
Abstract
Background
Data on the incidence of perioperative complications of surgical procedures for pelvic organ prolapse (POP) and their contributing factors are limited, sometimes conflicting, and often mixed with other urogynecologic surgeries.
Objectives
To estimate the incidence and contributing factors for perioperative complications of POP procedures.
Methods
A cross-sectional study was carried out between November 2016 and June 2017. POP procedures of different approaches were included irrespective of the surgeon involved, type of surgery (primary or repeat), or concomitant hysterectomy or incontinence repair. Data on perioperative complications were recorded prospectively.
Results
A total of 366 women were included in the current analysis. The average age was 61.0 ± 13.4 years. The surgical procedures performed were vaginal (75.3%), abdominal (11.3%), or combined (13.4%). Approximately 18.2% of these procedures were repeat surgeries. A total of 38 (11.3%) women developed perioperative complications (3.6% severe and 7.7% minor). These included: 25 (7.4%) intraoperative complications (2.4% severe and 5.1% minor) and 17 (5.1%) postoperative complications (2.1% severe and 3.0% minor). In multivariate analysis, abdominal surgery and McCall culdoplasty were significant predictors of intraoperative complications (alone or when combined with other postoperative complications). On the other hand, concomitant hysterectomy and concomitant incontinence repair procedure were associated with higher postoperative complication rates while vaginal surgery had fewer postoperative complications.
Conclusion
There was a low rate of perioperative complications. Abdominal surgery and McCall culdoplasty showed higher intraoperative complications. These data should help in preoperative counseling and target ways to further decrease complication rates.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pelvic organ prolapse (POP) is the most common form of pelvic floor dysfunction and refers to the drop of the pelvic organs, including the bladder, uterus, rectum, and/or small intestine, into or outside of the vagina [1]. Globally, it affects up to 30% of women over the age of 50 years [2,3,4]. Almost half of the women with symptomatic POP report moderate to great distress, which may significantly impact their physical, social, and sexual activities [5]. The development of POP has been linked to older age, obesity, multiple parity, and vaginal delivery [4, 6]. POP is one of the most common causes for gynecologic surgery with approximately 11–19% chance of undergoing at least one surgical procedure for POP or incontinence by the age of 85, in addition to a 30% reoperation rate [3, 7]. Each year, approximately 300,000 women require surgery for pelvic organ prolapse (POP) and stress urinary incontinence in the USA [8, 9]. As the current generation of women maintains a more active lifestyle into an older age, it is likely that an increasing number of women will seek treatment of POP. It has been projected that over the next 30 years, the rate of women seeking care for pelvic floor disorders will double [10].
The prevalence of perioperative complications associated with general gynecologic surgery has been reported to be between 0.2% and 26% [11,12,13]. In comparison with general benign gynecologic surgery, reconstructive operations for pelvic organ prolapse and urinary incontinence are generally longer, with more extensive dissection [14]. The prevalence of perioperative complications of urogynecologic surgeries mainly targeting POP and urinary incontinence has been estimated in a number studies, with the rates ranged between 26% and 46% [14,15,16]. The rate of perioperative complications of primary POP surgery without concomitant repair of urinary incontinence is lower, estimated at 3.2% at discharge and 15.5% at 8 weeks postoperatively, of which most are minor complications [17]. Interestingly, 3.1% of the surgical procedures for POP are followed by major postoperative complications including mortality, cardiovascular or cerebrovascular accidents, severe wound infection, wound dehiscence, mechanical ventilation, systemic infection morbidity, renal failure, blood transfusion, and reoperation [18]. Complications occur after native tissue repairs, but using synthetic materials and specially designed kits only adds to the new complication profile, e.g., injuries during passing the trocar and reaction of the body to the prosthesis (inflammation, infection, extrusion, rejection) [19].
Few studies examined potential risk factors for developing perioperative complications of urogynecologic procedures [14, 16]. Data examining such complications in different types of POP surgery are very limited [18]. The landscape of POP surgery has shifted away from using vaginal mesh, and thus there is a need to evaluate the incidence of complications in diverse POP surgeries. This will allow identification of risk factors with possible preoperative mitigation and allow comprehensive counseling prior to surgery.
Methods
Setting and population
The study was conducted at Foothills Medical Center (FMC), a tertiary care hospital in Alberta, Canada, serving a catchment area of 2.5 million population. The section of Pelvic Medicine and Reconstructive Surgery at FMC is served by five academic consultant urogynecologists who collectively operate on approximately 1000 patients every year. The target population included all inpatients who underwent pelvic reconstructive surgery for POP at FMC from November 2016 to June 2017. Surgical procedures of all approaches were included: abdominal (laparotomy or laparoscopy), vaginal (anterior, posterior, paravaginal, or apical compartment), and combined. There were no exclusions based on the surgeon involved, type of surgery (primary or repeat), use of mesh, or concomitant hysterectomy or incontinence repair. Patients who underwent outpatient surgeries (such as isolated incontinence surgeries and intravesicle botulinum toxin injections) or inpatient surgeries for non-POP reasons were excluded from the study.
Design
A cross-sectional design was used to allow for incidence estimation. The data were prospectively collected using a structured study data collection sheet. The variables collected included: demographics information, comorbidity, surgical history, surgical procedures performed, and intraoperative and postoperative complications. The study was approved by the Conjoint Health Research Ethics Board through the University of Calgary (REB17–0583).
Outcome definition
Both intraoperative and postoperative complications were examined, as per standard definitions [20]. Intraoperative complications included: injury to the bowel, bladder, ureter, or urethra as well as intraoperative bleeding that required blood or blood product transfusion. Postoperative complications included: (1) cardiac events (congestive heart failure, myocardial infarction, arrhythmias, and pulmonary edema), (2) respiratory events (pneumonia or use of a ventilator), (3) gastrointestinal events (paralytic ileus, small bowel obstruction, bowel injury), (4) venous thromboembolic events [deep venous thrombosis (DVT) or pulmonary embolism], (5) bleeding that required blood or blood product transfusion, (6) infections other than urinary tract infection or pneumonia (wound infection or pelvic abscess), (7) pelvic collection or hematoma, and (8) readmission due to surgical complications or for reoperation. Major or severe complications were defined as per the International Urogynecological Association (IUGA)/International Continence Society (ICS) joint terminology and classification of the complications and the Clavien-Dindo Classification System [17, 18, 21]. These included mortality, reoperation, organ lesions, severe wound infection, blood transfusion, cardiovascular accidents, mechanical ventilation, systemic infections morbidity, and renal failure. Prolonged hospital stay was defined as hospitalization for > 2 nights.
Statistical analysis
Categorical data were presented as frequencies and percentages, while continuous data were presented as mean and standard deviation (SD) or medians and interquartile ranges (IQR), as appropriate. Predictors (demographics, comorbidity, surgical history, and surgical procedures) of postoperative complications were tested using chi-square test or Fisher exact test (as appropriate) for categorical data and Student t-test or Mann-Whitney U-test (as appropriate) for continuous data. Independent associations between potential predictors and surgical complications (including perioperative, intraoperative, and postoperative complications) were evaluated using multivariate logistic regression models with stepwise backward elimination. Models were adjusted for all factors that showed significant associations (p < 0.05) or trend of associations (p < 0.10) in univariate analysis. p < 0.05 was considered significant. SPSS software (release 24.0, IBM Corp., Armonk, NY) was used for all statistical analyses.
Results
A total of 336 women who underwent POP procedures during the study period were included in the current analysis. Demographic and clinical characteristics are shown in Table 1. The average age was 61.0 ± 13.4 years, with 15.8% > 75 years old. The average body mass index (BMI) was 28.3 ± 5.6 years, with 32.7% being obese (≥ 30). More than half (57.1%) of the patients had undergone previous abdominal/pelvic surgery. Additionally, 22.6% of the patients had undergone previous POP surgery. Approximately 26.2% of the patients had comorbidity, including 4.2% who had multiple comorbid diseases.
Most surgeries were primary vaginal surgeries (Table 2). Close to half (47.9%) of the procedures involved concomitant hysterectomy, and 29.2% involved a concomitant incontinence repair procedure.
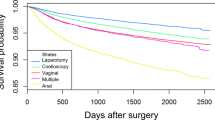
A total of 46 complications developed in 38 women who underwent surgery, with an overall complication rate of 11.3% (Fig. 1). Four patients (1.2%) developed both intraoperative and postoperative complications. Twelve patients (3.6%) had complications which were considered severe.

Incidence of complications developed in patients undergoing urogynecology surgeries (n = 336)
Table 3 shows the incidence of different types of complications and other study outcomes. Of 25 patients who developed intraoperative complications, 11 (3.3%) had ureteric obstruction, 5 (1.5%) had bladder perforation, 5 (1.5%) had intraoperative bleeding, and none had bowel injury. Ureteric obstruction was resolved with intraoperative ureteric catheterization (n = 6) or removal of the suspension sutures (n = 5). Bladder perforation was related to trocar insertion in the retropubic mid-urethral sling (n = 3) and the dissection done during abdominal hysterectomy (n = 1). In two patients, the intraoperative bleeding was secondary to significant vascular injury from the left common iliac vein during sacrocolpopexy and the internal pudendal artery during sacrospinous ligament suspension. Additionally, six (1.8%) patients had conversion of the surgical approach. This included conversion from laparoscopy to laparotomy (n = 3, due to bleeding, subcutaneous emphysema, and severe adhesions), switching from the vaginal approach to laparotomy (n = 2, due to bleeding and enlarged uterus), and conversion from a laparoscopic to vaginal approach (n = 1, due to severe adhesions).
Of the 17 patients who developed postoperative complications, 1 (0.3%) had Takotsubo cardiomyopathy (managed by cardiac intensive care), 3 (0.9%) had bowel injury (ileus that was managed conservatively and small bowel obstruction/perforation that required reoperation), 2 (0.6%) had chest pain (non-significant and required no intervention), 2 (0.6%) had vaginal bleeding (managed conservatively), 1 (0.3%) had postoperative hematoma (managed conservatively after readmission), 1 (0.3%) had pyelonephritis (managed by intravenous antibiotics after readmission), 2 (0.6%) had transient urinary retention (managed with short-term indwelling catheterization), and 2 (0.6%) had considerable pain (rectal and piriformis pain managed with short-term analgesics). Most perioperative complications were minor (26/38 = 68.4%) as per the (IUGA)/(ICS) classification. The Clavien-Dindo Classification System of complications is reported in Table 3.
The median hospital stay was 1 night, with only 25 (7.4%) patients having a prolonged hospital stay (> 2 nights). This was for management of complications (n = 9) or trial of voiding mainly related to an incontinence procedure (n = 9). A total five (1.5%) patients required readmission and five (1.5%) required reoperation. Readmissions were related to management of complications (n = 4) and reoperation on a small bowel obstruction (n = 1). Reoperations included lysis of a mid-urethral sling for prolonged voiding dysfunction (n = 3) (done as an outpatient procedure) and small bowel resection with anastomosis for small bowel obstruction/perforation (n = 2).
No demographic or clinical characteristics were significantly associated with perioperative complications (Table 1). Abdominal procedures (p = 0.03), concomitant hysterectomy (p = 0.01), and McCall culdoplasty (p < 0.001) were significantly associated with perioperative complications (Table 2). After adjusting for the variables that were significantly associated with perioperative complications in univariate analysis, abdominal surgery [odds ratio = 4.63, 95% confidence interval (CI) = 2.01–10.64, p < 0.001] and McCall culdoplasty (odds ratio = 6.44, 95% CI = 2.70–15.35, p < 0.001) were significant predictors of perioperative complications, including both intra- and postoperative complications. (**Some patients had more than one complication. Associated surgery: 1, abdominal/laparoscopic hysterectomy; 2, vaginal hysterectomy; 3, combined hysterectomy; 4, vaginal wall repair; 5, McCall culdoplasty; 6, suspensions including USLS, SSF, and sacrocolpopexy; 7, incontinence procedure including TVT and TOT; 8, colpocleisis; Table 4). Similar findings were obtained when intraoperative complications were considered alone. Concomitant hysterectomy and concomitant incontinence repair procedures were positive risk predictors for postoperative complications while vaginal surgery was a negative risk predictor (Table 4).
Discussion
We report an 11.3% perioperative complications rate (7.4% intraoperative and 5.1% postoperative) among a group of Canadian women of all ages who underwent one of the surgical procedures to correct POP. Comparing the current incidence to previous studies is challenging because of generally limited previous data, variability in urogynecologic procedures included, different complication definitions used, and age restrictions in some studies [14,15,16,17,18]. Nevertheless, the current incidence of perioperative complications appeared to be lower or at least similar to what has been reported before. For example, in a secondary analysis of a large multicenter database of > 33,000 women who underwent surgical correction of POP in the USA, only 3.1% had major postoperative complications [18]. As the study of Erekson and colleagues did not include intraoperative or minor complications [18], their lower rate is still slightly higher than the 2.1% severe postoperative complications observed in the current study. Additionally, another study that was done using Swedish national data of > 18,000 women who underwent surgical correction of POP reported perioperative complications of 3.4% at discharge and 14.6% after 8 weeks, with higher rates in repeat surgery compared with primary surgery [17]. The overall rates of Bohlin and colleagues were higher than those of the current study although the study excluded women who had concomitant repair of urinary incontinence and the complication definition did not include cardiovascular morbidity, respiratory morbidity, and readmission/reoperation [17]. This may reflect better surgical techniques and preparation in the current study, which had generally less organ injury, less infection, and no fistulas. However, as approximately 50% of the 8-week postoperative complications reported by Bohlin were urinary tract infections and wound infections, which are frequently diagnosed after discharge [17], their rates could be comparable to those in the current study, which excluded urinary tract infections (because of inability to track their true occurrence postoperatively) and probably missed non-severe surgical site infections (among patients who did not return to our hospital).
The incidence of perioperative complications in the current study was much lower than reported by studies done among women who underwent urogynecologic surgeries including POP, with rates ranging between 26% and 46% [14,15,16]. The difference was especially apparent in bowel/bladder injury, thromboembolic events, and infections. Being > 15 years old [14, 16], these studies may have missed some newly developed surgical techniques, postoperative prophylactic protocols targeting thromboembolic events, and preoperative prophylactic antimicrobials to reduce surgical site infections. Nevertheless, the finding should be interpreted cautiously as these studies generally had small sample sizes and had roughly 10% to 40% urogynecologic procedures that were not included in the current study [14,15,16]. Additionally, the study of Stepp and colleagues only examined women ≥ 75 years and reported a high proportion of largely subjective urinary tract infections [16].
Unlike incidence, data on factors contributing to perioperative complications of POP procedures are very limited [18] or examined in relation to all urogynecologic rather than POP procedures alone [14, 16]. In the only study that we could identify focusing on POP procedures [18], the list of potential risk factors was missing several preoperative medical and surgical characteristics, did not include intraoperative complications in the outcome, and did not report independent associations. This may explain (at least partially) their failure to detect differences between surgical approaches observed in the current study. The higher risk of perioperative complications observed in abdominal surgery may be related to the higher risk of complications from abdominal hysterectomy compared with vaginal hysterectomy [11, 22]. Additionally, sacrocolpopexy, which was done in approximately half of our patients with an abdominal approach, has been identified as a risk factor for perioperative complications of urogynecologic procedures [16].
Similar to previous findings [18], concomitant hysterectomy and incontinence repair procedures were independent predictors of perioperative complications in the current study. This may be related to increasing operative time and/or risk of surgical site infection [18]. Additionally, Lambrou and colleagues reported that adding more procedures is associated with more blood loss, which is an independent risk factor for perioperative complications [14]. Moreover, a relatively recent systematic review and meta-analysis of randomized trials found that adding incontinence repair to POP procedures is associated with more risk of perioperative complications, probably due to higher risk of bladder injury or increasing blood loss [23].
Surprisingly, McCall culdoplasty was an independent predictor of perioperative complications, especially intraoperative ones. Ureteric obstruction was seen almost exclusively in women having a modified McCall culdoplasty. Previous studies did not show that difference and rather showed equivocal safety compared with other suspension procedures [24, 25].
Older age and obesity, which are well-known predictors for the development of POP [4, 6, 26], were not associated with perioperative complications in the current study. The majority of previous studies failed to detect higher risk of perioperative complications among women of older age and/or with obesity [14, 16]. On the contrary, Stepp and colleagues reported a low incidence of significant perioperative morbidity in elderly women [16]. Additionally, perioperative complications were shown to be low and insignificantly different among obese and non-obese women undergoing vaginal surgery [27, 28]. It is worth mentioning that the choice of POP procedures in the current population was largely dependent on the patient choice and the surgeon assessment. These may have introduced a positive bias that attenuated the potentially harmful impact of these risk factors.
The current study has several advantages; it included all POP procedures among women of all ages operated on by all urogynecologist surgeons at a tertiary care center, which probably reflects realistic complication risks. The comprehensive list of preoperative and operative factors, the use of both univariate and multivariate analysis, and the standard definitions used should fix several limitations in previous studies. The prospectively collected data on perioperative complications probably limited the risk of bias and missing information. Nevertheless, we acknowledge a number of limitations. As the current study is a single-center study, generalizing the finding should be done with caution. As the incidence of perioperative complications was low, it was not possible to do a subgroup analysis to look for risk factors. As we did not have long-term follow-up, we may have missed some minor postoperative infections among women who did not return to the hospital.
However, we believe the current study is a unique addition by cataloging the complications of these increasingly performed procedures. This is an important step for benchmarking with other centers. It can also be used for preoperative counseling. These data should help in preoperative counseling and target ways to further decrease complication rates. This information is also useful for targeting ways to decrease perioperative complications in POP surgery.
References
Swift S, Woodman P, O’Boyle A, Kahn M, Valley M, Bland D, et al. Pelvic organ support study (POSST): the distribution, clinical definition, and epidemiologic condition of pelvic organ support defects. Am J Obstet Gynecol. 2005;192(3):795–806.
Hendrix SL, Clark A, Nygaard I, Aragaki A, Barnabei V, McTiernan A. Pelvic organ prolapse in the Women’s Health Initiative: gravity and gravidity. Am J Obstet Gynecol. 2002;186(6):1160–6.
Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89(4):501–6.
Walker GJ, Gunasekera P. Pelvic organ prolapse and incontinence in developing countries: review of prevalence and risk factors. Int Urogynecol J. 2011;22(2):127–35.
Rortveit G, Brown JS, Thom DH, Van Den Eeden SK, Creasman JM, Subak LL. Symptomatic pelvic organ prolapse: prevalence and risk factors in a population-based, racially diverse cohort. Obstet Gynecol. 2007;109(6):1396–403.
Vergeldt TF, Weemhoff M, IntHout J, Kluivers KB. Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecol J. 2015;26(11):1559–73.
Smith FJ, Holman CD, Moorin RE, Tsokos N. Lifetime risk of undergoing surgery for pelvic organ prolapse. Obstet Gynecol. 2010;116(5):1096–100.
Boyles SH, Weber AM, Meyn L. Procedures for pelvic organ prolapse in the United States, 1979-1997. Am J Obstet Gynecol. 2003;188(1):108–15.
Boyles SH, Weber AM, Meyn L. Procedures for urinary incontinence in the United States, 1979-1997. Am J Obstet Gynecol. 2003;189(1):70–5.
Luber KM, Boero S, Choe JY. The demographics of pelvic floor disorders: current observations and future projections. Am J Obstet Gynecol. 2001;184(7):1496–501. discussion 1501-1493.
Dicker RC, Greenspan JR, Strauss LT, Cowart MR, Scally MJ, Peterson HB, et al. Complications of abdominal and vaginal hysterectomy among women of reproductive age in the United States. The collaborative review of sterilization. Am J Obstet Gynecol. 1982;144(7):841–8.
Mirhashemi R, Harlow BL, Ginsburg ES, Signorello LB, Berkowitz R, Feldman S. Predicting risk of complications with gynecologic laparoscopic surgery. Obstet Gynecol. 1998;92(3):327–31.
Harris WJ. Early complications of abdominal and vaginal hysterectomy. Obstet Gynecol Surv. 1995;50(11):795–805.
Lambrou NC, Buller JL, Thompson JR, Cundiff GW, Chou B, Montz FJ. Prevalence of perioperative complications among women undergoing reconstructive pelvic surgery. Am J Obstet Gynecol. 2000;183(6):1355–8. discussion 1359-1360.
Cengiz H, Dagdeviren H, Kaya C, Helvacoğlu Ç, Ekin M. Perioperative complications of urogynecologic surgery: our experience in a tertiary care hospital. Gynecol Obstet Reprod Med. 2017:1–3.
Stepp KJ, Barber MD, Yoo EH, Whiteside JL, Paraiso MF, Walters MD. Incidence of perioperative complications of urogynecologic surgery in elderly women. Am J Obstet Gynecol. 2005;192(5):1630–6.
Bohlin KS, Ankardal M, Nussler E, Lindkvist H, Milsom I. Factors influencing the outcome of surgery for pelvic organ prolapse. Int Urogynecol J. 2018;29(1):81–9.
Erekson E, Murchison RL, Gerjevic KA, Meljen VT, Strohbehn K. Major postoperative complications following surgical procedures for pelvic organ prolapse: a secondary database analysis of the American College of Surgeons National Surgical Quality Improvement Program. Am J Obstet Gynecol. 2017;217(5):608 e601–17.
Haylen BT, Freeman RM, Swift SE, Cosson M, Davila GW, Deprest J, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint terminology and classification of the complications related directly to the insertion of prostheses (meshes, implants, tapes) & grafts in female pelvic floor surgery. Int Urogynecol J. 2011;22(1):3–15.
Toozs-Hobson P, Freeman R, Barber M, Maher C, Haylen B, Athanasiou S, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for reporting outcomes of surgical procedures for pelvic organ prolapse. Neurourol Urodyn. 2012;31(4):415–21.
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–96.
Al-Kadri HM, Al-Turki HA, Saleh AM. Short and long-term complications of abdominal and vaginal hysterectomy for benign disease. Saudi Med J. 2002;23(7):806–10.
van der Ploeg JM, van der Steen A, Oude Rengerink K, van der Vaart CH, Roovers JP. Prolapse surgery with or without stress incontinence surgery for pelvic organ prolapse: a systematic review and meta-analysis of randomised trials. BJOG. 2014;121(5):537–47.
Schiavi MC, Savone D, Di Mascio D, Di Tucci C, Perniola G, Zullo MA, et al. Long-term experience of vaginal vault prolapse prevention at hysterectomy time by modified McCall culdoplasty or Shull suspension: clinical, sexual and quality of life assessment after surgical intervention. Eur J Obstet Gynecol Reprod Biol. 2018;223:113–8.
Spelzini F, Frigerio M, Manodoro S, Interdonato ML, Cesana MC, Verri D, et al. Modified McCall culdoplasty versus Shull suspension in pelvic prolapse primary repair: a retrospective study. Int Urogynecol J. 2017;28(1):65–71.
Giri A, Hartmann KE, Hellwege JN, Velez Edwards DR, Edwards TL. Obesity and pelvic organ prolapse: a systematic review and meta-analysis of observational studies. Am J Obstet Gynecol. 2017;217(1):11–26. e13.
Nam KH, Jeon MJ, Hur HW, Kim SK, Bai SW. Perioperative and long-term complications among obese women undergoing vaginal surgery. Int J Gynaecol Obstet. 2010;108(3):244–6.
Chen CC, Collins SA, Rodgers AK, Paraiso MF, Walters MD, Barber MD. Perioperative complications in obese women vs normal-weight women who undergo vaginal surgery. Am J Obstet Gynecol. 2007;197(1):98 e91–8.
Acknowledgments
The authors wish to thank the Calgary Women’s Pelvic Health Research Group
Funding
This project has been funded by the section of Pelvic Medicine and Reconstructive Surgery.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Alshankiti, H., Houlihan, S., Robert, M. et al. Incidence and contributing factors of perioperative complications in surgical procedures for pelvic organ prolapse. Int Urogynecol J 30, 1945–1953 (2019). https://doi.org/10.1007/s00192-019-03873-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-019-03873-5