
Abstract
Purpose
Knowledge of the effect of hip pathologies on hip biomechanics is important to the understanding of the development of osteoarthritis, and the contribution of the labrum to hip joint stability has had limited study. The purpose of this study was to evaluate the effect of labral injury to stability of the femoral head in the acetabular socket.
Methods
Ten cadaver hip specimens were tested using a robotic system under four different loading conditions: axial loading (80 N) along the femoral axis and axial loading (80 N) combined with either anterior, posterior or lateral loading (60 N). The hip states were examined were intact, with a 1.5 cm capsulotomy and with a 1 cm resection of the anterosuperior labrum.
Results
At 30° of flexion, under axial load, the displacement of the hip with capsulotomy and labral resection (9.6 ± 2.5 mm) was significantly larger then the hip with capsulotomy alone (5.6 ± 4.1 mm, p = 0.005) and the intact hip (5.2 ± 3.8 mm, p = 0.005). Also, at 30° of flexion, the displacement under combined axial and anterior/posterior load was increased with capsulotomy and labral resection.
Conclusion
The acetabular labrum provides stability to the hip joint in response to a distraction force and combined distraction and translation forces. One centimetre of labral resection caused significant displacement (“wobbling” effect) of the femoral head within the acetabulum with normal range of motion. Successful labral repair could be crucial for restoration of the hip biomechanics and prevention of coxarthrosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Labral tears are the most common cause for intra-articular hip pain in young, non-arthritic patients. Also, most older patients with arthritic changes in the hip have labral tears; however, relation between labral tears and onset of arthritis continues to be unknown. While anatomy of the hip labrum is relatively well described in recent studies [24, 25, 30, 39, 40], its true function has lagged behind.
At the present time, only a limited number of biomechanical studies are available on the contribution of the labrum to the hip joint kinematics [4, 10, 26, 33, 37, 41]. Some studies recognized tears of the labrum as a possible factor leading to coxarthrosis [1, 16, 17, 29, 30]. The labrum resists lateral and vertical motion of the femoral head within the acetabulum by deepening the joint. Selders et al. [34] demonstrated that acetabular labrum increased acetabular volume by 21 % and articular surface area of acetabulum by 28 %. Lubrication of the hip joint is important for normal function, and Terayama et al. [41] demonstrated that under a 1275 N compressive load, there is no direct contact between acetabular and femoral cartilage with approximately 0.4 mm of joint fluid between surfaces. Takechi et al. [38] showed that the labrum provides a seal around the femoral head and restricts fluid flow into and out of articular space. This “suction effect” of the labrum and fluid enhances joint stability and distributes compressive loads between articular surfaces, which reduce peak cartilage stresses during weight bearing [8, 9]. It has been established that labrum plays critical role in cartilage preservation. The overall cartilage creep consolidation under constant load of 0.75 times bodyweight was 21 % greater without a labrum compared to with an intact labrum [9]. Without the labrum, articular cartilage must withstand significantly increased pressure, and a compromise of this system could lead to early joint deterioration and osteoarthritis. Crawford et al. [4] showed that capsular venting and loss of labral “seal” lead to destabilization of the hip at extreme range of motion. The study demonstrated femoral head subluxation approximately 1 mm during the extreme internal rotation manoeuvre and 0.5 mm with abduction. The force required to distract the hip a given distance decreased substantially with capsular venting and further decreased with the addition of full-thickness labral tear. Another study measured the strain in the labrum with the hips in different passive positions [33]. A more recent study also measured the labral strains under an average compressive joint force of 25 N [36]. At present time, biomechanical studies of the hip stability have been performed with either finite element computational models [8, 14], manual testing [33] or with a biaxial mechanical testing machine [4].
Hip distraction is less recognized, but common loading mode of the hip joint. Fluoroscopy studies showed hip subluxation during swing phase of gait in total hip arthroplasty patients [18, 22]. Labrum, capsular ligaments and muscles resist joint distraction during swing phase of gait and contribute to biomechanical joint stability. Distraction at 80–100 N is the common testing mode of hip stability [4, 15].
At present time, all biomechanical studies of the hip stability were performed with finite element analysis [8] or with biaxial mechanical testing machine [4]. Present work is the first robotic study of the hip joint that utilizes universal force-moment sensor (UFS) and allows more accurately record kinematics and forces applied to the hip, but also registers changes in hip kinematics occurring after labral injury.
The purpose of this study was to evaluate the contribution of the labrum and the effect of labral injury to stability of the femoral head in the acetabular socket. It was hypothesized that the labrum provides stability to the hip and the loss of mechanical restraint due to labral injury would cause abnormal motion of the femoral head in relation to acetabulum. Better knowledge of the effects of labral injury would aid in the understanding of the need of surgical repair of labrum and give insight into possible causes of the development of hip arthritis.
Materials and methods
Specimen preparation
Five fresh frozen whole pelvises (ten hips) complete with proximal femoral segments (age 43–49 years; four males and one female) were used. Prior approval for this study was obtained at University of Pittsburgh (Pittsburgh, PA, USA) from the Committee for Oversight of Research and Clinical Training Involving Decedents (CORID) #264.
Specimens were stored at −20 °C and thawed at room temperature 48 h prior the test. Prior to testing, specimens were checked for any abnormalities in the range of motion. All skin and muscles were removed leaving only hip joint ligaments and capsule, and the capsule was visually inspected for any injury. The proximal femoral shaft was encased in an epoxy compound for secure mounting in a custom-made aluminium clamp.
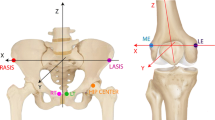
For testing, the pelvis was securely fixed to a flat plate. The pubic tubercles and the anterosuperior iliac spines were used as contact points with the plate and represented the anterior pelvic plane, as a reference for measuring pelvic orientation [5, 27]. The axis between both pubic tubercles and the axis between both anterosuperior iliac spines were parallel with the superior border of the plate. The pubic symphysis and the midline of the sacrum were placed along the midline of the plate.
The pelvic plate was then attached to the fixed base, while the femur was attached to the end-effector of the robot as shown in Fig. 1. For the starting position, the femur shaft was positioned parallel with the anterior pelvic plane and the midline of the pelvis and the femoral neck was set at 15° anteversion [40]. The hip capsules were kept moist throughout the experiment with 0.9 % sodium chloride solution.

Robotic testing of a hip specimen
Biomechanical evaluation
The robotic manipulator (Caspar, OrthoMaquet, Rastatt, Germany) is a six-joint serial articulation, which allows six-degree-of-freedom motion of the hip with repeatability of 0.02 mm at each joint according to the device specifications. The UFS (model 4015, JR3 Inc, Woodland, California, USA) can measure three orthogonal forces and moments with an accuracy of 0.2 N and 0.1 Nm, respectively. A custom computer program controlled the testing system and recorded both kinematics of the hip joint and the forces applied to the hip.
The path of passive flexion–extension of the intact hip was determined by the robotic system moving the femur from starting position (0° of flexion) to 30° degree of flexion by 0.5° degree increments. At each incremental movement, the forces and moments were recorded and minimized by the iterative algorithm of the robot control software. The positions at 0° and 30° of flexion were stored in the system and used as the starting positions for application of external loads.
Four external loads were applied to the femur at 0° and 30° of flexion: (1) an 80 N longitudinal axial force along the femoral shaft, (2) combined 80 N axial and 60 N anterior translation forces, (3) combined 80 N axial and 60 N posterior translation forces and (4) combined 80 N axial and 60 N lateral translation forces. The direction of the force was referenced to the femur. For the combined force loading, the axial force was applied first, and then, the translation force was applied. During each external load application, the 5-degree-of-freedom kinematics and applied forces and moments are recorded. The three sets of combined loads were used to evaluate position of the femoral head in relation to the acetabulum through arc of motion and assess the stabilizing effect of the capsular seal and labral support on hip joint kinematics. After the determination of the passive path of the intact hip, a 1.5 cm capsulotomy was performed at the superior part of the hip capsule in-line with the iliofemoral ligament [23]. The four loading conditions were then reapplied at both 0° and 30° of flexion to evaluate the changes in kinematics of the hip after capsulotomy. Subsequently, the recorded displacement of the intact hip under the given loading condition was repeated to the hip with capsulotomy, and the required forces and moments were recorded. The principle of superposition was applied to calculate the force contribution of capsulotomy [32]. Integrity of the hip capsule is important to the “seal” effect of the hip joint; however, capsular incision is necessary for the labral resection. Finally, 1 cm of the anterosuperior labrum was resected, and the hip was retested. The anterosuperior segment of the labrum was selected because it is a common location of labral tears [1, 24]. The four loading conditions were reapplied and the displacements measured. Then, the displacement of the intact hip in response to each load was also repeated and the forces measured. The force contribution of labral resection is the vector difference in the measured forces between the hip with capsulotomy alone and capsulotomy combined with labral resection. Testing of vented capsule alone and then vented capsule with labral resection allowed the differentiation of the effects of the two procedures on forces contribution and kinematics. The testing protocol is summarized in Table 1.
Statistical analysis
Statistical analysis for the differences in kinematic data, hip displacement in response to external loads, was performed using Friedman test, followed by a Wilcoxon signed ranks test for pair-wise comparisons. A Bonferroni approach was applied to adjust the alpha level for the pair-wise post hoc comparisons, and it was assumed that there was statistical significance when p < 0.05 for Friedman test and p < 0.017 for Wilcoxon signed ranks test. The difference in force contribution of capsulotomy and labral resection was analysed by Wilcoxon signed ranks test with statistical significance assumed when p < 0.05. All statistical calculations were performed using SPSS 16.0 (SPSS Inc., Chicago, Illinois, USA). Required sample size was calculated with PASS software (version 13.0.8). Ten specimens were sufficient to provide 80 % statistical power with 95 % statistical significance.
Results
Displacement of the femoral head in the acetabulum (“wobbling effect”) in response to four external loads in the intact hip, in the hip with capsulotomy alone and in the hip with labral resection is demonstrated in Table 2. The increasing “wobbling effect” of the femoral head in response to the 80 N axial distraction force and four external loads is shown in (Fig. 2) at 0° of flexion and in (Fig. 3) at 30° of flexion. The iliofemoral ligament, which is taut in extension (0° of flexion), stabilized the femoral head in the acetabulum. At 30° of flexion (with relaxed iliofemoral ligament), displacement under axial load of the hip with labral resection was significantly different from the intact hip and hip with capsulotomy alone. At 30° of hip flexion, the amount of anterior and posterior femoral head translation of the hip with labral resection was significantly higher than the hip with capsulotomy alone. The increased displacement of the femoral head in the acetabulum (“wobbling” effect) after labral resection was on average 0.9 mm in anterior direction and 2.5 mm in posterior direction.

Hip translation under distraction and distraction and anterior, posterior and lateral loads for different hip states at of 0° flexion. *Significantly different from intact, **significantly different from capsulotomy

Hip translation under distraction and distraction and anterior, posterior and lateral loads for different hip states at of 30° flexion. *Significantly different from intact, **significantly different from capsulotomy
Figures 4 and 5 demonstrate the force reduction in the hip with capsulotomy and capsulotomy with labral resection, compare to intact hip at 0° and 30° of flexion, respectively. The force reduction due the labral resection was most significant at 30° of flexion in response to axial (distraction) load alone, followed by distraction in full extension. At 0° of flexion, the amount of axial force need to distract the hip 2.6 mm was reduced by 14.1 N with the capsulotomy and by 39.3 N with the labral resection. Likewise at 30° of flexion, the required axial force was reduced from 80 N to 67.1 N and then to 14.9 N with capsulotomy and labral resection, respectively. Also, large reductions in force were found for the combined axial and lateral displacement at both flexion angles. The force reduction due to labrum resection was significantly higher than that of the capsulotomy in response to all external loads at both 0° and 30° of hip flexion, except for the response to combined axial and posterior translation at 0° of flexion. These data demonstrate significant anchoring effect of labrum that allows smooth motion of the femoral head in the acetabulum, compared to femoral head “wobble” with labrum resection.

In situ tissue forces of capsule and capsule and labrum under distraction and distraction and anterior, posterior and lateral loads at of 0° flexion. *Significantly different from capsulotomy

In situ tissue forces of capsule and capsule and labrum under distraction and distraction and anterior, posterior and lateral loads at of 30° flexion. *Significantly different from capsulotomy
Discussion
The most important finding in the present study was that the acetabular labrum provided stability to the femoral head in the acetabulum and 1 cm of labral resection caused a significant increase in displacement of the femoral head at 0° of flexion under combined axial and lateral load and at 30° of flexion under axial and combined axial and anterior/posterior load. This is consistent with the reduction in amount of external load required for these displacements when the labrum is resected. The previous work by Crawford et al. [4] showed that there was increasingly greater external rotation under the same external torque with capsule venting and labral injury. Additional, the study found substantially and sequentially reduced force was required to distract the hip a fixed distance (1, 3 and 5 mm) with capsule venting and subsequent labral injury. Similar to the current study, these data showed the reduced stiffness of the joint with injury; however, since the displacement was limited, it did not examine how femoral head instability changes with injury.
The robotic/UFS system has been previously used in biomechanical studies of the knee to evaluate knee kinematics to particular loading conditions and determine in situ force of the ligament or graft in response to those loads [11, 12, 21, 32, 42, 43]. The kinematics of different joint conditions in response to external loads can be evaluated with the force control mode. The precise repeatability of positioning of the testing system ensures the same starting position for each test. In addition, when the system is operated in the displacement control mode, the in situ force of a ligament or graft can be determined using the principle of superposition by calculating the difference in the force before and after removal of a ligament or graft [32]. This calculation method was used to determine the reduction in tissue force due to capsulotomy and labral resection. To our knowledge, this was the first study describing a method of biomechanical testing of the hip with the robotic/UFS system and using an anterior pelvic frame to position the pelvis.
The force reduction in capsulotomy represented the venting effect of the hip in addition to any change in stiffness due to the capsular incision. Because the labrum could not be resected without violating the joint capsule, it was opted to perform a capsular incision to create the venting effect and to provide exposure for the later labral resection and each factor was separately assessed. The incision was placed in-line with iliofemoral ligament to minimize damage to the capsular ligaments, which also provided stability to the hip joint [13]. The force reduction in the labral resection was most significant in axial loading and combined axial and lateral loading. It is apparent that the force restraint by the tissues is significantly lower for anterior and posterior translation, due to mechanical constraints of the acetabular socket. At 0° of flexion, the iliofemoral ligament is taut giving a greater contribution to joint stability. The increase in anterior-posterior motion with labral injury could explain prevalence of anterior labral tears in Caucasian population [3].
Pelvis positioning for robotic testing is difficult due to irregular shape and variety of functional orientation. The anterior pelvic plane was used as a frame of reference for positioning in space. The anterior pelvic plane is the plane passing through the tips of bilateral pubic tubercles and bilateral anterosuperior iliac spines. This plane has been used as a reference plane in measuring pelvic tilt [5, 27], acetabular orientation [17], and is also used in the acetabular component placement in computer-assisted total hip arthroplasty [2]. Previous biomechanical testing of the hip usually used a hemi-pelvis specimen [4, 10, 23], which is difficult to position in space due to a limited number of landmarks. Use of a whole pelvis specimen provided an anterior pelvic plane to position the pelvis, and this plane is also used as a reference to position the femur in flexion/extension and abduction/adduction movements. Anteversion of the femur at the starting position was set at 15° because it is the average value of anteversion in adults [39].
The labrum increases the articular area by 28 % and acetabular volume by 30 % [39]. Acetabular labral tears are caused by many conditions such as trauma [7, 30], instability [19, 29], hip dysplasia [16], iliopsoas impingement [35] and femoroacetabular impingement [1] that leads to hip or groin pain [25], but the most important aspect of the labral pathology is its association with degenerative change of the hip [24, 28]. The acetabular labrum provides a seal against fluid flow into and out of central compartment of the hip [10, 38, 41]. This creates hydrostatic pressure slowing cartilage consolidation during application of a compression load [8–10]. The labral seal also produces the “suction effect” resisting distraction of the femoral head from the acetabulum and also mechanical support by effectively deepening the socket. Labral resection can break the seal and reduced the mechanical stiffness of the tissue, which can significantly destabilize the femoral head in the acetabulum and cause “wobbling” effect, which could be detrimental for cartilage and may lead to osteoarthritis of the hip. If this mechanism is one of the possible causes of coxarthrosis, then labral repair could preserve the hip joint and lead to enormous socio-economic effect. It is clear that further studies are required to reveal the biomechanical benefits of labral repair. While favourable long-term results were reported after selective debridement of symptomatic labral tears [3], recent studies have demonstrated that better clinical outcomes were obtained in patients with labral repair compared to those with labral debridement [6, 20]. Recently, a technique of labral reconstruction was introduced with good early outcomes [31]. Better understanding of labral function is important in the selection of treatments for labral tears.
A limitation of this model is that it does not include muscle forces that can apply a compressive load to the hip in the in vivo situation. While the addition of muscle forces would serve to reduce the displacements in all three hip states, intact, vented capsule and labral resection, it is not known whether muscle forces could increase sufficiently to compensate for the significant loss of support provided by the labrum in the event of injury. Also, there may be in vivo situations when muscles are not active, and increased femoral head displacement would occur without the restraint of the labrum.
The clinical ramifications of this study suggest that labral repair should be done for significant labral injuries because the mechanical constraint provided by the labrum is severely compromised. Significantly, larger femoral head displacements occur under the same loads with injury, and it is not known under what, if any, in vivo conditions this will be compensated for by increased muscle support. If the loss of labral function is not offset by some other means of support, increased femoral head displacements may occur during activity. This would lead to increased joint contact load, and if repetitive, this could lead to cartilage injury.
Conclusion
The acetabular labrum provides stability to the hip joint in response to a distraction force and combined distraction and translation forces. One centimetre of labral resection caused significant displacement (“wobbling” effect) of the femoral head within the acetabulum with normal range of motion. Successful labral repair could be crucial for restoration of the hip biomechanics and prevention of coxarthrosis.
References
Beck M, Kalhor M, Leunig M, Ganz R (2005) Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br 87:1012–1018
Beckmann J, Luring C, Tingart M, Anders S, Grifka J, Kock FX (2009) Cup positioning in THA: current status and pitfalls. A systematic evaluation of the literature. Arch Orthop Trauma Surg 129:863–872
Byrd JW, Jones KS (2009) Hip arthroscopy for labral pathology: prospective analysis with 10-year follow-up. Arthroscopy 25:365–368
Crawford MJ, Dy CJ, Alexander JW, Thompson M, Schroder SJ, Vega CE, Patel RV, McCarthy JC, Lowe WR, Noble PC (2007) The 2007 Frank Stinchfield Award. The biomechanics of the hip labrum and the stability of the hip. Clin Orthop Relat Res 465:16–22
DiGioia AM, Hafez MA, Jaramaz B, Levison TJ, Moody JE (2006) Functional pelvic orientation measured from lateral standing and sitting radiographs. Clin Orthop Relat Res 453:272–276
Espinosa N, Rothenfluh DA, Beck M, Ganz R, Leunig M (2006) Treatment of femoro-acetabular impingement: preliminary results of labral refixation. J Bone Joint Surg Am 88:925–935
Feeley BT, Powell JW, Muller MS, Barnes RP, Warren RF, Kelly BT (2008) Hip injuries and labral tears in the national football league. Am J Sports Med 36:2187–2195
Ferguson SJ, Bryant JT, Ganz R, Ito K (2000) The acetabular labrum seal: a poroelastic finite element model. Clin Biomech 15:463–468
Ferguson SJ, Bryant JT, Ganz R, Ito K (2000) The influence of the acetabular labrum on hip joint cartilage consolidation: a poroelastic finite element model. J Biomech 33:953–960
Ferguson SJ, Bryant JT, Ganz R, Ito K (2003) An in vitro investigation of the acetabular labral seal in hip joint mechanics. J Biomech 36:171–178
Gabriel MT, Wong EK, Woo SL, Yagi M, Debski RE (2004) Distribution of in situ forces in the anterior cruciate ligament in response to rotatory loads. J Orthop Res 22:85–89
Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin TM, Woo SL (2000) Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 28:144–151
Harris JD, Slikker W, Gupta AK et al (2013) Routine complete capsular closure during hip arthroscopy. Arthrosc Tech 2:89–94
Henak C, Ellis B, Harris M, Anderson A, Peters C, Weiss J (2011) Role of the acetabular labrum in load support across the hip joint. J Biomech 44(12):2201–2206
Ito H, Song Y, Lindsey DP, Safran M, Giori N (2009) The proximal hip joint capsule and the zona orbicularis contribute to hip joint stability in distraction. J Orthop Research 27:989–995
Klaue K, Durnin CW, Ganz R (1991) The acetabular rim syndrome. A clinical presentation of dysplasia of the hip. J Bone Joint Surg Br 73:423–429
Kohnlein W, Ganz R, Impellizzeri FM, Leunig M (2009) Acetabular morphology: implications for joint-preserving surgery. Clin Orthop Relat Res 467:682–691
Komistek RD, Dennis DA, Ochoa JA, Haas BD, Hammill C (2002) In vivo comparison of hip separation after metal-on-metal or metal-on-polyethylene total hip arthroplasty. J Bone Joint Surg Am 84:1836–1841
Krych AJ, Thompson M, Larson CM, Byrd JW et al (2012) Is posterior hip instability associated with cam and pincer deformity? Clin Orthop Relat Res 470:3390–3397
Larson CM, Giveans MR (2009) Arthroscopic debridement versus refixation of the acetabular labrum associated with femoroacetabular impingement. Arthroscopy 25:369–376
Lertwanich P, Martins CAQ, Kato Y, Ingham SJH, Kramer S, Linde-Rosen M, Smolinski P, Fu F (2010) Contribution of the meniscofemoral ligament as a restraint to the posterior tibial translation in a porcine knee. Knee Surg Sports Traumatol Arthrosc 18:1277–1281
Lombardi AV, Mallory TH, Dennis DA, Komistek RD, Fada RA, Northcut FJ (2000) An in vivo determination of total hip arthroplasty pistoning during activity. J Arthroplasty 15:702–709
Martin HD, Savage A, Braly BA, Palmer IJ, Beall DP, Kelly B (2008) The function of the hip capsular ligaments: a quantitative report. Arthroscopy 24:188–195
McCarthy JC, Noble PC, Schuck MR, Wright J, Lee J (2001) The Otto E. Aufranc Award: The role of labral lesions to development of early degenerative hip disease. Clin Orthop Relat Res 393:25–37
Narvani AA, Tsiridis E, Kendall S, Chaudhuri R, Thomas P (2003) A preliminary report on prevalence of acetabular labrum tears in sports patients with groin pain. Knee Surg Sports Traumatol Arthrosc 11:403–408
Nepple JJ, Philippon MJ, Campbell KJ et al (2014) The hip fluid seal—Part II: the effect of an acetabular tear, repair, resection, and reconstruction on hip stability to distraction. Knee Surg Sports Traumatol Arthrosc 22(4):730–736
Nishihara S, Sugano N, Nishii T, Ohzono K, Yoshikawa H (2003) Measurements of pelvic flexion angle using three-dimensional computed tomography. Clin Orthop Relat Res 140–51, 123: 283–288
Petersen W, Petersen F, Tillmann B (2003) Structure and vascularization of the acetabular labrum with regard to the pathogenesis and healing of labral lesions. Arch Orthop Trauma Surg 123:283–288
Philippon MJ, Schenker ML (2005) Athletic hip injuries and capsular laxity. Oper Tech Orthop 15:261–266
Philippon MJ, Kuppersmith DA, Wolff AB, Briggs KK (2009) Arthroscopic findings following traumatic hip dislocation in 14 professional athletes. Arthroscopy 25:169–174
Philippon MJ, Briggs KK, Hay CJ, Kuppersmith DA, Dewing CB, Huang MJ (2010) Arthroscopic labral reconstruction in the hip using iliotibial band autograft: technique and early outcomes. Arthroscopy 26:750–756
Rudy TW, Livesay GA, Woo SL, Fu FH (1996) A combined robotic/universal force sensor approach to determine in situ forces of knee ligaments. J Biomech 29:1357–1360
Safran MR, Giordano G, Lindsay DP, Gold GE, Rosenberg J, Zaffagnini S, Giori NJ (2011) Strains across the acetabular labrum during hip motion: a cadaveric model. Am J Sports Med 39:92–102
Selders RM, Tan V, Hunt J, Katz M, Winiarsky R, Fitzgerald RH (2001) Anatomy, histological features and vascularity of the adult acetabular labrum. Clin Orthop Rel Res 382:232–240
Shindle MK, Voos JE, Nho SJ, Heyworth BE, Kelly BT (2008) Arthroscopic management of labral tears in the hip. J Bone Joint Surg Am 90(Suppl 4):2–19
Smith MV, Panchal HB, Thiele RA, Sekiya JK (2011) Effect of acetabular labrum tears on hip stability and labral strain in a joint compression model. Am J Sports Med 39:103–110
Song Y, Ito H, Kourtis L, Safran K, Carter D, Gion N (2012) Articular cartilage friction increases in hip joints after removal of the acetabular labrum. J Biomech 45(3):524–530
Takechi H, Nagashima H, Ito S (1982) Intra-articular pressure of the hip joint outside and inside the limbus. J Jpn Orthop Assoc 56:529–536
Tan V, Seldes RM, Katz MA, Freedhand AM, Klimkiewicz JJ, Fitzgerald RH Jr (2001) Contribution of acetabular labrum to articulating surface area and femoral head coverage in adult hip joints: an anatomic study in cadavera. Am J Orthop 30:809–812
Tayton E (2007) Femoral anteversion: a necessary angle or an evolutionary vestige? J Bone Joint Surg Br 89:1283–1288
Terayama K, Takei T, Nakada K (1980) Joint space of the human knee and hip joint under a static load. Eng Med 9:67–74
Woo SL, Fisher MB (2009) Evaluation of knee stability with use of a robotic system. J Bone Joint Surg Am 91(Suppl 1):78–84
Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL (2002) Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med 30:660–666
Conflict of interest
The authors declared no conflict of interest related to this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lertwanich, P., Plakseychuk, A., Kramer, S. et al. Biomechanical evaluation contribution of the acetabular labrum to hip stability. Knee Surg Sports Traumatol Arthrosc 24, 2338–2345 (2016). https://doi.org/10.1007/s00167-015-3555-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3555-2