
Abstract
Summary
Under current guidelines, based on prior fracture probability thresholds, inequalities in access to therapy arise especially at older ages (≥70 years) depending on the presence or absence of a prior fracture. An alternative threshold (a fixed threshold from the age of 70 years) reduces this disparity, increases treatment access and decreases the need for bone densitometry.
Introduction
Several international guidelines set age-specific intervention thresholds at the 10-year probability of fracture equivalent to a woman of average BMI with a prior fracture. At older ages (≥70 years), women with prior fracture selected for treatment are at lower average absolute risk than those selected for treatment in the absence of prior fracture, prompting consideration of alternative thresholds in this age group.
Methods
Using a simulated population of 50,633 women aged 50–90 years in the UK, with a distribution of risk factors similar to that in the European FRAX derivation cohorts and a UK-matched age distribution, the current NOGG intervention and assessment thresholds were compared to one where the thresholds remained constant from 70 years upwards.
Results
Under current thresholds, 45.1 % of women aged ≥70 years would be eligible for therapy, comprising 37.5 % with prior fracture, 2.2 % with high risk but no prior fracture and 5.4 % selected for treatment after bone mineral density (BMD) measurement. Mean hip fracture probability was 11.3, 23.3 and 17.6 %, respectively, in these groups. Under the alternative thresholds, the overall proportion of women treated increased from 45.1 to 52.9 %, with 8.4 % at high risk but no prior fracture and 7.0 % selected for treatment after BMD measurement. In the latter group, the mean probability of hip fracture was identical to that observed in women with prior fracture (11.3 %). The alternative threshold also reduced the need for BMD measurement, particularly at older ages (>80 years).
Conclusions
The alternative thresholds equilibrate fracture risk, particularly hip fracture risk, in those with or without prior fracture selected for treatment and reduce BMD usage at older ages.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The development of fracture risk assessment tools has enabled a step change in the management of osteoporosis as patients can now be selected for therapy on the basis of absolute fracture risk rather than bone mineral density (BMD) T-score alone. Of the several assessment tools available, the most widely used is FRAX® which is recommended in several national and international guidelines [1–7].
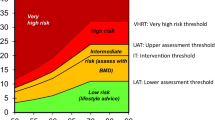
The clinical use of any risk assessment requires the establishment of assessment and/or intervention thresholds that guide the clinician to undertake further assessment or initiate therapy. In the UK, the National Institute of Health and Care Excellence (NICE) recommends the use of two risk assessment tools, QFracture or FRAX [7–9]. The latter is the most widely validated tool and has the advantage over QFracture of incorporating measurements of femoral neck BMD, a well-established predictor of fracture risk that may also influence skeletal responsiveness to therapy. The launch of FRAX in April 2008 was shortly followed by the National Osteoporosis Guideline Group (NOGG) thresholds, with an easy-to-use link via the FRAX UK calculator website. Briefly, the NOGG guidance “translated” the preceding Royal College of Physicians (RCP) guideline which indicated that women with a prior fragility fracture may be considered for intervention without the necessity for a BMD test for the purpose of making the treatment decision [3, 10]. The NOGG intervention threshold therefore reflects the age-specific fracture probability equivalent to a woman of average BMI (24 kg/m2) with a prior fragility fracture, no additional risk factors and without knowledge of BMD (Fig. 1). This FRAX-based approach is similar to that recently adopted by the International Osteoporosis Foundation (IOF), European Society for Clinical and Economic aspects of Osteoporosis and Osteoarthritis (ESCEO) and European Calcified Tissue Society for postmenopausal osteoporosis and/or glucocorticoid-induced osteoporosis in Europe [1, 6] and several other country-specific guidelines in addition to the UK [2, 5, 11, 12].

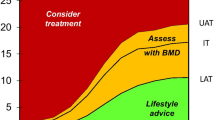
Graphs of intervention and assessment thresholds showing the current NOGG thresholds in the UK (a) and the alternative thresholds (b). The dotted line represents the intervention threshold while the assessment thresholds enclose the amber area (see text for details)
In addition to intervention thresholds, assessment thresholds for BMD testing were devised to represent threshold probabilities below which neither treatment nor a BMD test should be considered (lower assessment threshold; i.e. a patient with no risk factors) and a threshold probability above which treatment may be recommended without the need for BMD (upper assessment threshold; i.e. a 1.2-fold increase on the intervention threshold) (Fig. 1). The latter threshold was chosen to minimise the probability that a patient characterised to be at high risk on the basis of clinical risk factors alone would be reclassified as low risk with additional information on BMD [13].
Recently, a published comparison of the RCP and NOGG guidance in postmenopausal women demonstrated that both approaches identified patients at similar risk at younger ages, regardless of fracture status, but the NOGG thresholds were somewhat more conservative at older ages in women without prior fracture [14]. Thus, NOGG identified fewer older women without fracture as eligible for treatment, and those identified were at higher risk than those identified by prior fracture [14]. The lower risk in older women with fracture reflects the approach, endorsed by many agencies including NOGG and NICE, that such women can be treated without recourse to FRAX or BMD, so that some are treated at fracture probabilities below the NOGG-recommended intervention threshold [3, 15]. For example, the NOGG intervention threshold assumes an average BMI, but input of actual BMI and other risk factors in the calculation of an individual’s actual probability might yield a value which is somewhat lower than the threshold, but treatment would still be indicated in the presence of fracture. The very high threshold at older ages for women without fracture might be seen to disadvantage more elderly individuals.
A confusing situation can also arise where clinicians choose to measure BMD in older women with fracture, as many of these will come to lie below the intervention threshold after the inclusion of BMD in the FRAX calculation. The impact of acquiring a BMD measurement and recalculating the fracture probability on the decision to treat in older women with fracture has not been formally assessed.
In this study, we have undertaken an evaluation of the current NOGG assessment and intervention thresholds and examined the impact of a potential change to the thresholds at older ages.
Methods
The first step involved the production of a simulated population of women aged 50–90 years based on the UK age-distribution and European age-specific prevalence of risk factors. The multivariate distribution of the clinical risk factors by age was estimated by determination of a set of conditional distributions using cohorts of European women used in the development of FRAX. Except for BMD and BMI, the variables are zero-one (at a given age). The probability that a zero-one variable, representing the dichotomous present/absent clinical risk factors in FRAX, assumes the value one was estimated by multivariable logistic regression analysis including other variables that were significantly correlated to the current zero-one variable. The product of such conditional distributions yields the multivariate distribution given age. Normal two-dimensional variables were simulated, so they perfectly fitted a special matrix of covariance, and the dichotomous risk variables were simulated according to the results of the logistic regression analyses. A simulated population of 50,633 women aged 50–90 years in the UK was generated. Simulations of greater numbers of women (up to 100,000) indicated that this number provided stability of the estimates of the risk factor distribution.
Under the NOGG strategy, the risk of fracture is assessed on clinical risk factors alone which in turn provides guidance whether a BMD measurement or treatment is indicated, an approach that has been endorsed by NICE [7]. The initial decision is based on the presence of a prior fragility fracture with treatment to be considered in such patients without necessarily undertaking a BMD measurement, though the latter may still be useful in younger postmenopausal women. For the purpose of the main analysis, we have assumed that treatment would be considered in all women with prior fracture.
In the absence of fracture, the decision is based on the 10-year probability of major osteoporotic fracture with some individuals deemed at high risk (treatment without BMD), some at or near the intervention threshold (BMD indicated to finalise risk evaluation and stratification) and some at low risk (lifestyle advice, reassurance and re-evaluation in the future). Once BMD is entered into the calculation, the decision to treat or not is based on a comparison to age-specific thresholds for both major osteoporotic and hip fracture probability; a probability at or above either threshold indicates therapy. The current NOGG strategy was examined to see what proportion of the female population between the ages of 50 and 90 years would qualify for BMD measurement and/or treatment, with a particular emphasis on women aged 70 years and over. The thresholds for assessment and treatment were estimated for each age (in years) (Fig. 1a).
An alternative strategy was also examined. Considerations in choosing a new intervention threshold included the aim of capturing the vast majority of women aged 75 years and older with a prior fracture. The initiation of treatment without further assessment, for example BMD, in such women has been espoused in NICE guidance [15]. The fifth percentile of major osteoporotic fracture probability in UK women aged 75 years and older with prior fracture was 19.2 %. This value approximates to the mean value of major osteoporotic fracture probability at the age of 70 (20.3 %) so that for ease of translation, it was decided that the intervention and assessment thresholds would remain identical to those in the current NOGG strategy up until the age of 70 years but thereafter would remain constant at older ages (i.e. the thresholds at 70 years were applied to older ages) (Fig. 1b). The threshold of 20.3 % still captures approximately 92 % of the fracture cases over 75 years. The upper and lower BMD assessment thresholds were 11.08 and 24.41 %, respectively. The alternative threshold for intervention based on hip fracture probability, defined as the probability in women with BMI 24 kg/m2 and a prior fracture, was established to be 5.4 % at 70 years and was applied to women aged 70 years and above.
A formal statistical analysis was not conducted as the study represents a simple comparison of the two thresholds using an identical ‘population’. Differences in advice about whether or not to treat older women with fracture before and after BMD measurements were also explored for both thresholds.
Results
The characteristics of the simulated representative sample of women aged 50–90 years in the UK are shown in Table 1. As expected, there was a decline in the size of the age groups with increasing age (NB the 85–90 age group comprises 6 rather 5 years). Prior fracture was the most common risk factor and increased in prevalence from 22 % at 50–54 years to 43 % at 85–90 years. Other risk factors that increased in prevalence with increasing age included parental hip fracture and glucocorticoid use. The prevalence of low BMI (≤19 kg/m2) and rheumatoid arthritis was relatively stable across the ages, while current smoking, alcohol intake (≥3 units per day) and causes of secondary osteoporosis showed a decline with age, particularly marked for smoking.
Current and alternative NOGG thresholds
Given that prior fracture is an indication for therapy in both strategies, the proportion of women recommended for therapy for this reason was identical in both scenarios and rose with age. Overall, the current NOGG thresholds advocated therapy in 37.9 % of women between 50 and 90 years, comprising 30.1 % with prior fracture, 1.4 % with high risk in the absence of fracture and 6.4 % with high risk following BMD assessment (Table 2). The proportion indicated for treatment increased from 31.2 % at age 50–54 years to 49.5 % at 85–90 years (Table 2). As demonstrated previously, there was a discordance in the risk of fracture in the three groups identified for therapy under the current thresholds, and this discordance was most marked in women aged 70 years and over (Table 2, Fig. 2). For example, in women without fracture, the mean 10-year probability of hip fracture was 23.3 and 17.6 % in those deemed to be at high risk or selected for treatment after BMD compared with a mean of only 11.3 % in women with prior fracture (Table 2, Fig. 2). The corresponding mean probabilities of major osteoporotic fracture were 33.0 and 28.7 % compared with 25.5 % (Table 2).

Mean probability of hip fracture in patients identified for consideration of treatment under the current thresholds (open bars) and the alternative thresholds (solid bars). High risk captures those falling into the red areas in Fig. 1a and b, while those selected after BMD capture those within the amber zones that come to lay above the intervention threshold after BMD assessment
The alternative thresholds only slightly increased the total proportion of women aged 50–90 years selected for treatment (37.9 to 40.8 %) despite a more marked impact on treatment and BMD assessment at older ages (Table 2). For example, the proportion of 70–90-year-old women recommended for therapy increased from 45.1 to 52.9 % (Table 2, Fig. 3a) with a doubling of the proportion treated in the absence of a prior fracture (15.4 compared to 7.7 % under current thresholds) (Table 2). The latter was predominantly mediated by an increase in the number of women identified at high risk without the need for BMD (8.4 from 2.2 %) with a small increase in the proportion treated after BMD (7 from 5.4 %) (Table 2). It is important to note that the small increase in those aged 70 years and over treated following BMD was achieved despite a decrease in the proportion referred for BMD measurements (15.7 vs 19.7 %) (Fig. 3b). The impact on the proportion identified for treatment and the reduction in BMD requirement was more marked in the older age groups (Table 2, Fig. 3a, b). Importantly, in women without prior fracture who were identified for treatment, the alternative thresholds were associated with a reduction in average probability of major osteoporotic and hip fracture. These values were similar to those observed in women with a prior fracture (Table 2, Fig. 2). Indeed, the mean probability of hip fracture was identical in those identified by prior fracture and those identified after BMD (Table 2, Fig. 2). The mean probability of major osteoporotic fracture was slightly lower in those without prior fracture compared with those with fracture (22.1 vs 25.5 %). It is important to note, however, that all of the women without prior fracture will have a probability of at least 20.3 %, whereas this is not true for all the women with prior fracture.

Proportion of the population of women within each age band that would be recommended for consideration of treatment (a) or bone mineral density measurement (b) under current thresholds (open bars) and the alternative thresholds (solid bars)
Impact of current and alternative thresholds in older women with prior fracture (prior fracture handled as a risk factor)
This analysis explored the impact of the preference of many clinicians to still undertake BMD in older women with fracture, prior to deciding about therapy, i.e. prior fracture is not regarded as an absolute indication for therapy but rather as a risk factor. The impact of the current NOGG and alternative thresholds in women aged 70–90 years with prior fracture is shown in Table 3 and Fig. 4.

Proportion of the women with prior fracture selected for treatment if fracture is considered as a risk factor rather than a direct indication for therapy (open bars—current thresholds; solid bars—alternative thresholds)
Using current thresholds, a significant proportion (26.7 %) of women aged 70–90 years with fracture had FRAX major osteoporotic fracture probabilities above the upper assessment threshold where treatment is indicated without the need for BMD (Table 3). It is important to note that a small proportion of women with prior fracture actually had FRAX major osteoporotic fracture probabilities that lay below the lower threshold for BMD assessment. Overall, this occurs in 1.7 % of older women with prior fracture, ranging from 0.6 % at 70–74 years to 2.6 % at 85–90 years. The majority of older women with fracture (71.6 %) would be referred for a BMD measurement, and most would subsequently not be treated following entry of the BMD value into FRAX and NOGG; for example, of the 71.6 % referred for a scan, only a quarter (18.3/71.6, 25.6 %) would have treatment indicated when the FRAX probability is recalculated including the BMD result (Table 3). Overall, only 45 % of women aged 70 and above with prior fracture would have treatment indicated (Table 3, Fig. 4); this falls slightly further to 43.4 % in women aged 75 years and older if clinicians did not follow NOGG advice to treat all such women and instead processed them through BMD scanning and reapplication of the NOGG algorithm.
Compared to the current NOGG thresholds, the proportion of women aged 70 years and over with prior fracture treated using the alternative thresholds increased from 45.0 (Table 3) to 79.1 % (Table 3). The proportion treated without BMD increased from 26.7 to 64.7 %, with treatment recommended without BMD in 94.6 % of women with prior fracture at 85–90 years (Table 3). Only a very small proportion of women with prior fracture have FRAX major osteoporotic fracture probabilities that lie below the lower threshold for BMD assessment, and this is stable across the age groups (0.1–0.3 %). As more women with prior fracture are directly indicated for treatment at older ages, the total proportion referred for BMD also declined markedly from 71.6 to 35.1 %; only 16.9 and 5.3 % of 80–84 and 85–90-year olds, respectively, would be referred for scans. Despite the 51 % reduction in scanning requirement, the proportion identified for treatment after scans was similar (24.3 vs. 18.3 %; only a 22 % reduction) thus improving the yield from the BMD scans. Under the new thresholds, the majority of women with fracture would merit therapy, ranging from 56.2 % of 70–74-year olds to 91.8 and 98.7 % at the ages of 80–84 and 85–90 years, respectively (Table 3, Fig. 4).
Discussion
In this study, we have explored the impact of adjusting the NOGG thresholds for women aged over 70 years of age in a UK setting. We have demonstrated that the current thresholds require a higher risk of fracture, particularly hip fracture, for treatment to be indicated in older women without a prior fracture than those qualifying on the basis of fracture alone. Furthermore, if clinicians undertake BMD measurements in women aged 75 years and older with fracture, we have demonstrated a discordance in the current advice of NOGG to treat all such women and the recommendation that follows the inclusion of BMD in the risk assessment. The analysis suggests that the use of the tested alternative thresholds in women aged 70–90 years can address both of these anomalies; fracture risk is more comparable in the groups of women identified for therapy, and treatment is recommended in the majority of older women with fracture, with or without the inclusion of BMD, thus reducing the need for BMD measurement.
In osteoporosis, a number of criteria have been advocated as thresholds for intervention with the presence of a prior fracture being the most widely adopted and present in one form or another in most national and international guidelines [1, 3, 6, 12, 16–18]. The use of absolute fracture risk allows comparison across groups identified by different risk profiles and highlights some of the disparities in selecting patients for therapy. For example, in an analysis of a large DXA database in Manitoba, Leslie and colleagues examined the proportions of patients, predominantly women, at low (<10 % probability), medium (10–20 %) and high (>20 %) risk of fracture identified by different criteria within the National Osteoporosis Foundation guidance from the USA. There were marked differences in the risk profiles of patients identified by T-score ≤ −2.5, prior fracture or economically defined FRAX thresholds (>3 % hip fracture probability or >20 % major fracture probability). In patients aged 65 years and over, only 39.6 % of patients selected for treatment with a T-score ≤ −2.5 had a fracture probability greater than 20 %, while in the same age category, patients with osteopenia had 77.3 % lying above the 20 % threshold. The concept that women without fracture merit treatment if their risk of fracture is similar to or exceeds that of an average woman with a prior fracture is a concept that attempts to embrace fairness and equity of access to treatment. However, our previous analysis of the NOGG thresholds also indicated a disparity in risk between women at older ages with and without fracture qualifying for therapy [14]. This reflects the setting of the threshold using a prior fracture in a woman of average BMI (24 kg/m2) so that one might expect half of women with a prior fracture to actually lie below the threshold due to the distribution of BMI. The advice to treat all older women with prior fracture necessarily lowers the probability of fracture in this group relative to that observed in women without fracture who still have to achieve the intervention threshold. It is important to appreciate, however, that despite the “lowering” of risk, the average probability of fracture in older women with fracture still remains very high. In all women aged 70+ years with fracture, the average probabilities of major osteoporotic fracture and hip fracture were 25.5 and 11.3 %, respectively; these were even higher in women aged 85–90 years being 29.4 and 15.6 %, respectively.
It is important to place the current and alternative thresholds in a health economic perspective. In the context of osteoporosis and fracture risk, the intervention threshold that is relevant for payers can be defined as the probability of fracture at which intervention becomes cost-effective. This approach has not been used in the UK by NOGG, but it is still important to underpin the chosen intervention thresholds by cost-effectiveness. Both strategies included in this analysis are highly cost-effective. In a previous paper, the relationship between FRAX probabilities and cost-effectiveness was examined for all possible combinations of clinical risk factors with BMD T-scores ranging between 0 and −3.5 SD [19]. In that analysis, treatment with generic alendronic acid was modelled at £95 per year, which is a very conservative figure since the current price has subsequently fallen to approximately £12. At the higher price, cost-effectiveness with a willingness-to-pay of £20,000 per quality-adjusted life year (QALY) was demonstrated for FRAX major osteoporotic fracture probabilities that exceeded 7–8 %. A similar analysis with risedronate, which cost £264 at the time, showed cost-effectiveness at a probability threshold of 19 % [20], close to the alternative intervention threshold studied in this paper. The eightfold reduction in the cost of alendronic acid since then and the more recent availability of cheap generic forms of other osteoporosis agents including risedronate, ibandronic acid and zoledronic acid support the notion that both thresholds comfortably represent highly cost-effective scenarios.
The alternative thresholds examined in this paper have important implications for the decision to undertake BMD measurements in older women with prior fracture before making treatment decisions. As we have demonstrated, if the NOGG advice to treat all women aged 75 years and over with prior fracture is ignored and a BMD is requested, treatment would be indicated only in a minority of such women (e.g. 41.8 % of 80–84-year olds). Confusion over the advice to treat is a likely result. Using the alternative thresholds, the majority (82.9 %) of women aged 80–84 years with a fracture would lie in the high-risk area, and the total proportion selected for treatment would increase to 91.8 % following BMD; the latter only undertaken in 16.9 % of the age group. The fact that almost 92 % of women aged 80–84 years with fracture would be selected for therapy suggests that the use of BMD to identify patients suitable for therapy in this age group is irrational and supports the current NICE and NOGG advice to treat older women with fracture without necessarily measuring BMD. Certainly, in the absence of easy access to BMD or to make better use of limited BMD resources, the alternative thresholds are consistent with the recommendation to consider treatment in all older women with prior fracture. This would, of course, not preclude the measurement of BMD for other purposes such as monitoring response or assessment prior to accessing high-cost therapies.
This analysis has a number of strengths and limitations. One limitation is that the studied population is a simulated cohort rather than a real population sample. However, the analysis is a comparison of two sets of thresholds within the same population so that conclusions drawn about the relative performance of the thresholds are largely independent of the study population. Furthermore, the simulation allows the impact of any changes in thresholds to be modelled at a population level rather than in subsets of the population. The present analysis has only been conducted in a cohort modelled on the age distribution of the UK, but given that the risk factor prevalences were derived from several European cohorts, it is likely that similar conclusions would be drawn across other European countries, with the only differences being driven by variations in the age distributions within these countries. The present analysis does not allow an examination of the impact of threshold changes in men beyond the obvious conclusion that more men at older ages would be selected for treatment under the alternative thresholds compared to existing thresholds. It should be noted that whereas the alternative threshold appears markedly different at older ages, the overall impact on the proportion of women selected for treatment is relatively small. Indeed the proportion of the population aged 50 years and over only increases from 38.0 to 40.8 %; the largest increase in proportion is observed in the most elderly with 63.7 % of 85–90-year olds being considered for treatment compared to 49.4 % under the current thresholds. In practice, it is unlikely that 63.7 % of women aged 85–90 years would initiate osteoporosis therapy due to other health considerations, so this proportion simply represents a theoretical maximum if the guidance was fully implemented. The approach is still somewhat conservative compared to other national guidance such as that endorsed by the National Osteoporosis Foundation where over 87 % of 80+ year-old non-Hispanic women would be selected for treatment [16, 21]. Finally, it should be acknowledged that the identification of a threshold for major osteoporotic fracture at or around 20 % is not a validation of this threshold on a global scale but rather represents a chance occurrence. Fortuitously, this is the probability at the age of 70 years in a woman with a prior fracture in the UK, but will differ if the same NOGG-like approach is taken to determining fracture thresholds in other populations.
The goal of setting intervention thresholds in a chronic disease is to maximise the benefit on outcomes while limiting the risks and costs that accompany the intervention. It is a complex process that includes consideration of country-specific factors such as reimbursement, cost-effectiveness and society’s willingness to pay [1]. Within a country, it would seem desirable that at any given age, the selection criteria for intervention results in equitable access to therapy for patients with the same age-specific absolute probability of fracture. We conclude that the alternative thresholds examined here achieve this objective and may indicate the need for a revision of the current thresholds at older ages in the UK guidance and that using similar approaches elsewhere.
References
Kanis JA, McCloskey EV, Johansson H, Cooper C, Rizzoli R, Reginster JY (2013) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 24(23–57):23079689
Grigorie D, Sucaliuc A, Johansson H, Kanis JA, McCloskey E (2013) FRAX-based intervention and assessment thresholds for osteoporosis in Romania. Arch Osteoporos 8(164):24390553
Compston J, Bowring C, Cooper A et al (2013) Diagnosis and management of osteoporosis in postmenopausal women and older men in the UK: National Osteoporosis Guideline Group (NOGG) update 2013. Maturitas 75(392–396):23810490
Lekamwasam S (2013) Sri Lankan FRAX model and country-specific intervention thresholds. Arch Osteoporos 8(148):23975235
Tuzun S, Eskiyurt N, Akarirmak U, Saridogan M, Johansson H, McCloskey E, Kanis JA (2012) The impact of a FRAX-based intervention threshold in Turkey: the FRAX-TURK study. Arch Osteoporos 7(229–235):23060308
Lekamwasam S, Adachi JD, Agnusdei D et al (2012) A framework for the development of guidelines for the management of glucocorticoid-induced osteoporosis. Osteoporos Int 23(2257–2276):22434203
National Institute for Health and Care Excellence (2012) NICE Clinical Guideline 146. Osteoporosis: assessing the risk of fragility fracture
Kanis JA, Johnell O, Oden A, Johansson H, McCloskey E (2008) FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int 19(385–397):18292978
Hippisley-Cox J, Coupland C (2012) Derivation and validation of updated QFracture algorithm to predict risk of osteoporotic fracture in primary care in the United Kingdom: prospective open cohort study. BMJ 344(e3427):22619194
Compston J, Cooper A, Cooper C, Francis R, Kanis JA, Marsh D, McCloskey EV, Reid DM, Selby P, Wilkins M (2009) Guidelines for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK. Maturitas 62(105–108):19135323
Bruyere O, Fossi M, Zegels B, Leonori L, Hiligsmann M, Neuprez A, Reginster JY (2013) Comparison of the proportion of patients potentially treated with an anti-osteoporotic drug using the current criteria of the Belgian national social security and the new suggested FRAX criteria. Rheumatol Int 33(973–978):22842952
Briot K, Cortet B, Thomas T et al (2012) 2012 update of French guidelines for the pharmacological treatment of postmenopausal osteoporosis. Joint Bone Spine 79(304–313):22521109
Johansson H, Oden A, Johnell O, Jonsson B, de Laet C, Oglesby A, McCloskey EV, Kayan K, Jalava T, Kanis JA (2004) Optimization of BMD measurements to identify high risk groups for treatment—a test analysis. J Bone Miner Res 19(906–913):15190881
Johansson H, Kanis JA, Oden A, Compston J, McCloskey E (2012) A comparison of case-finding strategies in the UK for the management of hip fractures. Osteoporos Int 23(907–915):22234810
NICE (2010) TA161 (amended) Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women. National Institute for Health and Clinical Excellence
Dawson-Hughes B, Looker AC, Tosteson AN, Johansson H, Kanis JA, Melton LJ 3rd (2010) The potential impact of new National Osteoporosis Foundation guidance on treatment patterns. Osteoporos Int 21(41–52):19705046
Dawson-Hughes B, Tosteson AN, Melton LJ 3rd, Baim S, Favus MJ, Khosla S, Lindsay RL (2008) Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporos Int 19(449–458):18292975
Hagino H (2014) Revised osteoporosis diagnostic criteria and Japanese practice guideline on osteoporosis. Clin Calcium 24:11–18, 24369275
Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A (2008) Case finding for the management of osteoporosis with FRAX—assessment and intervention thresholds for the UK. Osteoporos Int 19(1395–1408):18751937
Borgstrom F, Strom O, Coelho J, Johansson H, Oden A, McCloskey EV, Kanis JA (2010) The cost-effectiveness of risedronate in the UK for the management of osteoporosis using the FRAX. Osteoporos Int 21(495–505):19565175
Dawson-Hughes B, Looker AC, Tosteson AN, Johansson H, Kanis JA, Melton LJ 3rd (2012) The potential impact of the National Osteoporosis Foundation guidance on treatment eligibility in the USA: an update in NHANES 2005–2008. Osteoporos Int 23(811–820):21717247
Acknowledgments
We thank the Committee of Scientific Advisors for its critical review and endorsement of the manuscript.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
McCloskey, E., Kanis, J.A., Johansson, H. et al. FRAX-based assessment and intervention thresholds—an exploration of thresholds in women aged 50 years and older in the UK. Osteoporos Int 26, 2091–2099 (2015). https://doi.org/10.1007/s00198-015-3176-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-015-3176-0