
Abstract
Summary
To determine whether new national guidance on the specifications of a fracture liaison service are realistically deliverable, 1 year of data on the performance of such a service were audited. Audit targets were mostly met. This audit demonstrates that these standards are deliverable in a real world setting.
Introduction
UK service specifications for a fracture liaison service (FLS) have been produced (National Osteoporosis Society, NOS) to promote effective commissioning and delivery of the highest quality care to patients with fragility fractures. How deliverable these standards are has not as yet been methodically reported. Our FLS was modelled on the ten NOS standards; performance was audited after 1 year to determine whether these standards could be delivered and to describe the lessons learnt.
Methods
Performance was audited against the NOS FLS Service Standards, with management based on the Fracture Risk Assessment Tool (FRAX®), the four-item Falls Risk Assessment Tool (FRAT), National Institute for Health and Care Excellence (NICE) and the National Osteoporosis Guideline Groups (NOGG) guidance. Data were recorded prospectively on a database. The FLS commenced in May 2014, was fully operational in August 2014 and data were captured from 1 September 2014 to 1 September 2015.
Results
The FLS detected 1773 patients and standards were largely achieved. Most, 94 %, patients were seen within 6 weeks, 533 DXA requests were generated, 804 outpatient FRAT assessments were recorded (134 required falls intervention) and 773 patients had bone treatments started. On follow-up at 3 months, between 78–79 % were still taking medication.
Conclusions
Preliminary evaluation of a FLS implemented according to UK NOS standards demonstrates that the model is practical to apply to a large teaching hospital population. Collection and review of outcome and cost effectiveness data is required to determine the performance of this model in comparison with existing models.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fragility fractures are common and costly. Estimated to affect 1 in 2 women and 1 in 5 men over 50 [1], they cost the UK NHS approximately UK £1.9 billion a year [2]. Associated morbidity and mortality are high including loss of independence [3]. Provision of a fracture liaison service (FLS) reduces re-fracture risk [4] cost effectively, estimated by some to be a risk reduction of at least 30 % [5–7] with possible additional reductions in mortality [6]. Most outcome data however are based on FLS models incorporating identification of fragility fractures with or without bone health assessment and treatment with no or little provision of falls prevention [5–8]. A high quality fully integrated FLS is therefore considered the gold standard for fragility fracture identification and management.
International benchmarking exercises and national audit programmes have revealed the wide spectrum of services currently offered despite the attempts of many organisations to produce standards of care [9, 10]. The gold standard model of an FLS has yet to be determined which accounts, in part for the wide variation in provision seen. To address this, the National Osteoporosis Society (NOS) published a set of 10 quality standards in 2015 identifying the cornerstone elements of what an ideal and quality-assured FLS should deliver in principle and in practise [2]. By using a ‘5IQ’ approach (see Table 1), the standards aim to guide services towards the most clinically and cost effective model of delivery addressing all aspects of care including falls prevention and follow-up [2]. Demonstration of operational delivery of these standards has not as yet been tested within a service implemented around these 10 quality standards. Data on the resource burden of such a service are also lacking. To be responsible in designing services and to provide commissioners with realistic cost and meaningful key performance indicators (KPIs), an evaluation of a 5IQ FLS model is required.
A FLS model based on the NOS 5IQ approach was evaluated after a year; an audit was performed against the standards below (Table 1) [2]. The hypothesis being tested was that a FLS based on the NOS standards is achievable and practical to run and to provide an estimate of resources required.
Methods
University Hospital Birmingham FLS
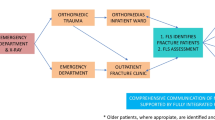
A FLS was commissioned and established at the University Hospitals Birmingham (UHB) and started to identify secondary fracture prevention outpatients in July and inpatients in August 2014. The FLS was based on the NOS standards (Table 1) with falls assessment only occurring for outpatients, an existing falls service for inpatients was already in place, and with a primary focus on non-vertebral fragility fractures [2]. Systematic identification and management of vertebral fractures at UHB is being addressed as a second phase service development, integrating pre-existing spinal services. However, ad hoc referrals into the FLS for spinal fragility fractures were managed in line with non-vertebral fracture pathways. Those ≥75 years old admitted with a neck of femur fracture were, and continued to be, managed by a pre-existing service; both teams however interact closely and the FLS reviews patients with the orthogeriatric team.
Patients accessing the service are aged ≥50 with an incident fragility fracture. Orthopaedic, general and elderly care inpatients are identified from inpatient and trauma lists reviewed daily. Orthopaedic and A&E outpatients are identified from hospital systems including databases and FLS nurses attend fracture clinics. All new inpatients falls must be reported and are thereby picked up by the FLS. Orange referral cards to the FLS, posters and business cards are left in appropriate departments.
Data are collected prospectively on a Microsoft Office Excel® spreadsheet database (Microsoft ®, Redmond, Washington, USA) held by the FLS team as part of internal service evaluation and audit. Limited information is also collected about all those patients seen by the orthogeriatric service (≥75 years old with neck of femur fracture) to ensure no duplication of effort. Clinical judgement is aided by guidance and risk calculators including standardised tools such as the Fracture Risk Assessment Tool (FRAX®) [11] and the four-item Falls Risk Assessment Tool (FRAT), on outpatients only [12]. Management is based on the National Institute for Health and Care Excellence (NICE) and the National Osteoporosis Guideline Groups (NOGG) guidance [13–17]. All patients assessed by the FLS found to have a fragility fracture and be appropriate for assessment and treatment are sent a fracture discharge letter which summarises the actions taken and further actions required for all three parties (patient, GP and FLS). Telephone follow-up calls are made to those started on treatment, initially 3, 6 and 12 months, protocol then changed to 4 and 12 months. If no one answers the phone on the third occasion then it is documented as a failure. Patients are also asked to fill in a 14-part questionnaire to assess satisfaction and experience of the service.
Data were analysed from a database gather performed on 23 September 2015 in regards to all fractures occurring from 1 September 2014 to 31 August 2015. Data analysis was performed using Microsoft Office Excel® (Microsoft ®, Redmond, Washington, USA). The radiology department provided the number of patients who did not attend (DNA) from the FLS for a DXA over the audit period. The number of fragility fractures occurring during a period may be estimated by multiplying the number of hip fractures by 5 and this method was applied to give a crude denominator [2]. This denominator however includes vertebral fractures that the phase one FLS was not commissioned to deliver at UHB. An alternative denominator was sought from the Trust’s information department who collected the total number of patient aged 50 years and over who presented during the year to the hospital coded as having a fracture, excluding vertebral, including those admitted and those discharged from A&E. This total will include trauma patients and neurosurgical patients transferred for care.
Results
The demographic details of the patient cohort are presented below (Table 2). Most patients had one fracture (87 % of inpatients, 96 % of outpatients, 99 % of ≥75 year olds); the commonest fracture type was distal radius followed by proximal humerus, femur, tibia and/or fibula, ankle, pelvis, ulnar and radius, clavicle, patella, foot or hand, vertebral, shoulder, ribs and mandible. The FLS reviewed 148 patients with hip fractures and a further 426 were seen by the existing elderly care team. The total number of fragility fractures expected (estimated by multiplying the total number of hip fractures by 5 [2]) suggests only 62 % of all fragility fractures were identified. The trust saw 3655 patients with a fracture during the same period in total, which suggests the FLS saw 49 % of all those aged 50 and over presenting to the hospital with a fracture. Workload increased steadily with four patients seen per working day in September 2014 to seven by the end of July 2015.
Results are summarised and related to NOS standards in Table 1 and detailed more fully in Table 2. From April 2015, when date of fracture was recorded, 212 inpatients and 425 outpatients were seen. Additional results include that all patients with FRAX® scores calculated also had NOGG risk documented; more of the outpatients (39 %) were low risk compared with inpatients (21 %) with only 22 % of outpatient high risk (35 % of inpatients). The bone density results are demonstrated below (Fig. 1a, b). According to the radiology department, 527 referrals were made by the FLS for the year, six less than recorded in the database. Extra DXA slots having been made available in March; the DNA rates fell between each quartile of the year.

a Frequency (percentage) bar chart to show bone density results of DXA based on T-score at the hip or lumbar spine on scans done prior to or after presenting with fragility fracture. b Chart to show bone density of those with DXA based on type of fracture as a percentage
There were no great differences in the percentage of patients started on specific therapies between inpatients and outpatients however slightly higher proportions of the inpatients were given more than just advice or vitamin D and calcium. In total, 4 patients were started on teriparatide, 41 on IV bisphosphonates and 10 on denosumab. Medications were changed in a large number of patients (Fig. 2a), mostly introduction of therapy however 14 patients had admission bisphosphonates stopped and 12 had vitamin D and/or calcium supplements stopped.

a Chart to show number of patients on treatment divided by supplements taken/recommended or not from 3-month follow-up cohort only (supplement being either calcium, vitamin D or both). Percentage of those on each type of active bone therapy on admission and percentage of each type of therapy recommended is quoted as data labels on the columns. b Chart to show frequency of reasons why medication stopped (percentage) in those in whom follow-up was successful at 3 and 6 months (n = 61)
Initially follow-up was set for 3 months, 6 months then 1 year, until end of June 2015 when FLS protocol changed from 4 to 12 months from 1 July 2015. Very few patients were due for their annual follow-up, 4 and 6 month follow-up therefore data for 3 months follow-up only is presented (Table 2). Follow-up was unsuccessful in a third of cases due to failure of contact (patient not answering telephone) and the rest have nothing documented. Of those with nothing documented, one third had been seen close to 3 months ago, and another 18 % were noted as lacking capacity to fill in the patient satisfaction questionnaire. Only 79 % of patients followed up at 3 months were taking prescribed bone medications, 53 % were meant to be on bisphosphonates and 93 % on vitamin D. Of the patients in whom follow-up was successful, the reasons why they were not on recommended therapy included the following: new co-morbidity, GP altered, stopped or did not prescribe, currently admitted, side effects, patient declined or forgot to go and get a prescription (Fig. 2b).
Standards 8 and 10 (Table 1) have been largely addressed by this study as well as recent external review. Patient satisfaction questionnaires were given to 1011 patients (336 lacked capacity), 21 % completed the first question. Most patients (77 %) stated that they were ‘extremely likely’ to ‘recommend our service to friends and family if they needed similar care or treatment’ and 18 % were ‘likely’ to. Reasons included (in descending order): staff approach, satisfied with service and treatment, satisfied with discussion and explanation, satisfied with purpose of intervention and promptly seen. The importance of the staff was highlighted, who were frequently described as ‘helpful, caring, polite and kind’ and the ‘efficient’ service and treatment generally with 60 % rating the FLS as ‘excellent’ (35 % as ‘very good’).
FLS nurses have attended relevant training including a master class in Glasgow, the annual NOS conference, regional meetings and online courses, such as the FLS competency course, and maintain a portfolio documenting CPD (standard 9, Table 1).
Discussion
This is believed to be the first published evaluation of an FLS based upon the NOS 5IQ standards [2]. The hypothesis, that a FLS based on the NOS standards is achievable and practical to run, has been confirmed. Main findings include the large workload that can be expected, 1773 patients/year despite a limited service with only a crude estimated 62 % detection rate for all fragility fractures and 49 % of total fracture work in this age group. Of the total fracture work, many will be inappropriate for FLS review as will include traumatic fractures such as polytrauma to finger injuries. Though a less than 100 % detection rate was expected, particularly as only non-vertebral fractures were sought, and the denominator for the rule of five statistics is only an estimate of uncertain accuracy, there is likely unmet need yet to be addressed. Patients were seen in a timely fashion, 100 % of inpatients and 99 % of outpatients seen within 3 months with 94 % seen within 6 weeks, and patient satisfaction was high. New DXA requests were generated for 177 inpatients and 356 outpatients and 804 outpatient FRAT assessments were recorded. Treatments were started in 303 inpatients and 470 outpatients, including 4 patients on teriparatide, 41 on IV bisphosphonates and 10 on denosumab however treatments or interventions performed on those referred to metabolic bone clinic are not recorded in the database. The extra work made for metabolic bone clinic is not collected by the FLS and therefore difficult to estimate. Falls interventions were required by 15 % (134 patients). In those in whom follow-up succeeded between 78–85 % were still taking medication, the commonest reason for not being on the recommended treatment was that the GP had not prescribed it. Telecare has been shown to cause a reduction by 15 % in A&E admissions however only 4 % of outpatients assessed both required and accepted the recommendation for a personal alarm [18]. Though further service refinements are required and the quantity of work generated should be appreciated, the NOS guidance is achievable in a large tertiary centre.
It is reported that approximately 70 % of those presenting with fractures have a bone density that is not osteoporotic [2] which matches the numbers seen in the inpatients with indeed even more of the outpatients having bone density >−2.5. In the experience of the West Glasgow FLS, only 46 % of the patients seen and having a DXA had osteoporosis indicating that even in a selected population not all will require bone treatments [4]. The DXA DNA rate calculated from the DXA department data (5 %) is less than that calculated from the database despite very similar numbers of referrals recorded by each. This may be accounted for by inaccuracies in the database. Prompt assessment occurred in the majority of patients except in those transferred from other hospitals, or with complex injuries not initially triggering referral.
Identification of high-risk groups is estimated to prevent 25 % of hip fractures [19, 20], primary prevention would require 5–6 times more patients to be identified to have the same impact as secondary prevention [21, 22] and half of the patients presenting with a hip fracture have had a previous fragility fracture [23]. Effective application of a FLS model of various types is cost effective, improves care and decreases fractures [4–8, 15, 24, 25]. Every year the National Hip Fracture Database (NHFD), as part of the Falls and Fragility Fracture Audit Programme (FFFAP), has demonstrated improvements in care and outcomes demonstrating the effectiveness of clear guidelines and the audit process [10]. The significance of these results is that the gold standard FLS model has yet to be widely agreed. Best practise guidelines abound and include the National Institute for Health and Care Excellence (NICE) clinical guideline (CG124), 12 quality standards (QS16) [13, 15], the National Service Framework (NSF) for older people (standard 6) [26], NICE [14, 16, 27] and SIGN [28]. These have been incorporated into the NOS standards, with the hope that this optimises benefit, the delivery of which and impact of it is unproven [2]. These data demonstrate successful delivery however the impact will need to be assessed by looking for a reduction in repeat falls, fractures and hospital attendances.
There were several limitations in the audit firstly the database was examined on 23 September 2015 therefore patients seen at the end of the audit period were still awaiting results and scans therefore not all data were available for review. Data are entered manually therefore errors were present in the spreadsheet and data were incomplete. Improvements have been introduced to improve data collection, reduce ambiguity and an administrator has been hired to assist. Complexities and changing patient circumstances are also difficult to code. Co-morbidities may only affect part of the services offered further confusing outcomes, and, as more fields are added, the complexity of the database may compound input errors. Automatic data population and further refinement of data entry (standard operating procedures, binary coding etc.) would improve the quality of the database. The rule of fives that resulted in a 62 % detection rate is considered inaccurate as the team felt that very few patients are missed and the appropriateness of this estimate should be questioned. Regional varieties in population demographics and alternative hospital services available may compound errors. For example, in the West Midlands, there are multiple hospitals serving overlapping areas and UHB is the regional trauma centre, which may influence case mix. An independent record of every single fragility fracture, even if patient refuses review or it is deemed inappropriate, would be useful to obtain a more accurate estimate of total workload. Despite these limitations the large number of patients seen hopefully minimises the effect of data entry errors.
Subjectively, having introduced and audited the NOS standards, it was felt that they were appropriate and improved patient care. No aspect was felt to be a poor fit or produced processes that did not add value. It was apparent however, that large quantities of activity were not captured in the audit, particularly in regards to management of frail community-dwelling adults. This included many aspects of fall prevention, social service and safe-guarding referrals as well as real time interventions created by a holistic approach to patient care. The benefit of taking responsibility for this holistic approach to fracture prevention was clear to the team but much of the work is not immediately captured in the current audit standards. We would support the continued inclusion of falls prevention in the NOS standards as it promotes this model of care which, we hope, will result in real improvements to patient quality of life, fracture prevention and benefits to the wider local health and social care economy. There are early indications of benefit as Birmingham has recently seen a reduction in the rate of female hip fractures (Public Health Data).
Despite the methodological limitations, this preliminary evaluation of an FLS, recently implemented according to NOS FLS standards, demonstrates that the model is practical to apply to a large teaching hospital population [2]. The workload will be large however but a step wise introduction succeeded in producing a FLS providing a service meeting its specifications. Satisfaction with the FLS, both patient and professionals, is high and can provide gold standard care to the desired population. The long-term goals of the FLS include reduced rates of the following: people falling with serious injury (A&E attendance, hospital admission), fragility fractures and ambulance transfers to hospitals for falls. These data need to be reviewed in the future to determine whether the service affects these outcomes.
References
van Staa TP, Dennison EM, Leufkens HG, Cooper C (2001) Epidemiology of fractures in England and Wales. Bone 29(6):517–522
National Osteoporosis Society (2015) Effective secondary prevention of fragility fractures: clinical standards for fracture liaison services. https://www.nos.org.uk/document.doc?id=1941. Accessed 26th September 2015
National Osteopororsis Society (2014) Life with osteoporosis: the untold story. National Osteoporosis Society, Bath
McLellan AR, Wolowacz SE, Zimovetz EA, Beard SM, Lock S, McCrink L, Adekunle F, Roberts D (2011) Fracture liaison services for the evaluation and management of patients with osteoporotic fracture: a cost-effectiveness evaluation based on data collected over 8 years of service provision. Osteoporos Int 22(7):2083–2098. doi:10.1007/s00198-011-1534-0
Nakayama A, Major G, Holliday E, Attia J, Bogduk N (2015) Evidence of effectiveness of a fracture liaison service to reduce the re-fracture rate. Osteoporos Int. doi:10.1007/s00198-015-3443-0
Huntjens KM, van Geel TA, van den Bergh JP, van Helden S, Willems P, Winkens B, Eisman JA, Geusens PP, Brink PR (2014) Fracture liaison service: impact on subsequent nonvertebral fracture incidence and mortality. J Bone Joint Surg Am 96(4):e29. doi:10.2106/JBJS.L.00223
Dell R (2011) Fracture prevention in Kaiser Permanente Southern California. Osteoporos Int 22(Suppl 3):457–460. doi:10.1007/s00198-011-1712-0
Yong JH, Masucci L, Hoch JS, Sujic R, Beaton D (2015) Cost-effectiveness of a fracture liaison service-a real-world evaluation after 6 years of service provision. Osteoporos Int 27(1):231–240. doi:10.1007/s00198-015-3280-1
IOF Fracture Working Group; EXCO, Javaid MK, Kyer C, Mitchell PJ, Chana J, Moss C, Edwards MH, McLellan AR, Stenmark J, Pierroz DD, Schneider MC, Kanis JA, Akesson K, Cooper C (2015) Effective secondary fracture prevention: implementation of a global benchmarking of clinical quality using the IOF Capture the Fracture® Best Practice Framework tool. Osteoporos Int 26(11):2573–2578. doi:10.1007/s00198-015-3192-0
Royal College of Physicians. Falls and Fragility Audit Programme, National Hip Fracture Database (NHFD) annual report 2015. Healthcare Quality Improvement Partnership 2015 http://www.nhfd.co.uk/20/hipfractureR.nsf/vwcontent/2014reportPDFs/$file/NHFD2014SummaryReport.pdf?OpenElement. Accessed 21 September 2015
FRAX®. WHO Fracture Risk Assessment Tool. https://www.shef.ac.uk/FRAX/. Accessed 30 September 2015
Stapleton C, Hough P, Bull K, Hill K, Greenwood K, Oldmeadow L (2009) A 4-item falls-risk screening tool for sub-acute and residential care: the first step in falls prevention. Australas J Ageing 28(3):139–143. doi:10.1111/j.1741-6612.2009.00375.x
National Institute for Health and Care Excellence (2011) The management of hip fracture in adults. Clinical guideline (CG124). London: NICE. www.nice.org.uk/guidance/cg124. Accessed 29 September 2015
National Institute for Health and Care Excellence (2013) Falls: assessment and prevention of falls in older people. NICE guidelines [CG161]. London: NICE. https://www.nice.org.uk/Guidance/CG161. Accessed 29 September 2015
National Institute for Health and Care Excellence (2012) Hip fracture quality standard (QS16). NICE, London, www.nice.org.uk/guidance/qs16. Accessed 29 September 2015
National Institute for Health and Clinical Excellence (2008) Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended): NICE technology appraisal guidance 161 [TA161]. NICE, London, https://www.nice.org.uk/Guidance/TA161. Accessed 29 September 2015
National Osteoporosis Guideline Group (NOGG) http://www.shef.ac.uk/NOGG/index.html. Accessed 30 September 2015
Department of Health (2011) Whole system demonstrator programme; headline findings—December 2011. Gateway Ref: 16972. Available https://www.gov.uk/government/publications/whole-system-demonstrator-programme-headline-findings-december-2011. Accessed 17 November 2015
Cooper C, Mitchell P, Kanis JA (2011) Breaking the fragility fracture cycle. Osteoporos Int 22(7):2049–2050. doi:10.1007/s00198-011-1643-9
Dell R, Greene D, Schelkun SR, Williams K (2008) Osteoporosis disease management: the role of the orthopaedic surgeon. J Bone Joint Surg Am 90:188–194. doi:10.2106/JBJS.H.00628
IOF CSA Fracture Working Group, Marsh D, Åkesson K, Beaton DE, Bogoch ER, Boonen S, Brandi ML, McLellan AR, Mitchell PJ, Sale JE, Wahl DA (2011) Coordinator-based systems for secondary prevention in fragility fracture patients. Osteoporos Int 22(7):2051–2065. doi:10.1007/s00198-011-1642-x
Mitchell PJ (2013) Fracture liaison services in the United Kingdom. Curr Osteoporos Rep 11(4):377–384. doi:10.1007/s11914-013-0166-z
Edwards BJ, Bunta AD, Simonelli C, Bolander M, Fitzpatrick LA (2007) Prior fractures are common in patients with subsequent hip fractures. Clin Orthop Relat Res 461:226–230
Skelton D, Neil F (2009) NHS Greater Glasgow and Clyde Strategy for Osteoporosis and Falls Prevention 2006-2010: An evaluation 2007-2009. http://library.nhsggc.org.uk/mediaAssets/OFPS/NHSGGC%20Strategy%20for%20Osteoporosis%20and%20Falls%20Prevention%202006-2010_An%20Evaluation_Skelton%20and%20Neil%202009.pdf. Accessed 29 September 2015
Department of Health (2009) Fracture prevention services: an economic evaluation. DH, London
Department of Health (2001) National Service Framework for Older People. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/198033/National_Service_Framework_for_Older_People.pdf. Accessed 29 September 2015
National Institute for Health and Clinical Excellence (2010) Denosumab for the prevention of osteoporotic fractures in postmenopausal women. NICE technology appraisal guidance 204. London: NICE. http://www.nice.org.uk/guidance/ta204/resources/guidance-denosumab-for-the-prevention-of-osteoporotic-fractures-in-postmenopausal-women-pdf. Accessed 29 September 2015
Scottish Intercollegiate Guidelines Network (SIGN) (2015) Management of osteoporosis and the prevention of fragility fractures. (SIGN publication no. 142). Edinburgh: SIGN; 2015. http://www.sign.ac.uk. Accessed 29 September 2015
Acknowledgments
The authors would like to thank the members of the FLS for their hard work, excellent data keeping and assistance with any enquiries regarding the audit. The authors would also like to thank Chris Boivin and the DXA department for all their hard work in both providing the service and data for the audit.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical standards in regards to audit and data protection were adhered to.
Conflicts of interest
NG chaired the NOS Service Standards document and is a Trustee of the NOS and Chair of the Clinical and Scientific Committee of the NOS.
Rights and permissions
About this article

Cite this article
Shipman, K.E., Stammers, J., Doyle, A. et al. Delivering a quality-assured fracture liaison service in a UK teaching hospital—is it achievable?. Osteoporos Int 27, 3049–3056 (2016). https://doi.org/10.1007/s00198-016-3639-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3639-y