
Abstract
Introduction and hypothesis
The efficacy of physiotherapy for postpartum lower urinary tract symptoms (LUTS) has attracted considerable research interest. In the current study we evaluated the efficacy and safety of pelvic floor muscle training (PFMT) combined with biofeedback (BF), electrical stimulation (ES) therapy, or both for postpartum LUTS.
Methods
PUBMED, EMBASE, Web of Science, Cochrane Library, Chinese Biomedical Literature Database, China National Knowledge Infrastructure, Chinese Science and Technique Journals Database, and Wanfang databases were searched from inception to December 2020. Eligible randomized controlled trials on postpartum LUTS comparing PFMT plus BF, ES, or both with PFMT alone were included. The Cochrane handbook was used to evaluate the quality of the studies.
Results
Seventeen studies were included. The results of the meta-analysis showed that PFMT plus ES with or without BF was more effective than PFMT alone. Patients receiving PFMT plus ES and BF achieved greater improvement than controls receiving PFMT alone in incontinence quality of life scores (mean difference: 15.33, 95% confidence interval [CI]: 11.70–18.97, P < 0.00001), pelvic floor muscle strength (risk ratio: 2.29, 95% CI: 1.53–3.43, P < 0.0001), and urodynamic parameters (maximum urethral closure pressure, abdominal leak point pressure, and maximum urinary flow rate), and 1-h urine leakage (standardized mean difference: −0.70, 95% CI: −1.23 to −0.17, P = 0.010) also decreased.
Conclusions
PFMT plus ES with or without BF exhibited better efficacy and safety for early postpartum LUTS than PFMT alone.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lower urinary tract symptoms (LUTS) are characterized as a departure from normal in structure, function, or sensation experienced by a woman throughout the micturition cycle [1]. An investigation [2] revealed that 55.3% of women experienced LUTS 6 weeks after delivery. For some women, postpartum LUTS are temporary, but a considerable number of postpartum women experience long-term issues. A longitudinal cohort study [3] revealed that the incidence of maternal urge urinary incontinence (UUI) and stress urinary incontinence (SUI) increased from 5.7% and 29.9% during pregnancy to 22.8% and 46.4% at 1 year after delivery and 10.2% and 23.7% at 7 years after delivery, respectively. Thus, early effective therapies are clearly needed to prevent and treat postpartum LUTS.
Pelvic floor muscle training (PFMT) is currently recommended as a first-line treatment for postpartum urinary incontinence (PUI) [4, 5]. Physiotherapy, particularly biofeedback (BF), is an active pelvic floor muscle exercise. Since Kegel reported a BF success rate as high as 84% in 1951, BF has been considered to be a valuable method for female urinary incontinence [6]. Conversely, electrical stimulation (ES) is a passive exercise that can contract the pelvic floor muscles to increase functional endurance [7]. Most of the previous meta-analyses [8,9,10,11] mainly focused on the efficacy of PFMT alone or in combination with other methods in treating postpartum LUTS. This review focused on analyzing the efficacy and safety of PFMT plus BF, ES, or both compared to PFMT alone for the management of postpartum LUTS.
Materials and methods
Eligibility criteria
Types of studies
Randomized controlled trials (RCTs) that evaluated PFMT combined with BF, ES, or both in treating LUTS in postpartum women were included in this meta-analysis. Non-RCTs, cohort studies, quasi-experimental studies, observational studies, cross-sectional studies, case reports, animal studies, reviews, and experience summaries were excluded. Studies published in English and Chinese were included, regardless of whether they were blinded or not.
Types of participants
Studies on women experiencing LUTS within 1 year after delivery were included, with diagnosis of LUTS being confirmed on the basis of urodynamic testing, ultrasonography, clinical symptoms, or the relevant guidelines for the diagnosis and treatment of female stress urinary incontinence [12]. Studies that comprised pregnant participants were excluded. We intended to exclude the history of PUI/prolapse before pregnancy; however, most studies did not report this criterion. Therefore, we removed this exclusion criterion.
Types of interventions
The experimental group was treated with PFMT combined with BF, ES, or both, without limiting the application regimen (duration or frequency of application) for the treatment of LUTS. The control group was treated with PFMT alone.
Outcome measurements
The primary outcomes were the therapeutic effect and pelvic floor muscle strength. The definition of total therapeutic effect in this meta-analysis was based on guidelines for the diagnosis and treatment of female stress urinary incontinence published in 2017 in China [12]. As for patients with PUI, cure was defined as no leakage of urine and/or the urine leakage of 1-h pad test was < 1 g in the case of increased abdominal pressure, such as coughing. Improvement was defined as reduced urine leakage and/or the urine leakage in the 1-h pad test was reduced by ≥ 50% compared with before treatment when abdominal pressure increased. Failure was defined as leakage of urine when coughing and other abdominal pressure increased and/or the 1-h urine pad test urine leakage decreased by < 50% compared with before treatment. For patients with postpartum urinary retention (PUR), cure was defined as the ability to urinate independently and post-void residual (PVR) < 50 ml. Improvement was defined as PVR between 50 and 100 ml. Failure was defined as an inability to urinate spontaneously or PVR > 100 ml. The total therapeutic effect of this meta-analysis included cure rate and improvement rate. The secondary outcomes were comprised of indicators based on storage and voiding LUTS in postpartum patients. Storage symptom outcomes were measured using incontinence quality of life scores (I-QoL) and the 1-h pad test. Voiding symptom outcomes were measured using urodynamic parameters, including abdominal leak point pressure (ALPP), maximum urethral closure pressure (MUCP), maximum flow rate (Qmax), and voiding time (VT). Adverse events associated with the therapies were also reported.
Literature search
This systematic review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [13]; the protocol was registered in the PROSPERO database (CRD42021238443). Electronic searches of the databases were independently conducted by two reviewers (Dai Zhu and Zhiqi Yang) from database inception to December 2020. The PUBMED, EMBASE, Web of Science, Cochrane Controlled Trail Register of Controlled Trials, Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), Chinese Science and Technique Journals Database (VIP), and Wanfang databases were systematically searched. The reference lists of the included studies and identified reviews were analyzed to replenish the grey literature. We used the retrieval method of medical subject headings (MeSH) in combination with free-text terms. The search terms used were as follows: “pelvic floor muscle exercise,” “pelvic floor muscle training,” “Kegel exercise,” “biofeedback,” “electrical stimulation,” “pelvic floor rehabilitation,” “physiotherapy,” “lower urinary tract symptoms,” “LUTS,” “overactive bladder,” “OAB,” “voiding dysfunction,” “urinary incontinenc,” “urinary retention,” “nocturia,” “enuresis,” “postpartum,” “after labor,” “after pregnancy,” “after birth,” “postnatal,” and “puerperium.” All the databases were searched. If the retrieved data were incomplete, the data were obtained by contacting the authors via e-mail.
Data extraction
One reviewer (Dai Zhu) independently screened the literature by reading the titles as well as the abstracts. The screening process was double-checked by a second reviewer (Zhijun Xia). After excluding studies that did not meet the inclusion criteria or could not be ascertained due to limited information, the full text of the studies that might fulfil the eligibility criteria was further read and finally the studies to be included were determined. The following details were extracted from each included study: basic research information (the first author’s name and publication year); basic demographic data of the participants (age, parity, sample size, delivery mode, the type of postpartum LUTS, and the baseline severity of LUTS); intervention measures of the experimental and control groups; evaluation time, intervention duration, and follow-up duration; and outcome indicators.
Quality assessment
To ascertain the validity of the eligible RCTs, two of the meta-analysis authors (Dai Zhu and Zhijun Xia) independently evaluated the methodological quality of all included studies according to the quality evaluation items recommended in the Cochrane Handbook for Systematic Reviews of Interventions [14]. The evaluation items included seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. For each study, each of the aforementioned items were judged as ‘high risk of bias,’ ‘low risk of bias,’ or ‘unclear risk of bias’ (lack of relevant information or uncertainty about bias).
Statistical analysis
Statistical analysis was performed using Review Manager 5.4 software (Cochrane Community, London, UK). First, heterogeneity analysis was performed. When I2 < 50% and P > 0.10, the effect values of the included independent studies were considered homogeneous, and the fixed-effect model was used for statistical analysis. When I2 > 50% and P < 0.10, the effect values of the included studies were considered heterogeneous, and the potential sources of heterogeneity were further analyzed through subgroup analysis and sensitivity analysis.
Subgroup analysis
Based on the intervention time, postpartum LUTS types, delivery mode, follow-up duration, and evaluation method of the pelvic floor muscles, subgroup analysis was performed to determine whether the results of the study were influenced by these factors.
Sensitivity analysis
Individual studies that caused heterogeneity were excluded using the leave-one-out approach, and the results of the meta-analysis before and after inclusion were compared to determine the impact of these studies on the pooled effect.
If heterogeneity could not be solved, the random-effect model was used for statistical analysis. When the outcome data were qualitative or dichotomous variables, the risk ratio (RR) and 95% confidence interval (CI) were used. When the outcome data were quantitative or continuous variables, the mean difference (MD) or standardized mean difference (SMD) and 95% CI were used. P < 0.05 was considered statistically significant. Furthermore, if the number of eligible trials was ≥ 10, funnel plots were drawn to evaluate whether there was publication bias in the results of the meta-analysis [15].
Results
Results of the literature retrieval
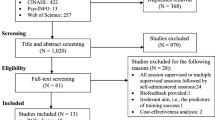
After systematic retrieval, 1248 studies were identified, including 593 Chinese studies and 655 English studies. After removing duplicate studies, 537 were eligible. By reading the titles and abstracts, 90 reviews and 386 studies that did not meet the inclusion criteria were excluded, and the remaining 51 Chinese and 10 English papers were further evaluated. Among 61 studies, 31 were excluded because the studies were not RCTs, 6 were excluded because the studies were not listed for specific implementation plans, 5 were excluded owing to ineligible control groups, and 2 were excluded owing to incomplete data. Finally, a total of 17 RCTs [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32] were included in this meta-analysis, all of which were published in Chinese. The specific screening process is illustrated in Fig. 1.

The flow diagram of literature searching, screening, and selecting eligible studies
Basic characteristics of the included studies
This meta-analysis included 17 studies, all of which were prospective RCTs. A total of 2315 cases were included (1158 in the experimental group and 1157 in the control group). The sample size of all the included studies ranged from 40 to 680 cases. Regarding the type of postpartum LUTS, 15 studies [16,17,18,19,20,21,22,23,24,25,26,27, 30,31,32] involved PUI and the other 2 studies [28, 29] involved PUR. The intervention methods in 15 studies [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30] involved PFMT plus BF and ES and two RCTs [31, 32] involved PFMT plus ES. No eligible studies involving PFMT plus BF for postpartum LUTS were retrieved. The basic characteristics and data of the studies included in the meta-analysis are summarized in Table 1. The specific intervention protocols for the intervention and control groups are listed in Table 2.
Quality assessment
The risk bias in the included studies was evaluated according to the quality evaluation items recommended in the Cochrane Handbook for Systematic Reviews of Interventions. All included studies referred to randomization, of which 11 studies [16,17,18, 20, 22,23,24, 27,28,29, 31] used the random number table method and therefore exhibited a low risk of bias. The remaining six studies [19, 21, 25, 26, 30, 32] did not specify the randomization sequence methods and therefore had a high risk of bias. None of the studies reported allocation concealment. Only one study [21] implemented blinding of the outcome assessment; the remaining 16 studies did not implement blinding. All participants in the 17 studies had undergone follow-up evaluations. No selective bias was reported in any study. The results of the literature bias evaluation are shown in Fig. 2.

a Risk of bias summary. b Risk of bias graph
Overall meta-analysis results
PFMT plus BF and ES versus PFMT alone
Fifteen studies were eligible [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30] for evaluation of PFMT plus BF and ES versus PFMT alone. The studies included 1965 postpartum women (983 in the PFMT plus BF and ES group and 982 in the PFMT group).
Therapeutic effects
Among the 14 eligible studies [16, 17, 19,20,21,22,23,24,25,26,27,28,29,30]that compared the interventions, the participants of 12 RCTs [16, 17, 19,20,21,22,23,24,25,26,27, 30] were PUI patients with a total of 1621 patients. The other two RCTs [28, 29] involved PUR patients with a total of 258 patients. Heterogeneity analysis (I2 = 0%, P = 0.64) indicated that there was homogeneity among the studies. The fixed-effect model was adopted for statistical analysis of the pooled effect. The pooled effect results (RR: 1.20, 95% CI: 1.15–1.24, P < 0.00001) showed a significant improvement in therapeutic effects in patients undergoing treatment with PFMT combined with ES and BF compared to those undergoing PFMT alone (Fig. 3a).

Forest plot of therapeutic effect: a PFMT+ES + BF vs PFMT alone. b PFMT+ES vs PFMT alone. CI: confidence interval
Pelvic floor muscle strength
The evaluation criterion for pelvic floor muscle (type I and type II) strength abnormalities was muscle strength ≤ grade III [33]. Five RCTs [18, 21, 23, 24, 30] analyzed the classification of pelvic floor muscle strength with a total of 340 patients. Heterogeneity analysis (I2 = 66%, P = 0.02) indicated that the heterogeneity among the studies was considerable. The random-effect model was adopted for statistical analysis of the pooled effect. The pooled effect results (RR: 2.29, 95% CI: 1.53–3.43, P < 0.0001) showed that the difference between the two groups was statistically significant. The results demonstrated that the incidence of pelvic floor muscle strength > grade III in the PFMT combined with the BF and ES group compared with the control group increased significantly, indicating that PFMT combined with BF and ES therapy effectively improved the pelvic floor muscle strength in postpartum women (Fig. 4a).

Forest plot of pelvic floor muscle strength (a), forest plot of pelvic floor muscle strength for sensitivity analysis (b), and forest plot of pelvic floor muscle strength for subgroup analysis (c). CI: confidence interval
Because the heterogeneity was significant, we performed a sensitivity analysis to determine the heterogeneity values following individual elimination of studies. The heterogeneity was reduced by 38% after eliminating the study by Zhang et al. [23] (RR: 1.93, 95% CI: 1.39–2.67, P < 0.0001; Fig. 4b), indicating that this study was likely the source of heterogeneity. This finding suggests that the research object of the eliminated study was PUI, whereas the research object of the other studies was postpartum stress urinary incontinence (PSUI). In addition, considering that the mode of delivery and follow-up time could be related to the change in pelvic floor muscle strength among postpartum women, we performed subgroup analysis according to them; however, the heterogeneity remained substantial. Moreover, we proceeded to perform subgroup analysis to further explore the sources of heterogeneity. The evaluation methods used in the studies for assessing pelvic floor muscle function were the PHENIX USB2 Pelvic Floor Rehabilitation Therapeutic Apparatus [23, 30] and Manual Muscle Testing (MMT) using the Muscle Strength Oxford Scale [18, 21, 24]. After subgroup analysis according to these evaluation methods, the heterogeneity was significantly reduced (I2 = 0% and I2 = 14%, respectively). The above results revealed that the evaluation method was the main source of heterogeneity (Fig. 4c).
One-hour pad test
To quantify urinary loss, the 1-h pad test was used. Five eligible RCTs [17, 18, 21, 22, 28] were included. Heterogeneity analysis (I2 = 92%, P < 0.00001) indicated that the heterogeneity among the studies was considerable. The random-effect model was adopted for statistical analysis of the pooled effect. The pooled effect results (SMD: −0.70, 95% CI: −1.23 to −0.17, P = 0.010) showed that PFMT combined with BF and ES reduced the 1-h urine leakage by −0.70 g. The results revealed that PFMT combined with BF and ES significantly reduced the amount of postpartum urine leakage compared to the control interventions (Fig. 5a).

Forest plot of 1-h pad test (a), subgroup analysis of 1-h pad test in two groups of patients with different type of postpartum LUTS (b) and with different treatment durations (c). CI: confidence interval
To explore the sources of heterogeneity, subgroup analysis was performed based on the type of postpartum LUTS (PUI and PUR). The heterogeneity within the subgroup was not significantly reduced compared with the overall heterogeneity after subgroup analysis (Fig. 5b). Subsequently, we performed subgroup analysis according to the intervention duration (< 8 weeks and ≥ 8 weeks). The heterogeneity was significantly reduced after subgroup analysis (I2 = 0% and I2 = 0%, respectively). The intervention duration < 8 weeks (SMD: −0.16, 95% CI: −0.31 to −0.02, P = 0.03) and the intervention duration ≥ 8 weeks (SMD: −1.12, 95% CI: −1.35 to −0.88, P < 0.00001) were both statistically significant (Fig. 5c). The above results suggested that the intervention duration was the main source of heterogeneity.
Incontinence quality of life scores
The I-QoL questionnaire was used to evaluate constraints on behavior, psychological impact, and social embarrassment [34]. In terms of quality of life, two eligible RCTs [16, 27] were included, with a total of 260 patients. Heterogeneity analysis (I2 = 66%; P = 0.09) indicated that the heterogeneity between the studies was considerable. The random-effect model was adopted for statistical analysis of the pooled effect. The pooled effect results (MD: 15.33, 95% CI: 11.70–18.97, P < 0.00001) demonstrated that compared to women trained with PFMT alone, the women trained with PFMT combined with BF and ES had greater I-QoL scores. Thus, PFMT combined with BF and ES effectively improved the postpartum quality of life (Fig. 6).

Forest plot of incontinence quality of life scores (I-QoL). CI: confidence interval
Urodynamic parameters
Urodynamic parameters, including MUCP, ALPP, detrusor leak point pressure (DLPP), Qmax, and PVR, are mainly associated with voiding dysfunction. Only two eligible RCTs [17, 27] evaluated some of the urodynamic parameters, including ALPP, MUCP, and Qmax, with a total of 334 patients. As shown in Fig. 7a–c, compared with PFMT alone, PFMT plus BF and ES boosted the ALPP (MD: 9.11, 95% CI: 5.75–12.46, P < 0.00001, I2 = 0%), MUCP (MD: 7.87, 95% CI: 6.41–9.33, P < 0.00001, I2 = 0%), and Qmax (MD: 2.62, 95% CI: 1.93–3.32, P < 0.00001, I2 = 0%).

Forest plot of urodynamic parameters: abdominal pressure urine leakage point pressure (ALPP) (a), maximum urethral closure pressure (MUCP) (b), and maximum urinary flow rate (Qmax) (c). CI: confidence interval
PFMT plus ES versus PFMT alone
Two studies were eligible [31, 32] for evaluation of PFMT plus ES versus PFMT alone. The studies included 350 women (175 in the PFMT plus ES group and 175 in the PFMT alone group). We included both studies in the quantitative analyses for at least one outcome.
Therapeutic effects
Both studies [31, 32] reported on the total therapeutic effect and were included in a fixed-random model showing that PFMT plus ES significantly improved the therapeutic effects in postpartum women compared to those undergoing PFMT alone (RR: 1.28, 95% CI: 1.16–1.41, P < 0.00001, I2 = 0%; Fig. 3b).
Pelvic floor muscle strength
Only one eligible study [32] assessed pelvic floor muscle strength using the PHENIX USB2 Pelvic Floor Rehabilitation Therapeutic Apparatus, and a significant difference was reported between the two groups (RR: 2.11, 95% CI: 1.33–3.35, P = 0.001), with stronger pelvic floor muscle strength observed in the PFMT plus ES group, although the CIs were very wide.
One-hour pad test
Only one eligible study [31] reported the 1-h urine leakage; a significant difference was observed between the two groups (RR: −0.76, 95% CI: −1.30 to −0.22, P = 0.006). Thus, compared with PFMT alone, PFMT combined with ES significantly reduced the amount of urine leakage.
Incontinence quality of life scores
Only one eligible study [31] presented an estimate that precisely demonstrated superior results in the PFMT plus ES group, with higher scores on the I-QoL scale observed in the PFMT plus ES group.
Urodynamic parameters
Only one study [32] involving 150 patients reported on urodynamic parameters, including MUCP, Qmax, and voiding time (VT). The result showed that the PFMT plus ES group had significantly improved parameters (MUCP and Qmax) and reduced VT compared to the control group.
Adverse effects
Among the 17 included studies, only 2 RCTs [25, 29] reported adverse effects. Huang et al. [25] reported that two patients in the experimental group and three patients in the control group experienced slight discomfort on probe insertion, without other obvious discomfort or adverse events, such as vaginal infections. Lin [29] reported that one patient in the experimental group had urinary tract infections, whereas in the control group four patients experienced urinary retention, three patients experienced dysuria during puerperium, and one patient developed urinary tract infections.
Publication bias
The publication bias was analyzed using a Review Manager 5.4 funnel plot for the total therapeutic effects of PFMT combined with BF and ES in a total of 14 studies [16, 17, 19,20,21,22,23,24,25,26,27,28,29,30]. The two sides of the funnel plot were relatively asymmetric; thus, it was thought that there was a publication bias in this study (Fig. 8). Indeed, it is easier to publish research in China that exhibits statistical significance than to publish research without statistical significance.

Funnel plot of the publication bias
Discussion
In the present systematic review, PFMT plus ES with or without BF was shown to have a significant therapeutic effect, enhance pelvic floor muscle strength, and improve the storage and voiding LUTS. These findings agree with the results obtained in the clinical trials conducted by Lee et al. [35]. After 6 weeks of PFMT combined with BF and ES therapy, the subjective LUTS in postpartum women improved significantly compared with the control group (PFMT alone). Since no eligible study was retrieved, the specific effect of PFMT combined with BF is still uncertain.
Our meta-analysis revealed that compared to the control group, the number of women with pelvic floor muscle strength > grade III in the experimental group significantly increased after treatment. The results favored the use of PFMT plus ES with or without BF therapy in pelvic floor muscle strength evaluation. After sensitivity analysis by eliminating the study by Zhang et al. [23], heterogeneity was significantly reduced. We have identified the differences among studies according to the type of PUI. We also performed subgroup analysis based on the delivery mode, follow-up duration, and evaluation methods used to assess the pelvic floor muscle function. The heterogeneity was significantly reduced after subgroup analysis according to the evaluation methods. We believe this finding may be because pelvic floor muscle strength test using digital palpation is somewhat subjective, and the results depend on the experience of the evaluators.
Notably, a previous systematic review [36] demonstrated that compared with alternative interventions, such as no training, PFMT, PFMT with a vaginal cone, ES, at-home PFMT exercises, physical therapy, PFMT with BF, and electromyographic abdominal muscle training, PFMT plus BF for women with SUI was not superior in terms of muscle strength measured using a perineometer. The pooled analysis demonstrated that the use of PFMT with BF did not offer a clear advantage in terms of improvement in muscle strength. This discrepancy in results may be related to the differences in inclusion criteria; specifically, the experimental group included in the review [36] underwent PFMT plus BF without ES and the participants were not postpartum women. In the current review, PFMT alone was used as a control, but Nunes et al. [36] pooled the alternative interventions as control studies, accounting for the difference in results. Combined with the current meta-analysis, it is possible that the main clinical benefit of ES is concerned with improvement in the perception of pelvic floor muscle contraction. One study [37] supported our hypothesis. Yang et al. [37] evaluated the efficacy of rehabilitation exercises combined with direct vagina low voltage electric stimulation (DES) on pelvic floor nerve electrophysiology and tissue function in primipara. The results revealed that rehabilitation exercise combined with DES was beneficial to the recovery of pelvic floor nerve tissue function, and types I and II muscle fiber strength were significantly strengthened. The efficacy of BF as an adjunct to PFMT for postpartum LUTS, however, remains uncertain, and further large-scale, well-designed RCTs on PFMT with BF in treating postpartum LUTS or improving pelvic floor muscle strength are clearly needed.
The theoretical basis for treatment of pelvic floor muscle dysfunction is to improve pelvic floor support structure, prolong the muscle activation time, and strengthen pre-contraction to prevent or reduce urinary leakage [38]. The forest plot of the 1-h pad test showed that urine leakage was significantly reduced after PFMT plus BF and ES. After subgroup analysis according to the intervention time (< 8 weeks and ≥ 8 weeks), the heterogeneity was significantly reduced and there was no accompanying heterogeneity in the two subgroups. Compared with the subgroup with intervention time < 8 weeks (SMD: −0.16, 95% CI: −0.31 to −0.02, P = 0.03), the subgroup with intervention time ≥ 8 weeks (SMD: −1.12, 95% CI: −1.35 to −0.88, P < 0.00001) provided more reason to conclude that the urine leakage between the two groups was different. Therefore, the present meta-analysis suggested that postpartum pelvic floor muscle rehabilitation should last ≥ 8 weeks. This result was largely consistent with the previous meta-analysis [4], suggesting that the postpartum PFMT protocol should follow the general strength-training principles and emphasize close to maximum contractions training for at least 8 weeks. Furthermore, a systematic review published in 2019 [39] recommended that the PFMT program should last 6–12 weeks, with > 3 sessions/week and a session length of < 45 min.
Urodynamic parameters are related to the measurement of voiding function and can reflect the integrity of intrinsic sphincter function. Our review only included two studies comparing PFMT plus BF and ES with PFMT alone and one study comparing PFMT plus ES with PFMT alone to analyze and evaluate MUCP, ALPP, and Qmax. After PFMT plus ES with or without BF therapy, the MUCP, ALPP, and Qmax values were significantly improved, which revealed that the voiding function as well as the urethral intrinsic sphincter integrity may be improved. In addition, three studies involved the I-Qol scores of physiotherapy for postpartum LUTS, two [16, 27] involved PFMT plus BF and ES, and the remaining study [31] involved PFMT plus ES. The result showed that PFMT plus ES with or without BF significantly improved the quality of life of postpartum women with LUTS, which is an important determinant of mental, physical, and social functioning.
In terms of safety, the most commonly reported adverse effects were probe-related discomfort or urinary tract infection. Two studies [25, 29] in our meta-analysis reported adverse events. Compared to the control group, the PFMT combined with BF and ES group showed significantly reduced incidence of adverse events, such as urinary retention and dysuria during puerperium, and probe-related discomfort was rare. As a result, PFMT combined with BF and ES was shown to be relatively safe.
Despite these advances, there were some limitations in our meta-analysis. First, the quality of the included literature was low, as most studies did not describe the method of allocation, concealment, and blinding, which led to the unavoidable bias in selection, implementation, and measurement, and interfered with the results. Second, the treatment protocol varied among the included studies regarding frequency and duration, which might lead to methodological heterogeneity. Third, there was a lack of evidence about the long-term efficacy of physiotherapy on postpartum LUTS. Few studies had a follow-up period > 12 months. Therefore, more RCTs are needed with follow-up extending > 12 months to determine the long-term effect of physiotherapy on postpartum LUTS. Moreover, the efficacy of physiotherapy in the treatment of postpartum LUTS mainly focused on one symptom, such as PUI or PUR, whereas the types of LUTS are diverse. The specific application efficacy of PFMT combined with BF, ES, or both for other LUTS warrants further verification and evaluation. Recently, no comparative studies on PFMT plus BF for postpartum LUTS have been retrieved. The efficacy of BF as an adjunct to PFMT therefore remains uncertain. Hence, further multicenter RCTs involving large cohorts should be conducted to verify our conclusion and confirm the efficacy of BF.
Conclusions
Based on the current evidence, PFMT plus ES with or without BF is a safe and effective method to relieve early postpartum LUTS; specifically, the storage and voiding symptoms of postpartum women were improved significantly. We conclude that postpartum training should last ≥ 8 weeks. However, more high-quality and adequately powered RCTs are required to verify the efficacy of PFMT combined with BF for postpartum LUTS as well as the optimal initiation time, duration of intervention, and appropriate intervention plan.
Abbreviations
- LUTS:
-
Lower urinary tract symptoms
- SUI:
-
Stress urinary incontinence
- PUI:
-
Postpartum urinary incontinence
- PFMT:
-
Pelvic floor muscle training
- BF:
-
Biofeedback
- ES:
-
Electrical stimulation
- RCT:
-
Randomized controlled trail
- I-QoL:
-
Incontinence quality of life scores
- ALPP:
-
Abdominal leak point pressure
- MUCP:
-
Maximum urethral closure pressure
- CI:
-
Confidence interval
- RR:
-
Risk ratio
- MD:
-
Mean difference
- SMD:
-
Standardized mean difference
References
Haylen BT, de Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010;21(1):5–26. https://doi.org/10.1007/s00192-009-0976-9.
Zhang L. Epidemiological investigation and follow-up study on lower urinary tract symptoms in Chinese adult women—multicenter cross-sectional and prospective cohort study. Doctor, Peking union medical college (2015)
Li Z, Xu T, Li Z, Gong J, Liu Q, Zhu L. Lower urinary tract symptoms 7 years after the first delivery: correlation to the mode of delivery. Neurourol Urodyn. 2019;38(2):793–800. https://doi.org/10.1002/nau.23922.
Mørkved S, Bø K. Effect of pelvic floor muscle training during pregnancy and after childbirth on prevention and treatment of urinary incontinence: a systematic review. Br J Sports Med. 2014;48(4):299–310. https://doi.org/10.1136/bjsports-2012-091758.
Deffieux X, Vieillefosse S, Billecocq S, Battut A, Nizard J, Coulm B, et al. Rééducation périnéale et abdominale dans le post-partum: recommandations [Postpartum pelvic floor muscle training and abdominal rehabilitation: Guidelines]. J Gynecol Obstet Biol Reprod (Paris). 2015;44(10):1141–6. French. https://doi.org/10.1016/j.jgyn.2015.09.023.
Kegel AH. Physiologic therapy for urinary stress incontinence. J Am Med Assoc. 1951;146(10):915–7. https://doi.org/10.1001/jama.1951.03670100035008.
Veldman MP, Gondin J, Place N, Maffiuletti NA. Effects of neuromuscular electrical stimulation training on endurance performance. Front Physiol. 2016;7:544. https://doi.org/10.3389/fphys.2016.00544.
Lu J, Zhang H, Liu L, Jin W, Gao J, Min M, et al. Meta-analysis of perinatal pelvic floor muscle training on urinary incontinence. West J Nurs Res. 2021;43(6):597–605. https://doi.org/10.1177/0193945920960779.
Woodley SJ, Lawrenson P, Boyle R, Cody JD, Mørkved S, Kernohan A, et al. Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst Rev. 2020;5(5):CD007471. https://doi.org/10.1002/14651858.CD007471.pub4.
Wu YM, McInnes N, Leong Y. Pelvic floor muscle training versus watchful waiting and pelvic floor disorders in postpartum women: a systematic review and meta-analysis. Female Pelvic Med Reconstr Surg. 2018;24(2):142–9. https://doi.org/10.1097/SPV.0000000000000513.
Davenport MH, Nagpal TS, Mottola MF, Skow RJ, Riske L, Poitras VJ, et al. Prenatal exercise (including but not limited to pelvic floor muscle training) and urinary incontinence during and following pregnancy: a systematic review and meta-analysis. Br J Sports Med. 2018;52(21):1397–404. https://doi.org/10.1136/bjsports-2018-099780.
Urogynocology Subgroup, Chinese Society of Obstetrics and Gynocology, Chinese Medical Association. Update of guideline on the diagnosis and treatment of female stress urinary incontinence (2017). Zhonghua Fu Chan Ke Za Zhi. 2017;52(5):289–93. Chinese. https://doi.org/10.3760/cma.j.issn.0529-567X.2017.05.001.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. https://doi.org/10.1136/bmj.b2700.
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. https://doi.org/10.1136/bmj.d5928.
Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol. 2005;58(9):882–93. https://doi.org/10.1016/j.jclinepi.2005.01.016.
Liu X, Huang W, Kuang H, Qiu J. Electrical stimulation biofeedback therapy for female postpartum stress urinary incontinence. Shenzhen J Integr Tradit Chin West Med. 2020;30(06):131–3.
Jin Y. Efficacy analysis of EMG biofeedback electrical stimulation + Kegel training in the treatment of postpartum stress urinary incontinence. Mod Diagn Treat. 2020;31(11):1794–6.
Zou L, Gao L. Effect of biofeedback instrument combined with pelvic floor muscle functional exercise on postpartum stress urinary incontinence patients. J Qilu Nurs. 2020;26(18):52–4.
Sun J, Zhang H, Chen M. Clinical efficacy analysis of biofeedback electrical stimulation and pelvic floor muscle training on postpartum stress urinary incontinence. Shenzhen J Integr Tradit Chin West Med. 2017;27(03):121–2.
Gu S, Xu Y, Zhao M. Effect of biofeedback electrical stimulation combined with pelvic floor functional training on postpartum stress urinary incontinence in primiparas. Med J Chin People Health. 2020;32(10):74–6.
Sun L, Shen M, Chen D, Wang S, Du N. Effect of biofeedback electrical stimulation combined with pelvic floor muscle exercise on patients with early postpartum stress urinary incontinence. Anhui Med J. 2017;38(01):81–3.
Zeng W, Zhu F. The application comparison of biofeedback electrical stimulation combined with pelvic floor exercise and simple pelvic floor exercise in patients with early postpartum stress urinary incontinence. Clin Med Eng. 2018;25(06):707–8.
Zhang J, Xiao L, Luo X, He Y. Effect of biofeedback electrical stimulation combined with pelvic floor muscle exercises assisted functional rehabilitation of pelvic floor Musclesin female urinary incontinence postpartum. Med Innova China. 2016;13(18):96–8 Chinese.
Liu J, Li D, He Y, Cui W, Zhao L. Observation on the effect of biofeedback electrical stimulation combined with pelvic floor muscle training on postpartum stress urinary incontinence. Chin Commun Dr. 2020;36(05):44–5.
Huang L, Gu Y, Fang G, Zhang H, Wang P, Liu X. Effects of biofeedback electrical stimulation combined with pelvic floor muscle training on postpartum stress urinary incontinence. J Hebei Med Univ. 2017;38(05):557–60.
Gao R. Effect of biofeedback pelvic floor electrical stimulation combined with pelvic floor muscle training on postpartum stress urinary incontinence. Henan J Surg. 2020;26(04):137–8.
Ge J, Ye H, Pu W, Wang Y, Tan L, Feng D, et al. Study on the effect of rehabilitation training combined with biofeedback and electrical stimulation in postpartum stress urinary incontinence. Chin J Clin Obstet Gynecol. 2019;20(01):59–60.
Yang F, Li Z. Effect of electrical stimulation biofeedback combined with PFMT nursing intervention on urinary incontinence in patients with postpartum urinary retention. Mod J Integr Trad Chin West Med. 2017;26(35):3980–3981+3990.
Lin L. Effect analysis of electrical stimulation biofeedback combined with pelvic floor muscle functional exercise nursing intervention on urinary incontinence in patients with postpartum urinary retention. Cap Food Med. 2019;26(09):86–7.
Deng C, Miao Q, Zhong Y, Chen H. Application of pelvic floor electromyography stimulation combined with biofeedback in postpartum women with urinary incontinence. Nurs Pract Res. 2017;14(08):77–8.
Du B, Yu X, Ma Y. Effect of electrical stimulation combined with pelvic floor muscle exercise on postpartum stress urinary incontinence in primipara. Matern Child Health Care Chin. 2020;35(22):4241–3.
He Y. The efficacy of pelvic floor rehabilitation combined with low-frequency electrical stimulation in the treatment of postpartum stress urinary incontinence. J Hubei Univ Sci Technol (Med Sci). 2019;33(04):320–3.
Caroci Ade S, Riesco ML, Sousa Wda S, Cotrim AC, Sena EM, Rocha NL, et al. Analysis of pelvic floor musculature function during pregnancy and postpartum: a cohort study: (a prospective cohort study to assess the PFMS by perineometry and digital vaginal palpation during pregnancy and following vaginal or caesarean childbirth). J Clin Nurs. 2010;19(17–18):2424–33. https://doi.org/10.1111/j.1365-2702.2010.03289.x.
Patrick DL, Martin ML, Bushnell DM, Yalcin I, Wagner TH, Buesching DP. Quality of life of women with urinary incontinence: further development of the incontinence quality of life instrument (I-QOL). Urology. 1999;53(1):71–6. https://doi.org/10.1016/s0090-4295(98)00454-3.
Lee IS, Choi ES. Pelvic floor muscle exercise by biofeedback and electrical stimulation to reinforce the pelvic floor muscle after normal delivery. Taehan Kanho Hakhoe Chi. 2006;36(8):1374–80. https://doi.org/10.4040/jkan.2006.36.8.1374.
Nunes EFC, Sampaio LMM, Biasotto-Gonzalez DA, Nagano RCDR, Lucareli PRG, Politti F. Biofeedback for pelvic floor muscle training in women with stress urinary incontinence: a systematic review with meta-analysis. Physiotherapy. 2019;105(1):10–23. https://doi.org/10.1016/j.physio.2018.07.012.
Yang S, Sang W, Feng J, Zhao H, Li X, Li P, et al. The effect of rehabilitation exercises combined with direct vagina low voltage low frequency electric stimulation on pelvic nerve electrophysiology and tissue function in primiparous women: a randomised controlled trial. J Clin Nurs. 2017;26(23–24):4537–47. https://doi.org/10.1111/jocn.13790.
Miller JM, Ashton-Miller JA, DeLancey JO. A pelvic muscle precontraction can reduce cough-related urine loss in selected women with mild SUI. J Am Geriatr Soc. 1998;46(7):870–4. https://doi.org/10.1111/j.1532-5415.1998.tb02721.x.
García-Sánchez E, Ávila-Gandía V, López-Román J, Martínez-Rodríguez A, Rubio-Arias JÁ. What pelvic floor muscle training load is optimal in minimizing urine loss in women with stress urinary incontinence? A systematic review and meta-analysis. Int J Environ Res Public Health. 2019;16(22):4358. https://doi.org/10.3390/ijerph16224358.
Acknowledgments
We thank all the authors who responded to us and those who provided their study data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhu, D., Xia, Z. & Yang, Z. Effectiveness of physiotherapy for lower urinary tract symptoms in postpartum women: systematic review and meta-analysis. Int Urogynecol J 33, 507–521 (2022). https://doi.org/10.1007/s00192-021-04939-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-021-04939-z