
Abstract
Purpose
To evaluate the effect of posterior tibial slope (PTS) on patient-reported outcomes (PROs) and posterior cruciate ligament (PCL) graft failure after PCL reconstruction.
Methods
Patients undergoing PCL reconstruction with a minimum 2-year follow-up were included in this retrospective cohort study. A chart review was performed to collect patient-, injury-, and surgery-related data. Medial PTS was measured on preoperative lateral radiographs. Validated PROs, including the International Knee Documentation Committee Subjective Knee Form, Knee injury and Osteoarthritis Outcome Score, Lysholm Score, Tegner Activity Scale, and Visual Analogue Scale for pain, were collected at final follow-up. A correlation analysis was conducted to assess the relationship between PTS and PROs. A logistic regression model was performed to evaluate if PTS could predict PCL graft failure.
Results
Overall, 79 patients with a mean age of 28.6 ± 11.7 years and a mean follow-up of 5.7 ± 3.3 years were included. After a median time from injury of 4.0 months, isolated and combined PCL reconstruction was performed in 22 (28%) and 57 (72%) patients, respectively. There were no statistically significant differences in PROs and PTS between patients undergoing isolated and combined PCL reconstruction (non-significant [n.s.]). There were no significant correlations between PTS and PROs (n.s.). In total, 14 (18%) patients experienced PCL graft failure after a median time of 17.5 months following PCL reconstruction. Patients with PCL graft failure were found to have statistically significantly lower PTS than patients without graft failure (7.0 ± 2.3° vs. 9.2 ± 3.3°, p < 0.05), while no differences were found in PROs (n.s.). PTS was shown to be a significant predictor of PCL graft failure, with a 1.3-fold increase in the odds of graft failure for each one-degree reduction in PTS (p < 0.05).
Conclusions
This study showed that PTS does not affect PROs after PCL reconstruction, but that PTS represents a surgically modifiable predictor of PCL graft failure.
Level of evidence
III.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Compared to anterior cruciate ligament (ACL) injuries, posterior cruciate ligament (PCL) injuries are rare and occur predominantly as combined injuries [1, 2]. While acceptable patient-reported outcomes (PROs) after PCL reconstruction (PCL-R) have been reported, the rates of return to sports and physically demanding activities are low [3,4,5]. However, athletic and physical performance is a key element of a high quality of life for many patients. This is especially true for young and physically active patients, whom are most frequently affected by PCL injuries [1]. Patient-reported outcomes are further compromised in patients who fail operative treatment of PCL injuries [6]. One study has shown that 70–80% of patients with failed operative treatment of PCL injuries never returned to sports activities and complained of moderate-to-severe pain during daily activities, underscoring the pervasive disability associated with PCL graft failure [6].
To date, only a few studies have identified risk factors for PCL graft failure [6,7,8]. Persistent posterolateral rotatory instability, femoral or tibial bone tunnel misplacement, and varus malalignment are all factors associated with increased risk for PCL graft failure [6, 8]. Biomechanically, it was shown that there is a significant and negative correlation between posterior tibial slope (PTS) and PCL graft forces, indicating a higher risk of PCL graft failure with decreased (flatter) PTS [7]. Clinical investigations have shown that sagittal alignment, represented by the PTS, affects the risk of PCL injury [9]. In particular, patients with primary PCL injury have been found to have lower PTS than healthy controls. The effect of PTS was even more pronounced when looking at the injury mechanism, with non-contact PCL injuries having the lowest PTS [9]. Furthermore, low PTS has been shown to result in decreased posterior tibial sag reduction and increased residual posterior tibial translation after PCL-R [10]. These studies demonstrate the biomechanical influence of PTS on PCL function and failure; however, there is a paucity of literature delineating how PTS affects PROs and PCL graft failure rates after PCL-R. Given that PTS is a patient-specific characteristic, it might be a surgically modifiable target that should be considered in the future as part of an individualized treatment approach to avoid PCL graft failure and improve functional outcomes after PCL-R [11].
Therefore, the objective of this study was to evaluate the effect of PTS on PROs and PCL graft failure in individuals that underwent PCL-R after a minimum 2-year follow-up. It was hypothesized that PTS would positively correlate with PROs, and that low (flat) PTS is a significant predictor of PCL graft failure.
Materials and methods
This retrospective study was approved by the Institutional Review Board of the University of Pittsburgh (No.: STUDY20070271).
Patients undergoing primary single-bundle isolated or combined PCL-R at the senior authors’ institution between 2008 and 2018 were retrospectively reviewed for eligibility for this study. A minimum 2-year follow-up was required for inclusion in this study. Exclusion criteria included previous or concomitant proximal tibia, distal femur, or patellar fracture; history of inflammatory arthritis; PCL repair; incomplete medical records or open physes at the time of PCL-R. Consistent with previous studies, patients undergoing concomitant ACL, posterolateral corner (PLC), or medial collateral ligament (MCL) reconstruction were also included and defined as “combined PCL-R” [10, 12].
Posterior cruciate ligament graft failure was defined if any of the following criteria were met: (1) complete PCL graft disruption confirmed by magnetic resonance imaging (MRI) or arthroscopy, (2) revision PCL-R, (3) conversion to knee arthroplasty, and (4) abnormal (grade C) or severely abnormal (grade D) posterior drawer test according to the International Knee Documentation Committee (IKDC) Knee Ligament Examination Form, combined with severe pain or reports of posterior instability.
Surgical technique and rehabilitation
Included patients underwent arthroscopic anatomic single-bundle PCL-R using a standardized transtibial technique. Graft choices for PCL-R included autografts (hamstring tendon and quadriceps tendon) and allografts, and were based on both surgeon preference and concurrent ligament reconstruction. The femoral tunnel was drilled in the center of the anterolateral bundle of the native PCL. To confirm anatomic tibial tunnel placement, a 70° scope was used. Graft fixation was performed at 70–90° flexion with simultaneous anterior tibial stress using either suspensory, interference screw, or hybrid (suspensory and interference screw) fixation techniques. A standardized postoperative rehabilitation protocol including use of static and dynamic PCL braces was recommended, as previously described in detail [2].
Demographic and surgical data
To collect patient-, injury-, and surgery-related data, a chart review was conducted between July 2020 and December 2020. Patient-specific data included age at the time of primary PCL-R, sex, laterality, and body mass index (BMI). The following injury-related data were recorded: injury mechanism, time from injury to PCL-R, and concomitant medial and lateral meniscal injuries. Injury mechanisms were categorized as sports-related, traffic-related, non-sports and non-traffic-related traumatic impact to the anterior proximal tibia (i.e., fall), and hyperextension [13, 14]. Surgical data that were collected included isolated or combined PCL-R, concomitant ligament reconstruction (ACL, PLC, and MCL), concomitant meniscal surgery (partial meniscectomy, repair), other concomitant surgical procedures (peroneal nerve neurolysis and cartilage surgery), graft type (hamstring or quadriceps tendon autograft, and allograft), graft diameter, and femoral and tibial graft fixation technique (suspensory, interference screw, and hybrid). Hybrid graft fixation was defined as a combined suspensory and interference screw fixation.
Posterior tibial slope measurement
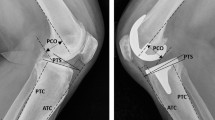
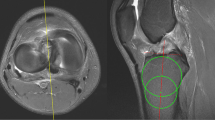
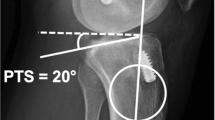
Preoperatively available lateral radiographs were used to measure the medial PTS. To avoid measurement inaccuracies related to malrotated radiographs, the posterior femoral condyle overlap was measured and lateral radiographs with > 6 mm overlap were excluded [15, 16]. The medial PTS was measured using a previously described technique [17, 18]. First, the proximal tibial shaft axis was determined as a line connecting the centers of two circles located 5 cm and 15 cm distal to the joint line, respectively, which touched the anterior and posterior cortex of the tibia. Next, a tangential line was drawn to the medial tibial plateau. Finally, the angle between the proximal tibial shaft axis and the line tangential to the medial tibial plateau was subtracted from 90° to obtain the medial PTS (Fig. 1). Posterior tibial slope measurements were performed by observer one (PWW) using Philips iSite PACS (Koninklijke Philips N.V., Amsterdam, The Netherlands), which allows a measurement accuracy of 0.1 mm and 0.1°, respectively. To ensure intra- and interrater reliability of measurements, intraclass correlation coefficients (ICC) were calculated. For this, ten lateral knee radiographs were randomly selected and the medial PTS was measured three times at 2-week intervals by observer one (PWW) and once each by observer two (NNW) and three (JDH). Excellent intrarater (ICC, 0.99 95% CI [0.98, 0.99]) and good-to-excellent interrater (ICC, 0.92 95% CI [0.76, 0.98]) reliability of measurements was found.

Posterior tibial slope (PTS) measurement. Preoperative strict lateral radiograph of a right knee with isolated posterior cruciate ligament injury and a medial PTS of 6.7°. To obtain the medial PTS, the angle between the proximal tibial shaft axis (line 1) and a tangential line to the medial tibial plateau (line 2) was subtracted from 90°
Patient-reported outcome scores (PROs)
Questionnaires with standardized and validated PROs including the International Knee Documentation Committee Subjective Knee Form (IKDC-SKF), Knee injury and Osteoarthritis Outcome Score (KOOS), Lysholm Score, Tegner Activity Scale, and Visual Analogue Scale (VAS) for pain were mailed to all eligible patients. All patients that agreed to participate in this study signed a written informed consent form.
Statistical analysis
A previous study demonstrated that patients with primary isolated and combined PCL injuries (5.7° ± 2.1°) have statistically significantly lower PTS compared to age- and sex-matched ligament-intact controls (8.6° ± 2.2°) [9]. The reported PTS values were used for an a priori power analysis to determine the sample size necessary to detect significant differences in PTS between patients with and without PCL graft failure. In addition, considering the reported rate of PCL revision surgery of 3–13% [5, 19], a group allocation (failure vs. non-failure) of 1:8 was assumed. To achieve a statistical power of 0.80, a total sample size of 46 patients was required (Failure group, n = 5; Non-failure group, n = 41; effect size, 1.35; level of significance, 0.05). G*Power (Erdfelder, Faul, Buchner, Lang, HHU Düsseldorf, Düsseldorf, Germany) was used for power analysis.
Categorical variables are presented as counts and corresponding percentages. According to the distribution of the data as determined by the Shapiro–Wilk Test, continuous variables are presented as mean ± standard deviation (normally distributed) or median and inter-quartile range (IQR; non-normally distributed). Spearman’s rank-order correlations were used to assess the relationship between medial PTS and PROs (IKDC-SKF, KOOS subscales, Lysholm Score, Tegner Activity Scale, VAS for pain) in patients undergoing PCL-R. Group comparisons of categorical variables were performed using the Chi-square test or the Fisher’s exact test, as appropriate. Group comparison of continuous variables was performed by the Mann–Whitney U test, unpaired t test, or one-way analysis of variance (ANOVA), as appropriate. In addition, a logistic regression model was performed to evaluate whether PCL graft failure (dependent variable) could be predicted by medial PTS (independent variable). Statistical analyses were performed using SPSS software version 26.0 (IBM-SPSS, New York, USA). The level of significance was set at p < 0.05.
Results
In total, 101 patients were screened for eligibility. After excluding 22 patients due to PCL repair (n = 8), incomplete medical records (n = 6), proximal tibia fracture (n = 5), distal femur fracture (n = 1), patellar fracture (n = 1), and congenital absence of ACL and PCL (n = 1), a total of 79 (78%) patients were included in this study. Patient-, injury-, and surgery-related characteristics of the total study group are shown in Table 1.
The mean age at the time of PCL-R was 28.6 ± 11.7 years (range 15–64 years) and the median time from injury to PCL-R was 4.0 months (IQR, 7.0 months). Isolated PCL-R was performed in 22 (28%) patients, while combined PCL-R was performed in 57 (72%) patients. Concomitant ACL, PLC, and MCL reconstruction was performed in 38 (48%), 27 (34%), and 12 (15%) patients, respectively. In addition, concurrent cartilage surgery (microfracture and chondroplasty) and peroneal nerve neurolysis was performed in 2 (3%) and 6 (8%) patients, respectively.
The mean medial PTS for the full sample was 8.8 ± 3.3° (range 1–17°). There was no statistically significant difference in medial PTS between the different types of injury mechanisms observed (non-significant [n.s.]): sports-related (8.8 ± 3.0°), traffic-related (8.9 ± 3.4°), non-sports and non-traffic-related traumatic impact to anterior proximal tibia (9.1 ± 3.0°), and hyperextension (7.3 ± 3.7°). In addition, there was no statistically significant difference in medial PTS between patients undergoing isolated and combined PCL-R (8.4 ± 3.4° vs. 9.0 ± 3.2°, n.s.; Fig. 2).

Isolated vs. combined PCL-R. A Patient-reported outcome scores (PROs). Indicators (triangle, rhombus) represent mean values. Error bars represent standard deviation. B Medial posterior tibial slope (PTS). ADL activities of daily living, IKDC-SKF International knee documentation committee subjective knee form, KOOS knee injury and osteoarthritis outcome score, PCL-R posterior cruciate ligament reconstruction, Sport/Rec sport and recreation function, QOL knee-related quality of life; No statistically significant difference was found between isolated and combined PCL-R with respect to PROs and medial PTS (n.s.)
Overall, 14 (18%) patients sustained PCL graft failure after a median time of 17.5 months (IQR, 21 months) following PCL-R. Individuals with PCL graft failure were found to have statistically significantly lower (flatter) medial PTS than individuals without PCL graft failure (7.0 ± 2.3° vs. 9.2 ± 3.3°, p < 0.05). The mean difference in medial PTS between patients with and without PCL graft failure was 2.2° (95% CI [0.2, 4.2], p < 0.05). No other variables were found to be statistically significantly different between patients with and without PCL graft failure (Table 2). Seventy-four cases were included in the logistic regression model, which correctly classified 82% of cases and was statistically significant (p < 0.05). The medial PTS was shown to be a statistically significant predictor of PCL graft failure (p < 0.05). According to the logistic regression model, a one-degree reduction in medial PTS resulted in 1.3-fold increase in the odds of PCL graft failure (95% CI [1.013,1.580], p < 0.05).
At a mean follow-up of 5.7 ± 3.3 years (range 2.0–12.4 years), PROs were available for 57 (72%) patients. A detailed summary of the PROs data is shown in Table 3. There was no statistically significant difference in PROs between patients undergoing isolated and combined PCL-R (n.s.; Fig. 2) and between patients with and without PCL graft failure (n.s., Table 2). In addition, there were no statistically significant correlations between medial PTS and any of the PROs (Table 4, n.s.).
Discussion
The most important finding of this study was that PTS does not affect PROs after PCL-R, but represents a significant and surgically modifiable predictor of PCL graft failure. Although a 1.3-fold increase in the odds of PCL graft failure for each one-degree reduction in PTS may appear to be a marginal increase, PTS-increasing osteotomies may be considered in cases with recurrent PCL insufficiency, and for those with high-grade posterior knee laxity and low PTS.
Residual posterior knee laxity is a common finding after PCL-R. Over the past decades, many studies have focused on surgical techniques (single-bundle vs. double-bundle; tibial-inlay vs. transtibial), graft fixation angles, and concurrent peripheral stabilization procedures to address residual posterior laxity and improve clinical outcomes [20,21,22,23]. Increased PTS has been demonstrated to be a relevant risk factor for primary and recurrent ACL injuries. Consequently, PTS correcting osteotomies are now performed in patients with ACL injuries, with recent studies showing good results [24, 25]. Although biomechanical studies have shown increased posterior knee laxity with decreased PTS in PCL-deficient knees [26], PTS-increasing osteotomies have not yet been clinically accepted for the treatment of PCL injuries.
In this study, patients with PCL graft failure (7.0 ± 2.3°) were found to have significantly lower PTS than patients without graft failure (9.2 ± 3.3°). In addition, a one-degree reduction in PTS was shown to result in a 1.3-fold increase in the odds of experiencing PCL graft failure. The findings of this study may be related to increased residual posterior knee laxity with lower PTS causing repetitive PCL graft overload, which ultimately results in PCL graft failure. This assumption is supported by one study, showing that low PTS is associated with higher residual posterior tibial translation (quantified on posterior stress radiographs) after single-bundle PCL-R [10]. In contrast, another study did not find an association between PTS and residual posterior tibial translation after double-bundle PCL-R at a mean follow-up of 18.5 months [12]. As a result, the authors concluded that double-bundle PCL-R may be superior to single-bundle PCL-R in preventing residual posterior knee laxity [12]. However, the results of that study should be interpreted cautiously, as the authors also showed a significant and positive correlation between posterior tibial translation and follow-up time [12]. Therefore, a mean follow-up of 18.5 months (range 6–84 months) may not be appropriate for final conclusion that double-bundle PCL-R is superior to single-bundle PCL-R in preventing residual posterior knee laxity.
The effect of PTS on functional outcomes in patients undergoing PCL-R is largely unknown. In this study, the associations between validated PROs (IKDC-SKF, KOOS subscales, Lysholm Score, Tegner Activity Scale, and VAS for pain) and medial PTS was assessed. After a mean follow-up of 5.7 years after PCL-R, none of the PROs were significantly associated with PTS. This is consistent with studies investigating the relationship between functional outcomes and PTS in patients undergoing ACL reconstruction. A recent study showed no difference in PROs between patients with high and low PTS undergoing primary ACL reconstruction after a minimum 10-year follow-up [27]. However, high PTS (> 5.6° medial PTS, > 3.8° lateral PTS measured by MRI) was associated with an increased ACL graft failure rate [27]. Accordingly, the biomechanically confirmed PTS-dependent change in knee kinematics appears to predominantly affect graft forces rather than clinical outcomes [7, 28, 29]. Increased graft forces may ultimately cause PCL graft failure.
Previous studies have shown that there is no difference in PTS between patients with isolated PCL injury and patients with combined (PCL + PLC, PCL + MCL, or PCL + PLC + ACL) injuries [9, 10]. Accordingly, subgroup analysis was performed in this study to account for combined PCL injuries as a potential confounder factor. Consistent with previous reports, there was no difference in PTS between isolated (8.4 ± 3.4°) and combined (9.0 ± 3.2°) PCL injuries. In addition, there was no significant difference in PCL graft failure rates between isolated and combined PCL-R. Increased PCL graft failure rates at low PTS, irrespective of isolated or combined PCL-R, underscore the importance of the PTS for PCL graft survival. Thus, a purely ligamentous reconstruction may be insufficient to maintain restored posterior knee stability, as this requires an intact PCL graft. Based on the findings of this study, additional procedures such as PTS-increasing osteotomy in patients with recurrent PCL insufficiency, high-grade posterior knee laxity, and low PTS may be considered. This is supported by previous research which has shown that an increase in PTS in PCL-deficient knees results in a significant anterior shift of the tibial resting position, thereby reducing posterior tibial translation [26]. Following PCL-R, an increase in PTS has been found to reduce PCL graft forces [7]. When all considered, these findings suggest that increased PTS may serve as a protective factor for PCL grafts against graft failure.
Despite biomechanical and clinical evidence advocating PTS-increasing osteotomies in the treatment of PCL injuries, there are no clinical studies demonstrating superiority of combined PCL-R and PTS-increasing osteotomy compared to isolated PCL-R or isolated PTS-increasing osteotomy. However, based on the findings of this study, PTS-increasing osteotomy should be considered in patients with high-grade posterior instability, low PTS, and concurrent risk factors for PCL graft failure. It is believed that isolated soft-tissue reconstruction will only partially restore posterior knee stability in patients with low PTS and high-grade posterior knee laxity. Future studies should focus on indications for PTS-increasing osteotomies in patients undergoing PCL-R.
This study aimed to determine the association of PTS for both graft failure following PCL-R and PROs. Strengths of this study included adequate follow-up, use of validated PROs, and a sufficient sample size to ensure statistical power of at least 80%. However, this investigation is not without limitations. This study included patients undergoing isolated and combined PCL-R, which may have caused selection bias. However, there was no difference in PTS and PCL graft failure rates between patients with isolated and combined PCL-R, which is consistent with previous reports, thus minimizing the risk of bias [9, 10]. Functional outcomes after PCL-R may also be affected by coronal lower limb alignment and residual posterior tibial translation. However, posterior tibial stress radiographs and long-leg radiographs were inconsistently available. Therefore, it was not possible in this study to assess the effects of coronal alignment and posterior tibial translation on PCL graft failure and PROs.
Conclusions
In this study, a 1.3-fold increase in the odds of PCL graft failure for each one-degree reduction in PTS was found. Accordingly, low PTS represents a significant and surgically modifiable factor associated with PCL graft failure. However, PTS did not affect PROs after an average time of 5.7 years after PCL-R. Posterior tibial slope increasing osteotomies might be a consideration when recurrent PCL insufficiency, high-grade posterior knee laxity, and associated low PTS are present in individuals undergoing PCL-R.
References
Winkler PW, Zsidai B, Wagala NN, Hughes JD, Horvath A, Senorski EH et al (2020) Evolving evidence in the treatment of primary and recurrent posterior cruciate ligament injuries, part 1: anatomy, biomechanics and diagnostics. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06357-y
Winkler PW, Zsidai B, Wagala NN, Hughes JD, Horvath A, Senorski EH et al (2020) Evolving evidence in the treatment of primary and recurrent posterior cruciate ligament injuries, part 2: surgical techniques, outcomes and rehabilitation. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06337-2
Lee DW, Kim JG, Yang SJ, Cho SI (2019) Return to sports and clinical outcomes after arthroscopic anatomic posterior cruciate ligament reconstruction with remnant preservation. Arthroscopy 35:2658-2668.e2651
Lutz PM, Merkle M, Winkler PW, Geyer S, Herbst E, Braun S et al (2021) Combined posterolateral knee reconstruction: ACL-based injuries perform better compared to PCL-based injuries. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06409-3
Tucker CJ, Cotter EJ, Waterman BR, Kilcoyne KG, Cameron KL, Owens BD (2019) Functional outcomes after isolated and combined posterior cruciate ligament reconstruction in a military population. Orthop J Sports Med 7:2325967119875139
Noyes FR, Barber-Westin SD (2005) Posterior cruciate ligament revision reconstruction, part 1: causes of surgical failure in 52 consecutive operations. Am J Sports Med 33:646–654
Bernhardson AS, Aman ZS, DePhillipo NN, Dornan GJ, Storaci HW, Brady AW et al (2019) Tibial slope and its effect on graft force in posterior cruciate ligament reconstructions. Am J Sports Med 47:1168–1174
Lee SH, Jung YB, Lee HJ, Jung HJ, Kim SH (2012) Revision posterior cruciate ligament reconstruction using a modified tibial-inlay double-bundle technique. J Bone Joint Surg Am 94:516–522
Bernhardson AS, DePhillipo NN, Daney BT, Kennedy MI, Aman ZS, LaPrade RF (2019) Posterior tibial slope and risk of posterior cruciate ligament injury. Am J Sports Med 47:312–317
Gwinner C, Weiler A, Roider M, Schaefer FM, Jung TM (2017) Tibial slope strongly influences knee stability after posterior cruciate ligament reconstruction: a prospective 5- to 15-year follow-up. Am J Sports Med 45:355–361
Winkler PW, Godshaw BM, Karlsson J, Getgood AMJ, Musahl V (2021) Posterior tibial slope: the fingerprint of the tibial bone. Knee Surg Sports Traumatol Arthrosc 29:1687–1689
Bernhardson AS, DePhillipo NN, Aman ZS, Kennedy MI, Dornan GJ, LaPrade RF (2019) Decreased posterior tibial slope does not affect postoperative posterior knee laxity after double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 47:318–323
Schlumberger M, Schuster P, Eichinger M, Mayer P, Mayr R, Immendörfer M et al (2020) Posterior cruciate ligament lesions are mainly present as combined lesions even in sports injuries. Knee Surg Sports Traumatol Arthrosc 28:2091–2098
Schulz MS, Russe K, Weiler A, Eichhorn HJ, Strobel MJ (2003) Epidemiology of posterior cruciate ligament injuries. Arch Orthop Trauma Surg 123:186–191
Pfeiffer TR, Burnham JM, Hughes JD, Kanakamedala AC, Herbst E, Popchak A et al (2018) An increased lateral femoral condyle ratio is a risk factor for anterior cruciate ligament injury. J Bone Joint Surg Am 100:857–864
Weinberg DS, Williamson DF, Gebhart JJ, Knapik DM, Voos JE (2017) Differences in medial and lateral posterior tibial slope: an osteological review of 1090 tibiae comparing age, sex, and race. Am J Sports Med 45:106–113
Napier RJ, Garcia E, Devitt BM, Feller JA, Webster KE (2019) Increased radiographic posterior tibial slope is associated with subsequent injury following revision anterior cruciate ligament reconstruction. Orthop J Sports Med 7:2325967119879373
Winkler PW, Wagala NN, Hughes JD, Lesniak BP, Musahl V (2021) A high tibial slope, allograft use, and poor patient-reported outcome scores are associated with multiple ACL graft failures. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-021-06460-8
Lind M, Nielsen TG, Behrndtz K (2018) Both isolated and multi-ligament posterior cruciate ligament reconstruction results in improved subjective outcome: results from the Danish knee ligament reconstruction registry. Knee Surg Sports Traumatol Arthrosc 26:1190–1196
Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin TM, Woo SL (2000) Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 28:144–151
Harner CD, Janaushek MA, Ma CB, Kanamori A, Vogrin TM, Woo SL (2000) The effect of knee flexion angle and application of an anterior tibial load at the time of graft fixation on the biomechanics of a posterior cruciate ligament-reconstructed knee. Am J Sports Med 28:460–465
Harner CD, Vogrin TM, Höher J, Ma CB, Woo SL (2000) Biomechanical analysis of a posterior cruciate ligament reconstruction. Deficiency of the posterolateral structures as a cause of graft failure. Am J Sports Med 28:32–39
Lee DY, Kim DH, Kim HJ, Ahn HS, Lee TH, Hwang SC (2018) Posterior cruciate ligament reconstruction with transtibial or tibial inlay techniques: a meta-analysis of biomechanical and clinical outcomes. Am J Sports Med 46:2789–2797
Akoto R, Alm L, Drenck TC, Frings J, Krause M, Frosch KH (2020) Slope-correction osteotomy with lateral extra-articular tenodesis and revision anterior cruciate ligament reconstruction is highly effective in treating high-grade anterior knee laxity. Am J Sports Med 48:3478–3485
Song GY, Ni QK, Zheng T, Zhang ZJ, Feng H, Zhang H (2020) Slope-reducing tibial osteotomy combined with primary anterior cruciate ligament reconstruction produces improved knee stability in patients with steep posterior tibial slope, excessive anterior tibial subluxation in extension, and chronic meniscal posterior horn tears. Am J Sports Med 48:3486–3494
Giffin JR, Stabile KJ, Zantop T, Vogrin TM, Woo SL, Harner CD (2007) Importance of tibial slope for stability of the posterior cruciate ligament deficient knee. Am J Sports Med 35:1443–1449
Yoon KH, Park SY, Park JY, Kim EJ, Kim SJ, Kwon YB et al (2020) Influence of posterior tibial slope on clinical outcomes and survivorship after anterior cruciate ligament reconstruction using hamstring autografts: a minimum of 10-year follow-up. Arthroscopy 36:2718–2727
Bernhardson AS, Aman ZS, Dornan GJ, Kemler BR, Storaci HW, Brady AW et al (2019) Tibial slope and its effect on force in anterior cruciate ligament grafts: anterior cruciate ligament force increases linearly as posterior tibial slope increases. Am J Sports Med 47:296–302
Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD (2004) Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med 32:376–382
Funding
No funding was received for the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All listed authors have contributed substantially to this work: PWW, NNW, MF, EMN, SC, and JDH collected data, and performed statistical analysis, literature review, and primary manuscript preparation. VM, BPL, DV, SR, and JJI assisted with interpretation of the results as well as editing and final manuscript preparation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
VM reports educational grants, consulting fees, and speaking fees from Smith & Nephew plc, educational grants from Arthrex, is a board member of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS), and Deputy Editor-in-Chief of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA). DV reports consulting fees from Arthrex and is a member of the editorial board of The American Journal of Sports Medicine.
Ethical approval
This study was approved by the Institutional Review Board of the University of Pittsburgh (No.: STUDY20070271).
Informed consent
Written informed consent was obtained from each patient who completed the questionnaire of this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The investigation was performed at the Department of Orthopaedic Surgery, University of Pittsburgh, Pittsburgh, PA, USA.
Rights and permissions
About this article

Cite this article
Winkler, P.W., Wagala, N.N., Carrozzi, S. et al. Low posterior tibial slope is associated with increased risk of PCL graft failure. Knee Surg Sports Traumatol Arthrosc 30, 3277–3286 (2022). https://doi.org/10.1007/s00167-021-06760-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06760-z