
Abstract
Purpose
Glenohumeral range of motion adaptations may affect throwing athletes and contribute to shoulder injury. The purpose of this study was to evaluate shoulder rotation deficits among elite professional handball players and its correlation to the presence of shoulder pain and morphological changes.
Methods
Eighty-seven elite professional handball players and 41 healthy non-athlete volunteers participated in the study. Evaluations included measurement of range of internal and external rotation, total arch of motion, identification of shoulder pain and ultrasound scan for diagnosis of rotator cuff tears and internal impingement.
Results
Glenohumeral rotational deficits (>20–25°) were found among 11 players group (13%). The throwing shoulders in the players group showed a decrease in internal rotation and an increase in external rotation with significantly larger ranges among players compared to the non-athlete group. Internal rotation deficit >20° was associated with higher incidence of shoulder pain among players. Both internal rotation deficits (>25°) and total arch of motion deficit (>20°) co-existed with higher incidence of internal impingement. Shoulder pain was common (36/97–41%) and was associated with decreased external rotation and total arch of motion. Internal impingement (found in 13/87–15%) correlated with decreased rotation ranges and a greater deficit in total arch of motion, whereas higher gain in external rotation correlated with a partial rotator cuff tear (found in 12/87–14%).
Conclusions
Shoulder pathologies and problems commonly affected the group of handball players. Greater glenohumeral rotational deficits in throwing shoulders of handball players correlate with shoulder pain and internal impingement, while increased external rotation with partial rotator cuff tears. Such deficits affect 13% of the athlete population. Major clinical relevance of the study is to monitor handball players’ shoulders both clinically and by proper imaging. Evaluation of range of rotation seems to identify shoulders at risk of the pathology.
Level of evidence
Cross-Sectional study with control group, Level II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The phenomenon of decreased shoulder internal rotation in overhead athletes’ throwing shoulder, has been termed glenohumeral internal rotation deficit (GIRD) [2, 3, 15, 20, 32]. A majority of the current literature has been based on baseball players. Handball, in comparison, is a very explosive, contact overhead sport, associated with multiple collisions, frequent direction changes and various techniques of throwing [12, 23, 30]. Epidemiology data show high prevalence of injury and self-reported shoulder pain [10, 23]. It has been suggested that athletes with GIRD >20° have twice as high an incidence of shoulder injury [3, 14]. On the other hand, Clarsen et al. have not found any association between injury and any internal rotation deficit [15]. It is also not very clear as to what is the incidence of GIRD among players and non-players. In general, the concept of pathological events of the throwing shoulder resulting in tissue compromise (internal impingement, fibrosis, rotator cuff tears) is well accepted. However, we have not yet found reliable studies which link morphological changes to rotational shoulder parameters, especially in handball players.
It has been hypothesized that shoulder pain and morphologic abnormalities detected by an ultrasound scan are associated with rotational profile deficits of the shoulder. There were several aims to the study. First, to compare shoulder rotation ranges and deficits between elite professional handball players and a control group of healthy non-athletes. Second, to assess the frequency of rotational deficits among the tested populations. Third, to correlate rotational shoulder properties to the presence of shoulder pain and morphological changes found on shoulder ultrasound scan. To our best knowledge, our study is the first to explore and find the association between shoulder pathologies in tissue morphology and various magnitudes of GIRD. It is also the first one to explore incidence of various magnitudes of GIRD among throwing athletes and relating to non-throwing population.
Materials and methods
This is a cross-sectional study (level II) in a group of Polish male elite professional handball players.
Participants
Study material was based on both professional handball players and control group of non-athletes. Eighty-seven elite professional male handball players from four Super League (the first Polish division) teams and one team from the first League (the second Polish division) were enrolled to the study. All the players were full-time professionals. Their typical training schedule included a 2-h session a day, 4–5 times a week. In addition, they played a competitive match every weekend during this period. The dominant shoulder was defined as the shoulder used to throw. All tests (described in detail below) were performed during the off-season, and none of the participants included in the study had any recent or current disabling shoulder injury or condition.
Forty-one healthy non-athlete volunteers were included in the control group based on the following inclusion criteria: age 20–30; no history of shoulder injury, surgery, pain and/or dysfunction; and no history of professional sport participation. The average age in the players group was 25 years (SD 4.7, range 18–38), height was 188 cm (SD 6, range 175–202) and weight was 92 kg (SD 11, range 64–125 kg). The right shoulder was dominant in 68 participants and the left one in 19. The average age of the control group was 25 years (SD 1, range 20–24), height was 181 cm (SD 5.1, range 174–189) and weight was 77.9 kg (SD 12.7, 61–105). The right shoulder was dominant in 38 and left in 3 participants. There was no difference in age between the groups. However, height and weight were significantly higher in the players group compared to the control group (p < 0.0001).
Study protocol
The study protocol included: measurement of shoulder range of internal rotation (IR) and external rotation (ER), registration of existing throwing shoulder pain and a shoulder ultrasound examination to assess for possible rotator cuff tears and posterior internal impingement.
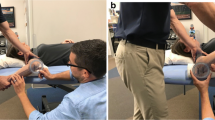
Measurements of range of shoulder rotation were performed with the participant lying in a supine position, having the shoulder abducted to 90° and the elbow flexed to 90°. Measurements were made in a passive mode. Two examiners (PK and PC) performed the evaluation. Shoulder rotation was established both visually and manually by one examiner, while the scapula was stabilized to elicit pure glenohumeral motion. The other examiner recorded the angle of rotation using a goniometer with the centre of rotation placed at the olecranon tip. One arm of the goniometer was placed along the axis of the ulna and the other perpendicular to the ground. Further calculations included total arch of motion (TAM—total of ER and IR), deficit of internal rotation (GIRD—difference of IR between non-dominant and dominant shoulders), total arch of motion deficit (TAMD—difference of TAM between non-dominant and dominant shoulders), external rotation gain (ERG—difference of ER between dominant and non-dominant shoulders), and total arc of motion gain (TAMG—difference of TAM between dominant and non-dominant shoulders).
Pilot study has been performed to evaluate the reliability of measurements in the first 20 control-group participants. Intraclass correlation coefficient was very high: 0.99 for IR and ER both within the raters and between the raters (at p < 0.0001 for both correlations).
Shoulder pain
The presence of shoulder pain was established as reported by participants when the pain level was at least 2 in the 0–10 visual analogue scale, which occurred for the duration of at least 1 week within the last month of playing.
Ultrasound scan
An ultrasound evaluation was performed by an experienced musculoskeletal radiologist, using the 5–12-MHz linear transducer (HD11 XE system, Phillips Ultrasound, Andover, MA, USA). The scan was preformed to screen for morphological changes including: rotator cuff integrity, presence of posterior internal impingement, possible changes in long head of the biceps, bursitis, inflammation of acromioclavicular joint. Postero-superior impingement was dynamically examined in the ABER position with diagnosis criteria including humeral head anterior translation with the posterior surface of the greater tuberosity facing the postero-superior glenoid rim and the interposition of the articular side of the rotator cuff in-between.
The study was approved by the Ethical Committee of the University of Medical Sciences in Poznan (962/11). All participants were informed about the purpose and study procedures. Informed consent was obtained from all individual participants included in the study.
Statistical analysis
Statistical analysis was performed using Statistica 10 software (StatSoft) and included power analysis, normality tests (Shapiro–Wilk), parametric (T student) and non-parametric tests (Mann–Whitney). A Fisher’s exact test had been applied to compare frequencies between specific subgroups. The level of significance was set at p < 0.05. Power analysis and sample size were calculated for IR, ER and TAM. The power was 0.9 for all and the size of valid sample was determined to be 37, 27 and 33, respectively.
Results
The throwing shoulder in the handball group showed a statistically significant decrease in IR and increase in ER, when compared to the opposite shoulder (Fig. 1). No such difference could be noted for the control group. Handball players revealed significantly higher ranges of IR and ER as well as TAM compared to the control group. Average IR deficit among handball players was statistically significantly larger than in control group. Neither the TAMD nor ERG showed statistically significant differences between the study groups.

Results of shoulder rotation ranges and deficits and gains among handball players and control group. Numbers over the top of the bars represent the average values; arrows with p values above represent statistical comparisons between particular values of handball and control groups (non-parametric Mann–Whitney test). Handball players’ results have been depicted by black bars and control group’s by the white bars. ERG external rotation gain, GIRD glenohumeral internal rotation deficit, HB handball, TAMD total arch of motion deficit
The incidence of pain in the throwing shoulder was 36 out of 87 handball players (41%).
An ultrasound scan revealed articular-side partial-thickness rotator cuff tear (RCT) in 12 out of 87 (14%) handball players, and postero-internal impingement in 13 out of 87 (15%). No such changes were detected in the opposite shoulders. There was no statistical difference for the incidence of pain related to the presence of RCT (painful RCT—54% vs. painless RCT—46%) nor any difference related to internal impingement (painful internal impingement—62% vs. painless internal impingement—38%). Incidence of RCT was not related to the presence of internal impingement. Other ultrasonographic abnormalities included subacromial bursitis (n = 3) and acromioclavicular degeneration (n = 2), and long head of the biceps tendinitis (n = 1). Ultrasound evaluation of the control group did not reveal any shoulder abnormalities.
Shoulder pain was associated with decreased ER and TAM. Internal impingement was accompanied by decreased ranges of rotations (IR, ER, and TAM) and larger TAMD (Table 1). There was increased ER in players diagnosed with a partial RCT.
Only larger deficits have been significantly associated with shoulder symptoms (Table 2). Shoulder pain was more common in players with GIRD >20°, and internal impingement was more common with GIRD >25° or TAMD >20°. Both increased ER and TAM co-existed with a higher prevalence of partial RCT.
The incidence of GIRD and TAMD decreased with higher range of deficits (Table 3). No statistically significant difference has been found between the incidence of GIRD and TAMD between the athletes and the control groups. The only difference close to significance was for GIRD >5° to be more frequent among handball players (p = 0.08). Incidence of ERG and TAMG was very similar between the groups.
Discussion
The most important finding of the present study was that larger rotational deficits (GIRD higher then 20°–25° or TAMD larger then 20°) co-existed with shoulder pain and postero-superior internal impingement, while external rotational gain with partial rotator cuff tears. However, several other important observations have been made. The results of this study show that the handball players group had significantly higher ranges of both IR, ER and TAM compared to the control group. There was a typical pattern of decreased IR (by 6°) and increased ER (by 4°) among athletes, compensating for total range of rotation. This adaptive phenomena, not seen in the control group, have been observed before [1, 29, 31] and are explained by soft tissue [8, 9, 32] and osseous adaptations [22, 26]. Ranges of rotation span as reported among different throwing sports, with IR of 20°–77°, ER 92°–142° and TAM 140°–216°; higher values had mostly been recorded among baseball pitchers [7, 8, 24, 25]. Lower ranges of ER and TAM among handball players, as suggested by Clarsen at al., could be attributed to the specificity and diversity of throwing techniques comparing to other sports [1, 5, 28]. Other factors could also have impact on different rotational ranges, such as: measurement techniques, time of season, age, injury, type of sport, pain or even climate [8, 13, 15, 32].
Incidence of pain in the throwing shoulder was 41% in the handball group. Shoulder problems and pain have been reported by handball players in relatively high numbers (32–52%), leading to absence from the game in 36% of cases or forcing them to modify training in 68–75% [1, 5, 23]. Therefore, it has been suggested that shoulder pain should warrant undertaking special measures, including injury and overuse monitoring during both training, matches and tournaments, and implementing prevention strategies [4, 29].
The ultrasound scans revealed partial-thickness articular-sided supraspinatus tendon tear in 12 players (14%), and internal impingement of the postero-superior cuff in 13 (15%). It has been shown by Jost at al., that 70% of handball playes have been affected by partial rotator cuff tears and 37% of them by postero-superior internal impingement [11]. Those numbers are much higher than in our study. The difference may be due to different study population (age of 27, vs. age of our group- 25), but also due to different imaging modality (MRI vs. ultrasound).
As this study showed, abnormalities were not predictors of pain. Less frequent pathologies were found in the study by Halbrecht at al.: postero-superior labral tears in 30% and partial tears in 40% of throwing baseball players [9]. Similar findings were also shown by Tehranzadeh et al. [27]. As in our study, these changes were not seen in contralateral shoulders.
Shoulder pain in the throwing shoulder may be attributed to various reasons, including pathological internal impingement, RCT, fatigue, labral tears, scapular dyskinesis and instability, etc. [14, 18, 20]. Shoulder pathologies identified in our handball group were associated with specific rotational parameters. Players suffering from shoulder pain presented with decreased ER and TAM. Postero-superior internal impingement was associated with decreased IR, ER and TAM, as well as larger TAMD. Partial RCT was accompanied by greater ER and TAMG. Routolo et al. reported a decrease in IR, ER and TAM associated with pain in baseball players [25]. Previous season shoulder pain in baseball pitchers did not affect rotational ROM but, however, was associated with posterior shoulder musculature weakness [29]. Contrary to our results, Almeida at al. have shown handball players with current pain to have decreased IR and increased ER, with no difference in TAM in the throwing arm [1]. One explanation would be that current shoulder pain affects shoulder rotational range. The occurrence of tears co-existed with increased ER. It may be suggested that an RCT may be a pathological effect of the gain in external rotation caused by the throwing. Asymptomatic tears do not usually need any intervention. However, the young and active sport population should be regularly followed clinically and by imaging, since asymptomatic lesions may convert into chronic pain [33]. Another aspect is that supraspinatus tears (even asymptomatic) lead to a decrease in strength parameters [19].
Based on the literature, no studies could be found to be correlating rotational parameters with morphologic abnormalities. One exception is the work by Burkhart et al., reporting unpublished data in which players with type II SLAP lesions would have a GIRD of more than 25° [3]. Tehranzadeh et al., reported MRI evaluation of 6 cases with clinical and arthroscopic manifestations of GIRD, found partial RCT, superoposterior subluxation of the humeral head and SLAP tears [27].
Contact between the rotator cuff and the postero-superior glenoid and labrum is considered to be physiologic [9]; however, such contact is very intense in the late cocking phase of throwing and may result in a whole range of possible pathologies, including RCT, SLAP tears, chondral erosions, and capsular injuries. [5, 9, 18]. Myers et al. found greater GIRD and posterior shoulder tightness with internal impingement in throwers [22]. No such effect on GIRD was shown in our study; however, the handball group revealed a decrease of IR, ER and TAM as well as larger TAMD. A possible explanation is that these findings reflect capsular- and/or muscular-related glenohumeral rotational stiffness.
The amount of GIRD that is clinically relevant is debatable. Burkhart et al. have suggested that GIRD >25° is associated with SLAP tears [3]. Myers at al. have found that throwers with internal impingement have an average GIRD of 19° [22]. Wilk at al. did not find a significant difference between injured and non-injured patients with GIRD [31]; however, TAMD >5° was associated with higher risk of shoulder injury. Ruotolo et al. has reported a 10° TAMD, and 14° GIRD for painful pitching shoulder in baseball players, as compared to 1° and 9°, respectively, for non-painful ones [25]. On the other hand, Clarsen et al. did not find any association between injury and any rotational deficits in elite handball players [5]. Our study showed that shoulder pain was more common (67 vs. 37%) when the IR deficit was over 20°. Postero-superior internal impingement was more frequent when GIRD was over 25° (50 vs. 13%) or TAMD was over 20° (43 vs. 13%).
The incidence of GIRD among the throwers has not been commonly and clearly reported. As had been shown in our study, greater deficits have less frequent occurrence (ranging from 61% for any GIRD to 2% for GIRD >25°) in the handball group. Other studies have reported a GIRD incidence of 5–40% [5, 26, 31]. Interestingly, Dwelly et al. have shown a changing incidence of any GIRD throughout the season (pre-fall 21%, pre-spring 3% and post-spring 14%) in baseball players [7]. Wilk at al. found TAMD >5° to be a significant marker of shoulder injury [31].
Several important clinical observations were made based on the current study. First of all, it was confirmed that handball players complain commonly on shoulder pain and discomfort despite being able to continue and play. The throwing shoulder in that group is most commonly affected by internal impingement. That does not occur in the non-throwing shoulder and non-throwing population. This young population is already at 14% risk of rotator cuff pathology. The most important finding is that larger rotational glenohumeral deficits are associated with pathologies like internal impingement or pain and increased ER with rotator cuff tear. Such deficits affected 13 and 6% (respectively) of our athletes (only 2% in control group for both GIRD and TAMD). This illustrates that although not every athlete is at risk, a significant number are. Therefore, this population should be monitored more closely by the medical team with the consideration of introducing preventive and therapeutic measures [4, 16, 17, 21]. Several studies suggest introducing an injury risk modification program. Laudner at al. have found that a stretching program has a profound effect on internal rotation among baseball players [16]. Consistent participation in internal rotation stretching programs may improve both IR and TAM among professional pitchers [17].
There are several limitations to this study. One is that various athletes playing at different positions may have different ROM and GIRD due to the diversity of throwing mechanisms in different positions. Differentiating this variable was not possible due to small numbers in each position subgroup. Another potential weakness is that there may also be other variables that have not been analysed, such as years of playing and different timings of examination throughout the season. Another weakness lies in the comparison between an elite professional athletic population and the non-athlete population—a non-matched comparison—with the related anthropometric differences. Athletes were taller and weigh more. Height and weight would not be possible and easy to match due to different body structure in the sports population. It may also be argued that MR might be more accurate to diagnose shoulder pathology. Ultrasound scan has been chosen in our study as imaging modality because of its established value in the evaluation of the shoulder. As analysed by de Jesus at al., its sensitivity and specificity in detecting rotator cuff abnormalities is comparable to MRI, provided that it is performed by a specialized musculoskeletal radiologist [6]. The US scan also allows for dynamic evaluation (internal impingement). Using the scan is a common practice. The aim was also to provide a good and simple assessment algorithm that could be repeated in any outpatient clinic.
The results of the study show that handball players are at the risk of the shoulder injury and pain. The exact mechanism is not known but adaptive changes in rotation movement may play the role. Since larger rotational deficits that develop in the throwing shoulders co-exist with various pathologies, medical team should routinely monitor shoulder function clinically and consider proper imaging to detect pathology. Evaluation of range of rotation seems to identify shoulders at risk of the pathology.
Conclusions
Handball players showed typical shoulder adaptation with increased external rotation and decreased internal rotation, with greater ranges of rotation compared to the non-athlete control group. Shoulder pathology was a common finding, however, not always symptomatic. Larger rotational deficits (GIRD higher then 20–25° or TAMD larger then 20°) co-existed with shoulder pain and postero-superior internal impingement, while external rotational gain with partial rotator cuff tears.
Author contribution statement
PL: group leader, conception and design, analysis, writing most of the manuscript. PK: conception, design, acquisition of data (clinical part), analysis, evaluation of handball players. PC: conception and design, acquisition of data, clinical part, evaluation of handball players. EB: conception and design, acquisition of data, clinical part, evaluation of control group. MG: revision of paper, part of manuscript, important intellectual content, statistical analysis, MD: acquisition of data (radiological part), analysis. TK: acquisition of data (radiological part), analysis. LL: involved in drafting the manuscript or revising it critically for important intellectual content, general supervision. LR: involved in drafting the manuscript or revising it critically for important intellectual content, general supervision.
Abbreviations
- GIRD:
-
Glenohumeral internal rotation deficit
- ER:
-
External rotation
- ERG:
-
External rotation gain
- D:
-
Dominant
- IR:
-
Internal rotation
- MRI:
-
Magnetic resonance imaging
- ND:
-
Non-dominant
- RCT:
-
Rotator cuff tear
- ROM:
-
Range of motion
- SD:
-
Standard deviation
- SLAP:
-
Superior labral anterior to posterior tear
- TAM:
-
Total arch of motion
- TAMD:
-
Total arch of motion deficit
- TAMG:
-
Total arch of motion gain
- US:
-
Ultrasound scan
References
Almeida GP, Silveira PF, Rosseto NP, Barbosa G, Ejnisman B, Cohen M (2014) Glenohumeral range of motion in handball players with and without throwing-related shoulder pain. J Shoulder Elbow Surg 22:602–607
Burkhart SS, Morgan CD, Kibler WB (2003) The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy 19:404–420
Burkhart SS, Morgan CD, Kibler WB (2003) The disabled throwing shoulder: spectrum of pathology. Part II: evaluation and treatment of SLAP lesions in throwers. Arthroscopy 19(5):531–539
Casáis L, Martínez M (2012) Intervention strategies in the prevention of sports injuries from physical activity; In: KR Zaslav (ed) An International Perspective on Topics in Sports Medicine and Sports Injury. InTech, Rijeka, pp 355–378
Clarsen B, Bahr R, Andersson SH, Munk R, Myklebust G (2014) Reduced glenohumeral rotation, external rotation weakness and scapular dyskinesis are risk factors for shoulder injuries among elite male handball players: a prospective cohort study. Br J Sports Med 48(17):1327–1333
de Jesus JO, Parker L, Frangos AJ, Nazarian LN (2009) Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: a meta-analysis. Am J Roentgenol 192:1701–1707
Dwelly PM, Tripp BL, Tripp PA, Eberman LE, Gorin S (2009) Glenohumeral rotational range of motion in collegiate overhead-throwing athletes during an athletic season. J Athl Train 44:611–616
Ellenbecker TS, Roetert EP, Bailie DS, Davies GJ, Brown SW (2002) Glenohumeral joint total rotation range of motion in elite tennis players and baseball pitchers. Med Sci Sports Exerc 34(12):2052–2056
Halbrecht JL, Tirman P, Atkin D (1999) Internal impingement of the shoulder: comparison of findings between the throwing and nonthrowing shoulders of college baseball players. Arthroscopy 15:253–258
Hoeberigs J, van Galen W, Philipsen H (1986) Pattern of injury in handball and comparison of injured versus noninjured handball players. Int J Sport Med 7:333–337
Jost B, Zumstein M, Pfirrmann CW, Zanetti M, Gerber C (2005) MRI findings in throwing shoulders: abnormalities in professional handball players. Clin Orthop Relat Res 434:130–137
Kaczmarek P, Lubiatowski P, Cisowski P, Grygorowicz M, Łepski M, Długosz, J, Romanowski L (2014) Shoulder problems in overhead sports. Part I—biomechanics of throwing. Pol Orthop Traumatol 15(79): 50–58
Kaplan KM, Elattrache NS, Jobe FW et al (2011) Comparison of shoulder range of motion, strength, and playing time in uninjured high school baseball pitchers who reside in warm- and cold-weather climates. Am J Sports Med 39:320–328
Kibler WB, Kuhn JE, Wilk K, Sciascia A, Moore S, Laudner K, Uhl T (2013) The disabled throwing shoulder: spectrum of pathology-10-year update. Arthroscopy 29:141–161
Kibler WB, Sciascia A, Thomas SJ (2012) Glenohumeral internal rotation deficit: pathogenesis and response to acute throwing. Sports Med Arthrosc 20:34–38
Laudner KG, Sipes RC, Wilson JT (2008) The acute effects of sleeper stretches on shoulder range of motion. J Athl Train 43:359–363
Lintner D, Mayol M, Uzodinma O, Jones R, Labossiere D (2007) Glenohumeral internal rotation deficits in professional pitchers enrolled in an internal rotation stretching program. Am J Sports Med 35:617–621
Lintner D, Noonan TJ, Kibler WB (2008) Injury patterns and biomechanics of the athlete’s shoulder. Clin Sports Med 27:527–551
Lubiatowski P, Kaczmarek P, Dzianach M, Ogrodowicz P, Bręborowicz M, Długosz JD, Romanowski L (2013) Clinical and biomechanical performance of patients with failed rotator cuff repair. Int Orthop 37:2395–2401
Lubiatowski P, Kaczmarek PK, Ślęzak M, Długosz J, Bręborowicz M, Dudziński W, Romanowski L (2014) Problems of the glenohumeral joint in overhead sports—literature review. Part II—pathology and pathophysiology. Pol Orthop Traumatol 23: 59–66
McConnell J, Donnelly C, Hamner S, Dunne J, Besier T (2012) Passive and dynamic shoulder rotation range in uninjured and previously injured overhead throwing athletes and the effect of shoulder taping. PM R 4:111–116
Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM (2006) Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med 34:385–391
Myklebust G, Hasslan L, Bahr R, Steffen K (2013) High prevalence of shoulder pain among elite Norwegian female handball players. Scand J Med Sci Sports 23:288–294
Nakamizo H, Nakamura Y, Nobuhara K, Yamamoto T (2008) Loss of glenohumeral internal rotation in little league pitchers: a biomechanical study. J Shoulder Elbow Surg 17:795–801
Ruotolo C, Price E, Panchal A (2006) Loss of total arc of motion in collegiate baseball players. J Shoulder Elbow Surg 15:67–71
Shanley E, Thigpen CA, Clark JC, Wyland DJ, Hawkins RJ, Noonan TJ, Kissenberth MJ (2012) Changes in passive range of motion and development of glenohumeral internal rotation deficit (GIRD) in the professional pitching shoulder between spring training in two consecutive years. J Shoulder Elbow Surg 21:1605–1612.
Tehranzadeh AD, Fronek J, Resnick D (2007) Posterior capsular fibrosis in professional baseball pitchers: case series of MR arthrographic findings in six patients with glenohumeral internal rotational deficit. Clin Imaging 31:343–348
Torres RR, Gomes JL (2009) Measurement of glenohumeral internal rotation in asymptomatic tennis players and swimmers. Am J Sports Med 37(5):1017–1023
Trakis JE, McHugh MP, Caracciolo PA, Busciacco L, Mullaney M, Nicholas SJ (2008) Muscle strength and range of motion in adolescent pitchers with throwing-related pain: implications for injury prevention. Am J Sports Med 36:2173–2178
Wagner H, Pfusterschmied J, von Duvillard SP, Müller E (2011) Performance and kinematics of various throwing techniques in team-handball. J Sports Sci Med 10:73–80
Wilk KE, Macrina LC, Fleisig GS, Porterfield R, Simpson CD, Harker P, Andrews JR (2011) Correlation of glenohumeral internal rotation deficit and total rotational motion to shoulder injuries in professional baseball pitchers. Am J Sports Med 39:329–335
Wilk KE, Reinold MM, Macrina LC, Porterfield R, Devine KM, Suarez K, Andrews JR (2009) Glenohumeral internal rotation measurements differ depending on stabilization techniques. Sports Health (London) 1:131–136
Yamaguchi K, Sher JS, Andersen WK, Garretson R, Uribe JW, Hechtman K, Neviaser RJ (2000) Glenohumeral motion in patients with rotator cuff tears: a comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 9:6–11
Acknowledgments
The work was supported by the National Science Center under Grant DEC-2011/01/B/NZ7/03596.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declare that they have no competing interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lubiatowski, P., Kaczmarek, P., Cisowski, P. et al. Rotational glenohumeral adaptations are associated with shoulder pathology in professional male handball players. Knee Surg Sports Traumatol Arthrosc 26, 67–75 (2018). https://doi.org/10.1007/s00167-017-4426-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-017-4426-9