
Abstract
Summary
Men and women with vertebral fractures due to osteoporosis are treated differently by society and health care professionals. This can lead to inequalities in health care and affects how men with fractures view themselves as people. We need to raise awareness that men get these fractures as well as women.
Introduction
There is a lack of research exploring the experience of osteoporosis from the male perspective. This study was undertaken to explore and describe the experiences of men with vertebral fractures due to osteoporosis, including their perceptions of diagnosis, treatment and changes in their sense of self.
Methods
The study consists of in-depth semi-structured interviews with nine male participants of the PROVE (Physiotherapy Rehabilitation for Osteoporotic Vertebral Fracture) study. Interviews were digitally audio recorded and fully transcribed. Data were coded in accordance with an interpretative phenomenological analysis approach to analyses.
Results
Three main themes are presented. (i) Osteoporosis is considered an old women’s disease. (ii) Men are diagnosed and treated differently than women in the NHS. Health care inequalities exist. (iii) Changes in self can occur in men after vertebral fracture/s due to osteoporosis.
Conclusions
Greater awareness that men get this condition is needed in both society in general and also by health care professionals who often do not expect osteoporosis to affect men. Approaches to diagnosis and treatment need to be considered and improved to ensure that they become appropriate and effective for men as well as women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vertebral fractures are the most common form of osteoporotic fractures and have been estimated to affect at least 20% of the older population, with incidence and prevalence increasing steadily with age [1,2,3]. Reported prevalence of vertebral fractures for people aged 50–80 years has shown slightly higher prevalence for women than men, ranging from 7 to 19% for women and 4–17% for men, depending upon how vertebral fracture has been defined in studies [4]. In addition to causing spinal deformity and alterations in spinal biomechanics [2, 5], vertebral fractures result in significant excess morbidity and mortality [1, 3, 6, 7]. These fractures have a considerable impact on people’s health-related quality of life due to pain, fatigue, low mood and limitations in activity and social participation [7, 8].
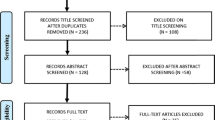
The PROVE trial (ISRCTN 49117867) evaluated the clinical and cost-effectiveness of two different physiotherapy programmes for people with osteoporotic vertebral fracture compared with one education session in the UK [9]. PROVE was a prospective, adaptive, multicentre (21 National Health Service (NHS) sites), assessor-blinded, three-arm randomised controlled trial (n = 615) and economic evaluation. PROVE included a qualitative study (n = 18) to explore the experiences and views of people with osteoporosis regarding their participation in the PROVE trial, their treatment interventions and adherence to the interventions [9]. Before the main trial started, a qualitative systematic review of patients’ experience of living with osteoporosis was undertaken that identified a lack of research exploring the experience of osteoporosis from the male perspective [10]. Of 773 participants included in this review, only 83 were men. The review suggested that osteoporosis is regarded as a women’s condition. This is likely to have an impact on men and women’s experience of living with osteoporosis and their decision to access health care [10]. Previous research has explored the experience of older men with osteoporosis attending an endocrinology department, finding negative psychological sequalae following diagnosis of osteoporosis including concern about future fracture and pain, limitations in treatment options and reluctance to take medications [11]. Previous research has also explored men’s experiences of living with osteoporosis and has identified the social construction of masculinity; men closely connected their ability to be physically active with their sense of self; they were fearful of weakness and constructed their identity through active decisionmaking in their health care management [12]. No studies have yet explored men’s experiences of having vertebral fractures due to osteoporosis. Nine men were interviewed as part of PROVE, and these interviews allowed us to explore their experiences of having vertebral fractures due to osteoporosis. The aim of this article is to explore and describe the experiences of men with vertebral fractures due to osteoporosis, including their perceptions of diagnosis, treatment and changes in their sense of self.
Methods
Participants
Men were eligible to participate in the PROVE trial if they were aged 18 or over and had a diagnosis of primary osteoporosis confirmed by radiograph or dual-energy X-ray absorptiometry (DEXA) scan (T-score − 2.5 SD below young adult mean) at the lowest lumbar level and at least one previous vertebral fracture due to osteoporosis. This qualitative study used purposive sampling and non-probability sampling to select a sample based on characteristics of a population and the objective of the study. We used this selective sampling approach to achieve a sample which included nine men of varying ages, with varying number/s and location/s of fracture from across a broad geographical area of England (UK). An interpretative phenomenological analysis (IPA) approach was used; this approach recommends involving small numbers of individuals to gain a rich and in-depth account [13].
Approaching and recruitment of participants
Potential participants were identified by the PROVE trial co-coordinator and posted invitations to participate in the qualitative study. Interviews were held at the homes of participants at a convenient time for them.
Interviews
Participants participated in in-depth semi-structured interviews. Written consent was obtained at the start of visits before interviews commenced. Where a spouse wished to attend and contribute to the interview, this was permitted and informed consent obtained from them (n = 1). An interview guide (supplementary file 1) was developed using data from the PROVE pilot (CML, KB); however, this was not followed rigidly: follow-up questions and probes were used to help the interview flow, ensuring that relevant areas were covered and allowing participants to introduce new areas of discussion they believed to be relevant [14]. The same experienced physiotherapy researcher completed all interviews (CML). One man became visibly upset during interview; the interview was not halted because the interviewee had participated in the interview to discuss and record this precise issue to try to help other people undergoing a similar experience. Participants were encouraged to discuss any areas they thought were relevant to their experiences of osteoporosis vertebral fracture, participating in PROVE and their perceptions about whether/how gender influenced their views. Time was spent after the interviews in everyday conversation to allow the interviewer to check the well-being of the interviewee [15]. Field notes and memos were recorded in a study diary. Interviews were digitally audio recorded and fully transcribed by CML, a health care secretary or a professional transcribing service. Following transcription, all transcripts were checked again against the recordings and transcribing errors corrected (CML).
Data analyses
Audio recordings were listened to and transcripts read until they became familiar. The data were coded in accordance with IPA [13]. Transcript data were broken down into discrete units, making concerted efforts to remain close to the data and continually explore meaning (CML). The first three transcripts were independently coded by two researchers (CML and KB), and codes were developed inductively. Discussion of these three transcripts agreed that, since similar coding units had been identified by both researchers, it was unnecessary in this instance for the other six transcripts to be independently coded. All transcripts were coded by one researcher who then grouped together units found to be conceptually similar into categories (CML). All categories, units and data for each unit were imported into NVIVO 11 software (CML) (NVIVO 11, QSR, Portsmouth, UK). The units, descriptors of the units and data for each unit were then checked (FT and KB) to ensure that the data fully supported the unit and category descriptors. The process of constantly comparing data, codes and categories occurred throughout all analyses, and the team met regularly to discuss data. Five randomly chosen transcripts were re-coded (by CML) at least 6 months after first coding to promote dependability. Field notes and reflexivity diary were used to refine the interview guide and identify/develop codes and questions that we wanted to explore in subsequent interviews. The use of independent coding, peer review, dependability and confirmability audits, a reflexivity diary, field notes and using an experienced researcher were all included to promote rigour [16].
Results
The characteristics for the male participants participating in the PROVE trial are presented in Table 1. Three main themes are presented. The first theme explores how osteoporosis is considered an old women’s disease and how this can cause difficulties for men. The second theme concerns how diagnosis and treatment were experienced by men in this study, and the third theme explores the changes in self that can occur after vertebral fracture/s due to osteoporosis. Figure 1 summarises the study findings.

Summary of study findings
Osteoporosis is considered an old woman’s disease
Osteoporosis is perceived to be an old women’s disease that “seems to hit women more than men obviously” (IV 2), and this led to people being surprised by their diagnosis “I was very surprised, I hadn’t thought of it as a man’s disease” (IV 6), “probably most men think this it’s not going to happen to them” (IV 2):
it’s always been women with osteoporosis, it’s not been noticed that men do until, well the last 10 years probably (IV 4)
I was quite surprised, you know, I was sort of, you know, not that old sort of bloke, you know, in reasonable health to get something which you associate with old ladies really, don’t you? (IV 8). A general perception is that “shrunken” old women have osteoporosis linked to their hormonal “kind of cycle” (IV 3), but as the wife of participant 1 observed, the same posture is assumed to be a sign of ageing in men rather than osteoporosis:
You see these little old men who have shrunk …people just don’t associate it with osteoporosis, they associate it with old age
Participants also describe how health care professionals were also more likely to attribute osteoporosis symptoms to muscular problems, to be baffled or to check for/or exclude sinister pathologies rather than suspect/expect OP “that expectation isn’t there with men”.
I went for the scans, “Oh, what are you doing here? But why? You’re a man.” Even within the hospital, there were people there who didn’t actually fully comprehend that it was a general problem, rather than just for women... it was a shock to them because so few men go through the system (IV 7)
they were a bit baffled as well that nothing had happened, there hadn’t been an incident or I’d fallen or... they did a number of tests and essentially he ruled out cancer, that was what he was really looking for (IV 8)
Whereas a postmenopausal woman with back pain may be assumed/clinically diagnosed to have OP as soon as they see their general practitioner (GP) and may not require a scan to establish the presence of OP “they just diagnose it” (IV 1). Participants felt that this was especially true when it is a younger man who is fit and active:
if I were a woman, in their 60’s who’d gone with back pain, the probably the doctor would immediately think this could be osteoporosis but with a man, that doesn’t happen does it, especially if it is a fit man (IV 1)
Not all of the men felt that OP was exclusive to women. One participant was not surprised because he did not think osteoporosis depended on sex “never occurred to me that would be any difference. I might tell you I am strangely pro women” (IV 5). Another participant wondered if, as the age of retirement increases, more men might be diagnosed with OP, especially those doing manual jobs, and “maybe there’ll be more men diagnosed, because of that” (IV 1).
A consequence of osteoporosis being considered a female condition is that some participants encountered disbelief from others when they are told about their diagnosis, even from family members “your mum, when you first told her you had got osteoporosis I don’t think she really believed it” (wife IV 1). This participant’s wife described how becoming aware he had osteoporosis had led to his sons becoming pro-active to prevent developing the condition themselves:
the boys…they probably wouldn’t have been as proactive in prevention, as they are because it’s their father that has got it, if you see what I mean (wife IV 1)
A couple of people spoke about telling friends/peers, whilst one participant’s good friends were easy to tell and “accepted it” (IV 7) accepting one participant has not told his friends except in response to someone discussing his wife’s osteoporosis which “only goes one way” downwards. He had not talked about it because osteoporosis is considered a women’s disease:
I haven’t mentioned it because it is thought of as a woman’s disease which is a bit stupid of me really but (IV 9).
Diagnosis and treatment as a man
In consequence to/as part of osteoporosis being considered a disease effecting old women, men describe being diagnosed and treated differently than women. Participants described a variety of routes to being diagnosed with vertebral fracture/s. A younger fitter man described quick diagnosis though because his GP suspected cancer “so within a week I went for a scan, MRI scan, which revealed two fractures” (IV 8). Other participants felt that health care professionals were slow to diagnose vertebral fractures because they were not expecting men to have osteoporosis and were surprised and even “shocked” (IV 7):
I think if GPs could be more aware that it could be, and talk to men about it… it could be flagged up. (IV 6)
Even within the hospital, there were people there who didn’t actually fully comprehend that it was a general problem, rather than just for women. (IV 7)
The consequences of this were perceived as important: if diagnosis was delayed until “years later”, then “it would’ve gone quite badly and I probably wouldn’t recover” (IV 7). Even when fracture/s were diagnosed, doctors were not expecting osteoporosis in male patients. Some felt that health care professionals initially did not do much to help; one participant eventually “decided to send myself up to the hospital to get an x-ray” (IV 4). Another participant underwent an MRI scan as part of an A&E visit for dizziness; his fracture was missed “no one spotted it”, and he raised the diagnosis with his GP on the advice of his doctor daughter-in-law (IV 9). His symptoms were considered “muscular doo dah” (IV 9), and this delayed him starting alendronic acid treatment for several years. He describes how he fractured L1 coughing in bed whilst ill, and his GP referred him for physiotherapy because he had not considered osteoporosis as a possibility. When referred for a course of treatment for osteoporosis, a participant also described how the osteoporosis course of treatment he attended was designed for older women rather than men and women “I did think crikey what am I doing here”:
I felt quite awkward about it because I was the youngest on the course and the others were all elderly ladies……the exercises were very basic compared to the exercises that I’d been doing…But even so I found that it helped a lot (IV 1)
He described that the physiotherapist adapted the programme and gave him “slightly more difficult exercises to do or a different level” (IV 1).
One participant described his perception of discrimination because of his gender. Although his consultant had prescribed him teriparatide, his local primary care Trust had refused to fund this:
I’ve written to NICE (UK National Institute for Health and Care Excellence) about it, and they say, we’re not saying it’s not good for men, we’re just saying the only tests we’ve done have been on women, so we can only recommend it for women (IV 1)
Despite appeals and the involvement of his Member of Parliament (MP), his consultant was still trying to get him this treatment:
our local MP wrote to the chief executive of NICE, and also the Chief Executive of (NAME) clinical commissioning Group and asked them both to do an investigation into my case, and they still came back and said No, it’s not justified (IV 1).
This participant and his wife spoke of their upset and distress; he found it “depressing” and “frustrating” and thought the decision was based on cost and the presence of a “postcode lottery”. Another participant, in a different geographical location, supports the presence of a “postcode lottery”. This participant was on teriparatide; he knows he has the “privilege” of being one of the first men to receive it and has had no further fractures since taking it. He appreciated the treatment was “not cheap” and had “to go through all sorts of processes” to get it.
The most important thing for me was that they then put me forward to go on this teriparatide
I know I am one of the first people who is a male to have this injection stuff…locally, whether it is nationwide or not, but I was certainly the first one here to have been given the privilege to get it (IV 3)
Another described that his Trust did not mind the cost of extensive treatments:
I know it’s quite expensive but they weren’t bothered, they don’t care about spending money here (IV 8).
Participants describe how inequalities of care exist, the treatment provided to men within the NHS is inconsistent and not all men can access treatments available to other men and women.’
Change in self
Participants described how having vertebral fractures due to osteoporosis can impact upon a man’s sense of self and change how he perceives himself. Participants described how getting an OP diagnosis can be a shock “And I didn’t see that coming at all…No I don’t think it made any kind of sense initially” (IV 1), and some described a conversion process from being capable to becoming dependent/having to take care. Changes in self were described as humiliating, involving a loss of dignity and a negative change in self-image. Some participants described how their wives now do more heavy jobs than previously, jobs that they would have always done before:
I don’t know if people actually realise how much impact it has on the family…. Because I have to do a lot more heavy things now than I used to. Not that I complain, no, but you do, there was a time that you would never have let me fetch a bag of logs in and a basket of logs and things like that. I have to do things like that now (wife IV 1)
When her husband tries to say he does more, his wife realises what she said and apologises “sorry I shouldn’t’ve said”. Several participants find changes in role hurtful, especially if they felt that their wives felt they “have” to do more, “I think she gets fed up sometimes” (IV 2) with this change in role. Several men also speak of the frustration of asking/seeing their sons take over their jobs from them, even if they accept they need the help or can modify their role and still be involved in the job or activity:
It is a bit frustrating, because simple things that I would have tackled, I give it to my son and he can do it (IV 6)
It is also hard for men to adjust to ask for/pay for help for things they previously easily achieved, and this is “a gender thing”:
It’s sort of humiliating really. The things I used to do which I can’t. Now that I know I’m paying other people to do (them) and stand by and watch some other bloke do it (IV 7)
For some, the potential impact of osteoporosis vertebral fracture upon sense of self was profound. One participant “was feeling what I could do to finish it all” and considered death by suicide due to pain and inability to be active and continue his previous activities (participant identity protected for this quote).
Modifying their activities helped participants to accept changes in self more easily. Having an understanding, caring family who also accepts the condition and who are willing to help enabled the men to adjust and accept their limitations more easily. The importance of an understanding family was emphasised by one participant:
If a spouse said that, “Men don’t get it. (osteoporosis) It’s not a problem. You just need to man up and get on with it,” I’d have done more damage to the back (IV 7).
Accepting help became easier when it was perceived as a natural part of progressively ageing. A 99–year-old participant described accepting help as a natural part of progressively ageing; in the early days, it is hard to accept help “you’re losing your dignity as a man” (IV 5), but as you age, you realise “you might as well accept it” (IV 5) and be grateful for the help offered. This gratefulness was also because “I am getting less and less confident of going out without a friend” (IV 5) with age. Sharing activities, e.g. housework after retirement, and working together as a team are perceived as a shared role by some participants “I do, toilets and all this type of stuff… (my wife) said “now you’ve retired…you can help out” (IV 3).
Changes in appearance, especially loss of height, can impact upon men “yes, it does affect me” (IV 7) and lead to self-consciousness and a negative impact on self esteem “your own feelings about yourself are not so good…it’s your own image of self” (IV 2), but then again, “as you get older, everybody gets shorter, and young people get taller”, and then, your son becomes taller than you (IV 7).
A few participants described risk taking, pushing the limits beyond the limits they believe/know to be safe to see how much they have changed, how much they can still do, or how effective a new treatment is, even if they know this is “stupid” and can cause harm:
I’m kind of pushing it a bit just to kind of see how far it can go without breaking something, which is stupid I know (IV 3)
I was doing too much. I was doing much too much in the garden of the heavy type of lifting, bending over. I wasn’t fit enough. I wasn’t doing the exercise I should be doing, and I came in one day and I was on ibuprofen painkillers for four or five days, knowing to bend and move properly (IV 7)
A few participants described how they had turned the “negative” of having vertebral fractures into something more positive to help them adapt to their changed self. Participant 4 developed osteoporosis as a consequence of alcoholism. After being given the choice by his consultant of stopping drinking or being dead in 6 months, he stopped drinking and had completely followed all the advice and treatment he was given by his consultant for his osteoporosis. He could now afford goods and take up new hobbies, like playing the guitar “something I always wanted to do” (IV 4) and which gave him great pleasure. Another participant looked for other things you can do so you can keep involved in activities/jobs:
‘No, I just can’t do it (heavy work) anymore. So, it’s frustrating, more than anything, but it doesn’t actually get you down…There are other things you can do. There are still ways you can get involved. (IV 7)
Humour was used to diffuse and deflect the impact of osteoporosis upon changes in self by many of the men in this study; they “laugh it off” even when discussing something severe/serious and use it as a coping strategy, even if they are unhappy about their osteoporosis:
I lost 2 inches in height which is not too bad because I’m still a bit taller than my wife so I don’t mind too much, you know.
Interviewer: What about if you had gone shorter than your wife?...
Oh well I would have had to have got high heels! That would have been good wouldn’t it! (IV 3)
Yeah. (laughter) But what can you do (about refracturing)? Well yeah, there’s no point, it’s annoying isn’t it really.
Does it get you down at all?
A bit, yeah. It’s a bit, yeah... It does really (IV 4)
A few participants used humour to make fun of the social view of men:
Like the typical man I am, I lift too much weight, I do it badly, etc., because we’re men, we can lift anything! (IV 7)
This use of humour also encompassed health in general; one person applies this to his cardiac surgery:
I make a joke when people ask about it and they said oh, do you have a double or a triple and I said no, real men have a quadruple (both laugh) (IV 9).
Humour/teasing was also used by this participant as a response when one of his peers made a negative comment about his wife’s osteoporosis:
I belong to a group of gentlemen… one of our number said the other day about his wife, “Well of course she’s got osteoporosis and that only goes one way” and I said, “Oh, thanks (Name)” (laughter).
Interviewer: How did you feel when he said that?
Well, I wasn’t overjoyed but I teased him about it and he was very embarrassed and he didn’t know I’d got it. (laughter) (IV 9)
Discussion
Summary of the main findings
This study is the first study exploring having vertebral fractures due to osteoporosis from the perspective of men. It has identified the impact and consequences of osteoporosis being considered an old women’s disease, unexpected for men and also by many health care professionals. The findings indicate that men and women are treated differently in the NHS and that inequalities of care exist. Diagnosis, unless a sinister cause for back pain is suspected, can be delayed. Treatment can also be delayed and tends to be targeted for women with one participant describing being refused a specific treatment due to their sex. Changes in self were described by participants, from being physically active to becoming less active/dependent and needing to change, or modify, their roles within their family and social groups. The potential impact of osteoporosis vertebral fracture upon sense of self should not be underestimated. Humiliation and frustration were described by participants, with one participant describing how changes in role and pain had led to him considering death by suicide.
How the study findings fit in, and add to, the existing evidence
The findings support the suggestion from our earlier review that osteoporosis is considered to be a women’s condition and that this has an impact on men’s decision to access health care [10]: we also show that this can have an impact on how men are treated in health care. Health care professionals cannot ignore the influence of gender, and Toye et al. make a call to get “gender on the health care agenda” [17]. Gender is not the same as biological sex; it refers to the socially ascribed and experienced aspects of being “female,” “male” or “other” [18]. Our gender incorporates what constitutes our “maleness” or “femaleness” in society. The findings of this study support the idea that a person’s ascribed gender can profoundly affect their experience of illness, and this can have serious repercussions on access and utilisation of health care [19]. This may help to explain why men are more susceptible to serious illness and live shorter lives than women [20].
Theories of gender can help us to understand men and women’s differential responses to health and illness [21, 22]. The findings of this study resonate with studies that demonstrate that men tell different stories about their bodies and tend to distance themselves from female-gendered stories [23, 24]. The findings also support studies that show that the capacity to laugh at yourself and not take things too seriously is highly valued by men [17, 19]. An exploration of the gendered experience of health and illness can have important clinical implications, and further gender-specific qualitative studies on specific conditions would facilitate provision of the most appropriate health care. Importantly, men and women do not always share the same experience of health and illness, and we need to consider this in provision of service. Gendered identity is an important aspect of who we are, and health care is likely to be more effective if it does not threaten a person’s sense of being male or female [25]. The need for interventions that fit gendered perspectives has been demonstrated in this study. Gender issues in health care are becoming more visible in society, and the need for gender identity data to understand inequality, inform and monitor policy development and allocate services for people in the UK has been identified [26].
Although there are no previous qualitative studies exploring osteoporosis vertebral fracture/s in men, the findings of this study support an earlier review about older men’s knowledge about osteoporosis. Gaines and Marx (2011) identified that community-dwelling older men know little about osteoporosis and its risk factors and prevention. They highlighted the scant research addressing the prevention, screening and education of men about osteoporosis and the need for innovative educational interventions to be developed and evaluated to influence the prevention and adverse consequences of osteoporosis [27]. In addition, since some participants in this study described how health care professionals were surprised by men having vertebral fractures due to osteoporosis, there is also a need to educate health care professionals and improve awareness about osteoporosis in men. The data from the observational osteoporotic fractures in men study (MrOS) identified that 2% (using World Health Organisation reference female-specific T-score) and 7% (using US National Osteoporosis male-specific T-score) of older men (aged 65 years or older) had osteoporosis when they entered the study [28]. The study demonstrated that lower bone mineral density in older men is associated with higher fracture risk, that bone loss increases with advancing age and that “high trauma” fractures are considered due to osteoporosis because of their association with low bone mineral density and increased risk of future fracture [28]. The rate of clinical vertebral fractures of men followed for 4.7 (average) years was 1% (61/5994), and our study supports its findings that it is important to recognise, treat and prevent osteoporosis in men [28].
Strengths and limitations
The purposive sampling used in this study achieved a sample of men of varying age and varying levels of being physical active and spread across a wide geographical area of England. We believe that this enabled us to capture wide-ranging views, perceptions and experiences from the study participants. It is recognised however that the study drew on a relatively small sample of English-speaking participants. These participants had previously volunteered to participate in the PROVE trial and subsequently also volunteered again to participate in the qualitative study. It is known that there are differences between those willing to participate in medical research studies and those not willing to participate [29]. Participation in PROVE may have influenced the views participants held about vertebral fractures and osteoporosis; however, it was beyond the scope of this study to explore how participation in a trial may influence views and beliefs. For these reasons, there may be aspects of men having vertebral fractures due to osteoporosis missing from this study. The research also took place in one health care setting, the NHS in England. Further research is required to explore the factors identified in this study and to explore these factors in non-NHS settings and other countries. We also acknowledge that interviews with a couple may have influenced their responses and provide different findings than those with a single interviewee; however, when people wanted to participate as a couple, we did not wish to refuse this request.
Summary and conclusion
Men and women are treated differently in the NHS health care setting. Health care inequalities exist. Awareness that men have vertebral fractures due to osteoporosis is lacking. Much greater awareness that men get this condition, that osteoporosis is not solely an old women’s disease, is needed in both society in general and also by health care professionals who often do not expect osteoporosis to affect men. Approaches to diagnosis and treatment need to be considered and improved to ensure that they become appropriate and effective for men as well as women.
References
Svedbom A, Hernlund E, Ivergard M, Compston J, Cooper C, Stenmark J et al (2013) Osteoporosis in the European Union: a compendium of country-specific reports. Arch Osteoporos 8(1–2):136
Kendler DL, Bauer DC, Davison KS, Dian L, Hanley DA, Harris ST, McClung MR, Miller PD, Schousboe JT, Yuen CK, Lewiecki EM (2016) Vertebral fractures: clinical importance and management. Am J Med 129(2):221 e1–221 10
Puisto V, Rissanen H, Heliovaara M, Impivaara O, Jalanko T, Kroger H et al (2011) Vertebral fracture and cause-specific mortality: a prospective population study of 3,210 men and 3,730 women with 30 years of follow-up. Eur Spine J 20(12):2181–2186
Melton JL III, Kallmes DF (2006) Gaines and Marx epidemiology of vertebral fractures: implications for vertebral augmentation. Acad Radiol 13:538–545
Broy SB (2016) The vertebral fracture cascade: etiology and clinical implications. J Clin Densitom 19(1):29–34
Ong T, Kantachuvesiri P, Sahota O, Gladman JRF (2018) Characteristics and outcomes of hospitalised patients with vertebral fragility fractures: a systematic review. Age Ageing 47(1):17–25
Sanchez-Riera L, Wilson N (2017) Fragility fractures & their impact on older people. Best Pract Res Clin Rheumatol 31(2):169–191
Svedbom A, Borgstom F, Hernlund E, Strom O, Alekna V, Bianchi ML et al (2017) Quality of life for up to 18 months after low-energy hip, vertebral, and distal forearm fractures-results from the ICUROS. Osteoporos Int 29:557–566. https://doi.org/10.1007/s00198-017-4317-4
Barker KL, Javaid MK, Newman M, Minns Lowe C, Stallard N, Campbell H, Gandhi V, Lamb S. Physiotherapy Rehabilitation for Osteoporotic Vertebral Fracture (PROVE): study protocol for a randomised controlled trial. Trials2014;15:22
Barker KL, Toye F, Minns Lowe CJ (2016) A qualitative systematic review of patients’ experience of osteoporosis using meta-ethnography. Arch Osteoporos 11:33
Solimeo SL, Weber TJ, Gold DT (2011) Older men’s explanatory model for ospteoporosis. The Gerontologist 51(4):530–539
Nielsen DS, Brixen K, Huniche L (2011) Mens’ experiences of living with osteoporosis: focus group interviews. Am J Mens Health 5:166–176
Smith JE, Osborn M (2008) Interpretative phenomenological analysis. In: Smith JA (ed) Qualitative Psychology: A Practical Guide to Methods, 2nd edn. Sage, London
Rubin HJ, Rubin IS (1995) Qualitative interviewing. The art of hearing data. Sage Publications, Thousand Oaks
Morse JM, Stern PN, Corbin J, Bowers B, Charmaz K, Clarke AE: Developing grounded theory. The second generation. Walnut Creek,: Left Coast Press, Inc; 2009:p.84
Krefting L (1991) Qualitative research: the assessment of trustworthiness. Am J Occup Ther 45:214–222
Toye F, Room J, Barker KL (2018) Do I really want to be going on a bloody diet? Gendered narratives in older men with painful knee osteoarthritis. Disabil Rehabil 40(16):1914–1920
Johnson JL, Greaves L, Repta R (2009) Better science with sex and gender: facilitating the use of a sex and gender-based analysis in health research. Int J Equity Health 8:14
Gill R, Henwood K, McLean C (2005) Body projects and the regulation of normative masculinity. Body Soc 11:37–62
Courtenay W (2011) Dying to be men. Routledge, East Sussex
Connell RW, Messerschmidt JW (2005) Hegemonic masculinity: rethinking the concept. Gend Soc 19:829–859
Bernardes SF, Keogh E, Lima ML (2008) Bridging the gap between pain and gender research: a selective literature review. Eur J Pain 12:427–440
Brink P, Ferguson K (1998) The decision to lose weight. West J Nurs Res 20(1):84–102
Monaghan L (2007) Body mass index, masculinities and moral worth: men's critical understanding of ‘appropriate’ weight-for-height. Sociol Health Illn 29(4):584–609
Monaghan LF, Malson H (2013) ‘Its worse for women and girls’: negotiating embodied masculiniteis through weight-related talk. Crit Public Health 23:304–319. https://doi.org/10.1080/09581596.2012.754843
Office for National Statistics. Accessed 13/12/2018. https://www.ons.gov.uk/methodology/classificationsandstandards/measuringequality/genderidentity/genderidentityupdate
Gaines JM, Marx KA (2011) Older men’s knowledge about osteoporosis and educational interventions to increase osteoporosis knowledge in older men: a systematic review. Maturitas 68:5–12
Cawthorn PM, Shahnazari M, Orwoll ES, Lane NE (2016) Osteoporosis in men: findings from the osteoporotic fractures in men study (MrOS). Therapeutic advances in musculoskeletal disease 8(1):15–27
Trauth JM, Musa D, Siminoff L, Jewell IK, Ricci E (2000) Public attitudes regarding willingness to participate in medical research studies. J Health Soc Policy 12(2):23–43
Acknowledgments
The assistance of the trial co-ordinators for the PROVE study, Varsha Gandhi and David Smith, in identifying and approaching potential participants for this study is gratefully acknowledged. We would also like to thank all the participants in this study for their help and time telling us about living with osteoporosis vertebral fracture/s; it is greatly appreciated.
Funding
This research was funded by the National Institute for Health Research Health Technology Assessment scheme, HTA Project Reference 10/99/01.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 25.8 kb)
Rights and permissions
About this article

Cite this article
Minns Lowe, C.J., Toye, F. & Barker, K.L. Men’s experiences of having osteoporosis vertebral fractures: a qualitative study using interpretative phenomenological analyses. Osteoporos Int 30, 1403–1412 (2019). https://doi.org/10.1007/s00198-019-04973-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-019-04973-0