
Abstract
Introduction and hypothesis
Urinary incontinence (UI) is prevalent among older women, but conservative treatment rates remain low due to limited accessibility, despite evidence supporting pelvic floor muscle training (PFMT) efficacy. Group-based approaches, including online options, could offer cost-effective alternatives. Recent evidence supports the feasibility of online group-based PFMT for treating UI in older women. This pilot study now evaluated the clinical effects of this program on the number of leakage episodes per day, additional UI-specific outcomes, and other symptoms and indicators.
Methods
Community-dwelling women aged 65 and over, with stress or mixed UI, were recruited. Eligibility was assessed through in-person evaluations conducted by pelvic floor physiotherapists, who instructed participants on pelvic floor muscle contraction using digital palpation. Participants engaged in a 12-week group-based PFMT program with weekly 1-h sessions. Data were collected at three time points: recruitment (PRE1), before the first session (PRE2), and after the program (POST). Participants recorded UI symptoms using 7-day bladder diaries and standardized questionnaires on UI symptoms, quality of life (QoL), UI self-efficacy, and perceived costs. After the program (POST), participants provided feedback on their impression of improvement and satisfaction.
Results
Participants reported a significant reduction in their number of leakage episodes per day. Standardized questionnaire scores also supported the positive effects of the program on UI symptoms and QoL, self-efficacy in avoiding leakage and performing PFMT exercises, and monthly costs for continence products. Older women expressed high satisfaction with symptom improvement and the program.
Conclusions
Online group-based PFMT improved UI symptoms, QoL, UI self-efficacy, and perceived UI costs among older women. Pragmatic randomized controlled trials are necessary for further validation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Urinary incontinence (UI) is a prevalent health concern among women aged 65 and over, affecting one in three women in that age group [1]. Left untreated, UI can have serious health consequences and negatively impact the quality of life (QoL) of older women. The recommended first-line treatment for UI is individual pelvic floor muscle training (PFMT) [2]. However, more than half of women with UI are not receiving treatment [3], primarily because of the limited accessibility of this non-invasive treatment option [4]. To address the needs of older women with UI, a randomized controlled trial demonstrated that group-based PFMT (the GROUP program) was not inferior to individual PFMT in treating UI in older women, despite using fewer resources, making it a more cost-effective option [5]. Furthermore, the COVID-19 pandemic highlighted the importance of online UI treatment options. In this context, the GROUP program was adapted to be delivered via telerehabilitation.
Telerehabilitation, which refers to the remote delivery of synchronous rehabilitation services, has demonstrated clinical effectiveness for other conditions [6]. However, evidence for the effectiveness of PFMT telerehabilitation is limited. Although two reviews explored this topic, neither of them included studies on synchronous group-based PFMT telerehabilitation [7, 8].
Recently, our pilot study on group-based PFMT telerehabilitation (the teleGROUP program) demonstrated good feasibility in older women [9]. Now, it is crucial to investigate its effects. Thus, this paper reports on the clinical effects of our pilot study evaluating the teleGROUP program for UI treatment in women aged 65 and over on the number of leakage episodes per day, additional UI-specific outcomes, and other symptoms and indicators.
Materials and Methods
Study Design
This pre-post pilot study is part of a larger research program aiming to assess the feasibility, acceptability, and effects of the teleGROUP program (ClinicalTrials.gov NCT05182632), the online adaptation of the GROUP program [5]. It follows the guidelines of the Consolidated Standards Of Reporting Trials extension statement [10]. A detailed protocol is available elsewhere [11].
Participants
Women were recruited through advertisements in community centres, newspapers, social media platforms, a research participant database, through promotion via relevant media and associations, and through referrals from three hospital-affiliated gynecology and urology clinics. Eligible women were aged 65 or older and had stress or mixed UI, confirmed by the Questionnaire for Incontinence Diagnosis (QUID) [12], with at least three weekly urine leakages persisting for 3 months or more [5]. Moreover, they were required to have internet access via their own device. Women with any risk factors or conditions known to interfere with PFMT or the evaluation of pelvic floor muscles (PFMs), such as the inability to voluntarily contract their PFM, important pelvic organ prolapse (Baden-Walker score > stage 2 [13]) or chronic constipation, were excluded from the study. The complete list is available elsewhere [11].
The study was aimed at recruiting at least 32 older women with UI to ensure a power of 1-β = 95% with an α error of 0.05 and an estimated effect size of 0.73 to detect a statistically significant difference in the number of urine leakages, with an anticipated attrition of 15% [5].
Intervention
Pelvic floor physiotherapists located in the participant's region conducted individual in-person evaluations to confirm eligibility [11]. During these sessions, they also provided instruction on correct PFM contraction through digital palpation and verbal cues.
Eligible participants then took part in the teleGROUP program, an online group-based PFMT program with 12 weekly 1-h training sessions delivered via Zoom by an experienced pelvic floor physiotherapist. An optional 13th session was available to all participants at the end of the program as a catch-up session for any missed sessions. Women participated in the program in groups of 6 to 11. The same physiotherapist delivered the intervention to all women groups. A brief Zoom familiarization session before starting the program and phone support throughout the sessions were offered as needed. All participants received a printed exercise booklet containing an exercise diary and educational material.
Each session began with a 3- to 5-min individual exchange between the physiotherapist and each participant in a private breakout room to quantify UI episodes in the previous week and reinforce exercise adherence through monitoring their exercise diary and offering brief individualized feedback. Meanwhile, the rest of the group socialized in the Zoom’s “main room.” Subsequently, all sessions included two parts: a 10- to 15-min educational component on topics relevant to UI and the pelvic floor, including anatomy, pathophysiology of incontinence and bladder control, and a 30- to 45-min PFM exercise component including a progression of four exercises, targeting strength, speed of contraction, endurance, and coordination. More in-depth information on both components is available elsewhere [9, 11]. In addition to group sessions, participating women also completed a home exercise program encompassing the same main four PFM exercises, 5 days per week for 12 weeks. The home exercises progressed over three phases, each lasting 4 weeks. This progression allowed for increasing difficulty in terms of duration, number of repetitions, and position (from lying to sitting to standing), reflecting the progression of the exercises through the group sessions.
Data Collection
Participants underwent pre-screening for eligibility through a phone interview. Subsequently, a specialized physiotherapist located in the women’s region conducted an individual in-person evaluation to confirm their eligibility. During this evaluation, the physiotherapist collected sociodemographic and health data, including age, height, weight, socioeconomic status, medical history, and general health characteristics, such as polypharmacy, parity, obstetric history, type of symptoms, and duration of UI symptoms. Additionally, the participants' cognition was assessed through the Mini-Mental State Exam [14] and Montreal Cognitive Assessment [15]. Furthermore, the physiotherapist also performed an intra-vaginal evaluation, using the PERFECT assessment scheme to assess PFM function through digital vaginal palpation [16], the Baden–Walker score [13] to investigate the presence and stage of any pelvic organ prolapse, and the Vaginal Atrophy Index to assess vaginal atrophy [17].
To assess the clinical effects of the teleGROUP program on their UI symptoms, participants reported urine leakage episodes in a 7-day bladder diary at three key time points: before the intervention during recruitment (PRE1), before the first session of the program (PRE2), and after the program (POST). Additionally, participants completed UI-specific questionnaires, including the International Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form (ICIQ-UI SF) [18], the International Consultation on Incontinence Questionnaire Lower Urinary Tract Symptoms Quality of Life Module (ICIQ-LUTSqol) [18], and the bladder subscale of the Australian Pelvic Floor Questionnaire (APFQ) [19] at PRE1, PRE2, and POST. PRE2 served as a second baseline measure to confirm the stability of the main UI-specific outcomes. Throughout the program, participants also recorded their weekly leakage episodes in a bladder diary. The primary outcome measures were the number of weekly leakages and their percentage reduction between PRE and POST measurements.
Participants also recorded data on other indicators by documenting their micturition in a 7-day bladder diary and completing other subscales of the APFQ [19] at PRE1, PRE2, and POST. Furthermore, all participants answered the Atrophy Symptom Questionnaire (ASQ) [20], the Geriatric Self-Efficacy index (GSE) [21], the Broome Pelvic Muscle Exercise Self-Efficacy Scale (PMSES) [22], the adapted Dowell-Bryant Incontinence Cost Index (DBICI) [23], and the Online Technologies Self-Efficacy Scale (OTSES) [24] at PRE1 and POST.
Following the program, participants provided feedback about the program using the Patient Global Impression of Improvement (PGI-I) index. They also completed single-item questionnaires to express their satisfaction with treatment outcomes, choosing between options such as “does not want other alternative treatments,” “would like another alternative treatment for UI,” “completely satisfied,” “somewhat satisfied,” or “unsatisfied.” Last, the women reported their satisfaction with their perceived improvement on a visual analog scale (VAS).
Analysis
Sociodemographic data were reported descriptively. When applicable, normality was assessed using Shapiro–Wilk tests, and means (SD) or medians (IQR) were reported accordingly. For the primary outcomes, differences in the median number of leakage episodes per day at PRE1, PRE2, and POST were examined using the Friedman test, followed by post-hoc Wilcoxon signed-rank tests. Leakage reduction, calculated as the median value of the leakage reduction percentage observed for each participant, was also investigated between PRE1 and POST.
Regarding secondary outcomes, differences between PRE1, PRE2, and POST were examined using one-way repeated analyses of variance (ANOVA), followed by post-hoc paired-samples Tukey’s tests for normally distributed data. For non-normally distributed data, Friedman tests were used, followed by post-hoc Wilcoxon signed-rank tests. PGI-I and satisfaction scores were reported using descriptive statistics.
In secondary analyses, Kaplan–Meier curves were used to estimate the probabilities of reducing weekly urine leakage episodes by the minimal clinically significant difference (MCID) of 50% and the incremental clinically significant difference (ICID) of 70% over time, considering both the overall sample and subgroups of interest (defined by age, UI duration, UI severity, and PFM strength). Sensitivity analyses used log-rank tests to compare specific subgroups (age, symptom duration, symptom severity, PFM strength) [25].
All statistical analyses were conducted using R version 4.3.1 and SPSS version 26.0.0.0, with an alpha level set at <0.05 for all statistical tests.
Results
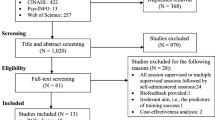
Out of the 34 participants recruited from March 2021 to April 2022, a total of 33 completed the program (Fig. 1). The median (IQR) interval between PRE1 and PRE2 was 23 (11.5–37.5) days. Included women had a median age of 69.0 (67.0–73.0) years. Their mean (SD) body mass index (BMI) was 25.2 (4.0). Almost 1 out of 2 were following hormonal treatment (15 out of 34, 44.1%), stable for at least 6 months, as per the eligibility criteria, with a median duration of 5.0 (3.0–10.0) years. Participants reported a median parity of 1.0 (0.0–2.0), and 55.9% had a history of gynecological surgery, with the most common procedure being a hysterectomy (12 out of 34, 35.3%). Most participants (32 out of 34, 94.1%) reported symptoms of mixed UI, with a median duration of 5.5 (3.0–16.0) years. When performing the PERFECT assessment, they demonstrated a median PFM strength of 3.0 (3.0–4.0) out of 5 for the power component of the scale, a median maximal contraction time of 5.0 (4.0–7.0) s for the endurance component, and a median maximal number of contractions of 5.5 (3.0–8.0) for the repetitions component. Table 1 presents all baseline characteristics of the participating women.

Flowchart of study participants
After the program, participants reported significant improvements in all UI-specific outcomes (Tables 2, 3). The Friedman test revealed a statistically significant difference in the number of daily leakage episodes among the three time points (χ2=33.207, p<0.001). Wilcoxon signed-rank post-hoc tests identified a significant reduction between PRE1 and POST, with the median number of daily leakage episodes decreasing from 1.9 (1.1–3.4) to 0.6 (0.3–0.9, p<0.001). This significant reduction was maintained between PRE2 and POST (p<0.001), whereas no significant difference was observed between PRE1 and PRE2 (p=1.000). Women achieved a median individual leakage reduction of 71% (51–86, Fig. 2).

Median reduction in urinary incontinence episodes
Among UI-specific questionnaires, ANOVA and Friedman tests revealed statistically significant differences in the ICIQ-UI SF, ICIQ-LUTSqol, and APFQ Bladder Function subscale scores among the three time points (F=14.93, p<0.001, χ2=26.807, p<0.001 and F=11.49, p<0.001 respectively, Table 2). Post-hoc tests identified significant improvements between PRE1 and POST in all three questionnaires, with mean ICIQ-UI SF scores decreasing from 12.4 (2.9) to 8.2 (3.9, p<0.001), median ICIQ-LUTSqol scores decreasing from 35.0 (28.5–41.3) to 29.3 (22.3–36.8, p=0.015), and mean APFQ Bladder Function subscale scores decreasing from 15.6 (5.3) to 10.0 (4.8, p<0.001). The significant reductions were also observed between PRE2 and POST (p<0.001, p=0.010, and p=0.001 respectively), whereas no differences were observed between PRE1 and PRE2 (p=0.773, p=1.000, and p=0.761 respectively).
Among other symptoms and indicators, the Friedman test revealed a statistically significant difference in micturition among the three time points (χ2=11.437, p=0.003). The median number of daily micturitions decreased from 7.1 (5.5–8.6) at PRE1 to 6.3 (5.3–7.9) at POST (p<0.001). The significant reduction was also observed between PRE2 and POST (p=0.001), whereas no difference was observed between PRE1 and PRE2 (p=0.761). Additionally, Wilcoxon signed-rank tests identified significant improvements after the program on the GSE, PMSES, and DBICI (Table 2). Median GSE scores increased from 62.0 (44.0–78.0) at PRE1 to 93.0 (68.0–102.5) at POST (p<0.001). PMSES median total scores increased from 66.1 (53.9–75.7) at PRE1 to 79.3 (70.2–92.0) in POST (p=0.001). DBICI perceived median monthly costs of disposable continence products decreased from $13.00 (3.1–26.3) at PRE1 to $2.00 (0.0–6.0) at POST (p=0.012). The participants reported no significant differences between PRE1 and POST on the APFQ Bowel Function, Prolapse or Sexual Function subscales, the ASQ, or the OTSES scores.
After the program, all participants (32 out of 32, 100%) reported a perceived improvement in their UI symptoms, with symptoms being described as “much better” (18 out of 32, 56.3%), “better” (6 out of 32, 18.8%) and “somewhat better” (8 out of 32, 25.0%). Most participants (29 out of 32, 90.6%) were satisfied with the treatment outcomes and were not interested in any alternative treatment. Regarding overall satisfaction, the majority of women were “completely satisfied” (23 out of 32, 71.9%) or “somewhat satisfied” (8 out of 32, 25.0%), whereas only one woman (3.1%) expressed being “unsatisfied,” as she perceived no improvement in her UI symptoms. Last, on the VAS, participants reported a high satisfaction level with their perceived improvement, with a median rating of 77.5% (65.0–90.0).
Regarding secondary analyses, individual leakage reduction was continuous throughout the program (Appendix 1). Median MCID (50% reduction) and ICID (70% reduction) were achieved by the 4th (95% CI 0.3 to 7.7) and 8th (95% CI 5.2 to 10.8) weeks of treatment respectively (Fig. 3). In sensitivity analyses, Kaplan–Meier curves indicated that no subgroup exhibited significant differences compared with the overall sample (Appendix 2).

Cumulative proportion of women with A minimal clinically important differences (MCID) and B incremental clinically important differences (ICID) by week
Discussion
This pilot study demonstrated promising results of group-based PFMT telerehabilitation for older women with UI, achieving a clinically significant leakage reduction of 71%. Participating women also reported a significant reduction in UI severity, with a difference in ICIQ-UI SF scores of 4.2 points, surpassing the clinically meaningful threshold of 2.5 [18]. Moreover, participants’ UI-associated QoL improved significantly, with a difference of 5.7 points in the ICIQ-LUTSqol score, exceeding the clinically meaningful threshold of 3.7 [18]. Additionally, there was a significant improvement in bladder function, with a difference of 5.6 in the APFQ Bladder Function subscale, surpassing the clinically meaningful threshold of 1.3 points [19]. Furthermore, participants achieved a significant reduction in daily micturition frequency by 0.8 (11.3%), although this reduction fell below clinically meaningful thresholds, ranging from 15% to 50% [26]. Participants also demonstrated an increased self-efficacy in avoiding urine leakage, with a difference in GSE scores of 31.0, twice the clinically meaningful threshold of 14.0 points [21]. Moreover, their self-efficacy in performing PFMT exercises improved from “moderate” to “high” on the PMSES [22]. Participants also reported a significant reduction in their perceived monthly costs of disposable continence products by $11.00 CAD (84.6%), exceeding other reports of nonsurgical UI treatment in older women, which described only a 68% reduction [27]. Overall, participants expressed a high level of satisfaction with the program, with the majority (29 out of 32, 90.6%) not being interested in any alternative treatment. Furthermore, in secondary analyses, participants achieved a median MCID by the 4th week of treatment and a median ICID by the 8th week of treatment.
The teleGROUP program is an online adaptation of the in-person GROUP program, which was shown to be non-inferior to individual PFMT for the treatment of stress and mixed UI in older women [5]. The recruited women in both studies shared similar characteristics. Women in teleGROUP had a median age of 69.0 (67.0–73.0) years old and a mean BMI of 25.0 (3.8), compared to a mean age of 68.0 (5.7) and a mean BMI of 27.0 (4.5) in GROUP [5]. Before the program, women in teleGROUP reported a median of daily leakages of 1.9 (1.1–3.4) at PRE1 and 1.6 (0.9–2.4) at PRE2, compared to a median of 1.43 (0.86–2.14) in GROUP [5]. In addition, women in teleGROUP obtained mean scores of 12.4 (2.9) at PRE1 and 11.8 (3.8) at PRE2 on the ICIQ-UI SF, compared to a median of 12.0 (10.0–15.0) in GROUP [5]. According to the current findings, teleGROUP also demonstrates comparable clinical effects, achieving a median leakage reduction of 71% compared with 74% in GROUP [5]. However, its benefits may take a little longer to appear, with women achieving a median MCID and ICID by the 4th and 8th weeks in teleGROUP respectively compared with the 4th and 6th weeks in GROUP [25]. The improvements in other UI-specific outcomes in teleGROUP were slightly lower, with a reduction of ICIQ-UI SF and ICIQ-LUTSqol scores by 4.2 and 5.7 respectively compared with 5.0 and 8.0 in GROUP [5]. Improvements in other indicators were also slightly lower, with a micturition frequency reduction of 0.8 and a GSE score reduction of 31.0 in teleGROUP, in comparison with 1.93 and 36.0 in GROUP respectively. Nevertheless, satisfaction rates were the same in both programs, with both teleGROUP and GROUP showing 91% satisfaction. Although participants from both studies shared overall similar characteristics, participants in teleGROUP showed a higher proportion of mixed UI symptoms (94% compared with 85% in GROUP) [5]. Mixed symptoms generally respond less effectively to treatment [28], which might account for the longer time needed to achieve ICID in teleGROUP and the slightly lower improvements in various UI-related outcomes. Nevertheless, this explanation should be interpreted with caution as the sample size of this study was limited to 34 women.
Although there are currently no similar pelvic floor telerehabilitation interventions targeting older women in the literature, other remote programs have shown clinical benefits in treating UI. In a review on telehealth for women with pelvic floor dysfunction, one study targeted older women [7]. Although not specifically on online PFMT, this study involved an 8-week continence management program in which participants attended a series of weekly educational talks led by a nurse, discussing PFM exercises, among other topics. Women were encouraged to complete PFM exercises at home. The nurse delivered this educational program either remotely to a group of older women, who attended the sessions using videoconference from a community center, or face-to-face. Thus, participating women in the “remote” group still had to travel to receive their care. All women first underwent an in-person pelvic floor evaluation, including vaginal digital palpation. Upon program completion, participants in both the “remote” and the “face-to-face” groups reported a significant reduction in the number of daily leakage episodes, with the “remote” group reporting a reduction of 1.1 (85%) [29]. These results align with the current findings supporting the positive effects of remotely provided continence care for older women following an in-person pelvic floor evaluation. Another systematic review further investigated remote rehabilitation methods for delivering PFMT, with a focus on asynchronous alternatives, while emphasizing the importance of investigating videoconferencing options. However, only one of the included studies targeted older women [8]. This underscores the importance of gathering more evidence on the impact of these innovative care options for older women with UI. Ultimately, this could help to support universal access to continence care for this population.
This study has several strengths. Building upon a strongly established PFMT program [5], it was to our knowledge the first to evaluate pelvic floor telerehabilitation for older women with UI. It provided timely evidence to address the previously identified accessibility issues to this type of care [4], thus laying the groundwork for further research in this domain. For instance, these findings could provide essential data for conducting power calculations in the design of larger-scale controlled trials with various designs, such as superiority or non-inferiority, involving two or more study arms. The trials can encompass diverse comparative groups, including in-person group-based PFMT, app-based PFMT, or other alternatives. Moreover, the study employed a rigorous design, moderating the lack of a control group by conducting repeated measures at baseline, with two pre-treatment evaluations (PRE1 and PRE2). It also evaluated the program’s clinical effects using multiple UI-related indicators to accurately assess emerging patterns, which further strengthened the design.
Conversely, this study also has some limitations, mostly due to its pilot design. Nevertheless, pilot studies play a pivotal role in the research process [30] and the current findings can guide the next steps of group-based PFMT telerehabilitation research. Notably, despite the inclusion of a second baseline measurement, the study design lacked randomization to both a treatment and a control group, thereby limiting the robustness of the findings. In addition, although both measurements occurred before the program, the interval between PRE1 and PRE2 was not standardized. It also lacked correction for multiple testing. Participant recruitment relied on a voluntary basis, and having internet access was part of the eligibility criteria, which may have resulted in a specific profile of older women with UI in the sample. Consequently, the generalizability of the results may be limited. However, group-based PFMT telerehabilitation still holds promise for a considerable proportion of older women, as more than two-thirds of older adults have internet access [31].
In conclusion, group-based PFMT telerehabilitation following in-person pelvic floor evaluation appears to be effective in improving UI symptoms, other urinary symptoms, and UI-related self-efficacy. Additionally, it leads to a reduction in perceived UI costs among older women and high levels of satisfaction. Pragmatic randomized controlled trials would be welcome to confirm these results.
References
Milsom I, Coyne KS, Nicholson S, Kvasz M, Chen C-I, Wein AJ. Global prevalence and economic burden of urgency urinary incontinence: a systematic review. Eur Urol. 2014;65(1):79–95.
Abrams P, Anderson KE, Apostolidis A, et al. Recommendations of the International Scientific Committee: evaluation and treatment of UI, bladder pain syndrome, POP and fecal incontinence. In: Abrams P, Cardozo L, Khoury AE, Wein A, editors. 6th Ed. International Consultation on Urinary Incontinence. 2. Plymbridge, UK: Health Publications. 2017. p. 2549–619.
Johnson T II, Kincade J, Bernard S, Busby-Whitehead J, DeFriese G. Self-care practices used by older men and women to manage urinary incontinence: results from the national follow-up survey on self-care and aging. J Am Geriatr Soc. 2000;48(8):894–902.
Le Berre M, Dumoulin C. Accessibility of pelvic floor physiotherapy for treating urinary incontinence in older women in Quebec: an online survey. Physiother Can. 2022;https://doi.org/10.3138/ptc-2021-0089.
Dumoulin C, Morin M, Danieli C, et al. Group-based vs individual pelvic floor muscle training to treat urinary incontinence in older women: a randomized clinical trial. JAMA Int Med. 2020;180(10):1284–93.
Cottrell MA, Galea OA, O’Leary SP, Hill AJ, Russell TG. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: a systematic review and meta-analysis. Clin Rehab. 2017;31(5):625–38.
Da Mata KRU, Costa RCM, Carbone ÉSM, et al. Telehealth in the rehabilitation of female pelvic floor dysfunction: a systematic literature review. Int Urogynecol J. 2021;32(2):249–59.
Papanikolaou DT, Lampropoulou S, Giannitsas K, Skoura A, Fousekis K, Billis E. Pelvic floor muscle training: novel versus traditional remote rehabilitation methods. A systematic review and meta-analysis on their effectiveness for women with urinary incontinence. Neurourol Urodyn. 2023;42(4):856–74.
Le Berre M, Filiatrault J, Reichetzer B, Dumoulin C. Group-based pelvic floor telerehabilitation to treat urinary incontinence in older women: a feasibility study. Int J Environ Res Public Health. 2023;20(10):5791.
Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239.
Le Berre M, Filiatrault J, Reichetzer B, Dumoulin C. Feasibility, acceptability and effects of a group pelvic floor muscle telerehabilitation program to treat urinary incontinence in older women. Digital Health J. 2022;8:1–13.
Bradley CS, Rahn DD, Nygaard IE, et al. The questionnaire for urinary incontinence diagnosis (QUID): validity and responsiveness to change in women undergoing non-surgical therapies for treatment of stress predominant urinary incontinence. Neurourol Urodyn. 2010;29(5):727–34.
Baden W, Walker T. Genesis of the vaginal profile: a correlated classification of vaginal relaxation. Clin Obstet Gynecol. 1972;15(4):1048.
Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–35.
Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–9.
Laycock J, Whelan M, Dumoulin C. Patient assessment. Therapeutic management of incontinence and pelvic pain. Berlin: Springer; 2008. p. 57–66.
Leiblum S, Bachmann G, Kemmann E, Colburn D, Swartzman L. Vaginal atrophy in the postmenopausal woman. The importance of sexual activity and hormones. JAMA. 1983;249(16):2195–8.
Nyström E, Sjöström M, Stenlund H, Samuelsson E. ICIQ symptom and quality of life instruments measure clinically relevant improvements in women with stress urinary incontinence. Neurourol Urodyn. 2015;34(8):747–51.
Baessler K, Mowat A, Maher CF. The minimal important difference of the Australian Pelvic Floor Questionnaire. Int Urogynecol J. 2019;30(1):115–22.
Davila GW, Singh A, Karapanagiotou I, et al. Are women with urogenital atrophy symptomatic? Am J Obstet Gynecol. 2003;188(2):382–8.
Tannenbaum C, Brouillette J, Michaud J, et al. Responsiveness and clinical utility of the geriatric self-efficacy index for urinary incontinence. J Am Geriatr Soc. 2009;57(3):470–5.
Broome BA. Development and testing of a scale to measure self-efficacy for pelvic muscle exercises in women with urinary incontinence. Urol Nurs. 1999;19(4):258–68.
Dowell CJ, Bryant CM, Moore KH, Simons AM. Calculating the direct costs of urinary incontinence: a new test instrument. BJU Int. 1999;83(6):596–606.
Miltiadou M, Yu CH. Validation of the Online Technologies Self-Efficacy Scale (OTSES). Educational Resources Information Center (ERIC). 2000.
Cacciari L, Morin M, Mayrand M, Dumoulin C. 288—When can we expect clinically important differences from pelvic floor muscle training for urinary incontinence in older women? Continence. 2023;7:101005.
Frankel J, Staskin D, Varano S, Kennelly M, Newman DK, Rosenberg MT, et al. Interpretation of the Meaningfulness of Symptom Reduction with Vibegron in Patients with Overactive Bladder: Analyses from EMPOWUR. Adv Ther. 2022;39(2):959–70.
Simons AM, Dowell CJ, Bryant CM, Prashar S, Moore KH. Use of the Dowell Bryant Incontinence Cost Index as a post-treatment outcome measure after non-surgical therapy. Neurourol Urodyn. 2001;20(1):85–93.
Nygaard IE. Evidence-based treatment for mixed urinary incontinence. JAMA. 2019;322(11):1049–51.
Hui E, Lee PSC, Woo J. Management of urinary incontinence in older women using videoconferencing versus conventional management: a randomized controlled trial. J Telemed Telecare. 2006;12(7):343–7.
Van Teijlingen E, Hundley V. The importance of pilot studies. Social research update. 2001;(35):1–4.
Jaana M, Tamim H, Pare G. National survey of older adults in Canada: social and health care system determinants of E-Health applications use. Proceedings of the 56th Hawaii International Conference on System Sciences. 2023.
Acknowledgements
We thank all participating women and physiotherapists for their support in the data collection phase of the study. We also thank the many community groups and associations that kindly assisted in relaying our advertisements for recruiting study participants. A special thank you to Sophie Mont-Briant for her support throughout the research process, as well as to Ali Filali and Licia Cacciari for their advice on statistical methodology.
Institutional Review Board Statement
The study was approved by the Ethics Committee Board of the Aging-Neuroimaging research of the Centre Intégré Universitaire de Santé et de Services Sociaux du Centre-Sud-de-l’île-de-Montréal on March 6th 2021 (CER VN 20-21-33).
Funding
This research was funded by the advisory committee for clinical research (CAREC) of the Research Centre of the Institut universitaire de gériatrie de Montréal (CRIUGM) clinical research support grant, and by the Quebec network for research on aging (RQRV) grant for pilot projects. The funders were not involved in any aspect of the study design, data acquisition, data analysis, interpretation of data, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
M. Le Berre: conceptualization, investigation, data curation, analysis, funding acquisition, project administration, writing—original draft; J. Filiatrault: funding acquisition, writing—review & editing; B. Reichetzer: conceptualization, funding acquisition, validation, writing—review and editing; D. Kairy: writing—review and editing; C. Lachance: writing—review & editing; C. Dumoulin: conceptualization, investigation, data curation, analysis, funding acquisition, supervision, validation, writing—review & editing.
Corresponding author
Ethics declarations
Conflicts of Interest
None.
Additional information
Handling Editor: Holly E. Richter
Editor in Chief: Maria A. Bortolini
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 247 kb)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Le Berre, M., Filiatrault, J., Reichetzer, B. et al. Online Group-based Pelvic Floor Muscle Training for Urinary Incontinence in Older Women: a Pilot Study. Int Urogynecol J 35, 811–822 (2024). https://doi.org/10.1007/s00192-024-05728-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-024-05728-0