
Abstract
Summary
We wanted to determine if there are any associations between birth factors and adult fracture risk. For women only, shorter birth length was associated with lower relative fracture risk. For women and men, individuals who were long at birth as well as tall in adulthood had a substantially higher relative fracture risk.
Purpose
We aimed to examine associations between birth anthropometry and adult fracture risk and to investigate if developmental mismatch is associated with fracture risk.
Methods
We included 4635 participants (476 women and 4159 men; born 1921–1950) with hospital and national registry-based data on birth anthropometry and adult fractures (≥ 50 years). We tested associations by Cox proportional hazards regressions and present hazard ratios (HR) with 95% confidence intervals.
Results
In total, 1215 (26%) suffered ≥ 1 fracture during a mean observation period of 26 years. In women, unadjusted analyses indicated that both higher birth weight (HR 1.42 per kg (1.10–1.84)) and birth length (1.10 per cm (1.05–1.17)) were associated to higher adult fracture risk. After adjustment (year of birth and gestational age), statistical significance remained only for birth length, HR 1.10 per cm (1.04–1.17). For men, no associations were apparent. We found no associations between developmental mismatch (lower birth weight followed by higher adult weight) and adult fracture risk. However, for both sexes, being born tall and staying tall into adulthood was associated with a markedly higher (55–105%) relative fracture risk (HR women 2.09 (1.18–3.68), men 1.55 (1.19–2.03)) compared to being born short and remaining short in adulthood.
Conclusion
In this study, being born shorter and lighter was associated with a lower risk for fractures ≥ 50 years in women. However, analyses indicated that tall adults who were also long at birth may be at markedly higher risk of fractures; this warrants further examinations.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Studies on birth weight and subsequent adult fracture risk have shown conflicting results. Byberg et al. studied the association between birth weight and fractures at the ages 50–94 years in two Swedish cohorts and were unable to find an association with incident fractures [1]. However, in a recent large study from the UK Biobank, including approximately 500,000 individuals, a Mendelian randomization analysis found that higher birthweight was causally associated with increased fracture risk [2].
Birth length as a determinant of fracture risk has only been investigated in a few studies. A study from New Zealand reported that birth length, but not birth weight, was positively associated with a prepubertal fracture risk ratio of 1.3 per standard deviation unit increase in birth length [3]. Another study from Brazil found that children with a higher birth length had a higher fracture risk (OR 1.6–1.8) from birth until 11 years of age compared to children with a shorter birth length [4].
According to the mismatch hypothesis, if the environment in early life including in utero is different from the environment encountered in later life, a developmental mismatch may occur and risks for certain cardiometabolic traits and diseases are increased, e.g., diabetes type 2 and obesity [5]. This is especially true for the antenatally low energy environment causing low birth weight later replaced by a postnatally high energy environment [5]. The fetal uterine environment has also been suggested to have an impact on adult bone health and fracture risk, e.g., by the programming of fracture risk and through epigenetic influences [6, 7].
Purpose
The aim of this observational, longitudinal study was to determine if there is an association between birth factors and fractures later in life and if developmental mismatch is associated to fracture risk.
Methods
Participants
In this study, participants from the Malmö Preventive Project (MPP) and the Malmö Diet and Cancer study (MDCS) with available birth parameters were included, please see the study flowchart in Fig. 1.

Flowchart for study inclusion for participants born 1921–1950 and participating in the Malmö Preventive Project (MPP) and Malmö Diet and Cancer Study (MDCS) with available birth data
The Malmö Preventive Project (MPP)
The Malmö Preventive Project is a cohort study that has been described in detail previously [8]. Between 1974 and 1992, men and women aged between 32 and51 years, and living in the city of Malmö, were invited to a screening examination including physical examination (e.g., weight (kg) and height (cm)), a self-administered questionnaire, laboratory tests, and mammography for all women over 45 years of age [8]. In total, 21,911 men and 8676 women attended the baseline screening with an overall attendance rate of 71.2%. Men were mostly screened during the first period of the study interval and women during a later period [8].
The Malmö Diet and Cancer Study (MDCS)
The prospective Malmö Diet and Cancer Study is another cohort study that has been described in full detail previously [9]. Between 1991 and 1996, inhabitants in the city of Malmö born between 1923 and 1950 (n = 74 138) were invited to participate in the study. Of the invited individuals, a total of 30,446 accepted the invitation that was sent out by postal mail and also via advertisements in newspapers and public places [9]. The baseline study included a questionnaire and a physical examination, e.g., measurement of weight (kg), height (cm), and measurements of waist and hip circumference (cm) [10]. The participants were given information about the study at a first visit during group meetings, and following signed informed consent anthropometric variables were measured individually [11]. Fourteen days later the participant returned with the filled-in questionnaire and went through the questionnaires with the study staff [12].
Data management
From the individual complete data sets of the two different cohorts, we created a new dataset including only participants with data on birth parameters. For a participant who participated in both studies (MPP and MDCS), the study in which the individual was included first was considered to reflect the baseline. One value of unlikely birth length of 64 cm was excluded [13, 14]. Nine values of unlikely gestational lengths: one < 140 days and eight > 335 days, respectively, were also excluded [15].
The Swedish Cause of Death Register (“Dödsorsaksregistret”) supplied data for causes of death until 2019 and Statistics Sweden (“Statistiska centralbyrån, SCB”) for dates of emigration and death until December 31, 2019. The National Prescribed Drug Register (“Läkemedelsregistret”) supplied information regarding prescribed medications from July 2005 until Dec 31, 2019. For fracture data, please see the separate section.
Baseline demographic data
Age (years) at baseline was calculated from birth date and date of inclusion in the study. Sex was extracted from every individual’s personal identification number. Weight (kg) and height (cm) as well as the waist (cm) and hip (cm) circumferences were measured at inclusion and were used to calculate body mass index (BMI) (kg/m2) and waist-hip ratio. Data in the questionnaires were self-reported. In the MDCS questionnaire, different response alternatives were given to each question, and the participant chose the appropriate alternative. For MPP, the response alternatives were yes/no. The different categories were as follows: level of education (did not finish 6-year elementary school, finished 6-year elementary school, finished 9-year elementary school, and finished high school or higher level); smoking status (regular smoker, occasional smoker, previous smoker, and never smoker); alcohol abstainer (yes/no); current snuff user (yes/no); marital status (unmarried, married/registered partner, divorced/separated from partner, and widow/widower/surviving partner); living alone (yes/no); self-reported stress during last year (yes/no); stress during the last 5 years (yes/no); use of the most commonly occurring medications (yes/no), see Online Resource 1a; diagnosis of the most commonly occurring diseases (yes/no), see Online Resource 1b; and history of previous fracture (yes/no).
Birth parameters
For the two cohorts, birth parameters including birth weight (kilogram), birth length (cm), head circumference at birth (cm), and gestational length at birth (weeks) were collected from midwives’ hospital charts, as described previously [16, 17]. Ponderal index (PI) was calculated using the formula weight (kg)/height3 (m).
The two studies that collected the birth data were two separate case–control studies studying either the effect of birth weight on either the risk of prostate cancer (from men in the MPP study) [17] or breast cancer (from women in the MDCS) [16]. No association between birth weight and future prostate cancer risk was observed in men [17], whereas for women, an increased breast cancer risk was observed in women with higher birth weight [16].
Military conscription data for men
Weight (kg) and height (cm) at military conscript testing were collected for men of the MPP study as reported previously and BMI (kg/m2) at conscription was calculated based on these values [17]. Conscript testing for the military service was compulsory for men in Sweden until 2010, and data were retrieved from the Swedish National Military Archives, Stockholm [17]. The military conscript testing was performed at a mean age of 19 years (range 16–22 years) [17].
Reproductive data for women
Data regarding reproduction were self-reported and included age at menarche (years), ever use of oral contraceptives (yes/no), duration of use of oral contraceptives (years), ever having given birth (yes/no), and total duration of breastfeeding (months). Age at menopause (years) was reported if having had occurred (yes/no). Ever use of menopausal hormone therapy (MHT) (yes/no) was reported as well as the duration of any use of MHT (years). Reproductive life span (years) was calculated by subtracting age at menarche (years) from age at menopause (years). Parity was reported as yes/no. Breastfeeding was self-reported, and the individual duration was reported per child, and all durations were added to a total sum of months. Regarding age at menarche, age at menopause, and duration of breastfeeding, data have been collected from either MPP or MDCS where available. The initial MPP questionnaires did not include any reproductive questions but these were added later; hence, women included early in the MPP study were not asked any of these questions.
Fracture data
Data on fractures were collected from national registries using the participants unique personal identification number. Data were retrieved from the National Patient Registry for in-patient data (“Slutenvårdsregistret, Socialstyrelsen”) between 1969 and 2019, for out-patient data (“Specialiserade Öppenvårdsregistret, Socialstyrelsen”) between 1997 and 2019, and supplementary regional data (“Specialiserade Öppenvårdsregistret, Region Skåne”) between 1973 and 2000. Multiple fractures sustained at the same event were considered as one fracture event. Several fractures sustained at different times (with a wash-out period of 6 months for identical fracture codes) were considered separate fracture events. Fractures were coded according to the International Classification of Diseases (ICD) versions 9 (1987–1997) and since 1998 according to ICD-10, see Online Resource 2 for details.
We included only fractures that occurred from 1987 and onwards and at an age of ≥ 50 years for the specific participant. The study start of 1987 was chosen since the coverage of the National Patient Register with its Inpatient Register is considered complete from this year and onwards [18]. This entails that a fracture may have occurred before an individual participant’s inclusion in the respective study cohort. For individuals included before 1987, the time period between inclusion and 1987 was truncated.
Statistical analysis
Continuous data are presented as means with standard deviations within brackets (SD). Categorical data are presented as the number of participants with percentage within brackets (%). To compare continuous variables between groups, we used the Students’ t-test for parametric data and the chi-squared test for categorical data.
Cox proportional hazards regression analysis
Cox proportional hazards regression analysis was performed for birth parameters as continuous variables separately for men and women. The Cox proportional hazards regression analyses were adjusted for the year of birth and gestational age at birth. For the Cox proportional hazards regression analysis, 50 years of age was considered as time zero. To model the effects of the effects of birth parameters on fracture events in adult life, we used an extended Cox proportional hazards model with recurrent events and robust standard errors, adjusted for year of birth and gestation week. In the model, non-proportionality was evident regarding the year of birth covariate. In order to solve this issue, we tried a model with a natural spline time-transformation function, allowing the effect of the year of birth to vary flexibly over time. This more complex model resulted in very similar estimates (data not shown) but made the output difficult to interpret. In the end, we therefore reverted to using the initial, more simplistic, Cox-model (without time-dependent covariates).
The results are presented as hazard ratios (HR) with a 95% confidence interval (CI). Plots showing relative fracture rates were constructed by first fitting a Cox proportional hazards model using a penalized spline basis for the predictor variable, then calculating the relative rate by dividing the predicted rate at each point with the center value.
Mismatch analysis was performed for birth weight, birth height, and body weight and height at baseline divided into tertiles with the following cut-offs for women: birth weight tertile 1 (T1) ≤ 3220 g and tertile 3 (T3) ≥ 3680 g; birth length T1 ≤ 50.0 cm and T3 ≥ 53.0 cm; body weight at baseline T1 ≤ 61.5 kg and T3 ≥ 71.0 kg; and height at baseline T1 ≤ 162.0 cm and T3 ≥ 168.0 cm. The corresponding values for men were as follows: birth weight T1 ≤ 3340 g and T3 ≥ 3780 g; birth length T1 ≤ 50.5 cm and T3 ≥ 53.0 cm; body weight at baseline T1 ≤ 73.0 kg and T3 ≥ 82.3 kg; and height at baseline T1 ≤ 174.0 cm and T3 ≥ 181.0 cm. Participants were then stratified into four subgroups depending on birth and baseline data: group 1 (birth data T1 and adult data T1), group 2 (birth data T1 and adult data T3), group 3 (birth data T3 and adult data T1), and group 4 (birth data T3 and adult data T3) performed for men and women separately. Cox proportional hazards regression analyses were performed as described previously. The incidence rate for multiple fracture events was calculated for men and women separately for the different mismatch groups regarding birth height and height at baseline.
Data management and statistical analyses
For data management and statistical analyses, we used IBM SPSS Statistics versions 25.0 and 28.0 (SPSS Inc., Chicago, IL, USA), SAS Enterprise Guide 8.3, and the R Stats packages version 4.1.2 with the survival package for the Cox proportional hazards regression analysis. All tests were two-sided and a p-value of < 0.05 was considered statistically significant.
Ethics approval and consent to participate
The original studies were approved by the Regional Ethics Committee in Lund (“Regionala Etikprövningsmyndigheten i Lund”) (MPP 85/2004 and MDCS LU 51–90). This project was approved by the steering board for the MDCS and MPP study cohorts (2016–017 #7 and 2016–008 #6, respectively). All participants of MDCS provided written informed consent, but this was not requested according to contemporary regulations at the MPP baseline screening 1974–1992. The study was conducted according to the guidelines of the Declaration of Helsinki.
Results
A total of 4635 participants (476 women and 4159 men) with available birth parameters were included in the study from the two original cohorts: MPP (n = 3681, 163 women) and MDCS (n = 954, 313 women). In total, 1215 (26.2%) of the participants experienced at least one fracture event. A larger proportion of women (37.8%) than men (24.9%) sustained at least one fracture. Descriptive baseline data for men and women with and without fracture are presented in Table 1.
Table 2 shows data regarding at birth, at military conscription (men only), and at cohort baseline. At birth, women with a future fracture had larger head circumference (p = 0.048) and were born after a slightly longer gestation (p = 0.003) compared to women without fracture, see Table 2. For men, we found a slightly shorter gestation length for men with fracture compared to men without fracture (p = 0.042). In both women and men, we found similar birth weight, birth length, and ponderal index at birth in those with and without fracture, see Table 2.
At military conscription, we found that men with a future fracture were taller than their counterparts but similar regarding body weight and BMI at conscription, see Table 2. At the study baseline, men with fracture were taller and had a higher waist-hip ratio compared to men without fracture during follow-up, while body weight and BMI seemed similar, see Table 2. For women, there was a non-statistically significant tendency (both p < 0.10) that women with fracture were thinner and taller than women without fracture, see Table 2.
For women, reproductive data are presented in Online Resource 3 separately for women with and without fracture. Among women with fracture, there were fewer ever-users of combined oral contraceptives, fewer that had given birth. Women with fracture had also used menopausal hormone therapy for longer periods of time compared to women without fracture, see Online Resource 3. We found similar age at menarche, duration of breastfeeding, duration of combined oral contraceptive use, age at menopause, ever-users of menopausal hormone therapy, and reproductive life span.
For women, increasing birth weight was associated with a higher relative risk for fracture, crude HR (95% CI) 1.42 (1.10–1.84), as was the birth length, crude HR (95% CI) 1.10 (1.05–1.17), see Fig. 2. In the adjusted Cox proportional hazards regression analysis for continuous birth parameters for women, an increasing birth length was associated with a higher relative risk for fracture HR (95% CI) 1.10 (1.04 – 1.17), see Table 3. For women, increasing birth weight seemed associated with increased risk for fracture of borderline statistical significance: HR (95% CI) 1.34 (0.995–1.81); p = 0.054, see Table 3. For men, we found no associations between birth parameters and fracture risk.


Relative fracture rates and crude hazard ratio (HR) with 95% confidence interval (CI) for A men and for B women born 1921–1950 and participating in the Malmö Preventive Project (MPP) and Malmö Diet and Cancer Study (MDCS). Included fractures occurred from 1987 and onwards at an age of ≥ 50 years of the participant. Relative fracture rates are shown separately for a birth weight, b birth length, c head circumference, and d ponderal index (kg/m.3) for fracture. Grey bands represent 95% confidence intervals. Vertical line represents the reference value (rounded mean value)
We found no associations between developmental mismatch and adult fracture risk, see Table 4. However, for both women and men, being born tall and remaining tall into adulthood was associated with a markedly higher (55–110%) relative fracture risk, HR women 2.09 (95% CI) (1.18–3.68), men 1.55 (95% CI) (1.19–2.03) compared to being born short and remaining short into adulthood. In men, being born long and belonging to the T1 for height in adulthood was associated to a 60% higher fracture risk: HR 1.5 (95% CI) (1.04–2.15). The incidence rate for multiple fracture events was calculated for men and women separately for the different mismatch groups regarding birth height and height at baseline, as shown in Online Resource 4. For both men and women, the incidence rate was the highest in the group of being born tall and remaining tall into adulthood, see Online Resource 4.
As a sensitivity analysis, the Cox proportional hazards regression analyses were performed for birth data as well as for the mismatch analysis excluding cancer cases thus only including female and male controls. The results are shown in Online Resource 5 and show similar results compared to including all participants with the addition that for male control participants being born small but being in the heavy as an adult was associated with a higher fracture risk: HR 1.4 (95% CI) (1.03–1.97), see Online Resource 5.
Relative fracture rates and crude hazard rates per examined trait are shown for men in Fig. 2A and for women in Fig. 2B. For men, we found similar rates per trait value for all examined traits. For women, a shorter birth length and lower birth weight were associated with lower relative fracture rates.
Discussion
This observational, longitudinal, and population-based study based on two cohorts from the same population examined the associations between birth parameters and adult fracture risk and found that for women, being born shorter was associated with lower relative fracture rate, not seen for men. For women, being born lighter was also associated with lower relative fracture rate, however not statistically significant in the adjusted Cox proportional hazards regression analysis.
In women, puberty in general occurs earlier than in men, and the earlier termination of bone lengthening and periosteal apposition leaves shorter and more slender bone than in men [19]. This results in differences between the female and male skeleton, with in general a smaller size in women and a skeleton that withstands aging less well [20]. During aging, the male skeleton also has a greater periosteal apposition, thus better compensating for age-related bone loss [20]. The timing of female puberty is influenced by body weight. In a Mendelian randomization study from 2022, the results suggest a causal effect between lower birth weight and earlier menarche as well as between higher childhood BMI and earlier menarche [21].
In a population-based cohort study of 31,971 Swedish men born in 1945–1961, it was observed that fracture risk was 15% higher in men with late pubertal timing compared with those with early puberty [22]. It may also be that being born heavy is associated to higher birth length [23], and this in turn predicts taller adult height which by itself, or via bone parameters, affects fracture risk. Birth length has, at least in men, been shown to be a stronger predictor of adult height and weight than birth weight [14]. It has also been shown that taller women have an increased risk of fracture in general and hip fracture in particular [24, 25], but also that fracture risk is site-specific in women and varies with body weight, height, and BMI [26]. Two studies, from New Zealand and Brazil, observed that birth length was positively associated with prepubertal fracture risk [3] and that children with a birth length of > 50.0 cm had an increased risk of fracture from birth until 11 years of age compared to children with a birth length < 46.0 cm [4]. To our knowledge, there is no previous study on associations between birth length and adult fracture risk.
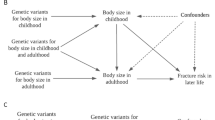
A recent Mendelian randomization study on BMI found that higher body size in childhood decreased fracture risk whereas higher body size in adulthood increased fracture risk [27]. The reasons for why birth weight and birth length may predict fracture risk differently during childhood, adolescence, and adulthood could be many and include, e.g., growth trajectories, nutrition, hormones, and timing of pubertal development [28]. In this study, however, we only have birth data and adult data and hence cannot include any childhood or adolescent weight or height data.
In the Cox proportional hazards regression analysis, the adjusted HR for fracture risk for women was of borderline significance (p = 0.054) and increased with increasing birth weight. In the crude analysis, lower relative fracture rates were observed for women being born small. Some reasons for this may be found among the causes of heavier birth weight. Maternal traits that increase the risk of fetal macrosomia are, e.g., higher age, maternal obesity, diabetes mellitus and hypertension, and being a non-smoker [29, 30]. A recent review found that a maternal diet including high fat intake and low intakes of calcium, phosphorus, and magnesium was associated with lower bone mineral density (BMD) in young adult offspring [31]. A Danish study observed that a maternal diet characterized by a high intake of fat, meat, and potatoes, but a low intake of fruit and vegetables, was associated to an increased risk of forearm fractures in the offspring [32]. A recent Finnish study on children born between 1998 and 2017 found that children born very preterm or with extremely low birthweight had a lower fracture incidence during childhood when compared to full-term children with normal birthweight. The authors speculated that this was due to a less fracture risk prone behavior in these children rather than early life factors [33].
In a recent observational study based on Mendelian randomization, a different effect of higher birth weight on adult bone area and BMC was observed, i.e., a higher birth weight predicted a higher effect on bone area than on BMC leading to a decreased adult BMD [34]. Two previous Swedish but smaller studies have also analyzed the effect of birth weight on BMC. Byberg et al. observed a positive association between birth weight and BMC [1], and Callréus et al. observed that lower birth weight was associated with lower BMC [35]. In the current study, we were unable to include analyses of BMC or BMD. We instead focused on the main outcome, i.e., fractures, and found that women born smaller were at lower relative fracture risk as adults. This is in line with the Mendelian randomization study on birth weight and fracture risk mentioned above [2].
In the current study, we found no such effect of developmental mismatch that low birth length followed by high adult height was associated to increased fracture risk. We, however, found that both men and women with birth length in the highest tertile and an adult height in the highest tertile corresponded to a higher fracture risk at ≥ 50 years of age. Whether this is due to the increased birth length, tall adult height, or a combination of both can only be speculated. Increased adult height has been shown, in another study from the UK Biobank, to be associated with increased fracture risk in men and women in both an epidemiological model: OR 1.19 (1.12–1.26), and a genetical model: OR 1.27 (1.17–1.39) [36]. This study substantiates this finding for women, but also further investigates the effect of birth length and adult height. For men, being born in the T3, but as an adult belonging to the T1 of body height, also increased fracture risk. It can only be speculated if this is a result of not growing according to one’s genetic potential due to disease or malnutrition (stunted growth), or if other causes could explain this observation. For every individual, reaching peak bone mass (PBM) is an essential determinant of future bone mass and is affected by, e.g., gender, ethnicity, genetic, and environmental factors [37]. If an individual does not attain the bone mass that the genetic potential entails, this could increase the risk of future fractures [37].
To further elucidate the mismatch analysis findings, we performed subsequent post-hoc adjusted Cox proportional hazards regression analyses for weight, height, and BMI at conscription (men only) and at basline (men and women separately). For men, increasing height at conscription was associated with higher relative fracture risk: HR 1.02 (95% CI) (1.01–1.02), and decreasing BMI at conscription was associated with lower relative fracture risk: HR 0.95 (95% CI) (0.92–0.99), whereas no effect of weight at conscription was identified (data not shown). At baseline, neither weight nor BMI was associated with an effect on fracture rates irrespective of sex (data not shown), whereas increasing height was associated with higher relative fracture rates: HR 1.01 (95% CI) (1.002–1.02) for men, and HR 1.03 (95% CI) (1.01–1.05) for women, respectively.
Strengths and limitations
This study has two important strengths. Firstly, fracture data were collected from national registries rather than being self-reported. Secondly, data regarding birth parameters were collected from hospital delivery records and were thus not self-reported [16, 17]. One of the limitations of the current study is that fewer women participated at baseline in the MPP study by design compared to the MDCS study. This is however due to the participation rates in the original study cohorts that were population-based. In the MPP, roughly 22,000 men and 11,000 women participated [8]. For the MDCS, the respective numbers were 11,000 men and 17,000 women [9]. Some of the participants participated in both cohorts and are only included once in this study. Two previous case–control studies abstracted birth data for participants of the original cohorts. The first of these studies by Lahmann et al. was focused on breast cancer risk in women from the MDCS and included 131 breast cancer cases with 345 age-matched controls [16]. The second study was performed by Gerdtsson et al. and included 1355 prostate cancer cases that were matched to date of birth within ± 1 year with 5271 controls from the MPP. Birth data were searched in midwifes reports for participants born at hospitals in the Skåne county of Sweden and two other major cities (Gothenburg and Stockholm) [16]. Hence, a risk of selection bias may be present, but we are unable to address the matter any further. Thus, we consider this study as exploratory, why the results need to be confirmed in larger population-based research cohorts. As a sensitivity analysis, the Cox proportional hazards regression analyses were performed including only female and male controls. The results remained the same.
The original studies are observational studies, and baseline data may not reflect values at later time-points, e.g., at the fracture event. In observational studies like the original studies, there is also always a risk of “the healthy cohort effect,” i.e., that healthier participants seek out participation in studies whereas eligible but not so healthy individuals to a larger extent choose not to participate for various reasons. For the MPP cohort, the total mortality was the same for the intervention and control group overall, but lower for participants under 40 years of age at entry in the study [8]. For the MDCS cohort, it was found that mortality was higher in non-participants than in participants both during recruitment and follow-up periods [38]. It was also observed that non-participants may have had a lower cancer incidence prior to recruitment but a subsequent higher incidence during the recruitment period [38].
The study cohort also reflects somewhat different time periods with more men included during the early study period and more women during the later study period [8]. During the study period, changes in care may have occurred with advances in intrauterine surveillance and neonatal care that might affect both the number of fetuses born alive and the number of surviving newborns, as well as the morbidity of the surviving newborns. In Sweden, national maternal health care was implemented in 1947 and further improved in 1955. This may affect the overall and specific health of the study participants differently (birth cohort effects). The measurement of length at birth might be more difficult than measuring, e.g., birth weight as birth length is dependent on the child stretching to its full length as not to underestimate its length. However, the measurement of the length of newborns has been shown to be reliable [39]. The fact that data on BMD were not available for any men and for only 194 women is a major limitation that rendered meaningful analyses futile. However, the notion of the classical osteoporotic fracture based on a low bone mineral density might be replaced by the notion that all fractures, both high-trauma and low-trauma, are to be considered risk markers for osteoporosis [40].
The non-proportionality of the Cox proportional hazards regression analysis could be considered a limitation of the study. However, in medical studies with a long follow-up period, the hazard ratio might not be constant from the start of the study until the end of the follow-up as this reflects the time-dependent nature of different diseases [41, 42]. For a given disease or condition, the hazards may change due to, e.g., given treatment or individual factors affecting the progression of the disease [41]. Hence, it can be argued that the hazard ratio from the Cox proportional hazards regression analysis should rather be interpreted as a weighted average of the true hazard ratios from the whole follow-up period [41] which is how we chose to interpret the Cox proportional hazards regression analyses of this study.
Conclusion
In conclusion, this longitudinal study shows that for women, shorter birth length is associated with a lower relative fracture risk while no such association was evident for men. We were unable to identify any traditional weight mismatch effects from birth parameters on adult fracture risk, i.e., higher risk for individuals who catch up from a low value at birth. However, for both women and men, being born in T3 of birth length and remaining in this tertile for tallness in adulthood was associated with substantially higher relative fracture risk (55–110%). This finding needs to be further explored in dedicated future studies.
Data availability
Restrictions apply to the availability of all data generated or analyzed during this study to preserve participant confidentiality. The corresponding author will on request detail the restrictions and any conditions under which access to some data may be provided.
References
Byberg L, Michaëlsson K, Goodman A, Zethelius B, Koupil I (2014) Birth weight is not associated with risk of fracture: results from two Swedish cohort studies. J Bone Miner Res 29:2152–2160
Yu XH, Wei YY, Zeng P, Lei SF (2021) Birth weight is positively associated with adult osteoporosis risk: observational and Mendelian randomization studies. J Bone Miner Res 36:1469–1480
Jones IE, Williams SM, Goulding A (2004) Associations of birth weight and length, childhood size, and smoking with bone fractures during growth: evidence from a birth cohort study. Am J Epidemiol 159:343–350
Hallal PC, Siqueira FV, Menezes AM, Araujo CL, Norris SA, Victora CG (2009) The role of early life variables on the risk of fractures from birth to early adolescence: a prospective birth cohort study. Osteoporos Int 20:1873–1879
Gluckman PD, Hanson MA, Low FM (2019) Evolutionary and developmental mismatches are consequences of adaptive developmental plasticity in humans and have implications for later disease risk. Philos Trans R Soc Lond B Biol Sci 374:20180109
Cooper C, Westlake S, Harvey N, Javaid K, Dennison E, Hanson M (2006) Review: developmental origins of osteoporotic fracture. Osteoporos Int 17:337–347
Holroyd C, Harvey N, Dennison E, Cooper C (2012) Epigenetic influences in the developmental origins of osteoporosis. Osteoporos Int 23:401–410
Berglund G, Nilsson P, Eriksson KF, Nilsson JA, Hedblad B, Kristenson H, Lindgarde F (2000) Long-term outcome of the Malmo preventive project: mortality and cardiovascular morbidity. J Intern Med 247:19–29
Manjer J, Elmståhl S, Janzon L, Berglund G (2002) Invitation to a population-based cohort study: differences between subjects recruited using various strategies. Scand J Public Health 30:103–112
Rosvall M, Persson M, Östling G, Nilsson PM, Melander O, Hedblad B, Engström G (2015) Risk factors for the progression of carotid intima-media thickness over a 16-year follow-up period: the Malmö Diet and Cancer Study. Atherosclerosis 239:615–621
Berglund G, Elmstähl S, Janzon L, Larsson SA (1993) The Malmo Diet and Cancer Study. Design and feasibility. J Intern Med 233:45–51
Byberg L, Gedeborg R, Cars T, Sundström J, Berglund L, Kilander L, Melhus H, Michaëlsson K (2012) Prediction of fracture risk in men: a cohort study. J Bone Miner Res 27:797–807
Sorensen HT, Sabroe S, Rothman KJ, Gillman M, Steffensen FH, Fischer P, Sorensen TI (1999) Birth weight and length as predictors for adult height. Am J Epidemiol 149:726–729
Eide MG, Oyen N, Skjaerven R, Nilsen ST, Bjerkedal T, Tell GS (2005) Size at birth and gestational age as predictors of adult height and weight. Epidemiology 16:175–181
Bergsjo P, Denman DW 3rd, Hoffman HJ, Meirik O (1990) Duration of human singleton pregnancy. A population-based study. Acta Obstet Gynecol Scand 69:197–207
Lahmann PH, Gullberg B, Olsson H, Boeing H, Berglund G, Lissner L (2004) Birth weight is associated with postmenopausal breast cancer risk in Swedish women. Br J Cancer 91:1666–1668
Gerdtsson A, Poon JB, Thorek DL et al (2015) Anthropometric measures at multiple times throughout life and prostate cancer diagnosis, metastasis, and death. Eur Urol 68:1076–1082
Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, Heurgren M, Olausson PO (2011) External review and validation of the Swedish national inpatient register. BMC Public Health 11:450
Seeman E (2008) Structural basis of growth-related gain and age-related loss of bone strength. Rheumatology (Oxford) 47(Suppl 4):iv2-8
Seeman E (2002) Pathogenesis of bone fragility in women and men. Lancet 359:1841–1850
Wang L, Xu F, Zhang Q, Chen J, Zhou Q, Sun C (2023) Causal relationships between birth weight, childhood obesity and age at menarche: a two-sample mendelian randomization analysis. Clin Endocrinol (Oxf). 98(2):212–220
Vandenput L, Kindblom JM, Bygdell M, Nethander M, Ohlsson C (2019) Pubertal timing and adult fracture risk in men: a population-based cohort study. PLoS Med 16:e1002986
Bertagnon JR, de Mattos Segre CA, Dall Colletto GM (2003) Weight-for-length relationship at birth to predict neonatal diseases. Sao Paulo Med J 121:149–154
Armstrong ME, Kirichek O, Cairns BJ, Green J, Reeves GK, Valerie Beral for the Million Women Study C (2016) Relationship of height to site-specific fracture risk in postmenopausal women. J Bone Miner Res 31:725–731
Xiao Z, Ren D, Feng W, Chen Y, Kan W, Xing D (2016) Height and risk of hip fracture: a meta-analysis of prospective cohort studies. Biomed Res Int 2016:2480693
Compston JE, Flahive J, Hosmer DW et al (2014) Relationship of weight, height, and body mass index with fracture risk at different sites in postmenopausal women: the Global Longitudinal study of Osteoporosis in Women (GLOW). J Bone Miner Res 29:487–493
Power GM, Tobias JH, Frayling TM, Tyrrell J, Hartley AE, Heron JE, Davey Smith G, Richardson TG (2023) Age-specific effects of weight-based body size on fracture risk in later life: a lifecourse Mendelian randomisation study. Eur J Epidemiol 38:795–807
Bonjour JP, Chevalley T (2014) Pubertal timing, bone acquisition, and risk of fracture throughout life. Endocr Rev 35:820–847
Jolly MC, Sebire NJ, Harris JP, Regan L, Robinson S (2003) Risk factors for macrosomia and its clinical consequences: a study of 350,311 pregnancies. Eur J Obstet Gynecol Reprod Biol 111:9–14
Boulet SL, Alexander GR, Salihu HM, Pass M (2003) Macrosomic births in the United States: determinants, outcomes, and proposed grades of risk. Am J Obstet Gynecol 188:1372–1378
Jensen KH, Riis KR, Abrahamsen B, Händel MN (2020) Nutrients, diet, and other factors in prenatal life and bone health in young adults: a systematic review of longitudinal studies. Nutrients. 12(9):2866
Petersen SB, Rasmussen MA, Olsen SF, Vestergaard P, Molgaard C, Halldorsson TI, Strom M (2015) Maternal dietary patterns during pregnancy in relation to offspring forearm fractures: prospective study from the Danish National Birth Cohort. Nutrients 7:2382–2400
Kuitunen I, Sund R, Sankilampi U (2023) Association of preterm birth and low birthweight with bone fractures during childhood. J Bone Miner Res 38(8):1116–1124
Xia JW, Zhang L, Li J et al (2022) Both indirect maternal and direct fetal genetic effects reflect the observational relationship between higher birth weight and lower adult bone mass. BMC Med 20:361
Callreus M, McGuigan F, Akesson K (2013) Birth weight is more important for peak bone mineral content than for bone density: the PEAK-25 study of 1,061 young adult women. Osteoporos Int 24:1347–1355
Lai FY, Nath M, Hamby SE, Thompson JR, Nelson CP, Samani NJ (2018) Adult height and risk of 50 diseases: a combined epidemiological and genetic analysis. BMC Med 16:187
Chevalley T, Rizzoli R (2022) Acquisition of peak bone mass. Best Pract Res Clin Endocrinol Metab 36:101616
Manjer J, Carlsson S, Elmståhl S, Gullberg B, Janzon L, Lindström M, Mattisson I, Berglund G (2001) The Malmö Diet and Cancer Study: representativity, cancer incidence and mortality in participants and non-participants. Eur J Cancer Prev 10:489–499
Doull IJ, McCaughey ES, Bailey BJ, Betts PR (1995) Reliability of infant length measurement. Arch Dis Child 72:520–521
Crandall CJ, Larson JC, LaCroix AZ, Robbins JA, Wactawski-Wende J, Johnson KC, Sattari M, Stone KL, Weitlauf JC, Gure TR, Cauley JA (2021) Risk of subsequent fractures in postmenopausal women after nontraumatic vs traumatic fractures. JAMA Intern Med 181(8):1055–1063
Stensrud MJ, Hernan MA (2020) Why test for proportional hazards? JAMA 323:1401–1402
Meuli L, Kuemmerli C (2021) The hazard of non-proportional hazards in time to event analysis. Eur J Vasc Endovasc Surg 62:495–498
Acknowledgements
We acknowledge support from Lund University Infrastructure grant “Malmö population-based cohorts” (STYR 2019/2046) as well as Statistics Sweden (“Statistiska Centralbyrån, SCB”) regarding data on dates of death or emigration.
Funding
Open access funding provided by Lund University. The work for the Malmö Diet Cancer Study (MDCS) was supported by grants from the Swedish Cancer Society (2684-B93_05XAA) and the Swedish Medical Research Council (B93-39X-09534-03C). The Malmö Preventive Project (MPP) was supported by the City of Malmö, the Swedish Medical Research Council, and the Swedish Heart- and Lung Foundation. The study was further funded by a FoU grant (Södra Sjukvårdsregionen) and an ALF grant (Vetenskapsrådet). LM was sponsored with a grant from the Sigrid Simonsson and Agni Olsson’s foundation, with the Alf Sjövall’s foundation. The study sponsors had no role in the design and conduct of the study, in the collection, analysis, and interpretation of the data, or in the preparation, review, or approval of the manuscript. The views expressed in this article are those of the authors and do not necessarily represent the views of the sponsors or authors’ affiliated institutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Moberg, L., Jehpsson, L., Nilsson, P.M. et al. Birth weight and birth length affect future fracture risk differently in men and women. Osteoporos Int (2024). https://doi.org/10.1007/s00198-024-07172-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00198-024-07172-8