
Abstract
Purpose
To determine the best angle to drill the femoral tunnels of an anterolateral ligament (ALL) anatomic reconstruction combined with a single-bundle anterior cruciate ligament (ACL) reconstruction to avoid tunnel collisions and cortical disruption.
Methods
Ten cadaveric knees were studied. Single-bundle anatomic ACL femoral tunnels were arthroscopically drilled. The starting point of the ALL femoral tunnel was located posterior and superior to the lateral epicondyle. ALL tunnels were drilled at four different angulations: (1) 0° axial/0° coronal, (2) 0° axial/30° coronal superior, (3) 30° axial anterior/0° coronal, and (4) 30° axial anterior 30° coronal superior. Specimens were scanned by computed tomography to measure the relations of each trajectory with the ACL socket and the nearest cortical bone.
Results
None of the four trajectories studied presented risk of collision with the ACL. The tunnel at 30° anterior/30° proximal presented the safest distance to the ACL socket (P = 0.01) [mean distance 18.6 mm (SD ± 6.7)]. However, both tunnels angled at 0° in the axial plane presented a high risk of posterior femoral cortex disruption (P = 0.01), either by close proximity or direct contact in some specimens (mean distance 3.1 mm (SD ± 2.8) at 0° axial/0° coronal and 3.7 mm (SD ± 2.2) at 0° axial/30° coronal).
Conclusions
When performing simultaneous ACL and ALL ligament reconstruction, the ALL femoral tunnel should be drilled with an angle of 30° anterior in the axial plane and 30° proximal in the coronal plane. Tunnels with an angle of 0° in the axial plane showed high risk of contact and disruption of the posterior femoral cortex; thus, these angles should be avoided. The clinical relevance of this work is that an ALL anatomical reconstruction does not represent a risk when performing a simultaneous ACL reconstruction as long as the ALL tunnel is reamed with a proximal and anterior angulation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite generally good outcomes after anterior cruciate ligament (ACL) reconstruction, a number of patients have persistent rotatory laxity and pivot shift on examination, and many are not able to return to preinjury performance after surgery [1].
Recently, interest in the anatomy and function of the anterolateral structures of the knee has been focused around the anterolateral ligament (ALL). Although the subject is still under debate, at present, many authors advocate for this ligament’s existence as an anatomic structure and its role as a secondary stabilizer controlling the internal rotation of the knee in the context of an injured or insufficient ACL [12, 20].
Based on detailed description of the anatomy, histology and biomechanics of the ALL as an anatomic structure [4, 20], in recent years, there has been an effort to develop an anatomic reconstruction based on the reasoning that restoration of the normal anatomy would produce an optimal biomechanic result. Many variations regarding ALL reconstruction techniques have been reported, all of which propose slightly different attachments for femoral graft fixation. These variations are perhaps due to the different reported femoral footprints of the ALL [6, 7].
Kennedy et al. [17] described a femoral attachment point located proximal and posterior to the epicondyle and to the lateral collateral ligament (LCL). Although it has been demonstrated that the ALL is not an isometric structure, Katakura et al. [16] reported that this position had the least tension change during knee range of motion, providing a physiological non-isometry with a favourable biomechanical behaviour with the graft tighter near extension when the ALL engages and prevents the pivot shift phenomenon. This ALL femoral footprint used in ALL reconstruction has been demonstrated to have good results in recent biomechanical studies [9, 14, 18].
The safety of femoral tunnel drilling for ALL reconstruction was assessed by Helito et al. [13] but only in terms of soft tissue regarding the safety distance to the LCL and the popliteus muscle tendon. Other previous studies have assessed the risk of femoral tunnel collisions during posterolateral and posteromedial ligament reconstructions in combination with posterior and anterior cruciate ligament injuries, remarking the importance of being aware of the correct tunnel placement when performing simultaneous multiligamentary reconstructions [2, 3, 10, 11].
The purpose of this study was to determine the best angle to drill the femoral tunnels of the ALL anatomic reconstruction combined with a single-bundle ACL reconstruction to avoid tunnel collisions and cortical disruption when performing an in–out ACL technique through a low anteromedial portal. The hypothesis was that an ALL tunnel angled 30° superior and 30° anterior represents the safest orientation to avoid collision with the ACL tunnel and cortical bone disruption. The importance of this study was that because of the tunnel’s proximity and the anatomy of the intercondylar notch, it is important that the surgeon be always aware of the safest tunnel placement to avoid potential complications of simultaneous ACL–ALL reconstructions.
Materials and methods
This study was performed after approval from the Institutional Review Board at the University of Barcelona (IRB00003099). Ten cadaveric knee specimens from donors (mean age of 70; five females and five males) were obtained from the tissue bank. No donor had a history of knee injury or prior surgical intervention. Specimens were kept at − 20 °C and were thawed at room temperature 24 h before the experiment. The femur and tibia diaphysis were cut 250 mm from the joint line. Skin and subcutaneous fat were removed along with soft tissue of more than 150 mm from the joint line.
ACL femoral tunnel
An arthroscopic procedure was performed. The femur was mounted on a fixed knee holder with the tibial side left free. A range of motion from 120° to 0° was confirmed. A high anterolateral (AL) portal was established as the initial viewing portal. A high parapatellar anteromedial portal (AM) was also established as a viewing portal for better visualization of the medial wall of the lateral condyle. Then an accessory anteromedial (AAM) portal, created under direct vision just superior to the medial joint line approximately 2 cm medial to the patellar tendon, was established as the working portal for the ACL femoral tunnel. The native ACL was resected, preserving 1–2 mm of the fibres of the femoral stump to facilitate footprint identification. The centre of the footprint was marked as the insertion point. A zero-offset Acufex Endofemoral Aimer (Smith and Nephew) was introduced through the AAM portal and placed at the desired location for the ACL femoral tunnel. The knee was flexed to 120°, and a 2.7-mm drill-tip guide pin was drilled through the lateral femoral condyle until resistance from the lateral femoral cortex was encountered. Finally, using an endoscopic graduated drill bit, a femoral socket 8 mm in diameter and 30 mm in length was created.
ALL dissection and tunnel orientations
The fascia lata was removed to more easily assess the lateral aspect of the joint. The lateral aspect of the knee was carefully dissected to identify the LCL and the trajectory and insertions of the ALL following the technique described by Dagett et al. [5]. It was found the ALL consistently overlapped the lateral collateral ligament near its attachment, with the location of the origin spanning posterior and proximal to the lateral epicondyle.
Once the starting point of the ALL femoral tunnel was located, approximately 5 mm posterior and 10 mm superior to the lateral epicondyle, a 2.4-mm guidewire was drilled through the centre of the femoral attachment of the ALL at four different orientations with the help of a manual goniometer. Angle measurements were performed using anatomical landmarks as reference to better reproduce a real surgical scenario. In the coronal plane, the 0° reference angulation was a perpendicular line to the anatomical axis of the femur. In the axial plane, two markers were placed at each epicondyle to outline the epicondylar axis such that a parallel line was used as the 0° reference angulation. Then a 0.5-mm radiopaque strand was passed through the eye of the guidewire and pulled from the medial side, leaving the radiopaque strand marking the trajectory for each of the four orientations through the femur. The radiopaque strands were later used to recognize the tunnels on the computed tomography (CT) images. This technique was used in previous similar studies to evaluate femoral tunnel orientations [10, 11].
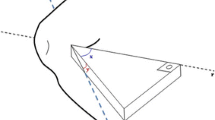
The orientation of the tunnels depicted by the guidewires was as follows: (1) 0° axial angulation and 0° coronal angulation (posteroinferior); (2) 0° axial angulation and 30° coronal superior angulation (posteorsuperior); (3) 30° axial anterior angulation and 0° coronal angulation (anteroinferior); and (4) 30° axial anterior angulation and 30° coronal superior angulation (anterosuperior) (Fig. 1).

Femoral tunnel orientation for the ALL in a left knee. Tunnels were created at 0° and 30° in the axial (a) and the coronal (b) planes. Starting point corresponding to the ALL femoral attachment located posterior and superior to the lateral epicondyle (*). Femoral anatomical axis (+)
Computed tomography scanning
Computed tomography (CT) was performed in every specimen using the Somaton Sensation 64 (Siemens Medical Systems, Erlangen, Germany). The images were obtained with a rotation time of 0.5 s, slice collimation of 0.6 mm, 120 kV, and 90 mA effective current. Axial reconstructions were performed with 1.5-mm sections. Using an open-source software RadiAnt DICOM Viewer 4.6.5 (64bit) for navigating in multidimensional DICOM images, the axial, coronal and sagittal plane CT images were obtained to generate 3D reconstructions. A radiologist with more than 15 years of musculoskeletal imaging experience performed all measurements, and an orthopaedic surgeon then repeated the measurements. Interobserver agreement was analysed using the intraclass correlation coefficient (ICC). First, it was confirmed that the actual tunnel angles drilled for the ALL approximately matched the authors’ intended angles. Then the orientations of the ACL tunnel in the sagittal and coronal planes were calculated. For each ALL tunnel, the shortest distance found from the ACL socket to each tunnel trajectory was measured, and the tunnel length from the entry point to the point where each ALL tunnel reached its shortest distance to the ACL tunnel was recorded. In addition, the shortest distance to the posterior femoral cortical was measured for the posterosuperior (0° axial, 30° coronal) and posteroinferior (0° axial, 0° coronal) ALL tunnels and to the intercondylar notch for the anteroinferior (30° axial, 0° coronal) and posteroinferior (0° axial, 0° coronal) ALL tunnels. The opposite remaining two trajectories in each case were discarded in this case because they aimed farther away from the posterior cortical and the intercondylar notch, respectively, as they advanced. Finally, the tunnel lengths from the entry point to the point nearest to the posterior cortical and the intercondylar notch, respectively, were recorded. The minimum longitude for each tunnel trajectory to be considered was 25 mm. Axial, coronal and sagittal views were combined with the Radiant DICOM Viewer imaging software, and the point with the shortest distance that matched the three planes was obtained.
Statistical analysis
Statistical processing was realized using SPSS (version 23.0.0; IBM Corp). Means and standard deviations were calculated for each continuous variable. Two-way repeated-measures analyses of variance (ANOVA) were used to compare the dependent variables obtained from the mean values of shortest distance to the ACL socket and closest cortical, across the independent categorical variables of the four different angles of ALL tunnel orientation. Tukey post hoc comparisons were performed; statistical significance was set at P < 0.05. A power calculation for a two-way analyses of variance test including a four-level categorical independent variable with a significance level of 5% has a power of 81% to detect mean value differences in continuous dependent variables with a sample size of ten cadaveric knees. Reliability analysis was performed using the intraclass correlation coefficient for a two-way mixed absolute agreement model with a 95% confidence interval.
Results
Using a starting point located posterior and proximal to the lateral epicondyle as the anatomic femoral attachment for the ALL reconstruction combined with an anatomic femoral ACL socket of 30 mm in length and 8 mm in diameter showed that none of the four trajectories presented direct contact with the ACL tunnel. Note that the measurements were made from the centre of the trajectory to the outer margin of the ACL tunnel, so that in case of the use of an interference screw for fixating the ALL, half of the screw diameter should be subtracted from these values, e.g. 4 mm with an 8-mm screw.
The two orientations with the shortest measurements to the ACL tunnel were 0° axial/0° coronal (11.5 mm SD ± 5.3) and 30° axial/0° coronal (11.1 mm SD ± 5.6). The two orientations that presented the longest distance were 0° axial/30° coronal (18.6 mm SD ± 6.7) and 30° axial/30° coronal [17.3 mm SD ± 6.1 (P = 0.01)]. The mean ALL tunnel lengths to reach this ACL nearest point measured from the entry point were 15.1 mm SD ± 6.1 (0° axial/0° coronal), 23.1 mm SD ± 5.6 (0° axial/30° coronal), 14.5 mm SD ± 5.2 (30° axial/0° coronal) and 23.2 mm SD ± 3.7 (30° axial/30° coronal).
However, both 0° axial/0° coronal and 0° axial/30° coronal presented specimens on which the trajectory disrupted the posterior femoral cortex (Fig. 2). The main shortest distance measured from these two trajectories to the posterior cortex was 3.1 mm SD ± 2.8 and 3.7 mm SD ± 2.2, respectively (P = 0.01), presenting a high risk of cortical disruption, especially for the use of an interferential screw. The mean ALL tunnel lengths to reach this nearest point were 24.6 mm SD ± 7.1 (0° axial/0° coronal) and 26.3 mm SD ± 7.5 (0° axial/30° coronal).

Computed tomography images of a right knee. a Sagittal cut at the level of lateral condyle showing the trajectory of the radiopaque strands angled at 0° axial/0° coronal and 0° axial/30° coronal (arrows) passing in very close proximity to the posterior femoral cortex. The ACL tunnel maintains a safe distance. b Axial cut at the level of the 0° axial/0° coronal angled trajectory shows the radiopaque strand (arrow) making contact with the posterior femoral cortex
The shortest distances measured from the two inferior trajectories to the intercondylar notch were 11.5 mm SD ± 3.8 (0° coronal/30° axial) and 10.2 mm SD ± 3.1 (0° coronal/0° axial) with mean tunnel lengths to reach this nearest point of 28.9 mm SD ± 3.3 and 27.8 mm SD ± 3.1, respectively. The mean orientation of the ACL tunnel was 44.3° SD ± 9.2 in the sagittal plane and 42.4° SD ± 8.3 (Table 1).
From these results, it should be noted that although the two orientations that maintained 0° axial orientation guarded a safe distance to the ACL socket, they presented a high risk of disrupting the posterior femoral cortical bone.
From the other two orientations aimed at 30° anterior in the axial plane, both maintained a safe distance to the ACL socket with the longest being the 30° axial/30° coronal trajectory aiming away from the ACL tunnel and the posterior femoral cortex.
Finally, the interobserver ICC obtained was considered high (0.92) and the actual angles of the ALL drilled tunnels were in the range ± 6° of the intended angles in all cases.
Discussion
The most important findings of this study were that the four angle orientations tested in this design did not produce any collision and maintained a safe distance to the ACL socket. Although collision with the ACL tunnel did not occur, an important finding was that both tunnels with the angles at 0° in the axial plane presented a very short distance to the posterior femoral cortex, with a direct cortex disruption being observed in 20% of the specimens.
This finding may be observed because the anatomic position of the ALL femoral footprint [17] located superior and posterior to the epicondyle places the origin of the femoral tunnel on a plane above the intercondylar notch but closer to the posterior femoral cortex; therefore, tunnel angulations of 0° in the axial plane should be avoided.
Regarding the coronal plane, the ALL femoral tunnel may be angled at either 0° or 30°, which both showed safe distance to the ACL tunnel and no cortical disruption. The 30° angle is perhaps the better option because of the longer safe distance and also less risk of an intraarticular exit point when using a guidewire technique to pull the tendon graft from the opposite side.
Recently, increased scientific and clinical interest in ALL reconstruction techniques has been observed. Following the increased knowledge of the ALL anatomy and biomechanics, it was recommended to drill the ALL tunnel in a position corresponding to its femoral footprint located proximal and posterior to the lateral epicondyle and LCL insertion site.
When describing a multiligamentary reconstruction technique, there is always the recommendation of taking care of the tunnel orientation to avoid unintended contact either with each other or the outer cortical bone to prevent any possible loss of graft fixation, graft impairment or bone weakening, but these studies rarely present detailed information about the safest angle for the tunnels. Few studies have evaluated the risk of tunnel collision when different ligaments are being reconstructed simultaneously in the knee. Given that ALL reconstruction is a relatively new technique, there is only one prior recent study to our knowledge, conducted by Smeets et al., that addresses the safety of the ALL anatomic femoral tunnel orientation [19]. In their results, these authors found that the safest ALL tunnel orientation is the one oriented proximal and anterior, confirming our findings. However, converse to our study, a high risk of tunnel convergence when using a 0° coronal and 20° axial angle was reported. Given that both studies were comparable in design, one explanation could be that our study probably used a higher starting point for the ALL tunnel as theirs described a starting point just superior and posterior to the lateral epicondyle. In our study, data regarding measurements to the posterior cortical bone and to the intercondylar notch were also included. Either way, both studies concluded that the safest orientation for the ALL tunnel should be in an anterior and superior direction.
Some authors described a single femoral tunnel technique using a single graft for reconstructing the ACL and the ALL [21] and eliminating the concern of tunnel collision. However, this technique has its limitations regarding the graft length needed and may not be suited for some revision cases. In addition, other authors [8, 15] also described the use of the anatomic ALL femoral attachment site for the femoral fixation site when performing the lateral extra-articular tenodesis (LET) procedure.
The clinical relevance of this study is that it provides insight into the knowledge gap regarding tunnel positioning during simultaneous ACL and ALL reconstruction. The results showed that an ALL anatomical reconstruction does not represent a risk when performing a simultaneous ACL reconstruction as long as the ALL tunnel is reamed with a proximal and anterior angulation.
This study has some limitations. First, only one specific ALL reconstruction technique was performed, although graft fixation with an interference screw in the described femoral attachment site is commonly performed in the clinical setting. Second, only four different angles were included so they were thought as representative of each quadrant to ease evaluation. Third, no actual tunnels were drilled because it would be impractical to perform simultaneous measurements destroying the bone in a small space; therefore, we used only thin trajectories representing the centre of a tunnel. However, calculations can be made by subtracting half of the diameter of any given diameter to any distance measurement. Finally, the angulations during the procedure were calculated only with the help of a manual goniometer. This method might provide low accuracy, but it was intended to mimic the clinical situation during a common surgery scenario.
Conclusions
When performing combined ACL and ALL ligament reconstruction surgery, the ALL femoral tunnel should be drilled with an angle of 30° anterior in the axial plane and 30° proximal in the coronal plane. This tunnel may also be angled 0° in the coronal plane with a shorter but still safe distance to the ACL. Although the tunnels with an angle of 0° in the axial plane maintained a safe distance to the ACL socket, they showed a high risk of contact and disruption of the posterior femoral cortex; thus, these angles should be avoided.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- ALL:
-
Anterolateral ligament
- LCL:
-
Lateral collateral ligament
- AL:
-
Anterolateral
- AM:
-
Anteromedial
- AAM:
-
Accessory anteromedial
- CT:
-
Computed tomography
- ANOVA:
-
Analyses of variance
- LET:
-
Lateral extra-articular tenodesis
- IC:
-
Intercondylar notch
- PC:
-
Posterior femoral cortex
- IRB:
-
Institutional Review Board
- ICC:
-
Intraclass correlation coefficient
References
Ardern CL, Webster KE, Taylor NF, Feller JA (2011) Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med 45:596–606
Camarda L, D’Arienzo M, Patera GP, Filosto L, LaPrade RF (2011) Avoiding tunnel collisions between fibular collateral ligament and ACL posterolateral bundle reconstruction. Knee Surg Sports Traumatol Arthrosc 19:598–603
Camarda L, Grassedonio E, Lauria M, Midiri M, D’Arienzo M (2016) How to avoid collision between PCL and MCL femoral tunnels during a simultaneous reconstruction. Knee Surg Sports Traumatol Arthrosc 24:2767–2772
Claes S, Vereecke E, Maes M, Victor J, Verdonk P, Bellemans J (2013) Anatomy of the anterolateral ligament of the knee. J Anat 223:321–328
Daggett M, Busch K, Sonnery-Cottet B (2016) Surgical dissection of the anterolateral ligament. Arthrosc Tech 5:e185–e188
Daggett M, Ockuly AC, Cullen M, Busch K, Lutz C, Imbert P, Sonnery-Cottet B (2016) Femoral origin of the anterolateral ligament: an anatomic analysis. Arthroscopy 32:835–841
DePhillipo NN, Cinque ME, Chahla J, Geeslin AG, LaPrade RF (2017) Anterolateral ligament reconstruction techniques, biomechanics, and clinical outcomes: a systematic review. Arthroscopy 33:1575–1583
Ferretti A, Monaco E, Fabbri M, Mazza D, De Carli A (2017) The fascia lata anterolateral tenodesis technique. Arthrosc Tech 6:e81–e86
Geeslin AG, Moatshe G, Chahla J, Kruckeberg BM, Muckenhirn KJ, Dornan GJ, Coggins A, Brady AW, Getgood AM, Godin JA, LaPrade RF (2018) Anterolateral knee extra-articular stabilizers: a robotic study comparing anterolateral ligament reconstruction and modified Lemaire lateral extra-articular tenodesis. Am J Sports Med 46:607–616
Gelber PE, Erquicia JI, Sosa G, Ferrer G, Abat F, Rodriguez-Baeza A, Segura-Cros C, Monllau JC (2013) Femoral tunnel drilling angles for the posterolateral corner in multiligamentary knee reconstructions: computed tomography evaluation in a cadaveric model. Arthroscopy 29:257–265
Gelber PE, Masferrer-Pino À, Erquicia JI, Abat F, Pelfort X, Rodriguez-Baeza A, Monllau JC (2015) Femoral tunnel drilling angles for posteromedial corner reconstructions of the knee. Arthroscopy 31:1764–1771
Getgood A, Brown C, Lording T, Amis A, Claes S, Geeslin A, Musahl V, ALC Consensus Group (2018) The anterolateral complex of the knee: results from the International ALC Consensus Group Meeting. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-018-5072-6
Helito CP, Bonadio MB, Gobbi RG, da Mota E, Albuquerque RF, Pécora JR, Camanho GL, Demange MK (2016) Is it safe to reconstruct the knee anterolateral ligament with a femoral tunnel? Frequency of lateral collateral ligament and popliteus tendon injury. Int Orthop 40:821–825
Inderhaug E, Stephen JM, Williams A, Amis AA (2017) Anterolateral tenodesis or anterolateral ligament complex reconstruction: effect of flexion angle at graft fixation when combined with ACL reconstruction. Am J Sports Med 45:3089–3097
Inderhaug E, Stephen JM, Williams A, Amis AA (2017) Biomechanical comparison of anterolateral procedures combined with anterior cruciate ligament reconstruction. Am J Sports Med 45:347–354
Katakura M, Koga H, Nakamura K, Sekiya I, Muneta T (2017) Effects of different femoral tunnel positions on tension changes in anterolateral ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 25:1272–1278
Kennedy MI, Claes S, Fuso FAF, Williams BT, Goldsmith MT, Turnbull TL, Wijdicks CA, LaPrade RF (2015) The anterolateral ligament: an anatomic, radiographic, and biomechanical analysis. Am J Sports Med 43:1606–1615
Samuelson M, Draganich LF, Zhou X, Krumins P, Reider B (1996) The effects of knee reconstruction on combined anterior cruciate ligament and anterolateral capsular deficiencies. Am J Sports Med 24:492–497
Smeets K, Bellemans J, Lamers G, Valgaeren B, Bruckers L, Gielen E, Vandevenne J, Vandenabeele F, Truijen J (2018) High risk of tunnel convergence during combined anterior cruciate ligament and anterolateral ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-018-5200-3
Sonnery-Cottet B, Daggett M, Fayard J-M, Ferretti A, Helito CP, Lind M, Monaco E, de Pádua VBC, Thaunat M, Wilson A, Zaffagnini S, Zijl J, Claes S (2017) Anterolateral Ligament Expert Group consensus paper on the management of internal rotation and instability of the anterior cruciate ligament-deficient knee. J Orthop Traumatol 18:91–106
Zein AMN, Ali M, Ali H, Saleh Elsaid AN, Mahmoud AZ, Osman MK, Mohamed Soliman AM (2017) Combined anatomic reconstruction of the anterior cruciate and anterolateral ligaments using hamstring graft through a single femoral tunnel and with a single femoral fixation. Arthrosc Tech 6:e567–e577
Funding
The authors declare that no funding was received to perform this study.
Author information
Authors and Affiliations
Contributions
CJ designed the study, carried out the anatomic dissection, arthroscopy procedures, and femoral tunnel placement and drafted the manuscript. JP carried out the image analysis and CT measurements. SS participated in the study design and coordination between departments. DG participated in the anatomic dissection, data gathering and performed the statistical analysis. ML participated in the coordination with the university and helped with the arthroscopy procedures. AC participated in the coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was performed after ethical approval from the Institutional Review Board at the Univesity of Barcelona (IRB00003099).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jette, C., Pomés, J., Sastre, S. et al. Safe drilling angles avoid femoral tunnel complications during combined anterolateral ligament and anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 27, 3411–3417 (2019). https://doi.org/10.1007/s00167-019-05388-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05388-4