
Abstract
Summary
This is the first study analyzing concomitantly osteoprotegerin (OPG)/receptor activator of nuclear factor kappa B ligand (RANKL) polymorphisms and OPG/RANKL serum levels and their association with bone mineral density (BMD), vertebral fractures, and vascular aortic calcification in a cohort of 800 subjects in community-dwelling older individuals.
Introduction
Osteoprotegerin (OPG) and RANKL play an important role in osteoclast activation and differentiation as well as in vascular calcification. At present, there are no studies of OPG or RANKL gene polymorphisms in Brazilian older populations. The aim of this study was to evaluate OPG/RANKL polymorphism and their association with vertebral fractures (VFs) and aortic calcification.
Methods
Eight hundred subjects (497 women/303 men) were genotyped for the OPG 1181G>C (rs2073618), 163C>T (rs3102735), 245T>G (rs3134069), and 209G>A (rs3134070) and RANKL A>G (rs2277438) single-nucleotide polymorphisms (SNPs). VFs were evaluated by spine radiography (Genant’s method). Aortic calcification was quantified using Kauppila’s method.
Results
The isolated genotype analyses and single-allele frequency data showed association of OPG 163C, 245G, and 209A alleles with presence of VFs (P < 0.05). Multiple logistic regression of subjects with absence of VFs vs. those with VFs (grades II/III) revealed only OPG 209A homozygosity as a risk factor for higher-grade VFs (odds ratio (OR) = 4.17, 95 % CI 1.03–16.93, P = 0.046). Regarding aortic calcification, the isolated genotype analysis frequency data revealed a significant association of OPG 1181G, 163C, 245G, and 209A alleles with absent aortic calcification (P < 0.05). Multiple logistic regression data confirmed that the OPG 209A allele was protective for aortic calcification (OR = 0.63, 95 % CI 0.45–0.88, P = 0.007) and the OPG 1181C allele was a risk factor for aortic calcification (OR = 1.26, 95 % CI 1.00–1.58, P = 0.046).
Conclusion
This study showed that the OPG 209AA genotype was a risk factor for higher-grade VFs, the OPG 209A allele was protective for aortic calcification, and the OPG 1181C was a risk factor for aortic calcification, supporting the involvement of OPG polymorphisms in the analyzed phenotypes and the concept that the related pathogenesis is multifactorial.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoprotegerin (OPG) is a glycoprotein produced by osteoblasts and a member of the tumor necrosis factor receptor superfamily. With a key role in bone remodeling, OPG acts as a soluble decoy receptor for the receptor activator of nuclear factor kappa B ligand (RANKL), a protein expressed on the osteoblast surface. OPG binding to RANKL blocks the interaction of the latter with the receptor activator of nuclear factor kappa B (RANK) on the osteoclast membrane. This OPG-RANKL interaction plays an antiresorptive role in bone [1]; it induces osteoclast apoptosis and inhibits osteoclast recruitment and activation.
OPG has a key role in the pathogenesis of osteoporosis [2–4], which is a complex bone disease with a strong genetic component [5]. Several genes and their polymorphisms have been associated with bone mineral density and osteoporosis, including transforming growth factor b1 (TGFB1) [6], vitamin D receptor (VDR) [7], estrogen receptor (ESR) [8], collagen type 1 alpha-1 (COL1A1) [9], and OPG [10–12]. OPG overexpression in transgenic mice results in osteopetrosis, while OPG knockout mice develop severe osteoporosis and arterial calcification [13].
Vascular calcification of normal tissue was previously recognized as a common component of atherosclerotic lesions. Previous evidence suggests that calcification of atherosclerotic arteries is an organized, regulated process rather than just a passive phenomenon of aging [14]. Several factors related to bone and mineral formation have been demonstrated within atherosclerotic plaques, including osteocalcin, osteopontin, osteonectin, bone morphogenetic proteins, and OPG [15, 16]. In addition, epidemiological studies have linked bone metabolism to aortic calcification [17, 18], including an analysis of a Brazilian population [19].
Previous studies that evaluated the association between OPG single-nucleotide polymorphisms (SNPs) and bone mineral density (BMD) displayed heterogeneous results that can likely be explained by ethnic diversity [3, 4, 10, 12, 20–24]. Several studies have analyzed the potential association of the 1181G>C, 245T>G, 163C>T, and 209G>A SNPs with BMD, osteoporosis, and fragility fractures [3, 12, 21, 24–30]. However, no published study has concurrently evaluated the potential association of such SNPs with the risk of vertebral fractures and aortic calcification, particularly in a miscegenated population.
The aims of this study were to evaluate OPG/RANKL gene polymorphisms (OPG SNPs 1181G>C, 245T>G, 163C>T, 209G>A; RANKL A>G) and OPG/RANKL serum levels in a Brazilian community-dwelling older representative population and to analyze their potential association with the prevalence of vertebral fractures and vascular aortic calcification.
Methods
Subjects
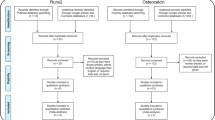
This study was based on data from the São Paulo Ageing & Health Study (SPAH). The survey was conducted on 65-year-old and over individuals living in a community in the Butantã district, located on the western zone of the city of São Paulo. Full details regarding the study population, assessments, and procedures have been previously reported [31]. Of the original 1020 participants, 205 (20 %) were excluded for the following reasons: 50 were using treatment drugs or supplements that affected bone metabolism (including bisphosphonates, vitamin D, and calcium), 104 were using lipid-lowering drugs or supplements, 18 had a past history of cancer (<5 years), 15 had primary hyperparathyroidism (serum calcium >10.5 mg/dL and PTH >65 pg/mL), 12 were in stage 5 of chronic kidney disease (estimated glomerular filtration rate (eGFR) <15 mL/min), and 6 had rheumatoid arthritis. None of the individuals included in our study presented with thyrotoxicosis based on the TSH and T4L serum levels. Hormone replacement therapy (HRT) and glucocorticoid (GC) used were not excluded.
Of the remaining 815 participants, 800 had DNA samples collected (497 women and 303 men) and were included in the genotype-based analyses.
This study was approved by the local ethics committee (no. 426/06), and all the participants provided written informed consent.
Data collection and assessments
Each subject was interviewed by a physician and responded to a standard questionnaire designed to gather information on putative risk factors for osteoporosis or fractures, including previous fragility fractures, family history of hip fractures, current smoking habits, current alcohol use, current use of glucocorticoids, daily calcium intake, history of falls during the past year, level of physical activity, lifestyle [31], and personal or family history of cardiovascular disease [19].
BMD measurement
Dual-energy X-ray absorptiometry (DXA) performed using a Hologic 4500 Discovery densitometry device (Hologic Inc. Bedford, MA, USA) was used to measure bone mineral density (BMD) at the following regions: lumbar spine, femoral neck, and total hip. All BMD measurements were performed by the same experienced technologist. Anatomically abnormal vertebrae were excluded from analysis of lumbar spine if they were clearly abnormal and not assessable within the resolution of the system or if there was more than a 1.0-T score difference between the analyzed vertebrae and the adjacent one, as recommended by the International Society for Clinical Densitometry (ISCD) [32]. We calculated the least significant change with 95 % confidence to be 0.033 g/cm2 for AP spine, 0.047 g/cm2 for femoral neck, and 0.039 g/cm2 for total femur.
BMD characterization was performed in the older subjects according to the WHO classification: normal, T-score ≥−1; osteopenia, T-score <−1 and >−2.5; and osteoporosis, T-score ≤−2.5 in the spine, femoral neck, or total hip sites [32].
Assessment of vertebral fracture
Standard lateral thoracic and lumbar spine radiographs were taken using a 40-in tube-to-film distance centered at T7 and L2. All images provided good visibility of all vertebrae from T4 to L4, and vertebrae could be reliably identified. Two experienced readers concomitantly performed the identification of vertebral fractures. Each of the T4–L4 vertebral images was evaluated. The agreement rate between the readers, which was established on a random subsample of 60 radiographs, was 96 % with a kappa coefficient of 0.82.
Vertebral fractures were classified using the Genant SQ approach. Each identified fractured vertebra was graded based on the Genant SQ scale, where mild (grade I) refers to a 20–25 % reduction of the anterior, middle, and/or posterior height; moderate (grade II) refers to a 26–40 % reduction in any height; and severe (grade III) refers to a >40 % reduction in any height [33].
Assessment of abdominal aortic calcification
The lateral lumbar spine radiographs were also used to quantify aortic calcification. Briefly, the index of abdominal aortic calcium deposit grades the severity of aortic calcification at the level of the first to the fourth lumbar vertebrae. Calcific deposits were considered present if the densities were visible in an area that was parallel to the lumbar spine and anterior to the lower part of the spine. These calcific densities were graded on a 0 to 3 scale at each lumbar vertebral segment: 0 denoted no aortic calcific deposits; 1 indicated small, scattered calcific deposits that occupied less than one third of the longitudinal wall of the aorta; 2 denoted that one to two thirds of the longitudinal aortic wall was calcified; and 3 indicated that two thirds or more of the aortic longitudinal wall was calcified. Separate scores were determined for the anterior and posterior walls of the aorta, and the values were summed across the four vertebrae. This resulted in an abdominal aortic calcium score (AACS) ranging from 0 to 24 [34]. The reproducibility of AACS blind assessment was analyzed using the Wilcoxon test for sum score as continuous and categorized data. In both cases, the P values were >0.10 (P = 0.129 for the continuous data analysis and P = 0.99 for the categorized data analysis), confirming appropriate level of reproducibility.
Measurement of OPG and RANKL serum concentration
Blood samples were collected under fasting conditions (between 8 and 10 a.m.) on the same day that the DXA and abdominal X-rays were obtained, and the samples were stored at −70 °C for later analysis.
The serum samples were analyzed using standard procedures, as outlined by the manufacturers. Serum OPG and free soluble RANKL (sRANKL) were measured using enzyme immunoassays (human OPG ELISA and sRANKL ELISA, Biomedica, Vienna, Austria) [35]. The detection limit established by the manufacturer was 0.02 pmol/L for sRANKL and 0.14 pmol/L for OPG. Thirty-seven percent (288/767) of the samples analyzed for sRANKL presented sRANKL values zero. The inter-assay and intra-assay CVs were 3.9 and 1.3 % for sRANKL and 6.2 and 1.1 % for OPG, respectively.
Genotyping
Genomic DNA was isolated from peripheral blood leukocytes using the salting-out methodology [35], and it was stored at −70 °C prior to analysis. The TaqMan allelic discrimination method was employed for genotyping, using specific probes labeled with VIC and FAM (Applied Biosystems, Foster City, CA, USA).
The analyzed SNPs were chosen in relation to previous data in the literature that suggested possible associations with bone mass, fracture risk, and functional significance [3–6, 10, 12]. The chosen SNPs comprised 1181G>C (rs2073618), located in exon 1 of OPG; 245T>G (rs3134069), 163C>T (rs3102735) and 209G>A (rs3134070), located in the promoter of OPG (chromosomal location 8q24) [25, 36]; and rs2277438, located in a 5′ untranslated region (UTR) of RANKL (13q14) [36].
All SNPs were genotyped using commercial TaqMan assays (OPG assay IDs: rs2073618: C_1971047_1; rs3134069: C_27464534_10; rs3102735: C_1971046_10; rs3134070: C_27466052_10 and RANKL assay ID: rs2277438: C_25473654_10) with TaqMan Genotyping Master Mix and were measured using a StepOne plus detection system (Applied Biosystems). Cycling conditions consisted of a denaturation step at 95 °C for 10 min followed by 40 cycles of denaturation at 92 °C for 15 s and annealing for 1 min at 60 °C.
To assess the genotyping quality, the SNPs were analyzed twice in 5 % of the all samples, yielding a 98 % concordance.
Statistical analysis
Allele frequencies were estimated using the gene counting method, and departures from the Hardy–Weinberg equilibrium were tested using a χ 2 test. The Kolmogorov–Smirnov normality test was applied for continuous and semi-continuous variables. Data with normal distributions are expressed as the mean ± standard deviation and were compared using the independent Student’s t test, with Welch’s adjustment when required. Non-parametric variables were analyzed by the Mann-Whitney’s test and are expressed as the median and the 25 and 75 percentiles. Categorical variables are expressed as absolute (n) and relative (%) frequencies and were analyzed using the Pearson’s chi-squared test and a calculated crude odds ratio.
For the development of the logistic regression model, continuous variables were categorized according to the inflection point on the receiver operating characteristic (ROC) curve and categorical variables underwent a chi-squared test. The variables with likelihood ratios associated with P < 0.20 were chosen and introduced as candidates for the logistic model and were adjusted through confusion co-variables. The compartmental model was applied for major performance of the logistic regression, with the variables grouped by similarity.
The logistic regression models included calculations of corresponding crude and adjusted odds ratios (ORs) and 95 % confidence intervals (CI).
Age was shown to affect the evaluated outcomes and was included in the multiple regression analyses. On the other hand, body mass index (BMI) and gender were not associated with such outcomes (P>0.2), being not included in those analyses. Moreover, gender- and age-adjusted and non-adjusted analyses performed for the SNPs found to be associated with vertebral fractures and aortic calcification (OPG 209G>A and 1181G>C) led to regression models that yielded similar odds ratio values. In this scenario, we decided to use the non-adjusted analysis based on a higher P value in the Hosmer–Lemeshow test (0.975 vs. 0.304).
Two-tailed P values ≤0.05 were considered significant. Statistical analyses were carried out using SPSS for Windows version 19.0 (Chicago, IL, USA).
Results
Allelic frequencies did not deviate from the Hardy–Weinberg equilibrium. Linkage disequilibrium among OPG SNPs was evaluated using Lewontin’s standardized coefficient, and no significant disequilibrium was detected. The demographic, anthropometric, and clinical data of the 800 subjects (497 women and 303 men) are shown in Table 1.
Only 1.38 % of the subjects included in the analyzed population were using GC, and 21 women (2.62 % of the sample) were taking HRT, not affecting the performed analyses. Our study included 12.4 % of the individuals with vitamin D deficiency (<10 ng/mL) and 55.6 % with <20 ng/mL. In both cases, vitamin D serum levels were not significantly associated with vertebral fracture grade and aortic calcification.
Vertebral fractures and OPG and RANKL SNPs
The vertebral fractures were classified as grades I, II, and III and analyzed according to SNP-based genotypes and alleles. The groups (absence of vertebral fracture (VF), grade I VF, and grades II/III VF) were gender balanced. Analysis of the isolated genotypes and single-allele frequencies revealed association between the 163C, 245G, and 209A alleles of OPG and presence of vertebral fractures (P < 0.05) (Table 2). The individual genotype analysis yielded no significant results for the RANKL A>G SNP, but the allele evaluation showed a significantly higher frequency of the G allele in patients with no vertebral fractures (P = 0.024) (Table 2).
Multiple logistic regression of subjects with absence of VFs vs. those with VFs (grade II/III) revealed OPG 209A homozygosity as a risk factor for VF grades II/III (OR = 4.17, 95 % CI 1.03—16.93, P = 0.046) (Table 3). A similar trend, though not significant, was also observed for the 209GA genotype (P = 0.053), strengthening the risk factor effect of the 209A allele. No difference was observed with adjustment for age, gender, BMI, GC use, and HRT use regarding vertebral fractures. Moreover, no significant differences were observed with respect to eGFR and vertebral fractures (absence of fracture plus eGFR ≥60 mL/min 78.2 % vs. absent of fracture plus eGFR <60 mL/min 80.9 %, P = 0.433)
BMD WHO classification and OPG and RANKL SNPs
Among the evaluated SNP genotypes and alleles, only the OPG 163T allele was associated with a lower frequency of osteoporosis (P = 0.033) (data not shown). No significant difference in WHO classification was observed in composed genotype analyses including the OPG SNPs 1181G>C, 163C>T, 245T>G, and 209G>A or the RANKL SNP A>G (data not shown).
Abdominal aortic calcification and OPG and RANKL SNPs
Abdominal aortic calcification was classified by absence (AACS = 0) or presence (AACS>0) of aortic calcification, and the frequency of calcification was determined for each of the evaluated OPG and RANKL SNP genotypes and alleles.
Isolated genotype analysis frequency showed a significant association of OPG 163C, 245G, and 209A alleles with absent vascular aortic calcification, while the 1181C allele was found to be associated with presence of aortic calcification (P < 0.05) (Table 4). Multiple logistic regression data confirmed that the OPG 209A allele was protective for aortic calcification (OR = 0.63, 95 % CI 0.45–0.88, P = 0.007) and OPG 1181C allele was a risk factor for aortic calcification (OR = 1.26, 95 % CI 1.00–1.58, P = 0.046) (Table 5(A)). The observation that the 209GA genotype is protective for aortic calcification (OR = 0.18, 95 % CI 0.05–0.70, P = 0.013; Table 5(B)) strengthens the 209A allele effect. Since the protective effect is also expected for the 209AA genotype and a non-significant trend for protection was indeed detected (OR = 0.29, 95 % CI 0.07–1.14, P = 0.076; Table 5(B)), this lack of significance likely occurred due to the low number of individuals present in this genotype group. Pearson’s chi-squared analyses supported this interpretation and corroborated the mentioned findings, revealing that the 209AA and 1181GG genotypes were associated with absence of aortic calcification (Table 4).
No difference was observed with adjustment for age, gender, BMI, GC use, and HRT use regarding vascular aortic calcification. Moreover, no significant differences were observed with respect to eGFR and aortic calcification (no aortic calcification plus eGFR ≥60 mL/min 37.4 % vs. no aortic calcification plus eGFR <60 mL/min 31.2 %; P = 0.097)
OPG and RANKL serum concentration vs. vertebral fractures, aortic calcification, and OPG and RANKL SNPs
The OPG and RANKL serum concentrations were determined in all of the evaluated subjects. Using a ROC curve approach, the OPG serum level was compared between patient groups with the presence (grades I, II, or III) or absence of vertebral fractures. Bivariated analyses using three different age ranges (60–69, 70–79, 80–89 years old) revealed no significant differences in OPG levels among the absence of VF, grade I VF, and grade II/III VF groups; consequently, no adjustment for age was made.
The analysis revealed that OPG concentration values ≥9.7 ng/mL displayed greater accuracy to discriminate the two groups. The frequency of subjects with OPG ≥9.7 was significantly lower in subjects with absence of vertebral fractures compared to those with grade I and grade II/III fractures (15.1 vs. 25.2 % and 24.6 %, respectively, P = 0.003).
A positive association was also found between OPG ≥9.7 ng/mL and the OPG 163 CC/CT composed genotypes (OR = 1.24, 95 % CI 1.003–1.535, P = 0.047). No association was detected for the other evaluated SNPs, including 1181G>C SNP alleles and genotypes and OPG serum levels.
However, no significant difference in OPG serum concentration was observed between individuals with absence or presence of aortic calcification (OPG ≥9.7 ng/mL, 15.5 vs. 19.1 %, P = 0.231). Although a significant P value (P < 0.001) was observed between aortic calcification score (AACS) and OPG serum levels, no significant correlation was detected because lower linearity was below 0.2 (r = 0.16). In addition, no association between RANKL serum levels and vertebral fractures or aortic calcification was detected (data not shown).
Discussion
The relationship between OPG gene polymorphisms and BMD has been addressed in previous studies [4, 24–26, 28, 30, 37–39]. However, this study is the first to analyze potential associations of such SNPs with BMD, osteoporosis, fractures, and abdominal calcification.
Our isolated allele and genotype analyses showed association between the 163C, 245G, and 209A alleles of OPG and presence of vertebral fractures. Further logistic multivariate analysis showed that 209A homozygosity is a risk factor for vertebral fracture grades II and III in community-dwelling older subjects. This SNP is positioned in the OPG promoter region, which rules out its interference on the amino acid sequence but opens the possibility of significant transcription modulation.
Only few studies evaluated vertebral fractures and 209G>A OPG polymorphism [3, 40, 41]. Previous findings in a Danish population showed that the OPG 163C and 245G alleles were significantly more common in patients with vertebral fractures [3]. Although this Danish study was a case–control that compared patients from a reference hospital with a history of fractures with healthy subjects with many confounding factors, such as bone-affecting medications, these data were comparable to our results obtained with older Brazilian subjects. Some studies found that the 209G>A OPG polymorphism is in linkage disequilibrium with 245T>C OPG, an observation that may explain our findings.
In contrast, in a study of a Spanish population from Barcelona, the risk of fractures was not associated with the 1181G>C and 245T>G OPG SNPs [42]. Surprisingly, in community-dwelling White women from the USA, the OPG 1181CC genotype was associated with not only a higher BMD but also an increased risk of hip fractures. The authors suggested that different genetic factors contribute to trabecular and cortical bone mass and risk for fractures, an interpretation that could potentially explain the opposite findings for spine and hip fractures [27].
The presence of a 163T OPG allele is a protective factor for osteoporosis (BMD WHO classification). Similarly, in a Danish population, Langdall et al. observed that the OPG 163C>T SNP significantly influenced BMD [3]. Additionally, in Asian populations, the OPG 163C>T SNP was associated with BMD [24, 28, 43]. A recently published meta-analysis of 14 studies investigated associations between the seven most common OPG polymorphisms and osteoporosis risk and showed that the 163C>T and 1181G>C OPG SNPs were significantly associated with the risk of osteoporosis [44]. This meta-analysis also suggested that the 163C allele is associated with an increased risk of osteoporosis, corroborating our findings.
Other relevant findings in our analysis were the association of OPG serum levels above 9.7 ng/mL with the risk for vertebral fractures as well as between these higher serum levels and the OPG 163 CC/CT composed genotypes. Consistent with our data, Jørgensen et al. found an increase in height loss following an increase in baseline OPG levels in males and females of a Norwegian population. However, these authors did not analyze any of the OPG polymorphisms [30]. Our observation that the OPG 163C allele was associated with osteoporosis in the analyzed population suggests an inappropriate regulation of the RANKL/RANK/OPG system, leading to increased bone resorption likely secondary to higher osteoclast activation. In this scenario, a compensatory response is necessary to protect BMD in patients at higher risk for osteoporosis, including elevation of OPG levels. It must be noted that the OPG 163C>T SNP is also located in the gene promoter region.
Our data showed that two OPG polymorphisms are relevant for the vascular phenotype: the 1181C allele constitutes a risk factor for abdominal aortic calcification, whereas 209A has a protective influence on this phenotype. Interestingly, no significant differences regarding aortic calcification and eGFR were observed in our population (data not shown).
Despite the well-established association between vascular calcification and bone metabolism, our study displayed some divergent data. While the presence of the 209A OPG homozygosity was found to be a risk factor for fracture, 209GA/AA exhibited a protective profile for aortic calcification in our community-dwelling subjects. Some confounding variables could potentially explain these data. In fact, some of the pathological factors underlying vascular calcification/atherosclerosis seem to protect against osteoporosis, such as high BMI, female gender, high alcohol intake, etc.
Some studies have reported a positive association between the 1181C OPG allele and cardiovascular events [45, 46], but BMD and fracture fragility were not analyzed in their populations. In contrast to our study, which revealed a protective role of the OPG 209A allele toward the development of aortic calcification, other authors found no association between the OPG 209G>A polymorphism and cardiovascular disease [46]. Therefore, additional studies are necessary to address the biological effects of the alleles associated with the OPG 1181G>C and 209G>A SNPs, with emphasis on bone metabolism and related pathology. Analyses of associations between other possible OPG genetic variants with BMD, fractures, or aortic calcification may clarify the clinical data in ethnically distinct populations and help to elucidate molecular mechanisms underlying bone metabolism and the pathogenesis of cardiovascular disease. Moreover, some discordant results in the literature could be related to the complexity of the biology encoded within this region of the genome
In contrast to other reports that analyzed ethnically homogeneous populations, including White American, Spanish, Danish, Italian, Korean, and Chinese [3, 12, 20, 24, 42], our study is original since it comprised a large, well-characterized, and miscegenated older community, without any ethnic predominance. Another strength of this analysis was the exclusion of patients on drugs that affect bone metabolism and lipid profiles. Additional relevant and confounding variables, such as primary hyperparathyroidism, kidney failure, cancer, and rheumatoid arthritis, were also excluded from our study. The inclusion of patients with such chronic conditions may have prevented the drawing of more definitive conclusions in previous reports [3, 47]. The concurrent analysis of two chronic health conditions, namely osteoporosis and vascular calcification, which are anchored on common underlying pathogenic factors, is one more strength of our study [13, 48]. Given the potential role of OPG in controlling bone remodeling [49] and aortic calcification [50], this protein is a robust candidate for modulating bone mass and influencing bone fractures and aortic calcification.
While our study corroborates several results reported by other investigators, it brings some distinct findings. These data indicate that such genetic associations must be interpreted with caution, particularly within the current setting of limited biological information. The results provided by our and others’ reports suggest a significant impact of ethnic background on such analyses, and the existence of a variety of factors capable of influencing bone metabolism and related medical complications.
References
Khosla S (2001) Minireview: the OPG/RANKL/RANK system. Endocrinology 142:5050–5055. doi:10.1210/endo.142.12.8536
Pocock NA, Eisman JA, Hopper JL et al (1987) Genetic determinants of bone mass in adults. A twin study. J Clin Invest 80:706–710. doi:10.1172/JCI113125
Langdahl BL, Carstens M, Stenkjaer L, Eriksen EF (2002) Polymorphisms in the osteoprotegerin gene are associated with osteoporotic fractures. J Bone Miner Res 17:1245–1255. doi:10.1359/jbmr.2002.17.7.1245
Arko B, Prezelj J, Kocijancic A et al (2005) Association of the osteoprotegerin gene polymorphisms with bone mineral density in postmenopausal women. Maturitas 51:270–279. doi:10.1016/j.maturitas.2004.08.006
Ralston SH (2002) Genetic control of susceptibility to osteoporosis. J Clin Endocrinol Metab 87:2460–2466. doi:10.1210/jcem.87.6.8621
Yamada Y (2001) Association of polymorphisms of the transforming growth factor-beta1 gene with genetic susceptibility to osteoporosis. Pharmacogenetics 11:765–771
Kurt O, Yilmaz-Aydogan H, Uyar M et al (2012) Evaluation of ERalpha and VDR gene polymorphisms in relation to bone mineral density in Turkish postmenopausal women. Mol Biol Rep 39:6723–6730. doi:10.1007/s11033-012-1496-0
Ioannidis JPA, Ralston SH, Bennett ST et al (2004) Differential genetic effects of ESR1 gene polymorphisms on osteoporosis outcomes. JAMA 292:2105–2114. doi:10.1001/jama.292.17.2105
Mann V, Ralston SH (2003) Meta-analysis of COL1A1 Sp1 polymorphism in relation to bone mineral density and osteoporotic fracture. Bone 32:711–717
Yamada Y, Ando F, Niino N, Shimokata H (2003) Association of polymorphisms of the osteoprotegerin gene with bone mineral density in Japanese women but not men. Mol Genet Metab 80:344–349. doi:10.1016/S1096-7192(03)00125-2
Vidal C, Formosa R, Xuereb-Anastasi A (2011) Functional polymorphisms within the TNFRSF11B (osteoprotegerin) gene increase the risk for low bone mineral density. J Mol Endocrinol 47:327–333. doi:10.1530/JME-11-0067
Arko B, Prezelj J, Komel R et al (2002) Sequence variations in the osteoprotegerin gene promoter in patients with postmenopausal osteoporosis. J Clin Endocrinol Metab 87:4080–4084. doi:10.1210/jc.2002-020124
Bucay N, Sarosi I, Dunstan CR et al (1998) osteoprotegerin-deficient mice develop early onset osteoporosis and arterial calcification. Genes Dev 12:1260–1268
Demer LL, Watson KE, Bostrom K (1994) Mechanism of calcification in atherosclerosis. Trends Cardiovasc Med 4:45–49. doi:10.1016/1050-1738(94)90025-6
Fitzpatrick LA, Severson A, Edwards WD, Ingram RT (1994) Diffuse calcification in human coronary arteries. Association of osteopontin with atherosclerosis. J Clin Invest 94:1597–1604. doi:10.1172/JCI117501
Bostrom K, Watson KE, Horn S et al (1993) Bone morphogenetic protein expression in human atherosclerotic lesions. J Clin Invest 91:1800–1809. doi:10.1172/JCI116391
von der Recke P, Hansen MA, Hassager C (1999) The association between low bone mass at the menopause and cardiovascular mortality. Am J Med 106:273–278
Schulz E, Arfai K, Liu X et al (2004) Aortic calcification and the risk of osteoporosis and fractures. J Clin Endocrinol Metab 89:4246–4253. doi:10.1210/jc.2003-030964
Figueiredo CP, Rajamannan NM, Lopes JB et al (2013) Serum phosphate and hip bone mineral density as additional factors for high vascular calcification scores in a community-dwelling: the Sao Paulo Ageing & Health Study (SPAH). Bone 52:354–359. doi:10.1016/j.bone.2012.10.019
Choi JY, Shin A, Park SK et al (2005) Genetic polymorphisms of OPG, RANK, and ESR1 and bone mineral density in Korean postmenopausal women. Calcif Tissue Int 77:152–159. doi:10.1007/s00223-004-0264-0
Ohmori H, Makita Y, Funamizu M et al (2002) Linkage and association analyses of the osteoprotegerin gene locus with human osteoporosis. J Hum Genet 47:400–406. doi:10.1007/s100380200058
Vidal C, Brincat M, Xuereb Anastasi A (2006) TNFRSF11B gene variants and bone mineral density in postmenopausal women in Malta. Maturitas 53:386–395. doi:10.1016/j.maturitas.2005.11.003
Wynne F, Drummond F, O’Sullivan K et al (2002) Investigation of the genetic influence of the OPG, VDR (Fok1), and COLIA1 Sp1 polymorphisms on BMD in the Irish population. Calcif Tissue Int 71:26–35. doi:10.1007/s00223-001-2081-z
Zhao H, Liu J, Ning G et al (2005) The influence of Lys3Asn polymorphism in the osteoprotegerin gene on bone mineral density in Chinese postmenopausal women. Osteoporos Int 16:1519–1524. doi:10.1007/s00198-005-1865-9
Garcia-Unzueta MT, Riancho JA, Zarrabeitia MT et al (2008) Association of the 163A/G and 1181G/C osteoprotegerin polymorphism with bone mineral density. Horm Metab Res = Horm und Stoffwechselforsch = Horm Metab 40:219–224. doi:10.1055/s-2008-1046793
Lee YH, Woo J-H, Choi SJ et al (2010) Associations between osteoprotegerin polymorphisms and bone mineral density: a meta-analysis. Mol Biol Rep 37:227–234. doi:10.1007/s11033-009-9637-9
Moffett SP, Oakley JI, Cauley JA et al (2008) Osteoprotegerin Lys3Asn polymorphism and the risk of fracture in older women. J Clin Endocrinol Metab 93:2002–2008. doi:10.1210/jc.2007-1019
Kim JG, Kim JH, Kim JY et al (2007) Association between osteoprotegerin (OPG), receptor activator of nuclear factor-kappaB (RANK), and RANK ligand (RANKL) gene polymorphisms and circulating OPG, soluble RANKL levels, and bone mineral density in Korean postmenopausal women. Menopause 14:913–918. doi:10.1097/gme.0b013e31802d976f
Ueland T, Bollerslev J, Wilson SG et al (2007) No associations between OPG gene polymorphisms or serum levels and measures of osteoporosis in elderly Australian women. Bone 40:175–181. doi:10.1016/j.bone.2006.06.022
Jorgensen HL, Kusk P, Madsen B et al (2004) Serum osteoprotegerin (OPG) and the A163G polymorphism in the OPG promoter region are related to peripheral measures of bone mass and fracture odds ratios. J Bone Miner Metab 22:132–138. doi:10.1007/s00774-003-0461-3
Lopes JB, Danilevicius CF, Takayama L et al (2011) Prevalence and risk factors of radiographic vertebral fracture in Brazilian community-dwelling elderly. Osteoporos Int 22:711–719. doi:10.1007/s00198-010-1258-6
Binkley N, Bilezikian JP, Kendler DL et al (2006) Official positions of the International Society for Clinical Densitometry and Executive Summary of the 2005 Position Development Conference. J Clin Densitom 9:4–14. doi:10.1016/j.jocd.2006.05.002
Domiciano DS, Figueiredo CP, Lopes JB et al (2013) Vertebral fracture assessment by dual X-ray absorptiometry: a valid tool to detect vertebral fractures in community-dwelling older adults in a population-based survey. Arthritis Care Res (Hoboken) 65:809–815. doi:10.1002/acr.21905
Kauppila LI, Polak JF, Cupples LA et al (1997) New indices to classify location, severity and progression of calcific lesions in the abdominal aorta: a 25-year follow-up study. Atherosclerosis 132:245–250
Bonfa AC, Seguro LPC, Caparbo V et al (2015) RANKL and OPG gene polymorphisms: associations with vertebral fractures and bone mineral density in premenopausal systemic lupus erythematosus. Osteoporos Int 26:1563–1571. doi:10.1007/s00198-015-3029-x
Piedra M, Garcia-Unzueta MT, Berja A et al (2011) Single nucleotide polymorphisms of the OPG/RANKL system genes in primary hyperparathyroidism and their relationship with bone mineral density. BMC Med Genet 12:168. doi:10.1186/1471-2350-12-168
Brandstrom H, Gerdhem P, Stiger F et al (2004) Single nucleotide polymorphisms in the human gene for osteoprotegerin are not related to bone mineral density or fracture in elderly women. Calcif Tissue Int 74:18–24. doi:10.1007/s00223-002-2136-9
Mencej-Bedrac S, Prezelj J, Marc J (2011) TNFRSF11B gene polymorphisms 1181G > C and 245T > G as well as haplotype CT influence bone mineral density in postmenopausal women. Maturitas 69:263–267. doi:10.1016/j.maturitas.2011.02.010
Wang Q, Chen Z, Huang Y et al (2013) The relationship between osteoprotegerin gene polymorphisms and bone mineral density in Chinese postmenopausal women. Int Immunopharmacol 17:404–407. doi:10.1016/j.intimp.2013.06.031
Boronova I, Bernasovska J, Macekova S et al (2015) TNFRSF11B gene polymorphisms, bone mineral density, and fractures in Slovak postmenopausal women. J Appl Genet 56:57–63. doi:10.1007/s13353-014-0247-4
Wang C, Zhang Z, Zhang H et al (2012) Susceptibility genes for osteoporotic fracture in postmenopausal Chinese women. J Bone Miner Res 27:2582–2591. doi:10.1002/jbmr.1711
Jurado S, Nogues X, Agueda L et al (2010) Polymorphisms and haplotypes across the osteoprotegerin gene associated with bone mineral density and osteoporotic fractures. Osteoporos Int 21:287–296. doi:10.1007/s00198-009-0956-4
Hsu Y-H, Niu T, Terwedow HA et al (2006) Variation in genes involved in the RANKL/RANK/OPG bone remodeling pathway are associated with bone mineral density at different skeletal sites in men. Hum Genet 118:568–577. doi:10.1007/s00439-005-0062-4
Guo L, Tang K, Quan Z et al (2014) Association between seven common OPG genetic polymorphisms and osteoporosis risk: a meta-analysis. DNA Cell Biol 33:29–39. doi:10.1089/dna.2013.2206
Soufi M, Schoppet M, Sattler AM et al (2004) Osteoprotegerin gene polymorphisms in men with coronary artery disease. J Clin Endocrinol Metab 89:3764–3768. doi:10.1210/jc.2003-032054
Strand M, Soderstrom I, Wiklund P-G et al (2007) Polymorphisms at the osteoprotegerin and interleukin-6 genes in relation to first-ever stroke. Cerebrovasc Dis 24:418–425. doi:10.1159/000108431
Straface G, Biscetti F, Pitocco D et al (2011) Assessment of the genetic effects of polymorphisms in the osteoprotegerin gene, TNFRSF11B, on serum osteoprotegerin levels and carotid plaque vulnerability. Stroke 42:3022–3028. doi:10.1161/STROKEAHA.111.619288
Speer MY, Giachelli CM (2004) Regulation of cardiovascular calcification. Cardiovasc Pathol 13:63–70. doi:10.1016/S1054-8807(03)00130-3
Findlay DM, Atkins GJ (2011) Relationship between serum RANKL and RANKL in bone. Osteoporos Int 22:2597–2602. doi:10.1007/s00198-011-1740-9
D’Amelio P, Isaia G, Isaia GC (2009) The osteoprotegerin/RANK/RANKL system: a bone key to vascular disease. J Endocrinol Invest 32:6–9
Acknowledgments
We thank Liliam Takayama for technical support and Jaqueline B. Lopes for her help in collected data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Funding
This work was supported by the following organizations and grants: Fundação de Amparo e Pesquisa do Estado de São Paulo (FAPESP no. 03/09313-0 and no. 09/11755-7), Conselho Nacional de Ciência e Tecnologia (CNPQ no. 472754/2013-0 to RMRP), Federico Foundation (to RMRP), and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES to CPF).
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 22 kb)
Rights and permissions
About this article

Cite this article
Pereira, R.M.R., Figueiredo, C.P., Cha, C.C. et al. Associations between OPG and RANKL polymorphisms, vertebral fractures, and abdominal aortic calcification in community-dwelling older subjects: the Sao Paulo Ageing & Health Study (SPAH). Osteoporos Int 27, 3319–3329 (2016). https://doi.org/10.1007/s00198-016-3664-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3664-x