
Abstract
Summary
We examined how patient beliefs, values, and preferences (BVPs) were included and conceptualized in international osteoporosis guidelines. The majority of guidelines did not mention BVPs. When mentioned, BVPs were conceptualized as preference for one medication over another. A broader conceptualization and inclusion of BVPs should be incorporated in osteoporosis guidelines.
Introduction
Our objectives were to determine (1) the extent to which osteoporosis guidelines reflected patients’ beliefs, values, and preferences (BVPs); (2) how BVPs were conceptualized; and (3) the methods used to elicit BVPs in the references cited by the guidelines.
Methods
We conducted a document analysis of English-language international osteoporosis guidelines based on the International Osteoporosis Foundation website. We examined each guideline and extracted all instances of statements pertaining to BVPs. The statements were reviewed by two independent researchers. Discrepancies in data extraction were resolved by the first author. We developed categories based on five common elements that represented the BVP statements.
Results
Twenty-seven of 70 (39%) guidelines included 95 statements about patient BVPs. Of the 95 statements, 32 statements (14 guidelines) were classified under BVP related to the choice of pharmacotherapy or general treatment, 10 (7 guidelines) under BVP related to adherence to pharmacotherapy or treatment in general, 5 (5 guidelines) under BVP related to financial costs and benefits, 43 (19 guidelines) under other BVP mentioned but not supported by a reference to a primary study or systematic review, and 5 (3 guidelines) under other BVP mentioned and supported by at least one reference to a primary study or systematic review. Twenty-nine references were cited to reflect the BVPs mentioned, including an editorial and quantitative studies.
Conclusions
Twenty-seven (39%) of the guidelines included mention of patients’ BVPs. In 19 guidelines, the importance of BVPs was mentioned but these statements were not supported by references to a primary study or systematic review. BVPs were most often (14 guidelines) conceptualized as preference for one medication over another. We suggest that qualitative data be included as evidence of BVPs in guidelines.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Patients’ beliefs, values, and preferences (BVPs) are fundamental tenets of evidence-based practice [1, 2] and the development of clinical practice guidelines [3]. BVPs have been shown to determine patients’ acceptance of clinical guidelines which in turn may affect patients’ behaviors and outcomes [4] and physicians’ adherence to those guidelines [5]. Patient preferences are also one component of building consensus about treatment in shared decision-making during the medical encounter [6].
There appear to be inconsistencies in how the terms “beliefs, values, and preferences” are defined. The terms “values and preferences” are often the concepts highlighted [7] and sometimes “beliefs” have been incorporated under the term “preference” [8]. Patient “values and preferences” has been defined as the “underlying processes we bring to bear in weighing what our patients and our society will gain or lose when we make a management decision” (p. 1291) [7].
Montori and colleagues consider patient preferences as an overarching term that includes patient perspectives, beliefs, expectations, and goals for health and life, and also to the process used by individuals in considering the potential benefits, harms, costs, and inconveniences of management options in relation to one another [8]. Patient preferences have been conceptualized as preferences for any type of treatment such as counseling, exercise, and surgical techniques [9] and preferences for medication [10, 11]. In one study, Utens and colleagues [12] reported that the definition of preference differed for patients and for guideline developers; patients defined preferences as their views and wishes in terms of treatment, whereas guideline developers defined preferences in terms of treatment choices. Thus, the wishes of patients to take or not take medication are conceptually different than the wishes of patients to take one medication over another.
Regardless of the definition of BVPs, there has been a call to include patients and their preferences in guideline development in conditions such as infertility [13] and kidney disease [14] because patients and providers have different clinical issues of concern [13] and different priorities [14]. Previous authors have reviewed clinical practice guidelines for treatment thresholds [15], declarations and conflicts of interest [16], and whether recommendations are supported by evidence [17]. We are not aware of any comprehensive reviews of patient BVPs in clinical practice guidelines for a particular disease group, such as osteoporosis.
We believe that an examination of BVPs in clinical practice guidelines is important for several reasons. Because BVPs are fundamental to the development of clinical practice guidelines [3], it is important to determine if, and how, they are included in guidelines. Further, because clinical decisions are value-laden [7], we believe it is important to examine how BVPs are described in these guidelines and whether there are common elements to the descriptions. Our objectives were to determine (1) the extent to which osteoporosis guidelines reflected patients’ BVPs, (2) how patients’ BVPs were conceptualized, and (3) the methods used to elicit BVPs in the references cited by the guidelines.
Methods
We conducted a document analysis [18] of English-language osteoporosis guidelines based on the International Osteoporosis Foundation (IOF) website (www.iofbonehealth.org/). As a non-profit organization, the IOF promotes the maintenance of bone, muscle, and joint health as a worldwide priority. Using the IOF website as a source of guidelines promoted the inclusion of guidelines written as reports. These guidelines may not have been captured through a search of the scientific databases such as PubMed. The IOF also produces educational resources to advance understanding of osteoporosis and related musculoskeletal disorders, and promotes medical innovation and improved patient care.
The purpose of the document analysis was to review, interrogate, and analyze the text in the guidelines which was considered our primary source of data [18]. These guidelines were considered an “authoritative source” under the assumption that they were produced as “unbiased knowledge” [18]. As individual countries update their clinical practice guidelines regularly, the document analysis was conducted on guidelines posted on the International Osteoporosis Foundation website as of May 10, 2018.
We examined each guideline and extracted all instances of statements (or related consecutive statements) pertaining to BVPs. The statements within each guideline were reviewed by two independent researchers (AM, FN) who met with each other regularly to discuss their independent extractions, and then with the first author to discuss the data overall. Discrepancies in data extraction (for example, how many of the consecutive statements were relevant) were resolved by the first author. After significant review of the statements as a team, we developed the following categories based on five common elements that appeared to represent BVP statements in the guidelines. Under the supervision of the first author, three of the researchers (AM, FN, WY) worked together to assign the statements into the five categories. The final assignment of the statements was reviewed and approved by the first author.
BVP related to the choice of pharmacotherapy or general treatment
This classification included patient BVPs about a specific medication or medications or general treatment for osteoporosis, including calcium and vitamin D. These statements were sometimes supported by references to other studies that included information related to side effects of specific treatments and information related to the efficacy of a particular medication or treatment option.
BVP related to adherence to pharmacotherapy or treatment in general
This classification included statements that linked patients’ BVPs to adherence and to patients’ ability to comply with their medications or treatment recommendations in general.
BVP related to financial costs and benefits
This classification included patient BVPs that addressed financial costs and benefits of treatment, either to the patient and/or to society. If a statement or cluster of statements considered the socioeconomic status of patients when recommending therapeutic interventions such as medication and surgery, these statements were included under this classification.
Other BVP mentioned but not supported by a reference to a primary study or systematic review
This classification was assigned to statements that mentioned patient BVPs in general but were not supported by references to a primary study or systematic review or were supported or linked to a reference that was an editorial or another clinical practice guideline. These statements could refer to several topics including duration of treatment, discharge management, diagnostic testing, exercise, and the importance of individualized care plans. In other words, these statements were about BVPs but it was not specified what those BVPs were and/or the studies cited were not aligned with our classification “Other BVP mentioned and supported by at least one reference to a primary study or systematic review” (see below).
Other BVP mentioned and supported by at least one reference to a primary study or systematic review
This classification was assigned to statements that were directly supported or linked to a reference that appeared to be a primary study or systematic review. A primary study was one that collected original data [19]. This classification excluded BVPs in relation to the above classifications, i.e., they were not BVPs for choosing between specific medications, or those related to adherence, or those related to financial costs and benefits. Further, the references cited were those that did not meet the criteria for pharmaceutical choice, adherence to medication, or financial costs and benefits. Statements under this classification encompassed patients’ needs, expectations, wishes, requests, concerns, interests, and perceptions. These statements also included patients’ wishes to take medication or not (as opposed to wishes to take one particular medication over another). Only statements that cited at least one primary study or systematic review related to BVPs were included in this classification.
For each classification, we calculated the total number of statements (or related consecutive statements) as well as the total number of guidelines with at least one statement (or related consecutive statements). All statements were placed in one classification only and are quoted directly from the guideline to minimize interpretation error. If a statement appeared to fit into more than one classification, it was assigned to the most appropriate classification based on the criteria described above. For example, Scotland B [20] included information about minor side effects of calcium supplementation influencing adherence but because the focus of this section of the guidelines was on adverse effects of calcium intake and calcium supplementation, we classified this statement as “BVP related to choice of pharmacotherapy or general treatment.” Similarly, statements from the UK G [21], Australia [22], and Hong Kong [23] also included elements related to patient compliance but these statements appeared overall to be focused on the choice of pharmacological therapy and were classified as “BVP related to choice of pharmacotherapy or general treatment.” In one case (Lebanon E [24]), the statement about patient BVPs appeared in the introduction and referenced another guideline, not the Lebanon guidelines. We classified this statement as “other BVP mentioned but not supported by a reference to a primary study or systematic review.”
Statements repeated in more than one location of the guideline were considered as separate statements. For example, in South Africa [25], the same statement appeared on pages 25 and 150 and another statement appeared on both pages 26 and 151.
The statements were searched for the terms “belief(s)/believe,” “preference(s)/prefer,” and “value(s)” to calculate how many times these terms were mentioned in the respective guideline. Each statement was examined for inclusion of at least one mention of these three terms. If the term, for example, “values,” was mentioned more than once in a particular statement or related consecutive statements, it was counted as occurring once in that statement. However, if both the term “value” and “preference” occurred, these were considered as one count for “value(s)” and one count for “preference(s)/prefer.”
For statements that cited a supporting reference(s), the supporting reference(s) was also noted and the methods used in these references to elicit BVPs were reviewed. Supporting references for the BVP statements were documented but not included in our classification system and they were not considered in our count of the terms “beliefs,” “values,” and “preferences” but they helped us to define the classification of the statement only if we were unsure of where to classify the statement. For example, Belgium E [26] reported that calcium and vitamin D supplementation was sometimes perceived by patients and physicians as an excessive medication and easily dismissed. The reference cited was on adherence to osteoporosis treatment and thus, this statement was classified as “BVP related to adherence to pharmacotherapy or treatment in general.” If the reference cited was not accessible through PubMed or the library catalogue system at the University of Toronto or St. Michael’s Hospital, we made a team decision to assign the statement or related consecutive statements to an appropriate classification.
Results
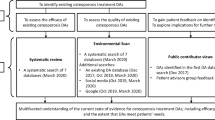
Twenty-seven of 70 guidelines (39%) included 95 statements or consecutive statements about patient BVPs. Figure 1 demonstrates the screening process of the guidelines. In descending order, the number of statements or related consecutive statements was 11 (Hong Kong), 10 (South Africa), 9 (Australia), 7 (Canada, Scotland B), 6 (India B), 5 (USA A, UK G, India C), 4 (Scotland A), 2 (USA B, Europe, Germany B, Greece A, Italy, UK E, UK F, Singapore, Middle East and North Africa A), and 1 (USA C, Latin America, Belgium C, Belgium E, Belgium F, Spain, Lebanon C, Lebanon E). The year of publication of the guideline ranged from 2008 to 2017 and the length of the guidelines ranged from 5 to 200 pages (with 24 of 27 guidelines being 10 pages or greater in length). No clear trends were noted in the number of statements by country/region, year of publication, or length of guideline (see Table 1).

Screening process for guidelines from the International Osteoporosis Foundation website
As shown in Tables 2, 3, 4, 5, and 6, 32 statements (14 guidelines) were classified under “BVP related to choice of pharmacotherapy or general treatment” (28 of the 32 statements were about choice of pharmacotherapy) (Table 2); 10 (7 guidelines) were classified under “BVP related to adherence to pharmacotherapy or treatment in general” (Table 3); 5 (5 guidelines) were classified under “BVP related to financial costs and benefits” (Table 4); 43 (19 guidelines) were classified under “other BVP mentioned but not supported by a reference to a primary study or systematic review” (Table 5); and 5 (3 guidelines) were classified under “other BVP mentioned and supported by at least one reference to a primary study” (Table 6). The category “other BVP mentioned but not supported by a reference to a primary study or systematic review” addressed a variety of topics. Many statements in this category mentioned the characteristics of patients such as risk of fracture, comorbidities, circumstances, abilities, indications for treatment, cognitive impairment, and mental status. Topics addressed within the category “other BVPs mentioned and supported by at least one reference to a primary study or systematic review” included fear of falling, falls reduction programs, exercises, menstrual problems or menopausal symptoms, and patient-clinician agreement on treatment goals. In the 95 statements, the term “preference(s)/prefer” appeared the most often (n = 43) followed by “value(s)” (n = 7) and then “belief(s)/believe” (n = 4). The term “preferences” appeared most often in the classification “BVP related to the choice of pharmacotherapy or general treatment” (n = 24), followed by the classification “other BVP mentioned but not supported by a reference to a primary study or systematic review” (n = 17).
Across all statements, 29 supporting references were linked with BVPs mentioned in the guidelines (see Tables 2, 3, 4, 5, and 6). Eight of the 29 cited references were not located through our external search of PubMed and the library catalogues at St. Michael’s Hospital or University of Toronto. We sent an email to two authors of these references and did not receive a response. We were unable to locate the contact information for the six remaining references cited. The 21 cited references that were located included an editorial, a systematic review, other guidelines, a website, a case study, a study not related to BVPs, or quantitative studies utilizing measures of preferences or beliefs such as the Preference and Satisfaction Questionnaire [47], standard gamble [48], and Beliefs about Medicines Questionnaire [49]. No qualitative studies were included as providing evidence of patients’ BVPs.
Discussion
In this document analysis, 27 of 70 (39%) guidelines included mention of patients’ BVPs. This suggests that there is room for improvement in consideration of BVPs of the patients for whom osteoporosis guidelines are targeted. These 27 guidelines accounted for 95 individual statements or related consecutive statements, of which less than half (n = 43) included the term “preferences.” There were fewer instances of the terms “values” (n = 7) and “beliefs” (n = 4) in the 95 statements. Patients’ BVPs were mentioned as an important factor to consider in 19 guidelines but appeared to be conceptualized mostly as preferences for one medication over another in 14 guidelines. Of interest, only 5 statements from 3 guidelines (Canada [27], Australia [22], India B [42]) fit within the classification “other BVP mentioned and supported by at least one reference to a primary study or systematic review.” This suggests that guidelines need to go beyond discussing BVPs as an important factor to consider in general and include relevant evidence in guideline development. Conceptualizing BVPs as the choice of pharmacotherapy, adherence to pharmacotherapy, and financial costs to individuals or society is also of concern as they do not appear to reflect BVPs of individuals with bone health issues. Rather, these conceptualizations appear to reflect the agenda of pharmaceutical companies and/or financial constraints of the individual or health care system, rather than health.
Our findings are specific to osteoporosis clinical practice guidelines but they may not be unique. McCormack and Loewen [1] reviewed 5 Canadian clinical practice guidelines for diabetes, dyslipidemias, hypertension, and osteoporosis and reported that while 3 of the 5 guidelines mentioned the importance of patient values and preferences, little attention was paid to patients’ values and preferences in therapeutic decision-making.
When guidelines accounted for BVPs, the conceptualization of BVPs appeared to focus on choosing between medications or adhering to medication. One reason for this may be the lack of patient involvement in the development of the guidelines themselves. Selva and colleagues [50] reported that most guidance documents for developing guidelines recommend the inclusion of patients and/or their views in the guideline development process. In the practice of guidelines examined in this study, patient characteristics were often conceptualized as proxies for BVPs. This is also potentially problematic. Tailoring treatment based on a patient’s disease severity and risk profile is not the same thing as taking an individual’s values into account [51]. As mentioned, only 3 guidelines provided what we considered to be evidence of patient BVPs based on studies cited. Further, no study cited by the statements in this document analysis used qualitative research to elicit patient BVPs. Krahn and Naglie [51] offer the explanation that narratives about patient experiences are not often regarded as evidence. These authors propose that preference-related evidence includes decision analyses in which preferences are represented using health utilities, preferences for health outcomes, or qualitative studies of patients’ experiences [51]. They also propose that recommendations should be preference-sensitive in that guideline developers should “distinguish between recommendations that nearly all patients will accept and recommendations that are likely to vary depending on an individual patient’s preferences for outcome, process, or choice” (p. 437).
Our study has several implications. In guidelines which mentioned BVPs, the term “preferences” was most often included, while “beliefs” and “values” were mentioned fewer times. In our study, preferences most often referred to the choice of one medication over another. As Guyatt and colleagues [7] point out, one challenge to evidence-based medicine is the ability to study the process of eliciting and understanding patient values and the best ways to incorporate them in the clinical decision-making process. Having said this, some authors appear to question the ability or desire of sick patients to examine their preferences and values [52]. They propose that patients may not be able to absorb complex information and make decisions under the stress and distraction of pain and illness. One option is to examine the experiential knowledge of patients as described by Caron-Flinterman and colleagues [53]. These authors refer to experiential knowledge as the implicit, lived experiences of individual patients with their bodies, their illnesses, and care. In the midst of this debate, it is important to note the rising interest in having patients as active participants in research related to their health. These include the Strategy for Patient-Oriented Research sponsored by the Canadian Institutes of Health Research (www.cihr-irsc.gc.ca/e/41204.html) and the Patient and Clinician Engagement Program of the North American Primary Care Research Group (www.napcrg.org/).
We believe that if preferences are not explicit in guidelines, physicians will rely on other patient factors in their decision-making. Otte and colleagues [54] reported that physicians’ assessment of age and general condition or prognosis of the patient played a role in treatment recommendations and that patient preferences were not generally considered. If osteoporosis clinical practice guidelines are not explicit in their conceptualization of BVPs, previous work suggests that patients may seek advice about bone health and fracture risk from their family physician and/or specialist [55, 56], yet may receive different messages from these providers [57, 58].
We distinguished a patient’s preference between two or more medications and a patient’s preference to take any medication at all because a patient’s beliefs, values, and preferences to not take medication is an option and should be acknowledged. For example, Rittenmeyer and colleagues [59] examined “watchful waiting” as an alternative approach to the medical management of certain diseases. They reported that the process to choose watchful waiting is a complex one that often leads to uncertainty and anxiety. However, the burden of this process can be lessened if patients have a reassuring relationship with their health care provider.
Our study has several strengths. Two individuals (AM, FN) independently extracted data and then met to consolidate their data extraction. All the authors met regularly to discuss and refine the categories developed. Three individuals (AM, FN, WY) then worked together to assign the statements to the five categories. The first author resolved any discrepancies with the grouping of statements into the categories and another author (WY) verified all data extraction at the end of the study. We have developed a classification scheme that others can use or revise further to examine guidelines in their own disease groups. One limitation of our study was that we were not able to examine guidelines that were written in languages other than English (n = 24) so cannot comment on whether these guidelines included data on patient BVPs. Also, we relied on the IOF website as a resource for the guidelines. The IOF site may not include the most current version of guidelines published by each country or region. Countries with multiple guidelines would be reliant on the various organizations within that country to send their guidelines to the IOF. Finally, we did not extract information on the methodology used to develop the guidelines or the presence of a patient in the development of the guidelines. Future studies should examine whether the methodology used to develop guidelines or the presence of a patient in guideline development influences the number and content of BVP statements.
In conclusion, 39% (n = 27) of English-language osteoporosis guidelines included mention of BVPs. In 19 guidelines, the importance of BVPs in general was mentioned. Of 95 BVP statements across the 27 guidelines, the term “preferences” occurred much more frequently (n = 43) than “values” (n = 7) and “beliefs” (n = 4) and when described, most often referred to the choice of one medication over another (32 statements in 14 guidelines). We propose that guideline developers consider strategies for a broader conceptualization and inclusion of BVPs in future osteoporosis clinical practice guidelines and provide clinicians with information about benefits and harms in a way that allows for shared decision-making.
References
McCormack JP, Loewen P (2007) Adding “value” to clinical practice guidelines. Can Fam Physician 53:1326–1327
Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS (1996) Evidence based medicine: what is is and what it isn’t: it’s about integrating individual clinical expertise and the best external evidence. BMJ 312(7023):71–72
Excellence NIfHaC (2014) Developing NICE guidelines: the manual, pp 1–234
Gill G (2001) Going Dutch? How to make clinical guidelines work: an innovative report from Holland. Clin Med 1(4):307–308
James PA, Cowan TM, Graham RP (1998) Patient-centered clinical decisions and their impact on physician adherence to clinical guidelines. J Fam Pract 46(4):311–318
Charles C, Gafni A, Whelan T (1997) Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med 44(5):681–692
Guyatt GH, Haynes RB, Jaeschke RZ et al (2000) Users’ guide to the medical literature: XXV. Evidence-based medicine: principles for applying the users’ guides to patient care. JAMA 284(10):1290–1296
Montori VM, Devereaux PJ, Straus S, Haynes B, Guyatt G (2008) Decision making and the patient. In: Guyatt G, Rennie D, Meade MO, Cook DJ (eds.) Users’ guides to the medical literature: a manual for evidence-based clinical practice. 2nd ed. 22:643–661. New York: The MacGraw-Hill Companies, Inc.
Group PCR (2008) Patients’ preferences within randomised trials: systematic review and patient level meta-analysis. BMJ 337:a1864
Purnell TS, Joy S, Little E, Bridges JF, Maruthur N (2014) Patient preferences for noninsulin diabetes medications: a systematic review. Diabetes Care 37(7):2055–2062
Joy S, Purnell T, Little E, Bridges J (2013) Patient preferences for the treatment of type-2 diabetes: a scoping review. PharmacoEconomics 31:877–892
Utens CMA, Dirksen CD, Weijden TV, Joore MA (2016) How to integrate research evidence on patient preferences in pharmaceutical coverage decisions and clinical practice guidelines: a qualitative study among Dutch stakeholders. Health Policy 120(1):120–128
Breejen EM, Hermens RP, Galama WH, Willemsen WN, Kremer JA, Nelen WL (2016) Added value of involving patients in the first step of multidisciplinary guideline development: a qualitative interview study among infertile patients. Int J Qual Health Care 28(3):299–305
Tong A, Tunnicliffe DJ, Lopez-Vargas P et al (2016) Identifying and integrating consumer perspectives in clinical practice guidelines on autosomal-dominant polycystic kidney disease. Nephrology 21(2):122–132
Kanis JA, Harvey NC, Cooper C et al (2016) A systematic review of intervention thresholds based on FRAX: a report prepared for the National Osteoporosis Guideline Group and the International Osteoporosis Foundation. Arch Osteoporos 11(1):25. https://doi.org/10.1007/s11657-016-0278-z
Wang X, Chen Y, Yao L et al (2018) Reporting of declarations and conflicts of interest in WHO guidelines can be further improved. J Clin Epidemiol 98:1–8
Ospina NS, Rodriguez-Gutierrez R, Brito JP, Young WF, Montori VM (2015) Is the endocrine research pipeline broken? A systematic evluation of the Endocrine Society clinical practice guidelines and trial registration. BMC Med 13:187
O'Leary Z (2004) The essential guide to doing research. Sage Publications, London
Guyatt G, Rennie D, Meade MO, Cook DJ (2008) User’s guide to the medical literature: a manual for evidence-based clinical practice, 2nd edn. McGraw Hill, New York
Scottish Intercollegiate Guidelines Network (SIGN 142) Management of osteoporosis and the prevention of fragility fractures. Healthcare Improvement Scotland. 1–128. http://www.sign.ac.uk/pdf/SIGN142.pdf
National Institute for Health and Clinical Excellence (2010) Denosumab for the prevention of osteoporotic fractures in postmenopausal women. Technology appraisal 1–60. http://guidance.nice.org.uk/TA204
The Royal Australian College of General Practitioners (2010) Clinical guideline for the prevention and treatment of osteoporosis in postmenopausal women and older men. 1–83
Ip TP, Cheung SK, Cheung TC et al (2013) The Osteoporosis Society of Hong Kong (OSHK): 2013 OSHK guideline for clinical management of postmenopausal osteoporosis in Hong Kong. Hong Kong Med J 19(Suppl 2):1–40
Chakhtoura M, Leslie WD, McClung M, Cheung AM, Fuleihan GE (2017) The FRAX-based Lebanese osteoporosis treatment guidelines: rationale for a hybrid model. Osteoporos Int 28(1):127–137. https://doi.org/10.1007/s00198-016-3766-5
Hough S, Ascott-Evans B, Brown S et al (2010) NOFSA guideline for the diagnosis and management of osteoporosis. J Endocrinol Metab Diabetes S Afr 15(3):1–188
Body JJ, Bergmann P, Boonen S et al (2010) Evidence-based guidelines for the pharmacological treatment of postmenopausal osteoporosis: a consensus document by the Belgian Bone Club. Osteoporos Int 21(10):1657–1680. https://doi.org/10.1007/s00198-010-1223-4
Papaioannou A, Morin S, Cheung AM, et al. (2010) Clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: Background and technical report. Toronto, 1–89
Cosman F, de Beur SJ, LeBoff MS et al (2014) Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int 25(10):2359–2381. https://doi.org/10.1007/s00198-014-2794-2
Camacho PM, Petak SM, Binkley N et al (2016) American Association of clinical endocrinologists and American college of endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis - 2016. Endocr Pract 22(Suppl 4):1–42. https://doi.org/10.4158/ep161435.gl
Nordin C (2011) Screening for osteoporosis: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 155(4):356–364. https://doi.org/10.7326/0003-4819-155-4-201108160-00021
(SIBOMM) ISoOaMM (2009) IBEROAMERICAN CONSENSUS ON OSTEOPOROSIS SIBOMM 2009: Osteoporosis: prevention, diagnosis, and treatment.1–49
Kanis JA, McCloskey EV, Johansson H et al (2013) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 24(1):23–57
Body JJ, Bergmann P, Boonen S et al (2012) Extraskeletal benefits and risks of calcium, vitamin D and anti-osteoporosis medications. Osteoporos Int 23(Suppl 1):S1–S23. https://doi.org/10.1007/s00198-011-1891-8
Body JJ, Bergmann P, Boonen S et al (2007) Management of cancer treatment-induced bone loss in early breast and prostate cancer -- a consensus paper of the Belgian Bone Club. Osteoporos Int 18(11):1439–1450. https://doi.org/10.1007/s00198-007-0439-4
Osteologie D (2011) DVO guideline 2009 for prevention, diagnosis and therapy of osteoporosis in adults. Osteologie 20:55–74
Makras P, Vaiopoulos G, Lyritis GP (2012) 2011 guidelines for the diagnosis and treatment of osteoporosis in Greece. J Musculoskelet Neuronal Interact 12(1):38–42
Rossini M, Adami S, Bertoldo F et al (2016) Guidelines for the diagnosis, prevention and management of osteoporosis 2016. Reumatismo 68(1):1–39
Network SIG (2009) Management of hip fracture in older people. 1–56
González-Macías J, del Pino-Montes J, Olmos J, Nogués X (2015) Clinical practice guidelines for postmenopausal, glucocorticoid-induced and male osteoporosis. Rev Clin Esp 215(9):515–526
Excellence NIfHaC (2008) Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women: technology appraisal guidance. United Kingdom. 1–87
Excellence NIfHaC (2008) Alendronate, etidronate, risedronate, raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women. 1–82
Meeta DL, Agarwal N, Vaze N, Shah R, Malik S (2013) Clinical practice guidelines on menopause: an executive summary and recommendations. J Mid-life Health 4(2):77–106
Meeta S, Harinarayan CV, Marwah R, Sahay R, Kalra S, Babhulkar S (2013) Clinical practice guidelines on postmenopausal osteoporosis: an executive summary and recommendations. J Mid-life Health 4(2):107FNx01 Copyright 2013 Medknow Publications and Media Pvt. Ltd. (HTML document version posted as of May 10, 2018)
Ministry of Health S. Osteoporosis (2008) MOH Clinical Practice guidelines. 1–94
Maalouf G, Gannage-Yared MH, Ezzedine J et al (2007) Middle East and North Africa consensus on osteoporosis. J Musculoskelet Neuronal Interact 7(2):131–143
Maalouf G, Bachour F, Issa M, Yazbeck P, Maalouf N, Daher C, Yaghi Y, Eid R (2012) Guidelines for fragility fractures in Lebanon. J Med Liban 60(3):153–158
Kendler DL, Bessette L, Hill CD et al (2010) Preference and satisfaction with a 6-month subcutaneous injection versus a weekly tablet for treatment of low bone mass. Osteoporos Int 21:837–846
Cranney AB, Coyle D, Hopman WM, Hum V, Power B, Tugwell PS (2005) Prospective evaluation of preferences and quality of life in women with hip fractures. J Rheumatol 32:2393–2399
Freemantle N, Satram-Hoang S, Tang E-T et al (2012) Final results of the DAPS (Denosumab Adherence Preference Satisfaction) study: a 24-month, randomized, crossover comparison with alendronate in postmenopausal women. Osteoporos Int 23:317–326
Selva A, Sanabria AJ, Pequeno S et al (2017) Incorporating patients’ views in guideline development: a systematic review of guidance documents. J Clin Epidemiol 88:102–112
Krahn M, Naglie G (2008) The next step in guideline development: incorporating patient preferences. JAMA 300(4):436–438
Grimen H (2009) Power, trust, and risk: some reflections on an absent issue. Med Anthropol Q 23(1):16–33
Caron-Flinterman JF, Broerse JEW, Bunders JFG (2005) The experiential knowledge of patients: a new resource for biomedical research? Soc Sci Med 60:2575–2584
Otte I, Salloch S, Reinacher-Schick A, Vollmann J (2017) Treatment recommendations within the leeway of clinical guidelines: a qualitative interview study on oncologists’ clinical deliberation. BMC Cancer 17:780
Sale JEM, Beaton DE, Sujic R, Bogoch ER (2010) “If it was osteoporosis, I would have really hurt myself”. Ambiguity about osteoporosis and osteoporosis care despite a screening program to educate fracture patients. J Eval Clin Pract 16(3):590–596
Sale J, Gignac M, Hawker G et al (2011) Decision to take osteoporosis medication in patients who have had a fracture and are ‘high’ risk for future fracture. BMC Musculoskelet Disord 12:92
Sale JEM, Hawker G, Cameron C, Bogoch E, Jain R, Beaton D, Jaglal S, Funnell L (2015) Perceived messages about bone health after a fracture are not consistent across health care providers. Rheumatol Int 35(1):97–103
Sale JE, Bogoch E, Hawker G et al (2014) Patient perceptions of provider barriers to post-fracture secondary prevention. Osteoporos Int 25(11):2581–2589. https://doi.org/10.1007/s00198-014-2804-4
Rittenmeyer L, Huffman D, Alagna M, Moore E (2016) The experience of adults who choose watchful waiting or active surveillance as an approach to medical treatment: a qualitative systematic review. JBI Database System Rev Implement Rep 14(2):174–255
Funding
Joanna Sale holds a Canadian Institutes of Health Research New Investigator Salary Award (Funding Reference No. COB-136622).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sale, J., Marwah, A., Naeem, F. et al. Evidence of patient beliefs, values, and preferences is not provided in osteoporosis clinical practice guidelines. Osteoporos Int 30, 1325–1337 (2019). https://doi.org/10.1007/s00198-019-04913-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-019-04913-y