
Abstract
Summary
We compared bone outcomes in children with breech and cephalic presentation at delivery. Neonatal whole-body bone mineral content (BMC) and area were lower in children with breech presentation. At 4 years, no differences in whole-body or spine measures were found, but hip BMC and area were lower after breech presentation.
Introduction
Breech presentation is associated with altered joint shape and hip dysplasias, but effects on bone mineral content (BMC), area (BA) and density (BMD) are unknown.
Methods
In the prospective Southampton Women’s Survey mother-offspring cohort, whole-body bone outcomes were measured using dual-energy X-ray absorptiometry (DXA) in 1430 offspring, as neonates (mean age 6 days, n = 965, 39 with a breech presentation at birth) and/or at age 4.1 years (n = 999, 39 breech). Hip and spine bone outcomes were also measured at age 4 years.
Results
Neonates with breech presentation had 4.2 g lower whole-body BMC (95% CI −7.4 to − 0.9 g, P = 0.012) and 5.9 cm2 lower BA (− 10.8 to − 1.0 cm2, P = 0.019), but BMD was similar between groups (mean difference − 0.007, − 0.016 to 0.002 g/cm2, P = 0.146) adjusting for sex, maternal smoking, gestational diabetes, mode of delivery, social class, parity, ethnicity, age at scan, birthweight, gestational age and crown-heel length. There were no associations between breech presentation and whole-body outcomes at age 4 years, but, in similarly adjusted models, regional DXA (not available in infants) showed that breech presentation was associated with lower hip BMC (− 0.51, − 0.98 to − 0.04 g, P = 0.034) and BA (− 0.67, − 1.28 to − 0.07 cm2, P = 0.03) but not with BMD (− 0.009, − 0.029 to 0.012 g, P = 0.408), or spine outcomes.
Conclusions
These results suggest that breech presentation is associated with lower neonatal whole-body BMC and BA, which may relate to altered prenatal loading in babies occupying a breech position; these differences did not persist into later childhood. Modest differences in 4-year hip BMC and BA require further investigation.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The prenatal period has a strong and persisting influence on skeletal development and health. Maternal factors such as smoking, body composition, parity and activity influence accrual of bone mass during pregnancy [1, 2]. In addition, factors intrinsic to or influenced by pregnancy including birthweight and gestational age [2] and placental size [3] are also determinants of neonatal bone mass. Birthweight in particular remains predictive of bone mass throughout childhood [4] and into older age [5], whilst preeclampsia has been associated with reduced hip BMD in adolescence [6]. Therefore, it is important to identify predictors of foetal bone mineral accrual during pregnancy to develop preventative strategies against future osteoporosis and fractures [7]. However, whilst mechanical loading via physical activity and exercise has a dominating influence on bone area/mass throughout early childhood [8], adolescence [9,10,11] and into old age [12,13,14], the influence of foetal presentation on bone development remains little explored.
Breech presentation (where the foetus is lying bottom-down in pregnancy) may be considered as a natural model of altered foetal loading and is associated with restricted foetal movement [15]. Breech presentation is common throughout pregnancy, evident in ~ 50% of foetuses at 25 weeks’ gestation [16] falling to approximately ~ 5% at birth [17]. Breech presentation results in restriction of lower limb movements in the third trimester, particularly at the hip joint [15]. This is particularly important as the mechanical loading of the skeleton caused by foetal movements is greatest in late pregnancy [18]. However, it has been proposed that poor foetal movement may also be responsible for the failure to attain a cephalic position [19], i.e. reduced movements in breech foetuses may not solely be attributable to foetal position [20]. This is supported by a higher frequency of breech presentation in children with conditions affecting motor development such as cerebral palsy [21]; the incidence increases with disease severity [19]. Given the importance of foetal skeletal loading as demonstrated in animal [22] and in silico [23] models, it is not surprising that breech presentation has consequences for skeletal development. Breech presentation at birth is associated with a ten-fold higher incidence of developmental hip dysplasias [24], whilst femoral anteversion is 10° higher (equivalent to 1.25 SD) in breech rather than cephalic presentation [25]. However, the effects of breech presentation on bone mass accrual during gestation and early life have not been explored. Tibial bone ultrasound speed of sound (an indirect indicator of bone quality) was lower in breech than that in cephalic presentation [26], but clinical measures of bone mass, area and density have not previously been assessed—nor have longer-term associations been examined.
In this study, we compared bone mass, area and density at birth and age 4 years in children born with breech or cephalic presentation in a large prospective mother-offspring cohort—the Southampton Women’s Survey (SWS). It was hypothesised that breech presentation would be associated with deficits in bone outcomes at birth and early childhood, which would not be explained by lower gestational age or birthweight in this group.
Methods
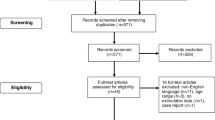
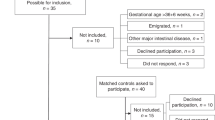
The SWS recruited 12,583 women living within the city of Southampton in southern England when they were not pregnant. Women in the cohort who subsequently became pregnant were invited to complete a lifestyle assessment questionnaire at 11 and 34 weeks’ gestation, from which details of maternal smoking, ethnicity, parity, gestational diabetes and social class were extracted. Only singleton pregnancies and the first pregnancy per study mother were included. At birth, gestational age, mode of delivery and foetal presentation were recorded, as were crown-heel length measured using a neonatometer (CMS Ltd., UK) and birthweight using calibrated digital scales (Seca, UK). Within 2 weeks of birth and following maternal consent, total body dual-energy X-ray absorptiometry (DXA) scans were taken using a Lunar DPX-L scanner (GE Corporation, Madison, WA, USA) using pediatric software (pediatric small scan mode v4.7c). During the neonatal scan, visit infants were fed if necessary, undressed completely and then swaddled in a standard towel. They were placed in a standard position on a waterproof sheet and kept in position using rice bags placed over the bottom end of the towel. At age 4 years, height was measured using a calibrated stadiometer and weight using calibrated digital scales (Seca, UK); total body and dedicated hip and spine scans were performed using a Discovery DXA scanner (Hologic Inc., Bedford, MA, USA). The scan machines underwent a daily quality assessment, alongside a weekly calibration against a water phantom. To encourage compliance, the scanner bed was covered with a sheet with appropriate coloured cartoons and was laid on the couch prior to scan positioning. To help reduce movement artefact, children were shown a suitable cartoon on DVD. From the neonatal total body scan, measurements of bone mineral content (BMC), bone area (BA) and bone mineral density (BMD) for the whole body including the head were obtained. Size-adjusted or SA BMC (BMC adjusted for height, weight and BA) was also assessed as a proxy for volumetric BMD. At age 4 years, BMC, BA and BMD were recorded for whole-body (less head), hip and spine scans, and SA BMC was assessed. Scans were assessed by two independent operators; 31 neonatal scans and 32 4-year scans were excluded from analysis due to movement artefacts. Babies with a known congenital anomaly (n = 7) and children with a foetal position other than breech or cephalic, e.g. transverse (n = 14) were excluded from analysis. The study was approved by Southampton and Southwest Hampshire Local Research Ethics Committee (approval numbers 267/97, 307/97, 153/99 and 005/03/t) and parental informed consent was given at both scan timepoints.
Statistical analysis
A complete case analysis was performed with no imputation, resulting in a cohort of 1430 participants (745 male). The neonatal and 4-year cohorts partially overlapped such that 534 individuals had complete data at both timepoints, and the maximum number of participants was used at either timepoint to optimise statistical power. Nine hundred sixty-five infants (498 male) had complete data at birth and were included in neonatal analyses; 999 children (515 male) had complete data at age 4 years. In a sensitivity analysis, the cohort was limited to the offspring with data at both timepoints. Crown-heel length and birthweight were converted to Z-scores using WHO Child Growth Standards [27]. Differences in cohort characteristics by presentation type (conventional/breech) were assessed by Fisher’s exact test, χ2 tests and t tests for binary, categorical and continuous variables respectively. Associations between presentation type and bone outcomes were assessed with multiple linear regression models using the R statistical environment (version 3.1.2, www.r-project.org). There was no evidence of sex interactions in relation to presentation mode and its associations with bone outcomes, so separate analyses were not conducted by sex. A minimal model 1 was adjusted only for sex. In model 2, potential confounders known to be associated with both breech presentation and bone outcomes were included. In model 3, potential mediating factors relating to length of gestation and body size were included, in order to identify the direct association between breech presentation and bone outcomes independent of these known differences between breech and cephalic births. The structure of model predictors was as follows:
-
Model 1 (minimal): presentation + sex (4-year scans additionally adjusted for height)
-
Model 2 (confounders): model 1 + maternal smoking + gestational diabetes + delivery mode + social class + parity + ethnicity + age at scan
-
Model 3 (mediators): model 2 + birthweight + gestational age + crown-heel length (neonatal outcomes) or height at time of scan (4-year outcomes)
Model residuals were checked for heteroscedasticity, and variance inflation factors (VIFs) were used to check for multicollinearity. Outcomes are presented as means and 95% confidence intervals, unless otherwise stated.
Results
Of the 965 participants with neonatal scans, 39 (19 male) had a breech presentation at birth; 39 (20 male) of the 999 children with 4-year scans had a breech presentation at birth (Table 1). Breech presentation was associated with lower birthweight, and shorter crown-heel length and gestational age, whilst primiparity and caesarean section delivery were more common in children with breech presentation. There were no differences in height, body mass or body composition between breech and cephalic presentation children at age 4 years (data not shown).
Breech presentation was associated with lower neonatal total body BMC and BA, but not BMD or SA BMC (Fig. 1). After adjustment for potential confounders in model 2, children with breech presentation had 25% lower BMC, 22% lower BA and 3% lower BMD than those with cephalic presentation (equivalent to 0.9 SD, 0.9 SD and 0.5 SD deficits respectively). After adjustment for gestational age, birthweight and length in model 3, these associations were substantially attenuated, although lower BMC (7% or 0.26 SD) and BA (5% or 0.22 SD) were still evident in breech presentation.

Neonatal bone outcomes in breech presentation, shown as regression coefficients and 95% CI. Data adjusted as follows: model 1—presentation + sex; model 2—model 1 + maternal smoking + social class + birthweight + parity + ethnicity + age at scan; model 3—model 2 + birthweight + gestational age + crown-heel length
There were no group differences evident in outcomes from total body (less head) or spine scans at age 4 years (Supplementary Figure 1). However, in unadjusted model 1, breech presentation was associated with lower hip BMC and BA (but not BMD or SA BMC) (Fig. 2). There was little effect of adjustment in further models, such that in fully adjusted analyses, BMC was 7% (0.33 SD) and BA 5% (0.35 SD) lower in children who had a breech presentation at delivery than in those with a cephalic presentation (Table 2).

Hip bone outcomes at 4 years of age in breech presentation, shown as regression coefficients and 95% CI. Data adjusted as follows: model 1—presentation + sex; model 2—model 1 + maternal smoking + social class + birthweight + parity + ethnicity + age at scan; model 3—model 2 + birthweight + gestational age + height at scan
Sensitivity/additional analyses
Similar results were observed when using total body measures without subtraction of head segment (values not shown). Head circumference at birth was similar in breech (35.0 ± 1.4 cm) and cephalic (35.0 ± 1.1 cm) births (P = 0.77), and additional adjustment for head circumference did not attenuate associations between breech presentation and bone outcomes. Restricting analyses only to those individuals with neonatal and 4-year scans resulted in similar regression coefficients (Supplementary Table 1). VIF analysis indicated moderate multicollinearity (3 < VIF < 3.5) for birthweight and birth length in neonatal outcome models, but not 4-year outcomes where VIF < 2 in all cases. However, these variables were strong independent predictors of neonatal outcomes, and removal of either variable in additional sensitivity analyses did not substantially affect regression coefficients for other variables including breech presentation.
Discussion
In this large mother-offspring cohort study, breech presentation at delivery was associated with lower bone mass, area and density at birth. These associations were substantially attenuated by adjustment for birthweight, crown-heel length and gestational age, although residual associations were observed. These associations did not persist at age 4 years, but here, breech presentation was modestly associated with lower hip bone mass and area (but not density).
Comparison with previous findings
A previous study found lower tibia bone ultrasound speed of sound measurements (an indicator of bone quality) in breech- versus cephalic-presenting babies at birth [26]. To the best of our knowledge, this is the first study to examine bone outcomes using DXA in breech and cephalic presentations. In addition, this study extends previous work by investigating whether deficits in bone outcomes persist into later childhood. Whilst deficits in total body outcomes were not evident at age 4 years, localised deficits in hip bone mass and area were observed even after consideration of potential confounding factors. This site corresponds with the location of dysplasias [24] and joint instability [28] which are more commonly found in breech births, and with altered femoral geometry [25].
Potential explanations of findings
Whilst large deficits in neonatal bone mass and area were observed in breech births, a large proportion of this difference was explained by shorter gestation and lower birthweight in these infants. Foetal growth has previously been shown to be impaired in children who present as breech at birth even accounting for differences in gestational age [29], although, in this cohort, sex- and gestation-adjusted birthweight was not affected by presentation. However, when mediating factors such as birthweight and gestational age were considered, residual deficits in neonatal bone mass and area were still evident in breech presentation.
A potential cause of skeletal deficits associated with breech presentation independent of body size and length of pregnancy is the restriction of normal frequency and type of foetal movements, particularly later in pregnancy. However, the exact cause of reduced foetal movements is unknown and could relate to maternal or foetal factors. Whilst maternal mechanical factors such as oligohydramnios or uterine malformations likely contribute to reduced foetal movement, they are only evident in a small percentage of breech presentation births [29]. Breech presentation may be a result of poor neuromuscular development, leading to poor movement and an inability to attain a cephalic position. Evidence for this includes the higher breech incidence in children with conditions affecting motor development such as cerebral palsy [21], and correlation between breech incidence and severity of impairments either between or within clinical conditions (e.g. thoracic rather than lumbar level meningocele) [19]. In addition, umbilical cord length correlates with foetal movement [30] (and in turn bone ultrasound measures at birth [31]), and cords are shorter in breech than cephalic presentation [32]. Regardless of the cause, it seems likely that reduced foetal movements contribute to the size-independent deficits in bone outcomes in breech presentation evident in this study.
Significance and implications
Individuals born in the breech position are a substantial group when considered at the population level (approximately 22,500 p.a. in the UK). Therefore, any health deficits identified in this group have implications for a large number of individuals. Childhood is an important time for the attainment of a high-peak bone mass, which is protective against fractures in later life [7]. Total body and regional deficits in bone mass identified at birth and in early childhood may therefore have implications for osteoporosis and fracture risk in later life. Studies examining bone outcomes in adult or elderly individuals whose mode of presentation at birth is known would be a valuable development of this study. Effective interventions to reverse breech presentation are available [33]. However, whilst they substantially reduce the incidence of hip dysplasias in breech presentation, residual excess risk still exists [34]. This may be due to the lack of information on time sensitivity of exposure to breech position during pregnancy. From a 50% incidence of breech presentation at 25 weeks’ gestation, there is a roughly linear decline to only ~ 5% incidence at term [17]. Therefore, studies combining regular observations of foetal position with neonatal bone mass and broader skeletal outcomes might reveal periods during which cephalic version must be maintained to ensure healthy skeletal development.
Strengths and limitations
The strengths of the study are the use of a large, representative cohort and consideration of a number of potential maternal and offspring confounders, in addition to exclusion of foetuses with known congenital malformations. However, as this was an observational study, causality cannot be attributed. Longitudinal measurements of offspring bone outcomes were only available in a limited sample, although associations between breech presentation and bone outcomes observed in this sub-cohort were similar to those found in larger groups of children with complete data at only one timepoint. In addition, foetal position was only recorded at birth with no information on position throughout pregnancy. Around 45% of the individuals with cephalic presentation at birth will have occupied a breech position around 25 weeks [35]. A decreasing percentage of these children will have occupied the breech position from 25 to 36 weeks, although the likelihood of version to a cephalic position decreases with length of gestation [36]. Conversely, very few babies move from cephalic to breech position in the later stages of pregnancy. Therefore, whilst we can be confident that individuals presenting as breech at birth will have occupied that position for the later stages of pregnancy, many individuals with cephalic presentation will have occupied a large portion of their prenatal life in a breech position. As a result, we may have underestimated the effects of a continual breech position compared to a continual cephalic position throughout the third trimester, when mechanical loading of the skeleton is greatest [18].
The breech-presenting cohort was small and we may not have been powered to detect minor effects of breech position on total bone measures in early childhood. Whilst hip DXA scans have been used to examine bone strength in children of similar age in this and other cohorts [37,38,39], regional bone scans are not commonly used in clinical practice at this age and are likely to yield a less reliable measure than those at the whole body or spine. Similar studies in older children would reveal whether hip bone mass deficits persist at a stage where they become clinically relevant.
Conclusions
Breech presentation is associated with lower neonatal total body bone mass and area, differences which, although attenuated, remained statistically significant after adjustment for gestation, birthweight and length. They did not persist at 4 years, although modest deficits in hip bone mass and area were observed at this age. The findings of this study extend previous work reporting altered neonatal hip geometry and higher risk of joint instability and dysplasias at birth in breech presentation, but confirmation of a localised effect in later childhood is required. Future studies examining foetal position throughout pregnancy and neonatal skeletal health could give valuable information on key mechanosensitive periods for the developing skeleton.
References
Harvey NC, Javaid MK, Arden NK, Poole JR, Crozier SR, Robinson SM, Inskip HM, Godfrey KM, Dennison EM, Cooper C, the SWS Study Team (2010) Maternal predictors of neonatal bone size and geometry: the Southampton Women’s Survey. J Dev Orig Health Dis 1:35–41
Godfrey K, Walker-Bone K, Robinson S, Taylor P, Shore S, Wheeler T, Cooper C (2001) Neonatal bone mass: influence of parental birthweight, maternal smoking, body composition, and activity during pregnancy. J Bone Miner Res 16:1694–1703
Holroyd CR, Osmond C, Barker DJ, Ring SM, Lawlor DA, Tobias JH, Smith GD, Cooper C, Harvey NC (2016) Placental size is associated differentially with postnatal bone size and density. J Bone Miner Res 31:1855–1864
Rogers IS, Ness AR, Steer CD, Wells JC, Emmett PM, Reilly JR, Tobias J, Smith GD (2006) Associations of size at birth and dual-energy X-ray absorptiometry measures of lean and fat mass at 9 to 10 y of age. Am J Clin Nutr 84:739–747
Dennison EM, Syddall HE, Sayer AA, Gilbody HJ, Cooper C (2005) Birth weight and weight at 1 year are independent determinants of bone mass in the seventh decade: the Hertfordshire cohort study. Pediatr Res 57:582–586
Hannam K, Lawlor DA, Tobias JH (2015) Maternal preeclampsia is associated with reduced adolescent offspring hip BMD in a UK population-based birth cohort. J Bone Miner Res 30:1684–1691
Cooper C, Westlake S, Harvey N, Javaid K, Dennison E, Hanson M (2006) Review: developmental origins of osteoporotic fracture. Osteoporos Int 17:337–347
Ireland A, Rittweger J, Schönau E, Lamberg-Allardt C, Viljakainen H (2014) Time since onset of walking predicts tibial bone strength in early childhood. Bone 68:76–84
Ireland A, Maden-Wilkinson T, McPhee J, Cooke K, Narici M, Degens H, Rittweger J (2013) Upper limb muscle-bone asymmetries and bone adaptation in elite youth tennis players. Med Sci Sports Exerc 45:1749–1758
Sayers A, Deere K, Tobias JH (2015) The effect of vigorous physical activity and body composition on cortical bone mass in adolescence. J Bone Miner Res 30:584
Ireland A, Sayers A, Deere KC, Emond A, Tobias JH (2016) Motor competence in early childhood is positively associated with bone strength in late adolescence. J Bone Miner Res 31:1089–1098
Ireland A, Muthuri S, Rittweger J, Adams JE, Ward KA, Kuh D, Cooper R (2017) Later age at onset of independent walking is associated with lower bone strength at fracture-prone sites in older men. J Bone Miner Res 32:1209–1217
Hannam K, Deere KC, Hartley A, Al-Sari UA, Clark EM, Fraser WD, Tobias JH (2017) Habitual levels of higher, but not medium or low, impact physical activity are positively related to lower limb bone strength in older women: findings from a population-based study using accelerometers to classify impact magnitude. Osteoporos Int 28:2813–2822
Johansson J, Nordström A, Nordström P (2015) Objectively measured physical activity is associated with parameters of bone in 70-year-old men and women. Bone 81:72–79
Sival DA, Prechtl HF, Sonder GH, Touwen BC (1993) The effect of intra-uterine breech position on postnatal motor functions of the lower limbs. Early Hum Dev 32:161–176
Miller E, Kouam L (1981) Zur Haufigkeit von Beckenendlagen im Verlauf Der Schwangerschaft und zum Zeitpunkt der Geburt. Zentralbl Gynakol 103:105–109
Cammu H, Dony N, Martens G, Colman R (2014) Common determinants of breech presentation at birth in singletons: a population-based study. Eur J Obstet Gynecol Reprod Biol 177:106–109
Verbruggen SW, Kainz B, Shelmerdine SC, Hajnal JV, Rutherford MA, Arthurs OJ, Phillips AT, Nowlan NC (2018) Stresses and strains on the human fetal skeleton during development. Journal of The Royal Society Interface
Bartlett D, Okun N (1994) Breech presentation: a random event or an explainable phenomenon? Dev Med Child Neurol 36:833–838
Fong BF, Savelsbergh GJ, de Vries JI (2009) Fetal leg posture in uncomplicated breech and cephalic pregnancies. Eur J Pediatr 168:443–447
Andersen GL, Irgens LM, Skranes J, Salvesen KA, Meberg A, Vik T (2009) Is breech presentation a risk factor for cerebral palsy? A Norwegian birth cohort study. Dev Med Child Neurol 51:860–865
Nowlan NC, Sharpe J, Roddy KA, Prendergast PJ, Murphy P (2010) Mechanobiology of embryonic skeletal development: insights from animal models. Birth Defects Res C Embryo Today 90:203–213
Giorgi M, Carriero A, Shefelbine SJ, Nowlan NC (2015) Effects of normal and abnormal loading conditions on morphogenesis of the prenatal hip joint: application to hip dysplasia. J Biomech 48:3390–3397
Chan A, McCaul KA, Cundy PJ, Haan EA, Byron-Scott R (1997) Perinatal risk factors for developmental dysplasia of the hip. Arch Dis Child Fetal Neonatal Ed 76:F94–F100
Hinderaker T, Uden A, Reikerås O (1994) Direct ultrasonographic measurement of femoral anteversion in newborns. Skelet Radiol 23:133–135
Tshorny M, Mimouni FB, Littner Y, Alper A, Mandel D (2007) Decreased neonatal tibial bone ultrasound velocity in term infants born after breech presentation. J Perinatol 27:693–696
World Health Organisation (2006) WHO child growth standards: length/height for age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age, methods and development. World Health Organization, Geneva
Hinderaker T, Daltveit AK, Irgens LM, Udén A, Reikerås O (1994) The impact of intra-uterine factors on neonatal hip instability. An analysis of 1,059,479 children in Norway. Acta Orthop Scand 65:239–242
Luterkort M, Persson PH, Weldner BM (1984) Maternal and fetal factors in breech presentation. Obstet Gynecol 64:55–59
Moessinger AC, Blanc WA, Marone PA, Polsen DC (1982) Umbilical cord length as an index of fetal activity: experimental study and clinical implications. Pediatr Res 16:109–112
Wright D, Chan GM (2009) Fetal bone strength and umbilical cord length. J Perinatol 29:603–605
Soernes T, Bakke T (1986) The length of the human umbilical cord in vertex and breech presentations. Am J Obstet Gynecol 154:1086–1087
Hofmeyr GJ, Kulier R, West HM (2015) External cephalic version for breech presentation at term Cochrane Database Syst Rev CD000083
Lambeek AF, De Hundt M, Vlemmix F, Akerboom BM, Bais JM, Papatsonis DN, Mol BW, Kok M (2013) Risk of developmental dysplasia of the hip in breech presentation: the effect of successful external cephalic version. BJOG 120:607–612
Suzuki S, Yamamuro T (1985) Fetal movement and fetal presentation. Early Hum Dev 11:255–263
Witkop CT, Zhang J, Sun W, Troendle J (2008) Natural history of fetal position during pregnancy and risk of nonvertex delivery. Obstet Gynecol 111:875–880
Harvey NC, Cole ZA, Crozier SR et al (2012) Physical activity, calcium intake and childhood bone mineral: a population-based cross-sectional study. Osteoporos Int 23:121–130
Janz KF, Burns TL, Torner JC, Levy SM, Paulos R, Willing MC, Warren JJ (2001) Physical activity and bone measures in young children: the Iowa bone development study. Pediatrics 107:1387–1393
Johannsen N, Binkley T, Englert V, Neiderauer G, Specker B (2003) Bone response to jumping is site-specific in children: a randomized trial. Bone 33:533–539
Funding
KMG is supported by the UK Medical Research Council (MC_UU_12011/4), the National Institute for Health Research (as an NIHR Senior Investigator (NF-SI-0515-10042) and through the NIHR Southampton Biomedical Research Centre) and the European Union’s Erasmus+ Capacity-Building ENeASEA Project. The work was supported by the European Union’s Seventh Framework Programme (FP7/2007-2013), projects EarlyNutrition and ODIN under grant agreement numbers 289346 and 613977, and the ALPHABET project [an award made through the ERA-Net on Biomarkers for Nutrition and Health (ERA HDHL)], Horizon 2020 grant agreement number 696295 (UK component: BBSRC: BB/P028179/1). HMI is supported by the UK Medical Research Council (MC_UU_12011.4). This work was supported by grants from the Medical Research Council, British Heart Foundation, Arthritis Research UK, National Institute for Health Research (NIHR) Southampton Biomedical Research Centre, University of Southampton and University Hospital Southampton NHS Foundation Trust, Nestec and NIHR Biomedical Research Centre, University of Oxford.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by Southampton and Southwest Hampshire Local Research Ethics Committee (approval numbers 267/97, 307/97, 153/99 and 005/03/t) and parental informed consent was given at both scan timepoints.
Conflicts of interest
None.
Electronic supplementary material
Fig. S1
(PPTX 68.7 kb)
Rights and permissions
About this article

Cite this article
Ireland, A., Crozier, S.R., Heazell, A.E.P. et al. Breech presentation is associated with lower bone mass and area: findings from the Southampton Women’s Survey. Osteoporos Int 29, 2275–2281 (2018). https://doi.org/10.1007/s00198-018-4626-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-018-4626-2