
Abstract
Summary
This study, characterizing the incidence of hip fractures in Mexico, showed not only that the crude number of fractures has increased, but also there has been a decrease in fracture rates. Nonetheless, as the population ages in the coming decades, the current declines rate of could be expected to reverse.
Purpose
This study is to examine the incidence, rates, and time trends of hip fractures from 2006 to 2019 in Mexico. Additionally, an analysis of the follow-up of the birth cohorts was carried out.
Methods
Hip fractures registered during the period of the study were obtained through the Mexican Social Security Institute (IMSS) national discharge records. The incidence per 100,000 individuals was calculated from the IMSS population at risk. A time trend analysis was conducted using linear regression, and the identification of breakpoints in linear trends.
Results
There was an increase of hip fractures for both sexes ≥ 60 years (43% for women and 41%, for men). However, the rates diminished from 167.8/100,000 in 2006 to 138.5 /100,000 in the population 60 and over (1.9% and 0.9% per year in women and men respectively). When the information was analyzed by age groups, hip fracture rates were similar in both sexes but higher in women. The most significant contribution to the total number of fractures is due to the groups ≥ 70 years; people born before 1937 are accounting for the burden of fractures over the total data. In contrast, the younger generations appear to have lower rates.
Conclusion
Rates of hip fracture have steadily declined in Mexico since 2006; however, with the population aging in the coming decades, current rates declines could be expected to reverse.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Accordingly with the 2019 global, regional, and national burden of bone fractures (GBD 2019) [1], there were 178 million (95% UI 162–196) new fractures in the year 2019, an increase of 33.4% since 1990; 455 million of prevalent cases (an increase of 70.1%) and 25.8 million years lived with disability for this very same condition, also with a rise of 65.3% since 1990 [1]. Although these figures include fractures in both sexes and any age, in this same report, when numbers were disaggregated for age and sex, an exponential increase in the number of fractures after age 60 is notable, with a clear predominance of women (presumably, the majority of them were associated with bone fragility). The age-standardized rates of fractures in 2019 were 2292.2 incident cases per 100,000 population; a decrease of 9.6% in the standardized rates from the year 1990 was noted.
The decrease in hip fracture rates has been reported in several countries since the 1990s. Brauer et al. [2] reported the incident rates from Medicare claims in the USA from 1966 to 2004 and noticed a decrease in incident rates starting in 1994 in both sexes, more pronounced in the population over 84 years old. Leslie et al. [3] in Canada reported the same phenomenon where age-standardized rates of hip fractures decreased while the crude rate remained the same. Cooper et al. reported in England and, more recently Sweden and Chile analyzed the trends of hip fractures rates in these two countries finding that rates decreased significantly in both genders over time [4,5,6].
In Mexico, we reported the age and sex-specific rates of hip fracture between 2000 and 2006 [7], where we found that the age-specific incidence of hip fracture increased significantly in both sexes by 1% per year in the period of the study, finding 29,732 fractures by 2005, and projected an increment in these fractures of 155,874 by the year 2050 if no change in trends were expected. However, the trends in the rates of hip fractures, as noticed above by the different reports in other regions and countries over the globe have decreased. Hence, we decided to analyze the hip fracture incidence trends in a more extended period in our country to determine if changes in age- and sex-specific fracture rates have occurred in Mexico. The purpose of this study was to report the time trends of hip fractures in the population 50 and over from 2006 to 2019.
Methods
For this study, we gathered national data on hip fractures from the most extensive public health system in Mexico, the Mexican Institute of Social Security (Instituto Mexicano del Seguro Social (IMSS), as we did in 2011. The IMSS provides coverage for all formally employed workers and their families. Additionally, IMSS extends coverage to approximately 10 million people through IMSS Bienestar (formerly INSABI) including the informally employed. Therefore, the IMSS delivers health care to nearly 50% of the Mexican population [7]. For this analysis, we include information on the incidence of hip fractures from the years 2006 to 2019. The ICD-10 codes included were S72.0, S72.1 and S72.2. The data was gathered from the IMSS annual discharge database for each year of the study (SUI). This database follow the steps required from the Manual of Medical Indicators 2016 that contains the methodology for the construction and operation of the indicators of the Institutional Medical Area [8]. Fracture reporting methods remained unchanged during the study period. The incidence per 100,000 was calculated from the IMSS population at risk; therefore, the denominators were the population over 50 years old for each year of the study.
Fracture data was analyzed in three categories: people over 50 years of age, people over 60 years of age, and 5-year periods from 2006 to 2019.
To find out the time trend of the rates, we performed a time trend analysis using linear regression and identification of breakpoints in linear trends using join point analysis (Joinpoint Regression Program, Version 4.9.1.0. April 2022; Division of Applications and Statistical Research, National Cancer Institute, USA).
The temporal evolution of the number of fractures and the crude rates according to sex and at one year were plotted using MATLAB R2022b. In addition, a follow-up of the birth cohort of the different 5-year periods of age was carried out to establish which cohorts are currently causing the burden of fractures and, to evaluate the changes in the rates through the different age groups in the period of years analyzed.
Results
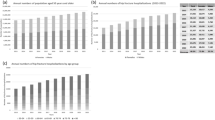
The number of fractures and the incidence rates in people older than 50 years from 2006 to 2019 are shown in Fig. 1.

Annual numbers (crude) and rates per 100,000 population of hip fractures
The number of hip fractures has been increasing in Mexico in women and men over 50 years, from 6357 in 2006 to 9028 in 2019, an increase of 42% and 40%, respectively. As reported elsewhere, women are more affected by this condition than men in an approximate ratio of 2:1. A positive percent change in the crude number of hip fractures is noted in both sexes. However, while the total number of fractures has increased, the fracture rates have decreased in men and women by 1.9% and 0.9% per year, respectively. Similarly, when considering the population over 60 years, there was an increase of 43% in women and 41% in men (Table 1).
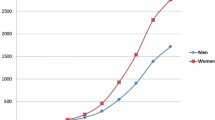
Figure 1 shows the number of hip fractures and incidence rates per 100,000 people older than 50 years. The bars represent the number of fractures in men and women (men gray and women pink), and the lines represent the rates. It is clear that while the number of fractures increases sustainably, the rates start to decrease in both sexes from the year 2011 and the rest of the study period. This decrease is more marked in women than in men. The rates dropped in women from 139.7 in 2006 to 109.2 in 2019/100,000 and in men from 83.3 to 70.6/100,000.
The join point analysis showed that the general rate of hip fractures (≥ 50 years) decreased in both sexes, in women by 1.9% per year, while in men, they decreased by 0.9% per year. These percentages are similar when the population over 60 years of age were analyzed separately; in this case, in women and men, they decreased by 1.9% and 0.5% per year between 2006 and 2019, respectively.
On the other hand, when the percentages of annual change in the rates for 5 years in women were reviewed, it was observed that in all these categories, there was an increase in the rates until approximately the beginning of the 2010. Then, the rates began to decrease in the nine different groups over 5-year periods. Similarly, although the overall percentage change for men decreased when reviewed, the percentage fluctuated, with increases and decreases occurring at different points in each 5-year age period (Table 2).
The results of the calculation from each year of follow-up for the individuals are presented in Fig. 2. The birth cohorts organized by 5-year stratum can be traced diagonally from left to right in the table. For example, individuals aged 50 to 54 from the first period (2006 to 2010) were born from 1952 to 1956 (indicated by the yellow color in the figure). These same individuals were between 55 and 59 years old during the following period (2011–2015), and are located one row down and one column to the right, starting from the top left column.

Incidence of hip fracture (rate/100,000) by 5-years birth cohorts in Mexican men and women by age and sex
When the information was analyzed by age groups, hip fracture rates were similar in both sexes but were higher in women. The most significant contribution to the total number of fractures occurs to the groups ≥ 70 years; individuals born before 1937 are responsible for the burden of fractures over the total data in men. Conversely, in women, the burden of fractures is more prevalent in those aged ≥ 65 years. In contrast, the younger generations of both sexes appear to have lower rates.
Discussion
This study provides an update on the trends in the risk of hip fracture in Mexico compared the previous study published in 2011 [7]; it presents the accumulated results between 2006 and 2019. During the 14 years of observation, a total of 171,488 hip fractures were recorded, of which nearly two-thirds occurred in women.
The results of this new analysis showed changes in the total number, as well as in the pattern of hip fracture rates that occurred in Mexico during this period of observation. In these observations, although there was an increase in the crude numbers of fractures in patients older than 50 years, a decrease in the incidence rates of fractures was observed simultaneously.
The Mexican population has increased the number of women and men aged 50 years and over between 81 and 66%, respectively, leading to an increase in the number of hip fractures in the period of 2006–2019 by \(\sim\) 40%. The increases were comparable to those observed in other countries such as the USA, China, and Finland [9,10,11,12,13,14].
Nonetheless, it is relevant to notice that a decrease in the rates of hip fractures between 15% in women and 22% in men was observed. Fracture rates declined faster during the second half of the study period. The turning point in this change in trends was around 2012; although it would be risky to say that the drop in these rates is linear due to the amount of data and the oscillations that these data present throughout the period, but the observed lower trends in hip fracture incidence appear to be consistent with previously observed phenomena in the USA, Sweden, the Netherlands, Finland, Norway, and France [14,15,16,17,18], and in Chile in the Latin American Region [6]. Mexico is not an exception; however, this phenomenon occurred more than a decade after its appearance in these other countries. As far as we are concerned, only Hong Kong and Taiwan seem to have continued the rise in hip fractures.
In the USA [19,20,21], the decrease in rates was reported between 1993 and 2003 among women and men aged 45 years and over, determining that both women and men decreased by around 20%. It has been estimated that this phenomenon began to occur in this country from the 1950s [22]. On the other hand, in Canada, the results published by Leslie et al. in 2009 [3] showed a decrease in hip fracture rates from 1996 with a percentage change per year of around 1.2%; somewhat similar to the percentage we found in the Mexican data.
In France, the incidence of hip fractures in people over 60 years of age decreased by 14% in women and 1.4% in men from 2002 to 2013 [23]. Likewise, the annual number of hip fractures (≥ 50 years) increased in both men and women in Sweden and Denmark until the mid-1990s, and after this year, the numbers began to decrease in both Swedish and Danish women [5].
In Latin America, Chile [6], reported a pattern of behavior similar to the one we have been describing in the other countries, observing an increase in the crude number of hip fractures in the population over 65 years of age, but at the same time presenting a decrease at rates of 1.4% per year in men and 0.9% per year in women. These figures are very similar to the results found in Mexico, with the only difference that in Chile, the period 2001–2019 was analyzed with people over 60 years of age, and our Mexican data begins 5 years later (2006–2019) in people over 50 years.
In the projections reported in our previous publication [7], an increase in the number of fractures had been predicted in the years following 2011; so, the decrease in hip fracture rates detected in the analysis presented here had not been anticipated in the outlook.
The results show that the burden of fractures in the health system is caused by people born approximately before and during the 1930s. Moreover, in the latest research, attempts have been made to investigate the effect of birth cohorts on these rate-reducing phenomena [5]. Age cohort effects can potentially influence the occurrence of osteoporosis. When studying age cohort effects, researchers examine how individuals who share a birth year or a similar range of birth years may exhibit similar characteristics, attitudes, and behaviors due to their shared exposure to special circumstances such as medical advancements and awareness, nutrition, dietary habits, and other lifestyle factors [24,25,26].
The phenomenon of declining fracture rates coincides with a simultaneous increase in the crude number of fractures. These phenomena can be attributed to several factors: first, the changing age structure in the population over the years, with an increasing number of older people at increased risk of hip fracture. This phenomenon is transitory since the population at risk is also more significant, and the rates will grow again in the future.
In the same way, different aspects could influence the reduction of fracture rates, including increasing awareness of osteoporosis among health professionals and the general population, recognizing it as a significant public health issue. Additionally, improved access to diagnostic equipment and patient follow-up studies involving densitometry have played a role. Similarly, access to diverse treatment for osteoporosis and to primary and secondary prevention programs has likely contributed. These previous factors would not explain the declines seen in men who have not initially been a priority group in medical campaigns for screening and treatment of osteoporosis. Besides, the care of patients with fractures has gradually changed in our country with the introduction of fracture coordinating units (FLS). To date, 33 FLS has been registered in the IOF capture the fracture map in Mexico (https://www.capturethefracture.org/map-of-best-practice). Additionally, the IMSS started the orthogeriatrics program in 2022, with plans to open 32 of these units in the near future. IOF Latino America is also delivering the Capture the Fracture mentorship program to selected geriatricians and orthopedic surgeons to help them adapt the model to their institution [27].
In addition, diet could affect the cohort effects since, between 1935 and 1950 in Mexico, several dietary patterns and nutritional practices were altered, potentially influencing the occurrence of osteoporosis and fractures. Socioeconomic changes during this period, including urbanization, may have controlled access to nutritious foods. For example, lower income individuals or those residing in urban areas might have had less access to nutrient-rich foods, which could have impacted on their overall nutrition and bone health [28].
It has also been suggested that the phenomenon of urbanization in developing countries could have some influence. It has been proposed that urbanization could lead people to reduce the time of adequate physical activity, thereby increasing body weight and the percentage of obesity in the population. Moreover, as it noted in the literature, an increased in BMD has been associated with a potentially protective factor against falls, but this information is quite controversial [29,30,31].
Nevertheless, the burden related to hip fractures is expected to increase over time as the proportion of frail older people at high risk of falls and fractures increases dramatically in the coming decades [26].
As described by Partida Bush and collaborators [32] from the National Council on Population of Mexico, the phenomenon of the aging process that is taking place in the population is mainly based on the decline in fertility from previous years. However, the reduction of mortality and the incidence of migration will be the most critical factors in the distant future, particularly beyond 2050, which will determine this structural change in the population that could cause an increase in the number of fracture rates again.
As we know, projections predict that by the year 2030, life expectancy will increase to 79.8 (77.5 for men and 82.1 for women) in 2030 and to 81.3 years (79.0 for men and 83.6 for women) in 2050 [32]. In addition, the displacement of economically active age groups to older ones leads to an unfavorable relationship between the productive and dependent population groups (known as the dependency ratio) [32]. The total dependency ratio will increase rapidly because of the aging process, reflected in the increase in the old-age dependency ratio. This would leave the country and our health systems in a situation of alert due to the economic burden that the increase in fractures will generate in the future [32, 33].
The limitations of this study include that only data from the databases of a single Health Institute (IMSS) were collected. However, in the other hand, the IMSS coverage is high (\(\sim 50\%\)) and covers all geographical areas making it representative of the Mexican population.
We included only data up to 2019 since during the COVID-19 pandemic, must of the hospitals were converted to COVID facilities receiving only patients with respiratory symptoms [34]. Consequently, the flow of patients with other comorbidities stopped, undoubtedly affecting the figures related to fracture care.
It should also be taken into account that one of the limitations of working with this type of database is the possibility of double-counting as readmissions for hip fracture within the same calendar year may lead to this error. However, the number of such cases could be attributed to the probability of subsequent fracture risk within 1 year after a hip fracture.
Finally, it should be considered that a more in-depth analysis of age-period-cohort effects was not conducted using the general APC model. Therefore, future studies that include data from additional years should consider implementing such analyses to gain a deeper understanding of the effects produced.
Conclusions
In the present study, incidence and temporal trends in the crude number and rates of hip fractures in Mexico are reported. Hip fracture rates in Mexico have consistently decreased since 2006, but the crude numbers have increased. This phenomenon is due to demographic changes in the age cohorts in the population. Since the population continues to age, in the coming decades this phenomenon will likely reverse which could place a burden on Mexican Healthcare Systems. Therefore, it is essential to strengthen prevention programs among the younger population.
Data availability
All the necessary data is presented in the article.
References
The Lancet Healthy Longevity (2021) Care for ageing populations globally. Lancet Healthy Longev 2(4):e180
Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB (2009) Incidence and mortality of hip fractures in the United States. JAMA 302(14):1573–1579
Leslie WD, O’Donnell S, Jean S, Lagacé C, Walsh P, Bancej C, Morin S, Hanley DA, Papaioannou A, Osteoporosis Surveillance Expert Working Group (2009) Trends in hip fracture rates in Canada. JAMA 302(8):883–889
Nordström P, Bergman J, Ballin M, Nordström A (2022) Trends in hip fracture incidence, length of hospital stay, and 30-day mortality in Sweden from 1998–2017: a nationwide cohort study. Calcif Tissue Int 111(1):21–28
Rosengren BE, Björk J, Cooper C, Abrahamsen B (2017) Recent hip fracture trends in Sweden and Denmark with age-period-cohort effects. Osteoporos Int 28(1):139–149
Ormeño JC, Martínez R, Frías C, Von Plessing C, Quevedo I (2022) Decreasing hip fracture rates among older adults in Chile, 2001–2019. Arch Osteoporos 17(1):26
Johansson H, Clark P, Carlos F, Oden A, McCloskey EV, Kanis JA (2011) Increasing age- and sex-specific rates of hip fracture in Mexico: a survey of the Mexican Institute of Social Security. Osteoporos Int 22(8):2359–2364
Instituto Mexicano del Seguro Social (2016) Manual metodológico de indicadores médicos, pp 1–452
Jaglal SB, Weller I, Mamdani M, Hawker G, Kreder H, Jaakkimainen L et al (2005) Population trends in BMD testing, treatment, and hip and wrist fracture rates: are the hip fracture projections wrong? J Bone Miner Res 20(6):898–905
Icks A, Haastert B, Wildner M, Becker C, Meyer G (2008) Trend of hip fracture incidence in Germany 1995–2004: a population-based study. Osteoporos Int 19(8):1139–1145
Chang KP, Center JR, Nguyen TV, Eisman JA (2004) Incidence of hip and other osteoporotic fractures in elderly men and women: Dubbo Osteoporosis Epidemiology Study. J Bone Miner Res 19(4):532–536
Brown CA, Starr AZ, Nunley JA (2012) Analysis of past secular trends of hip fractures and predicted number in the future 2010–2050. J Orthop Trauma 26(2):117–122
Zhang C, Feng J, Wang S, Gao P, Xu L, Zhu J et al (2020) Incidence of and trends in hip fracture among adults in urban China: a nationwide retrospective cohort study. PLoS Med 17(8):e1003180
Korhonen N, Niemi S, Parkkari J, Sievänen H, Palvanen M, Kannus P (2013) Continuous decline in incidence of hip fracture: nationwide statistics from Finland between 1970 and 2010. Osteoporos Int 24(5):1599–1603
Abrahamsen B, Vestergaard P (2010) Declining incidence of hip fractures and the extent of use of anti-osteoporotic therapy in Denmark 1997–2006. Osteoporos Int 21(3):373–380
Ballane G, Cauley JA, Luckey MM, Fuleihan GH (2014) Secular trends in hip fractures worldwide: opposing trends East versus West. J Bone Miner Res 29(8):1745–1755
Guilley E, Chevalley T, Herrmann F, Baccino D, Hoffmeyer P, Rapin CH et al (2008) Reversal of the hip fracture secular trend is related to a decrease in the incidence in institution-dwelling elderly women. Osteoporos Int 19(12):1741–1747
Dimai HP, Svedbom A, Fahrleitner-Pammer A, Pieber T, Resch H, Zwettler E et al (2011) Epidemiology of hip fractures in Austria: evidence for a change in the secular trend. Osteoporos Int 22(2):685–692
Gehlbach SH, Avrunin JS, Puleo E (2007) Trends in hospital care for hip fractures. Osteoporos Int 18(5):585–591
Kannus P, Niemi S, Parkkari J, Palvanen M, Vuori I, Järvinen M (2006) Nationwide decline in incidence of hip fracture. J Bone Miner Res 21(12):1836–1838
Chevalley T, Guilley E, Herrmann FR, Hoffmeyer P, Rapin CH, Rizzoli R (2007) Incidence of hip fracture over a 10-year period (1991–2000): reversal of a secular trend. Bone 40(5):1284–1289
Melton LJ, 3rd, Atkinson EJ, Madhok R (1996) Downturn in hip fracture incidence. Public health reports (Washington, DC : 1974) 111(2):146–50; discussion 51
Briot K, Maravic M, Roux C (2015) Changes in number and incidence of hip fractures over 12 years in France. Bone 81:131–137
Li S, Fan W, Zhu B, Ma C, Tan X, Gu Y (2022) Effects of age, period, and cohort on the prevalence of frailty in Chinese older adults from 2002 to 2014. Front Public Health 10:935163
Reither EN, Hauser RM, Yang Y (2009) Do birth cohorts matter? Age-period-cohort analyses of the obesity epidemic in the United States. Social science & medicine (1982) 69(10):1439–48
Yang Y, Land KC (2008) Age–period–cohort analysis of repeated cross-section surveys: fixed or random effects? Sociol Methods Res 36(3):297–326
Javaid MK, Calo M, Wullich S, Mohsin Z, Osorio EC, Orjuela AM, Cooper C (2023) Development, implementation and evaluation of a multinational FLS mentorship programme in Latin America. Osteoporos Int 34(11):1881–1891
Torres JMM, Aguilar LA (2015) Para una historia del cambio alimentario en México durante el siglo XX: El arribo del gas y la electricidad a la cocina. HIB: revista de historia iberoamericana 8(2):76–101
Looker AC, Melton LJ 3rd, Borrud LG, Shepherd JA (2012) Changes in femur neck bone density in US adults between 1988–1994 and 2005–2008: demographic patterns and possible determinants. Osteoporos Int 23(2):771–780
Khosla S, Atkinson EJ, Riggs BL, Melton LJ 3rd (1996) Relationship between body composition and bone mass in women. J Bone Miner Res 11(6):857–863
Leslie WD, Lix LM, Yogendran MS, Morin SN, Metge CJ, Majumdar SR (2014) Temporal trends in obesity, osteoporosis treatment, bone mineral density, and fracture rates: a population-based historical cohort study. J Bone Miner Res 29(4):952–959
Partida Bush V (2005) Demographic transition and the aging process in Mexico. Papeles de población 11(45):9–27
Wachs D, Roman-Urrestarazu A, Brayne C, Onrubia-Fernández J (2020) Dependency ratios in healthy ageing. BMJ Global Health 5(4):e002117
Doubova SV, Leslie HH, Kruk ME, Pérez-Cuevas R, Arsenault C (2021) Disruption in essential health services in Mexico during COVID-19: an interrupted time series analysis of health information system data. BMJ Global Health 6(9):e006204
Acknowledgements
We would like to thank the different departments of the Mexican Social Security Institute (IMSS who provided us with the data for the report of these analyses, as well as Berenice Araiza-Nava for her critical appreciation of the results obtained.
Author information
Authors and Affiliations
Contributions
G-A C-P, PC, and AB did research on the current panorama of the topic and wrote the introduction to the topic. RA R-P and VH B-A provided the data from the Mexican Social Security Institute and supported the discussion of results. G-A C-P performed the analysis of all fracture data, interpretation of results, and drafting of the final manuscript; PC contributed with the clinical relevance interpretation the results and discussion.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Conflicts of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Clark, P., Cruz-Priego, GA., Rascón-Pacheco, R.A. et al. Incidence of hip fractures in Mexico 2006–2019: increasing numbers but decreasing rates. Osteoporos Int 35, 1041–1048 (2024). https://doi.org/10.1007/s00198-024-07045-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-024-07045-0