
Abstract
Summary
Marked trabecular and cortical bone loss was observed at the proximal femur short-term after spinal cord injury (SCI). 3D-DXA provided measurement of vBMD evolution at both femoral compartments and cortical thinning, thereby suggesting that this technique could be useful for bone analysis in these patients.
Introduction
SCI is associated with a marked increase in bone loss and risk of osteoporosis development short-term after injury. 3D-DXA is a new imaging analysis technique providing 3D analysis of the cortical and trabecular bone from DXA scans. The aim of this study was to assess the evolution of trabecular macrostructure and cortical bone using 3D-DXA in patients with recent SCI followed over 12 months.
Methods
Sixteen males with recent SCI (< 3 months since injury) and without antiosteoporotic treatment were included. Clinical assessment, bone mineral density (BMD) measurements by DXA, and 3D-DXA evaluation at proximal femur (analyzing the integral, trabecular and cortical volumetric BMD [vBMD] and cortical thickness) were performed at baseline and at 6 and 12 months of follow-up.
Results
vBMD significantly decreased at integral, trabecular, and cortical compartments at 6 months (− 8.8, − 11.6, and − 2.4%), with a further decrease at 12 months, resulting in an overall decrease of − 16.6, − 21.9, and − 5.0%, respectively. Cortical thickness also decreased at 6 and 12 months (− 8.0 and − 11.4%), with the maximal decrease being observed during the first 6 months. The mean BMD losses by DXA at femoral neck and total femur were − 17.7 and − 21.1%, at 12 months, respectively.
Conclusions
Marked trabecular and cortical bone loss was observed at the proximal femur short-term after SCI. 3D-DXA measured vBMD evolution at both femoral compartments and cortical thinning, providing better knowledge of their differential contributory role to bone strength and probably of the effect of therapy in these patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
After spinal cord injury (SCI) there is marked bone loss leading to an increased risk of osteoporosis development and fragility fractures, mostly affecting sublesional sites [1,2,3,4]. This bone loss occurs shortly after injury [2, 3, 5, 6] and is especially marked during the first year of SCI [6, 7]. Indeed, prospective studies have reported a 15–20% decrease in bone mineral density (BMD) at total hip within only 12 months [1, 2, 4, 5, 8,9,10,11,12,13,14], resulting in the development of densitometric osteoporosis in up to 60% of these subjects during this period of time [1,2,3, 15].
DXA measurements are limited to two-dimensional evaluation of integral bone mineral mainly at lumbar spine and/or proximal femur and, contrary to quantitative computed tomography (QCT), cannot differentiate between trabecular and cortical bone compartments [6, 16]. In this sense, prospective studies using QCT have shown a higher decrease in bone mass compared to DXA assessment [6, 17], with a reduction of ~ 3% monthly of integral bone mineral content (BMC) and volumetric bone mineral density (vBMD) at proximal femur within the first 6 months after injury [18], and up to 60% decrease of BMC at femoral neck 2 years after injury [4] in both the trabecular and cortical bone compartments [18,19,20]. However, the high-dose radiation and cost, as well as the limited access to QCT, constitute some of the main limitations for its applicability in clinical practice.
Alternatively, 3D analysis methods have been proposed using DXA scans. Solutions were developed to model the femoral shape [21, 22] or the spinal shape [23, 24] in 3D using frontal and lateral DXA scans. Langton et al. [25] proposed a method to model the geometry of the femur by wrapping a template over a frontal DXA scan. Recently, new methods have been proposed to model the bone density distribution in addition to the shape and to analyze the cortical and trabecular bone in 3D from DXA scans [26, 27]. These “3D-DXA” techniques use a proximal femur statistical shape and density model that is registered onto the DXA scan of the patient and provides accurate estimates of trabecular and cortical vBMD and cortical thickness in comparison with QCT. Nevertheless, at present, there are no data on the usefulness of 3D-DXA in patients with SCI, one of the clinical situations associated with the highest and fastest bone loss.
Therefore, the aim of the present study was to analyze the trabecular macrostructure and cortical bone using 3D-DXA in patients with recent SCI and evaluate their evolution during a 12-month follow-up.
Patients and methods
Study design and subjects
This prospective observational study was aimed at analyzing the effect of recent SCI (< 6 months from SCI) on bone turnover and BMD evolution and the factors related to bone loss in these subjects. The detailed study design and characteristics of the participants have been published previously [3]. Forty-two patients with recent motor SCI were initially included in the study and followed every 6 months at the Metabolic Bone Diseases Unit of the Hospital Clinic. Patients with low calcium intake and/or low serum values of 25 hydroxyvitamin D (25OHD) (< 20 ng/ml) were treated with calcium and/or vitamin D supplements. Additionally, in patients with osteoporosis development during follow-up, antiosteoporotic therapy was recommended [28].
In the present study, we evaluated only the patients with at least 12 months of follow-up without antiosteoporotic treatment and with DXA analysis available at all three time points (baseline, 6 months and 12 months of follow-up [20 subjects]). Of the 20 patients, 4 were excluded because the 3D-DXA analysis could not be performed at one of the three time points due to artifacts in the DXA scan (in all cases this was due to the presence of the urinary collector device over the femur). Finally, 16 male patients with recent SCI were included in this study. Clinical assessment and BMD measurements were performed at baseline and at 6 and 12 months of follow-up. This subgroup of 16 SCI patients was comparable in age, body mass index (BMI), and type and duration of time since SCI in relation to the whole group of SCI patients [3] (data not shown).
Ethical approval was obtained from the Neurorehabilitation Guttmann Institute and from the Hospital Clinic of Barcelona Ethics Committees, and all participants provided written informed consent.
Methods
Risk factors for osteoporosis were assessed in all participants, including weight, height (obtained from clinical history of the neurorehabilitation center [measured in the supine position using a recumbent measuring board]), BMI, tobacco and alcohol consumption, dietary calcium intake (mg/day), as well as the main characteristics of the SCI including the level (paraplegia/tetraplegia), type (spastic/flaccid), and severity of SCI (according to the International Standards for Neurological Classification of Spinal Cord Injury [ISNCSCI], assessed by the ASIA Impairment Scale [AIS]) [29].
DXA scans (Lunar Prodigy, General Electric Medical Systems, WI) were acquired at baseline and after a 6- and 12-month follow-up, analyzing the areal bone mineral density (aBMD [g/cm2]) at the proximal femur (neck, trochanter, total femur and femoral shaft) and lumbar spine. The DXA scans were processed using the enCORE 2011 software version 13.60.033 (GE Healthcare). The coefficients of variations are 0.6% for total femur aBMD and 0.8% for lumbar spine aBMD. Osteoporosis was defined according to the WHO criteria [30].
The 3D-DXA software algorithm (version 2.2, Galgo Medical) [26] was used to assess in 3D the trabecular macrostructure and the cortex from DXA scans at baseline, and at 6 and 12 months of follow-up. The method relies on a statistical shape and density model of the proximal femur built from a database of QCT images. The 3D statistical model is registered onto the DXA scan to obtain a 3D patient-specific model of the proximal femur shape and BMD distribution of the patient. The cortical thickness and density is computed by fitting a mathematical function to the density profile computed along the normal vector at each node of the proximal femur surface mesh [31]. 3D-DXA measurements include the vBMD and BMC of the cortical, trabecular and integral (trabecular + cortical) bone compartments, and mean cortical thickness. All 3D-DXA measurements are performed at the total femur. The accuracy of models and measurements provided by the 3D-DXA software algorithm was evaluated in a previous study by comparing 3D-DXA and QCT analyses [26]. Briefly, integral, trabecular, and cortical vBMD computed by QCT and 3D-DXA at total femur have shown correlation coefficients of 0.95, 0.86, and 0.93, respectively. The correlation coefficient between mean cortical thickness computed by 3D-DXA and QCT at total femur was 0.91. The least significant changes (LSC) for the 3D-DXA (measurements evaluated in postmenopausal women) were 0.057 mm for the mean cortical thickness, 16.8 mg/cm3 for the integral vBMD, 15.5 mg/cm3 for the trabecular vBMD, and 16.6 mg/cm3 for the cortical vBMD (total hip) [32].
Statistical analysis
Quantitative variables were described using means and standard deviations (SD) whereas frequencies and percentages were reported for qualitative variables. The 3D-DXA and DXA measurements computed at baseline, 6-, and 12-month follow-up were compared using paired samples Student’s t test. A Bland-Altman plot was used to analyze the agreement between percentage changes in total hip BMC measured by 3D-DXA and DXA. The average cortical thickness and density anatomical distribution were computed at each time points over the 16 study subjects. The statistical significance of the differences found at each vertex of the femoral shape was analyzed using paired samples Student’s t test. All hypothesis tests with a p value lower than 5% were considered significant.
Results
The clinical characteristics of the SCI patients at baseline are shown in Table 1. Briefly, 16 male patients with a mean age of 42.3 ± 18.5 years (range 18–67 years) and complete medullar motor involvement (16 AIS A) were included at 93 ± 25 days after injury. Seven patients had paraplegia and 9 had tetraplegia. The most frequent cause of SCI was traffic accident (63%). Most patients had spasticity (87.5%).
The 12-month evolution of 3D-DXA vBMD, cortical thickness, and BMC is shown in Table 2. As can be seen in the table, the 3D-DXA vBMD significantly decreased at 6 months of follow-up in all femoral compartments: integral vBMD, trabecular vBMD, and cortical vBMD. The mean cortical thickness also decreased up to − 8.0% within the same period of time. The estimated monthly decreases over the first six months of follow-up were − 2.3 and − 1.9% per month for trabecular BMC and vBMD and − 2.0 and − 0.4% per month for cortical BMC and vBMD, respectively. A further decrease in integral vBMD, trabecular vBMD, cortical vBMD, and mean cortical thickness was observed from 6 to 12 months of follow-up. As a result, the overall mean integral, trabecular, and cortical vBMD decreases at 12 months were − 16.6, − 21.9, and − 5.0%, respectively, while the overall decrease in cortical thickness was − 11.4%. BMC values significantly decreased in all the locations evaluated (Table 2).
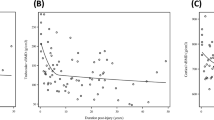
Figure 1 shows the Bland-Altman plot agreement analysis between the percentage changes at 6 and at 12 months of total hip BMC measured by DXA and 3D-DXA. As can be seen in the figure, a confidence interval (± 1.96 SD) between − 8.2 and 12.8 was observed. In addition, the mean difference between percentage changes in BMC measured by DXA and 3D-DXA was not statistically significant (2.3%, p = 0.11, one-sample t test).

Bland-Altman plot showing the agreement between percentage changes in total hip BMC measured by 3D-DXA and by DXA. Solid line represents the mean difference; dotted lines represent the limits of agreement (± 1.96 SD). p value obtained from a one-sample t test. 3D-DXA, three-dimensional dual-energy X-ray absorptiometry; DXA, dual-energy X-ray absorptiometry; BMC, bone mineral content; SD, standard deviation
The anatomical distribution of the changes in cortical thickness and density is shown in Fig. 2. As can be seen at the top of the figure, cortical thinning was more pronounced in regions of thick cortex such as the femoral shaft. However, when computed as a percentage, changes in cortical thickness were rather homogeneously distributed over the femoral shape. A marked decrease in cortical density was observed at the greater trochanter and in the region of the lesser trochanter (bottom of Fig. 2).

Anatomical distribution of the average changes in cortical thickness (in mm and as a percentage) and cortical density (in mg/cm3 and as a percentage) computed by 3D-DXA at 6 and 12 months compared with baseline. The color-coded regions indicate the changes at each vertex compared to baseline, when statistically significant (p < 0.05). The regions in gray indicate nonsignificant changes (p > 0.05). Changes at the femoral head are not shown
As shown in Table 2, aBMD (measured by DXA) markedly decreased at 6 months in all the sites evaluated: femoral neck, trochanter, femoral shaft, and total femur, with a further decrease at the femoral neck, trochanter, femoral shaft, and total femur within 6 to 12 months of follow-up. The resulting overall mean decreases of aBMD at 12 months were as follows: femoral neck (− 17.7%), trochanter (− 23.7%), femoral shaft (− 20.9%), and total femur (− 21.1%) (Table 2).
Discussion
Our study used 3D-DXA to evaluate the evolution of the different bone compartments at the proximal femur in SCI patients. We observed a marked decrease in trabecular (22%) and cortical (5%) vBMD 1 year after SCI, the latter also associated with a significant decrease in cortical thickness (11%).
In a prospective pQCT-based study including patients with recent SCI followed for 12 months, Coupaud et al. [17] observed trabecular and cortical BMC losses of 15 and 3%, respectively, in the distal femur. In our study, a decrease of 20.6% in trabecular BMC and 15.1% in cortical BMC was found at the proximal femur at 12 months. Along the same line, in a group of early SCI patients with 4 months of follow-up analyzed by QCT, Edwards et al. [7, 18, 19, 33] described a marked decrease in trabecular BMC and vBMD (up to 3.1–4.4 and 2.7–4.7% per month, respectively) and also in cortical BMC (3.8–5.4% per month) at the proximal femur, with lower decreases in cortical vBMD (0.6–0.8% per month) at this location. In our study, the estimated monthly decreases over the first six months of follow-up were − 2.3 and − 1.9% per month for trabecular BMC and vBMD and − 2.0 and − 0.4% per month for cortical BMC and vBMD, respectively. It is of note that our 3D-DXA results were concordant with those obtained with QCT. Thus, we observed not only a different magnitude of bone loss of the trabecular and cortical compartments during this early period after SCI but also a similar amount of bone loss in these locations compared with QCT. This bone loss pattern could be attributed to several factors, such as the particular characteristics of the femur, which mainly contains cortical bone, and the markedly high bone remodeling status that occurs in this clinical condition, especially affecting trabecular and endocortical bone [6, 34, 35]. Thus, it should be noted that the absolute amounts of vBMD loss at 12 months were similar in the two compartments (− 47.9 mg/cm3 at trabecular bone and − 42.4 mg/cm3 at cortical bone) (Table 2), indicating that cortical femur sustains the same decrease in total vBMD amount (mg/cm3), but not in the percentage, since cortical bone is denser than trabecular bone. Indeed, we observed a significant decrease in cortical thickness of up to − 11.4% at 12 months after injury, with recent data also indicating a − 8% decrease by QCT in the cross-sectional area (CSA) of the cortical bone at the femoral shaft 1 year after injury [17], further confirming the potential usefulness of 3D-DXA in the analysis of these two bone compartments in SCI patients.
Previous studies have reported higher BMD losses during the first months after injury [1, 2, 6, 13, 34]. In this sense, mean monthly losses of 2% at total hip by DXA [7] and of 3% at integral bone (vBMD and BMC by QCT) [19] have been described within the first months after injury, with up to a 8.3% decrease in integral (BMC) during the first 6 months after injury [33]. In our study, we also observed a monthly aBMD loss by DXA of ~ 2% at total hip within the first 6 months of follow-up (− 14% at 6 months) and ~ 1.5% monthly loss of integral vBMD by 3D-DXA, confirming the marked early bone loss that is produced after injury. Similarly, BMC loss at the total hip seemed to be greater during the first 6 months after injury, with the magnitude being similar with both DXA and 3D-DXA.
Additionally, whereas the bone loss at the trabecular compartment seemed to be similar in magnitude in both 6-month periods during the first year after SCI, bone loss at the cortical compartment was higher during the first 6-month period resulting in a higher initial decrease in cortical thickness. Thus, cortical thickness decreased by 8% in the first 6 months after injury and by 3.7% thereafter (Table 2). Although the reasons for the more marked early cortical decrease are not completely understood, a potential influence of the associated muscle loss could be hypothesized. In fact, marked muscle atrophy usually precedes bone loss and is commonly observed after SCI, with previous studies reporting a good correlation between cortical bone and muscle losses in these subjects [2, 36]. Indeed, when we analyzed the anatomical distribution of the average changes in cortical thickness and density, a more marked decrease was observed in the cortical thickness at the inferior-anterior area in these patients. This is in contrast with previous reports during the aging process in which a relative preservation of the inferior-anterior area is described. This finding was attributed to the mechanical load from walking [37]. Our patients had a complete SCI, all of whom were wheelchair users and thereby lacking muscle strength and loading in this area. All these data may explain the different pattern of bone loss in this clinical situation.
The present results support the potential usefulness of 3D-DXA in these patients, not only in the assessment of the differential evolution of the cortical and trabecular bone compartments after injury but also in evaluating if there is a differential response to antiosteoporotic treatment. Thus, it is well known that trabecular and cortical compartments are both contributors to bone strength, with previous reports indicating the need for the development of noninvasive methodologies to analyze the thickness and density of cortical regions of femur to improve the prediction of fracture risk [38]. It seems logical to assume that having better differentiation between the bone compartments might allow better identification of their differential contribution to bone strength and probably determine if there is a more preferential action of different types of antiosteoporotic treatments. In this sense, denosumab, a potent antiresorptive agent, which has recently shown promising results in osteoporotic SCI patients [28], has also shown to increase bone strength by increasing trabecular and cortical bone compartments [39].
Although DXA measurement is considered the clinical standard for BMD analysis and fracture risk prediction [40], it cannot differentiate between the cortical and trabecular bone compartments [6, 16]. Thus, some authors support the role of other imaging studies such as QCT in SCI. Nonetheless, the lower repeatability at peripheral sites [17], the high-dose radiation, high cost, and limited access to QCT analysis [40] limit the applicability of QCT in clinical practice. For years, 3D modeling approaches using DXA scans were limited to the analysis of bone shape [21,22,23,24,25]. Nowadays, 3D-DXA imaging analysis techniques provide 3D analysis of cortical and trabecular bone density from DXA scans and could be an appropriate and complementary assessment tool in SCI patients. Indeed, our study, which is the first to assess bone mass evolution at the proximal femur by 3D-DXA in early SCI patients, allowed us to assess the trabecular and cortical bone compartments in this clinical situation.
Since DXA provides areal density measurements, a direct comparison with volumetric density measurements by 3D-DXA is not straightforward. Nevertheless, both methods provide the BMC at the total hip, a measurement that can be compared. In the present study, no significant differences were observed between the percentage change in BMC measured by DXA and 3D-DXA, a finding that was corroborated with the Bland-Altman agreement plot observing a CI between − 8.2 and 12.8%, which can be compared with the average percentage decrease in BMC for these SCI patients at 6 and 12 months by DXA. The main limitation of this comparison is related to the definition of the regions of interest used in both approaches. The 3D-DXA total hip region was defined over the 3D subject-specific femoral shapes, while the DXA total hip region was identified in the DXA scan. Further studies are needed to assess the agreement in measuring changes in bone density using 3D-DXA compared to other techniques, such as DXA or QCT, to potentially improve the 3D-DXA measurement technique. In addition, it should be noted that precision is critical to monitor changes in bone density. Variability in BMC changes at 6 and 12 months was quite similar (i.e., similar SD) when measured by DXA and 3D-DXA. However, a greater variability (i.e., higher SD in relation to the mean change) was found for changes in vBMD compared to aBMD. This finding could be partly due to greater intersubject variability and/or to higher precision errors for 3D-DXA measurements in these patients, which could be a potential limitation for 3D-DXA compared to DXA.
The present study has several limitations, such as the absence of a healthy control group, the lower accuracy of 3D-DXA compared to QCT assessment, the higher variability of 3D-DXA compared to DXA, and the low number of patients included in the study. Nonetheless, the homogeneity of our patients, the prospective nature of the study with 1 year follow-up analysis of patients with recent SCI, allows adequate clinical interpretation of the results.
In conclusion, 3D-DXA allowed assessment of the marked bone loss that occurs at both proximal femoral compartments (cortical and trabecular) short-term after SCI. The present data suggest that 3D-DXA could be a useful complementary assessment tool in SCI patients allowing better identification of the differential contribution of the bone compartments to bone strength. Further studies are needed to assess whether the use of this technique will be of benefit in the clinical approach to SCI patients.
Abbreviations
- SCI:
-
Spinal cord injury
- BMD:
-
Bone mineral density
- DXA:
-
Dual-energy X-ray absorptiometry
- QCT:
-
Quantitative computed tomography
- BMC:
-
Bone mineral content
- vBMD:
-
Volumetric bone mineral density
- 3D-DXA:
-
Three-dimensional dual-energy X-ray absorptiometry
- BMI:
-
Body mass index
- AIS:
-
ASIA Impairment Scale
- aBMD:
-
Areal bone mineral density
- SD:
-
Standard deviation
References
Jiang SD, Dai LY, Jiang LS (2006) Osteoporosis after spinal cord injury. Osteoporos Int 17(2):180–192
Giangregorio L, McCartney N (2006) Bone loss and muscle atrophy in spinal cord injury: epidemiology, fracture prediction, and rehabilitation strategies. J Spinal Cord Med 29(5):489–500
Gifre L, Vidal J, Carrasco JL, Filella X, Ruiz-Gaspà S, Muxi A, Portell E, Monegal A, Guañabens N, Peris P (2015) Effect of recent spinal cord injury on wnt signaling antagonists (sclerostin and dkk-1) and their relationship with bone loss. A 12-month prospective study. J Bone Miner Res 30(6):1014–1021
Biering-Sørensen F, Bohr HH, Schaadt OP (1990) Longitudinal study of bone mineral content in the lumbar spine, the forearm and the lower extremities after spinal cord injury. Eur J Clin Investig 20(3):330–335
Garland DE, Stewart CA, Adkins RH, SS H, Rosen C, Liotta FJ, Weinstein DA (1992) Osteoporosis after spinal cord injury. J Orthop Res 10(3):371–378
Edwards WB, Schnitzer TJ (2015) Bone imaging and fracture risk after spinal cord injury. Curr Osteoporos Rep 13(5):310–317
Edwards WB, Schnitzer TJ, Troy KL (2014) Reduction in proximal femoral strength in patients with acute spinal cord injury. J Bone Miner Res 29(9):2074–2079
Bauman WA, Cirnigliaro CM, La Fountaine MF, Martinez L, Kirshblum SC, Spungen AM (2015) Zoledronic acid administration failed to prevent bone loss at the knee in persons with acute spinal cord injury: an observational cohort study. J Bone Miner Metab 33(4):410–421
Bubbear JS, Gall A, Middleton FR, Ferguson-Pell M, Swaminathan R, Keen RW (2011) Early treatment with zoledronic acid prevents bone loss at the hip following acute spinal cord injury. Osteoporos Int 22(1):271–279
Shapiro J, Smith B, Beck T, Ballard P, Dapthary M, BrintzenhofeSzoc K, Caminis J (2007) Treatment with zoledronic acid ameliorates negative geometric changes in the proximal femur following acute spinal cord injury. Calcif Tissue Int 80(5):316–322
Gilchrist NL, Frampton CM, Acland RH, Nicholls MG, March RL, Maguire P, Heard A, Reilly P, Marshall K (2007) Alendronate prevents bone loss in patients with acute spinal cord injury: a randomized, double-blind, placebo-controlled study. J Clin Endocrinol Metab 92(4):1385–1390
Garland DE, Adkins RH, Stewart CA (2008) Five-year longitudinal bone evaluations in individuals with chronic complete spinal cord injury. J Spinal Cord Med. 31(5):543–550
Zehnder Y, Risi S, Michel D, Knecht H, Perrelet R, Kraenzlin M, Zäch GA, Lippuner K (2004) Prevention of bone loss in paraplegics over 2 years with alendronate. J Bone Miner Res 19(7):1067–1074
Zehnder Y, Lüthi M, Michel D, Knecht H, Perrelet R, Neto I, Kraenzlin M, Zäch G, Lippuner K (2004) Long-term changes in bone metabolism, bone mineral density, quantitative ultrasound parameters, and fracture incidence after spinal cord injury: a cross-sectional observational study in 100 paraplegic men. Osteoporos Int 15(3):180–189
Gifre L, Vidal J, Carrasco JL, Muxi A, Portell E, Monegal A, Guañabens N, Peris P (2015) Risk factors for the development of osteoporosis after spinal cord injury. A 12-month follow-up study. Osteoporos Int 26(9):2273–2280
Dudley-Javoroski S, Shields RK (2012) Regional cortical and trabecular bone loss after spinal cord injury. J Rehabil Res Dev 49(9):1365–1376
Coupaud S, McLean AN, Purcell M, Fraser MH, Allan DB (2015) Decreases in bone mineral density at cortical and trabecular sites in the tibia and femur during the first year of spinal cord injury. Bone 74:69–75
Edwards WB, Schnitzer TJ, Troy KL (2013) Bone mineral loss at the proximal femur in acute spinal cord injury. Osteoporos Int 24(9):2461–2469
Edwards WB, Schnitzer TJ, Troy KL (2014) Bone mineral and stiffness loss at the distal femur and proximal tibia in acute spinal cord injury. Osteoporos Int 25(3):1005–1015
Eser P, Frotzler A, Zehnder Y, Denoth J (2005) Fracture threshold in the femur and tibia of people with spinal cord injury as determined by peripheral quantitative computed tomography. Arch Phys Med Rehabil 86(3):498–504
Kolta S, Le Bras A, Mitton D, Bousson V, de Guise JA, Fechtenbaum J, Laredo JD, Roux C, Skalli W (2005) Three-dimensional X-ray absorptiometry (3D-XA): a method for reconstruction of human bones using a dual X-ray absorptiometry device. Osteoporos Int 16(8):969–976
Le Bras A, Kolta S, Soubrane P, Skalli W, Roux C, Mitton D (2006) Assessment of femoral neck strength by 3-dimensional X-ray absorptiometry. J Clin Densitom 9(4):425–430
Kolta S, Quiligotti S, Ruyssen-Witrand A, Amido A, Mitton D, Bras AL, Skalli W, Roux C (2008) In vivo 3D reconstruction of human vertebrae with the three-dimensional X-ray absorptiometry (3D-XA) method. Osteoporos Int 19(2):185–192
Kolta S, Kerkeni S, Travert C, Skalli W, Eastell R, Glüer CC, Roux C (2012) Variations in vertebral body dimensions in women measured by 3D-XA: a longitudinal in vivo study. Bone 50(3):777–783
Langton CM, Pisharody S, Keyak JH (2009) Generation of a 3D proximal femur shape from a single projection 2D radiographic image. Osteoporos Int 20(3):455–461
Humbert L, Martelli Y, Fonolla R, Steghofer M, Di Gregorio S, Malouf J, Romera J, Barquero LM (2017) 3D-DXA: assessing the femoral shape, the trabecular macrostructure and the cortex in 3D from DXA images. IEEE Trans Med Imaging 36:27–39
Väänänen SP, Grassi L, Flivik G, Jurvelin JS, Isaksson H (2015) Generation of 3D shape, density, cortical thickness and finite element mesh of proximal femur from a DXA image. Med Image Anal 24:125–134
Gifre L, Vidal J, Carrasco JL, Muxi A, Portell E, Monegal A, Guañabens N, Peris P (2016) Denosumab increases sublesional bone mass in osteoporotic individuals with recent spinal cord injury. Osteoporos Int 27(1):405–410
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M, Jones L, Krassioukov A, Mulcahey MJ, Schmidt-Read M, Waring W (2011) International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med 34(6):535–546
Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 843:1–129
Humbert L, Hazrati Marangalou J, del Río Barquero LM, van Lenthe GH, van Rietbergen B (2016) Technical note: cortical thickness and density estimation from clinical CT using a prior thickness-density relationship. Med Phys 43:1945–1954
Humbert L, Di Gregorio S, Del Rio L (2017) Short-term precision assessment and monitoring time interval to assess bone status in postmenopausal women by 3D-DXA. Osteoporos Int 28(suppl 1):462
Edwards WB, Schnitzer TJ, Troy KL (2014) The mechanical consequence of actual bone loss and simulated bone recovery in acute spinal cord injury. Bone 60:141–147
Troy KL, Morse LR (2015) Measurement of bone: diagnosis of SCI-induced osteoporosis and fracture risk prediction. Top Spinal Cord Inj Rehabil 21(4):267–274
Minaire P, Berard E, Meunier PJ, Edouard C, Goedert G, Pilonchery G (1981) Effects of disodium dichloromethylene diphosphonate on bone loss in paraplegic patients. J Clin Invest 68(4):1086–1092
Dionyssiotis Y, Stathopoulos K, Trovas G, Papaioannou N, Skarantavos G, Papagelopoulos P (2015) Impact on bone and muscle area after spinal cord injury. Bonekey Rep 4:633
Poole KE, Mayhew PM, Rose CM, Brown JK, Bearcroft PJ, Loveridge N, Reeve J (2010) Changing structure of the femoral neck across the adult female lifespan. J Bone Miner Res 25(3):482–491
Crabtree N, Loveridge N, Parker M, Rushton N, Power J, Bell KL, Beck TJ, Reeve J (2001) Intracapsular hip fracture and the region-specific loss of cortical bone: analysis by peripheral quantitative computed tomography. J Bone Miner Res 16(7):1318–1328
Keaveny TM, McClung MR, Genant HK, Zanchetta JR, Kendler D, Brown JP, Goemaere S, Recknor C, Brandi ML, Eastell R, Kopperdahl DL, Engelke K, Fuerst T, Radcliffe HS, Libanati C (2014) Femoral and vertebral strength improvements in postmenopausal women with osteoporosis treated with denosumab. J Bone Miner Res 29(1):158–165
Engelke K, Lang T, Khosla S, Qin L, Zysset P, Leslie WD, Shepherd JA, Schousboe JT (2015) Clinical use of quantitative computed tomography (QCT) of the hip in the management of osteoporosis in adults: the 2015 ISCD official positions—part I. J Clin Densitom 18(3):338–358
Funding
The study was funded by the Fundació la Marató de TV3. LH received support by the Programa Estatal de Promoción del Talento y su Empleabilidad—Torres Quevedo, Ministerio de Economía y Competitividad (Reference: SPTQ1300X006124XV0).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval was obtained from the Neurorehabilitation Guttmann Institute and from the Hospital Clinic of Barcelona Ethics Committees, and all participants provided written informed consent.
Conflicts of interest
Ludovic Humbert is a stakeholder of Galgo Medical. LG, AM, LR, JV, EP, AMo, NG, and PP state that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Gifre, L., Humbert, L., Muxi, A. et al. Analysis of the evolution of cortical and trabecular bone compartments in the proximal femur after spinal cord injury by 3D-DXA. Osteoporos Int 29, 201–209 (2018). https://doi.org/10.1007/s00198-017-4268-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-017-4268-9