
Abstract
Introduction and hypothesis
Connective tissue disorders may contribute to pelvic floor disorders (PFDs). Like PFDs, abdominal wall hernias are more common in patients with systemic connective tissue disorders. We conducted this study to explore the possible association between PFDs and hernias in adult women.
Methods
We obtained the data for this study from a study of PFDs among parous women. At enrollment, stress urinary incontinence (SUI), overactive bladder (OAB), and anal incontinence (AI) were assessed using the Epidemiology of Prolapse and Incontinence Questionnaire (EPIQ) and pelvic organ prolapse (POP) was assessed through the Pelvic Organ Prolapse Quantification (POP-Q) examination. Participants were asked to report hernia surgery and list their hernia types. We compared the prevalence of PFDs in those with and without hernias using chi-square test. We used multiple regression analysis to adjust for obstetric and sociodemographic variables.
Results
Among 1529 women, 79 (5.2%) reported history of hernia surgery. The prevalence of POP was 7.6% (6 cases) vs. 7.4% (107 cases), the prevalence of SUI was 7.6% (6 cases) vs. 9.9% (144 cases), the prevalence of OAB was 7.6% (6 cases) vs. 5.7% (83 cases), and the prevalence of AI was 7.6% (6 cases) vs. 10.8% (156 cases) in those with hernias compared to those without hernias, respectively. None of these differences were statistically significant. There was no association between hernias and PFDs after adjustment for type of delivery, number of deliveries, age group, primary racial background, weight category, and smoking status.
Conclusion
In this study, we could not find any association between hernias and PFDs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pelvic floor disorders (PFDs) are very common in the US and worldwide [1]. They include bladder control problems such as stress urinary incontinence (SUI) and overactive bladder (OAB), anal incontinence (AI), and pelvic organ prolapse (POP). A large cross-sectional study has found about a quarter of all women and a third of older women in the US in 2005–2006 had at least one PFD [1]. PFDs significantly affect a woman’s qualify of life [2, 3], and they have substantial surgical and ambulatory costs [4, 5]. Another large study in the US has found a 20% lifetime risk of undergoing a surgery for SUI or POP by the age of 80 years [6]. It is estimated that the number of women in the US with at least one PFD will increase by 55% in 2050 compared to 2010 [7]. Delivery mode [8], parity, age, body mass index (BMI) [9], race [10], and genetics [11] are some known risk factors for PFDs. Connective tissue disorders are suggested as an etiology for PFDs, such as SUI [12], AI [13], and POP [14]. The role of connective tissue disorders in the pathophysiology of PFDs is supported by studies that observed a higher prevalence of PFDs in patients with systemic connective tissue disorders [15, 16] and studies that observed changes in collagen content and activity in patients with PFDs [17].
Undergoing a surgery to repair groin (inguinal and femoral) or abdominal wall (umbilical and epigastric) hernias is a very common surgical procedure in western countries [18, 19], and an incisional hernia is a common complication of a laparotomy [20]. Male gender, conditions and activities that increase intra-abdominal pressure such as chronic cough or type of work, age, lower BMI, race, genetics, and smoking have been described as risk factors for developing hernias [21,22,23,24]. Unlike PFDs, no association has been observed between multiple deliveries and inguinal hernias in women [25]. However, like PFDs, hernias are more common in patients with systemic connective tissue disorders [26], and connective tissue alterations are present in patients with hernias [27, 28]. Several studies have pointed out a commonality between the etiology of hernias and PFDs [29].
We hypothesized PFDs and hernias may be associated because of a common etiology. We performed this study using the data obtained from the Mothers’ Outcomes After Delivery (MOAD) cohort study to explore the possible association between PFDs and hernias in adult women.
Methods
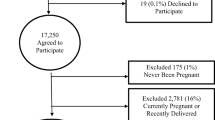
This study was a secondary data analysis using data from the MOAD cohort study. The MOAD study was designed and conducted by researchers from the Johns Hopkins University and the Greater Baltimore Medical Center, and it was approved by the institutional review boards at both institutions. Parous women, 5 to 10 years after their first delivery, were recruited from October 2008 to December 2013 and followed up annually until April 2017 [8]. Women who had delivered their first child at Greater Baltimore Medical Center 5 to 10 years before enrollment were eligible for that study. Participants were identified using hospital discharge diagnoses, and eligibility was verified by reviewing hospital charts and telephone interview. Exclusion criteria, applied to the index birth, included maternal age < 15 or > 50 years at the time of the delivery, delivery at < 37 weeks of gestation, placenta previa, multiple gestation, known fetal congenital anomaly, stillbirth, prior myomectomy, and abruption. Each eligible delivery was classified as a vaginal delivery, unlabored cesarean delivery (performed prior to the onset of active labor, defined as regular contractions with cervical dilation ≥ 3 cm), or labored cesarean delivery. Each eligible delivery was also classified by the participant’s age at delivery (organized into 5-year strata) and the number of years from first delivery to recruitment (organized into ¼-year strata). The recruitment strategy was designed to match participants across the three birth groups for age at first delivery and years since first delivery. Eligible participants within each stratum were randomly selected for recruitment until the sample size was obtained [30]. Specifically, the study team contacted 4124 women who were selected for this study; 52 of those were found to be ineligible. Among the 4072 who were contacted and eligible, 1529 enrolled.
PFDs, including SUI, OAB, AI, and POP, were assessed at study enrollment. The self-administered Epidemiology of Prolapse and Incontinence Questionnaire (EPIQ) was used to detect SUI, OAB, and AI. The EPIQ generates a score for each of these disorders, where higher scores represent greater bother. Participants with scores above the previously validated thresholds for SUI, OAB, and AI were considered to have the disorder [31]. A gynecologic examination at the enrollment visit was performed to detect POP. The gynecologic examination was performed by physicians and a research nurse using the Pelvic Organ Prolapse Quantification (POP-Q) system [32]. Those who performed the gynecologic examination were not aware of the questionnaire results. Participants with descent of the most dependent point of the vaginal walls or the cervix to or beyond the hymen during the Valsalva maneuver were considered to have POP. History of hernia surgery and type of hernia were self-reported using a questionnaire.
We also included other obstetric and sociodemographic variables in our analysis. Participants were categorized into six groups based on type of their delivery: unlabored cesarean delivery, labored cesarean delivery without full cervical dilation, labored cesarean delivery with full cervical dilation, spontaneous vaginal delivery, vaginal delivery with the use of forceps, and vacuum-assisted vaginal delivery. It is hypothesized the harm to the pelvic floor increases across these groups [30], and women with multiple deliveries were placed into a group based on the delivery that was potentially the most harmful to the pelvic floor (e.g., participants with an unlabored cesarean delivery and a spontaneous vaginal delivery were placed into the spontaneous vaginal delivery group). Parity was categorized into three groups: one, two, and three or more. Participants’ age at recruitment was categorized into these tertiles: < 36.31 years, 36.31–41.04 years, and ≥ 41.04 years. Primary racial background was categorized as: white, African American, Asian, and other. BMI was calculated using the height and the weight measured at the enrollment visit, and participants were categorized into three weight categories, based on their BMI: < 25 kg/m2 (underweight or normal), 25–29.9 kg/m2 (overweight), and ≥ 30 kg/m2 (obese). Cigarette smoking status was categorized as never or ever, based on whether the participant reported smoking at least 100 cigarettes in her life.
We used the chi-square test to compare binary and categorical variables across groups, and we used logistic regression to estimate odds ratios. We adjusted for potential confounders using multiple logistic regression. P values < 0.05 and 95% confidence intervals not containing the null value of 1 were defined as statistically significant. All statistical analyses were performed using Stata version 15 [33].
Results
Among 1529 participants in the MOAD study, 79 (5.2%) reported history of hernia surgery. This included 25 (32%) inguinal or femoral hernias, 34 (43%) umbilical hernias, 12 (15%) incisional or ventral hernias, and 8 (10%) who did not remember their type of hernia or had other types of hernias.
The EPIQ score for SI, OAB, and AI was above the threshold in 150 (9.8%), 89 (5.8%), and 163 (10.7%) participants, respectively, and 113 (7.4%) participants were identified to have POP in gynecologic examination. Some women had more than one PFD. Specifically, of those without history of hernia surgery, 250 (17.21%) had one PFD, 74 (5.09%) had two PFDs, 28 (1.93%) had three PFDs, and 2 (0.14%) had four PFDs. Of those with history of hernia surgery, 13 (16.46%) had one PFD, 4 (5.06%) had two PFDs, and 1 (1.27%) had three PFDs. The study population characteristics and the distribution of SI, OAB, and AI among participants with and without history of hernia surgery are described in Table 1. No differences were seen between women with and without a history of hernia surgery except for BMI (p value = 0.046).
The relative odds for each PFD associated with history of hernia surgery are presented in Table 2. Estimates from univariable and multivariable models are presented. We did not find a statistical difference in the odds of any PFD among those with history of hernia surgery compared to those without such history. Odds ratios remained non-significant after adjusting for type of delivery, number of deliveries, age group, primary racial background, weight category, and smoking status.
Given that these data suggest no significant associations between hernia surgery and any of the PFDs considered, post hoc power calculations were performed, using the observed proportions of SI, OAB, AI, and POP in the non-hernia group of 9.9%, 5.7%, 10.8%, and 7.4%, respectively. Assuming these proportions and the observed sample sizes, this study would have had 80% power a priori to detect an absolute difference of 10.8%, 8.8%, 11.1%, and 9.7% in the proportion of SI, OAB, AI, and POP between the non-hernia and hernia groups, respectively. However, when incorporating the observed proportion of 7.6% for each of the PFD types (SI, OAB, AI, and POP) in the hernia group, the post hoc calculated power ranged from 5% to 17% across the four PFD types.
Discussion
In this study, the results did not confirm our hypothesis. We did not find any association between hernias and any of the PFDs considered, including POP, SI, OAB, and AI. This finding did not change after adjustment for type of delivery, number of deliveries, age group, primary racial background, weight category, and smoking status.
In contrast to our results, prior studies have suggested a possible association. In a case-control study on 114 Turkish women who underwent a surgery for different types of abdominal wall hernias and 100 age-matched women (mean age 50 years), researchers found an increased odds of SUI in those with history of hernia surgery [34]. Using the Bristol Female Lower Urinary Tract Symptoms Questionnaire to assess incontinence symptoms, they found that 41.4% in the hernia group complained of SUI at least weekly versus 19.7% among those without a hernia. Statistical significance persisted after adjustment for BMI and gravity. In a retrospective case-control study on 60 Israeli women who underwent a surgery for POP (mean age 63.6 years) and 60 age-matched controls (mean age 58 years), researchers found a higher prevalence of prior surgery for inguinal hernia in those with POP (15% versus 3%) [35]. The observed association remained statistically significant after controlling for BMI and parity. In addition, in a cross-sectional study on 1380 women, researchers reported an increased odds of previous hernia surgery among those who also underwent a surgery for POP and/or incontinence surgery [36]. This study included women aged 45–85 years. Previous hernia surgery was reported by 14/119 (12%) of those who also reported a history of surgery for SUI or POP compared to 83/1261 (6.7%) of those without a history of surgery for SUI or POP. Their study population was comprised of mainly Caucasian women, and the odds ratio was adjusted for age group, BMI group, and POP symptoms during pregnancy. In the present study on 1534 women of multiple races and with different obstetric histories, we did not find such associations after adjusting for type of delivery and other potential confounders.
The present study has several strengths, including a relatively large sample size, inclusion of different races, and use of validated measures for PDFs. We used a validated symptom questionnaire (EPIQ) and a structured examination to assess PFDs. Another strength of this study is that obstetric risk factors were extracted from hospital records rather than from self-reported questionnaires.
Weaknesses of the present study include our definition of hernia, narrow age range of participants, and low statistical power based on the available sample size. With respect to the definition of hernia, we only considered those participants who reported a history of hernia surgery as having hernias; however, there may be other participants with hernias who did not seek treatment or participants who were unaware of having a hernia. Earlier studies on this issue also either used history of previous hernia surgery [34, 36] or did not explain their diagnostic criteria [35]. Future research in this area would be advanced by a valid hernia assessment that could be implemented in clinical research. With respect to the age of our population, the peak incidence of hernia surgery in US women is after 65 years [37]. In contrast, women in this study were younger than 57 years. Therefore, our results are most relevant to women who develop a hernia at a young age. On one hand, this could limit the generalizability of our findings to older populations. Alternatively, we speculate that an association between hernia and PFD would be strongest in young women because women susceptible to both because of underlying connective tissue characteristics would have onset of these conditions at a young age.
Despite potentially having a common etiology at the molecular or histologic level, the results of our study do not support that hernias and PFDs are likely to occur concurrently. This may indicate the higher importance of environmental risk factors specific to these conditions (e.g., obstetrics risk factors for PFDs or occupational risk factors for hernias) compared to genetic predisposition.
References
Nygaard I, Barber MD, Burgio KL, Kenton K, Meikle S, Schaffer J, et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008;300(11):1311–6. https://doi.org/10.1001/jama.300.11.1311.
Jelovsek JE, Barber MD. Women seeking treatment for advanced pelvic organ prolapse have decreased body image and quality of life. Am J Obstet Gynecol. 2006;194(5):1455–61. https://doi.org/10.1016/j.ajog.2006.01.060.
Kwon BE, Kim GY, Son YJ, Roh YS, You MA. Quality of life of women with urinary incontinence: a systematic literature review. Int Neurourol J. 2010;14(3):133–8. https://doi.org/10.5213/inj.2010.14.3.133.
Subak LL, Waetjen LE, van den Eeden S, Thom DH, Vittinghoff E, Brown JS. Cost of pelvic organ prolapse surgery in the United States. Obstet Gynecol. 2001;98(4):646–651. https://doi.org/10.1016/S0029-7844(01)01472-7.
Sung VW, Washington B, Raker CA. Costs of ambulatory care related to female pelvic floor disorders in the United States. Am J Obstet Gynecol. 2010;202(5):483.e481–4. https://doi.org/10.1016/j.ajog.2010.01.015.
Wu JM, Matthews CA, Conover MM, Pate V, Jonsson Funk M. Lifetime risk of stress urinary incontinence or pelvic organ prolapse surgery. Obstet Gynecol. 2014;123(6):1201–6. https://doi.org/10.1097/aog.0000000000000286.
Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in U.S. women: 2010 to 2050. Obstet Gynecol. 2009;114(6):1278–83. https://doi.org/10.1097/AOG.0b013e3181c2ce96.
Blomquist JL, Muñoz A, Carroll M, Handa VL. Association of Delivery Mode with Pelvic Floor Disorders after Childbirth. JAMA. 2018;320(23):2438–47. https://doi.org/10.1001/jama.2018.18315.
Vergeldt TFM, Weemhoff M, IntHout J, Kluivers KB. Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecol J. 2015;26(11):1559–73. https://doi.org/10.1007/s00192-015-2695-8.
Graham CA, Mallett VT. Race as a predictor of urinary incontinence and pelvic organ prolapse. Am J Obstet Gynecol. 2001;185(1):116–20. https://doi.org/10.1067/mob.2001.114914.
Lince SL, van Kempen LC, Vierhout ME, Kluivers KB. A systematic review of clinical studies on hereditary factors in pelvic organ prolapse. Int Urogynecol J. 2012;23(10):1327–1336. https://doi.org/10.1007/s00192-012-1704-4.
Ulmsten U, Falconer C. Connective tissue in female urinary incontinence. Curr Opin Obstet Gynecol. 1999;11(5):509–15. https://doi.org/10.1097/00001703-199910000-00017.
Wang JY, Abbas MA. Current management of fecal incontinence. Perm J. 2013;17(3):65–73. https://doi.org/10.7812/tpp/12-064.
Schaffer JI, Wai CY, Boreham MK. Etiology of pelvic organ prolapse. Clin Obstet Gynecol. 2005;48(3):639–47. https://doi.org/10.1097/01.grf.0000170428.45819.4e.
Carley ME, Schaffer J. Urinary incontinence and pelvic organ prolapse in women with Marfan or Ehlers Danlos syndrome. Am J Obstet Gynecol. 2000;182(5):1021–3. https://doi.org/10.1067/mob.2000.105410.
Lammers K, Lince SL, Spath MA, van Kempen LCLT, Hendriks JCM, Vierhout ME, Kluivers KB. Pelvic organ prolapse and collagen-associated disorders. Int Urogynecol J. 2012;23(3):313–319. https://doi.org/10.1007/s00192-011-1532-y.
Jackson SR, Avery NC, Tarlton JF, Eckford SD, Abrams P, Bailey AJ. Changes in metabolism of collagen in genitourinary prolapse. Lancet. 1996;347(9016):1658–61. https://doi.org/10.1016/s0140-6736(96)91489-0.
Burcharth J, Pedersen M, Bisgaard T, Pedersen C, Rosenberg J. Nationwide prevalence of groin hernia repair. PLoS One. 2013;8(1):e54367. https://doi.org/10.1371/journal.pone.0054367.
Burcharth J, Pedersen MS, Pommergaard HC, Bisgaard T, Pedersen CB, Rosenberg J. The prevalence of umbilical and epigastric hernia repair: a nationwide epidemiologic study. Hernia. 2015;19(5):815–9. https://doi.org/10.1007/s10029-015-1376-3.
Le Huu Nho R, Mege D, Ouaïssi M, Sielezneff I, Sastre B. Incidence and prevention of ventral incisional hernia. J Visc Surg. 2012;149(5, Supplement):e3–e14. https://doi.org/10.1016/j.jviscsurg.2012.05.004.
Tue Sorensen L, Friis E, Jorgensen T, Vennits B, Ristorp Andersen B, Iben Rasmussen G, et al. Smoking is a risk factor for recurrence of groin hernia. World J Surg. 2002;26(4):397–400. https://doi.org/10.1007/s00268-001-0238-6.
Sørensen LT, Hemmingsen UB, Kirkeby LT, Kallehave F, Jørgensen LN. Smoking is a risk factor for incisional hernia. Arch Surg. 2005;140(2):119–23. https://doi.org/10.1001/archsurg.140.2.119.
Ruhl CE, Everhart JE. Risk factors for inguinal hernia among adults in the US population. Am J Epidemiol. 2007;165(10):1154–61. https://doi.org/10.1093/aje/kwm011.
Sazhin A, Zolotukhin I, Seliverstov E, Nikishkov A, Shevtsov Y, Andriyashkin A, et al. Prevalence and risk factors for abdominal wall hernia in the general Russian population. Hernia. 2019;23(6):1237–42. https://doi.org/10.1007/s10029-019-01971-3.
MSL L, van der Graaf Y, Zwart RC, Geurts I, TJMV v V, Group botCT. Risk factors for inguinal hernia in women: a case-control study. Am J Epidemiol. 1997;146(9):721–6. https://doi.org/10.1093/oxfordjournals.aje.a009347.
Liem MS, van der Graaf Y, Beemer FA, van Vroonhoven TJ. Increased risk for inguinal hernia in patients with Ehlers-Danlos syndrome. Surgery. 1997;122(1):114–115. https://doi.org/10.1016/s0039-6060(97)90273-7.
Fachinelli A, Trindade MRM, Fachinelli FA. Elastic fibers in the anterior abdominal wall. Hernia. 2011;15(4):409–15. https://doi.org/10.1007/s10029-011-0804-2.
Öberg S, Andresen K, Rosenberg J. Etiology of inguinal hernias: a comprehensive review. Front Surg. 2017;4(52). https://doi.org/10.3389/fsurg.2017.00052.
Read RC. Signs of herniosis in women with vaginal prolapse and/or stress incontinence. Hernia. 2008;12(5):449–52. https://doi.org/10.1007/s10029-008-0372-2.
Handa VL, Blomquist JL, Knoepp LR, Hoskey KA, McDermott KC, Muñoz A. Pelvic floor disorders 5-10 years after vaginal or cesarean childbirth. Obstet Gynecol. 2011;118(4):777–84. https://doi.org/10.1097/AOG.0b013e3182267f2f.
Lukacz ES, Lawrence JM, Buckwalter JG, Burchette RJ, Nager CW, Luber KM. Epidemiology of prolapse and incontinence questionnaire: validation of a new epidemiologic survey. Int Urogynecol J Pelvic Floor Dysfunct. 2005;16(4):272–84. https://doi.org/10.1007/s00192-005-1314-5.
Bump RC, Mattiasson A, Bø K, Brubaker LP, DeLancey JOL, Klarskov P, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol. 1996;175(1):10–7. https://doi.org/10.1016/S0002-9378(96)70243-0.
StataCorp. Stata Statistical Software. Release 15 edn. StataCorp LLC, College Station; 2017.
Tok EC, Ertunc D, Dilek U, Pata O, Erdogan O, Aydin S. The prevalence of stress urinary incontinence among women operated on for abdominal wall hernias. Acta Obstet Gynecol Scand. 2004;83(10):962–4. https://doi.org/10.1111/j.0001-6349.2004.00521.x.
Segev Y, Auslender R, Feiner B, Lissak A, Lavie O, Abramov Y. Are women with pelvic organ prolapse at a higher risk of developing hernias? Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(12):1451–3. https://doi.org/10.1007/s00192-009-0968-9.
de Boer TA, Slieker-ten Hove MCP, Burger CW, Kluivers KB, Vierhout ME. The prevalence and factors associated with previous surgery for pelvic organ prolapse and/or urinary incontinence in a cross-sectional study in the Netherlands. Eur J Obstet Gynecol Reprod Biol. 2011;158(2):343–9. https://doi.org/10.1016/j.ejogrb.2011.04.029.
Beadles CA, Meagher AD, Charles AG. Trends in emergent hernia repair in the United States. JAMA Surgery. 2015;150(3):194–200. https://doi.org/10.1001/jamasurg.2014.1242.
Acknowledgments
We greatly appreciate Prof. Marie Diener-West (Department of Biostatistics, Johns Hopkins University, Baltimore, MD, USA) for her help with the post hoc power analysis and for reviewing the manuscript.
Funding
This study was supported by funding from the National Institutes of Health, R01HD056275.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors claim no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tadbiri, H., Handa, V.L. Association between pelvic floor disorders and hernias. Int Urogynecol J 32, 3017–3022 (2021). https://doi.org/10.1007/s00192-021-04762-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-021-04762-6