RHI:
-
Rump height index
- RI:
-
Recovery index
- SAH:
-
Subarachnoid hemorrhage
- SCI:
-
Spinal cord injury
- TBI:
-
Traumatic brain injury
- TLR4:
-
Toll-like receptor-4
- TRPV4:
-
Transient receptor potential vanilloid-type 4
- TNF:
-
Tumor necrosis factor
References
Agalave NM, Svensson CI (2014) Extracellular high-mobility group box 1 protein (HMGB1) as a mediator of persistent pain. Mol Med 20:569–578
Anwar MA, Al Shehabi TS, Eid AH (2016) Inflammogenesis of secondary spinal cord injury. Front Cell Neurosci 10:98
Cabrera-Aldana EE, Ruelas F, Aranda C, Rincon-Heredia R, Martínez-Cruz A, Reyes-Sánchez A, Guizar-Sahagún G, Tovar-y-Romo LB (2017) Methylprednisolone administration following spinal cord injury reduces aquaporin 4 expression and exacerbates edema. Mediators Inflamm 2017: 4792932
Cho N, Hachem LD, Fehlings MG (2017) Spinal cord edema after spinal cord injury: from pathogenesis to management. Brain Edema. Elsevier, pp 261–275
Fakhri S, Abbaszadeh F, Dargahi L, Jorjani M (2018a) Astaxanthin: A mechanistic review on its biological activities and health benefits. Pharmacol Res 136:1–20
Fakhri S, Dargahi L, Abbaszadeh F, Jorjani M (2018b) Astaxanthin attenuates neuroinflammation contributed to the neuropathic pain and motor dysfunction following compression spinal cord injury. Brain Res Bull 143:217–224
Fakhri S, Dargahi L, Abbaszadeh F, Jorjani M (2019) Effects of astaxanthin on sensory-motor function in a compression model of spinal cord injury: involvement of ERK and AKT signalling pathway. Eur J Pain 23:750–764
Figley SA, Khosravi R, Legasto JM, Tseng Y-F, Fehlings MG (2014) Characterization of vascular disruption and blood–spinal cord barrier permeability following traumatic spinal cord injury. J Neurotrauma 31:541–552
Huang Y, Li S-n, Zhou X-y, Zhang L-x, Chen G-x, Wang T-h, Xia Q-j, Liang N, Zhang X (2019) The dual role of AQP4 in cytotoxic and vasogenic edema following spinal cord contusion and its possible association with energy metabolism via COX5A. Front Neurosci 13:584
Huang S, Jiang H, Hu H, Lv D (2021) Targeting AQP4 localization as a novel therapeutic target in CNS edema. Acta Biochim Biophys Sin 53:269–272
Ieong C, Sun H, Wang Q, Ma J (2018) Glycyrrhizin suppresses the expressions of HMGB1 and ameliorates inflammative effect after acute subarachnoid hemorrhage in rat model. J Clin Neurosci 47:278–284
Illarionova N, Gunnarson E, Li Y, Brismar H, Bondar A, Zelenin S, Aperia A (2010) Functional and molecular interactions between aquaporins and Na, K-ATPase. Neuroscience 168:915–925
Jin L-Y, Li J, Wang K-F, Xia W-W, Zhu Z-Q, Wang C-R, Li X-F, Liu H-Y (2021) Blood–spinal cord barrier in spinal cord injury: a review. J Neurotrauma 38:1203–1224
Kitchen P, Day RE, Taylor LH, Salman MM, Bill RM, Conner MT, Conner AC (2015) Identification and molecular mechanisms of the rapid tonicity-induced relocalization of the aquaporin 4 channel. J Biol Chem 290:16873–16881
Kumar H, Ropper AE, Lee S-H, Han I (2017) Propitious therapeutic modulators to prevent blood-spinal cord barrier disruption in spinal cord injury. Mol Neurobiol 54:3578–3590
Laird MD, Shields JS, Sukumari-Ramesh S, Kimbler DE, Fessler RD, Shakir B, Youssef P, Yanasak N, Vender JR, Dhandapani KM (2014) High mobility group box protein-1 promotes cerebral edema after traumatic brain injury via activation of toll-like receptor 4. Glia 62:26–38
Lee JY, Kim HS, Choi HY, Oh TH, Yune TY (2012) Fluoxetine inhibits matrix metalloprotease activation and prevents disruption of blood–spinal cord barrier after spinal cord injury. Brain 135:2375–2389
Liu X, Wang Y, Yang J, Liu Y, Zhou D, Hou M, Xiang L (2015) Anti-edema effect of melatonin on spinal cord injury in rats. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 159:220–226
Liu S, Mao J, Wang T, Fu X (2017) Downregulation of aquaporin-4 protects brain against hypoxia ischemia via anti-inflammatory mechanism. Mol Neurobiol 54:6426–6435
Masoudi A, Dargahi L, Abbaszadeh F, Pourgholami MH, Asgari A, Manoochehri M, Jorjani M (2017) Neuroprotective effects of astaxanthin in a rat model of spinal cord injury. Behav Brain Res 329:104–110
Nishibori M, Wang D, Ousaka D, Wake H (2020) High mobility group box-1 and blood–brain barrier disruption. Cells 9:2650
Noble LJ, Donovan F, Igarashi T, Goussev S, Werb Z (2002) Matrix metalloproteinases limit functional recovery after spinal cord injury by modulation of early vascular events. J Neurosci Res 22:7526–7535
Ohnishi M, Monda A, Takemoto R, Fujimoto Y, Sugitani M, Iwamura T, Hiroyasu T, Inoue A (2014) High-mobility group box 1 up-regulates aquaporin 4 expression via microglia–astrocyte interaction. Neurochem Int 75:32–38
Oklinski MK, Skowronski MT, Skowronska A, Rützler M, Nørgaard K, Nieland JD, Kwon T-H, Nielsen S (2016) Aquaporins in the spinal cord. Int J Mol Sci 17:2050
Oshio K, Binder D, Yang B, Schecter S, Verkman A, Manley G (2004) Expression of aquaporin water channels in mouse spinal cord. Neuroscience 127:685–693
Pan YI, Guo Y, Ma Y, Wang L, Sy Z, Mm L, Gc H (2019) Aquaporin-4 expression dynamically varies after acute spinal cord injury-induced disruption of blood spinal cord barrier in rats. Neuropathology 39:181–186
Pan Q-L, Lin F-X, Liu N, Chen R-C (2022) The role of aquaporin 4 (AQP4) in spinal cord injury. Biomed Pharmacother 145:112384
Papadopoulos MC, Verkman AS (2013) Aquaporin water channels in the nervous system. Nat Rev Neurosci 14:265–277
Park CS, Lee JY, Choi HY, Lee K, Heo Y, Ju BG, Choo H-YP, Yune TY (2020) Gallic acid attenuates blood-spinal cord barrier disruption by inhibiting Jmjd3 expression and activation after spinal cord injury. Neurobiol Dis 145:105077
Poon PC, Gupta D, Shoichet MS, Tator CH (2007) Clip compression model is useful for thoracic spinal cord injuries: histologic and functional correlates. Spine 32:2853–2859
Saini V, Lutz D, Kataria H, Kaur G, Schachner M, Loers G (2016) The polysialic acid mimetics 5-nonyloxytryptamine and vinorelbine facilitate nervous system repair. Sci Rep 6:1–12
Sandner B, Pillai DR, Heidemann RM, Schuierer G, Mueller MF, Bogdahn U, Schlachetzki F, Weidner N (2009) In vivo high-resolution imaging of the injured rat spinal cord using a 3.0 T clinical MR scanner. J Magn Reson Imaging Magn Reson Med 29:725–730
Sharma HS, Badgaiyan RD, Alm P, Mohanty S, Wiklund L (2005) Neuroprotective effects of nitric oxide synthase inhibitors in spinal cord injury-induced pathophysiology and motor functions: an experimental study in the rat. Ann N Y Acad Sci 1053:422–434
Sun L, Li M, Ma X, Feng H, Song J, Lv C, He Y (2017) Inhibition of HMGB1 reduces rat spinal cord astrocytic swelling and AQP4 expression after oxygen-glucose deprivation and reoxygenation via TLR4 and NF-κB signaling in an IL-6-dependent manner. J Neuroinflammation 14:1–18
Sun L, Li M, Ma X, Zhang L, Song J, Lv C, He Y (2019) Inhibiting high mobility group box-1 reduces early spinal cord edema and attenuates astrocyte activation and aquaporin-4 expression after spinal cord injury in rats. J Neurotrauma 36:421–435
Teng Z, Guo Z, Zhong J, Cheng C, Huang Z, Wu Y, Tang S, Luo C, Peng X, Wu H (2017) ApoE influences the blood-brain barrier through the NF-κB/MMP-9 pathway after traumatic brain injury. Sci Rep 7:1–8
Verkman A, Binder DK, Bloch O, Auguste K, Papadopoulos MC (2006) Three distinct roles of aquaporin-4 in brain function revealed by knockout mice. Biochim Biophys Acta Biomembr 1758:1085–1093
Wagner FC, Stewart WB (1981) Effect of trauma dose on spinal cord edema. J Neurosurg 54:802–806
Wang Z-R, Li Y-X, Lei H-Y, Yang D-Q, Wang L-Q, Luo M-Y (2016) Regulating effect of activated NF-κB on edema induced by traumatic brain injury of rats. Asian Pac J Trop Med 9:274–277
Zhang J, Takahashi HK, Liu K, Wake H, Liu R, Maruo T, Date I, Yoshino T, Ohtsuka A, Mori S (2011) Anti-high mobility group box-1 monoclonal antibody protects the blood–brain barrier from ischemia-induced disruption in rats. Stroke 42:1420–1428
Zhang XS, Zhang X, Zhang QR, Wu Q, Li W, Jiang TW, Hang CH (2015) Astaxanthin reduces matrix metalloproteinase-9 expression and activity in the brain after experimental subarachnoid hemorrhage in rats. Brain Res 1624:113–124
Zhang M, Cui Z, Cui H, Wang Y, Zhong C (2017) Astaxanthin protects astrocytes against trauma-induced apoptosis through inhibition of NKCC1 expression via the NF-κB signaling pathway. BMC Neurosci 18:1–12
Zhang X, Lu Y, Wu Q, Dai H, Li W, Lv S, Zhou X, Zhang X, Hang C, Wang J (2019) Astaxanthin mitigates subarachnoid hemorrhage injury primarily by increasing sirtuin 1 and inhibiting the Toll-like receptor 4 signaling pathway. FASEB J 33:722–737
Funding
This study was performed as a part of the Ph.D. thesis of Fatemeh Abbaszadeh. It was supported by a grant from the Department of Neuroscience of Iran University of Medical Science (Grant No. 18555) and the Neuroscience Research Center of Shahid Beheshti University of Medical Sciences (Grant No. 31278).
Author information
Authors and Affiliations
Contributions
F.A. was involved in the literature search, the data analysis, the conceptualization and design of the study, the graphic design and the drafting of the manuscript. S. R. was involved in performing MRI procedures and analyzing MRI data. M. J. (principal investigator), MT. J. and S. M. were involved in the conceptualization and design of the study, the critical revision of the manuscript for important intellectual content and the supervision of the study. The authors declare that all data were generated in-house and that no paper mill was used.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
All protocols for animal experiments were approved by the institutional animal Ethical Committee, the Iran University of Medical Sciences (IR.IUMS.REC.1399.1007).
Conflict of interest statement
The authors declared that they have no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Abbaszadeh, F., Jorjani, M., Joghataei, M.t. et al. Astaxanthin ameliorates spinal cord edema and astrocyte activation via suppression of HMGB1/TLR4/NF-κB signaling pathway in a rat model of spinal cord injury. Naunyn-Schmiedeberg's Arch Pharmacol 396, 3075–3086 (2023). https://doi.org/10.1007/s00210-023-02512-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00210-023-02512-7