
Abstract
This study is one of the first to present causal evidence of the morbidity costs of fine particulates (PM2.5) for all age cohorts in a developing country, using individual-level health spending data from a basic medical insurance program in Wuhan, China. Our instrumental variable (IV) approach uses thermal inversion to address potential endogeneity in PM2.5 concentrations and shows that PM2.5 imposes a significant impact on healthcare expenditures. The two-stage least squares (2SLS) estimates suggest that a 10 μg/m3 (micrograms per cubic meter) reduction in monthly average PM2.5 leads to a 2.36% decrease in the value of health spending and a 0.79% decline in the number of transactions at pharmacies and healthcare facilities. Also, this effect, largely driven by spending at pharmacies, is more salient for males and children, as well as middle-aged and older adults. Moreover, our estimates may provide a lower bound on individuals’ willingness to pay, amounting to CNY 43.87 (or USD 7.09) per capita per year for a 10 μg/m3 reduction in PM2.5.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
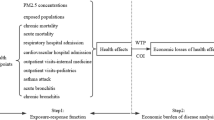
A large body of literature examines the effects of air pollution on health-related outcomes, including mortality (Anderson 2020; Chay and Greenstone 2003; Greenstone and Hanna 2014; He et al. 2016), life expectancy (Chen et al. 2013; Ebenstein et al. 2017), hospitalization (Moretti and Neidell 2011; Schlenker and Reed Walker 2016), and birth outcomes (Currie and Neidell 2005; Currie et al. 2009), as well as defensive expenditures on facemasks and air purifiers (Ito and Zhang 2020; Zhang and Mu 2018). However, evidence on the causal effect of air pollution on health spending is relatively limited. The morbidity costs of air pollution could provide a lower bound estimate of individuals’ willingness to pay (WTP) for better air quality, which would be a requisite for the government to know when conducting cost–benefit analyses and introducing more optimal environmental regulations. A wide range of social costs of pollution other than solely morbidity costs, such as avoidance costs (e.g., masks, air filters) and mortality costs, have been documented in the existing literature and are therefore not accounted for in this study.
While there has been a large number of epidemiological studies on the association between air pollution and health spending, it is still important to carefully design causal evaluations for examining the effect of air pollution on medical expenditures in order to address sources of bias due to the endogeneity problem. The first source is unobserved factors. In this regard, time-varying local shocks may be correlated with both health spending and exposure to air pollution, and these cannot be fully removed by individual fixed effects and time fixed effects. The second source of bias relates to avoidance behaviors that are not fully observable given the limited information in the data. In recent years, air pollution has attracted greater public attention in China. On days when pollution levels are high, residents may reduce their outdoor activities (Neidell 2009), postpone visits to healthcare facilities, or take preventive measures by wearing particulate-filtering facemasks or using air-filtering products (Ito and Zhang 2020; Sun et al. 2017; Zhang and Mu 2018). The third source of bias is measurement errors with regard to measuring air pollutants, which could also lead to attenuation bias. Measurement errors may be attributable to the aggregation of pollution data from sporadic monitoring stations or pollution data manipulations (Chen et al. 2012; Ghanem and Zhang 2014).
Only a few studies have attempted to identify the causal effects by employing plausibly exogenous variations. Deschênes et al. (2017) examine the effect of a decline in nitrogen oxide (NOX) emissions on pharmaceutical expenditures at the county-season-year level, employing a cap-and-trade NOX Budget Program (NBP) as a quasi-experiment. Instrumenting air pollution using changes in local wind directions, Deryugina et al. (2019) estimate the causal effects of daily fine particulates (PM2.5) on county-level inpatient emergency room (ER) spending for those aged 65 years old or older. Williams and Phaneuf (2019) identify the impact of PM2.5 on quarterly household health spending via instrumenting local air pollution using emissions from distant sources. Utilizing a similar instrumental variable (IV) strategy, Barwick et al. (2021) first analyze the medical burden from PM2.5 in a developing country, based on city-level credit and debit card transactions in China. Their IV estimates suggest that a 10 μg/m3 increase in PM2.5 over the past 90 days would lead to a 2.65% increase in the number of healthcare transactions and a 1.5% increase in out-of-pocket expenses. Liu and Ao (2021) estimate the impact of the daily air quality index (AQI) on outpatient healthcare expenditures for respiratory diseases at the township level using thermal inversion as an IV. Employing a similar IV, Xia et al. (2022) identify the short-term impact of PM2.5 concentrations on medical costs at a subpopulation level in Beijing.
In this paper, we examine the causal impact of PM2.5 exposure on medical expenses at both pharmacies and all levels of healthcare facilities. Matching individual-level health spending data with air pollution exposure between 2013 and 2015, we also estimate people’s WTP for cleaner air. We instrument PM2.5 concentrations using thermal inversion, a widely-used IV in recent studies (Arceo et al. 2016; Chen et al. 2018; Chen et al. 2022; Xia et al. 2022) to address potential endogeneity in air pollution. Thermal inversion is a meteorological phenomenon that occurs when the air temperature is abnormally higher than that at lower altitudes. It reduces the vertical circulation of the air and thus traps air pollutants near the ground. While thermal inversion does not pose a direct threat to health, it does lead to higher concentrations of air pollutants (Arceo et al. 2016). Our results suggest that a 10 μg/m3 reduction in monthly average PM2.5 would lead to a 2.36% decrease in the value of health spending, and a 0.79% decrease in the number of transactions in pharmacies and healthcare facilities. This effect is more salient for males and children (up to age 10), as well as middle-aged and older adults (age 51 and older). Valuing air quality using total health spending data, our estimates suggest that people would be willing to pay 43.87 Chinese yuan (CNY) per capita per year for a 10 μg/m3 reduction in PM2.5.
This study aims to contribute to the literature in several dimensions. First, the insurance claims data adopted by most of the existing studies do not cover drug expenses at pharmacies. As we possess detailed information on each category of transactions from pharmacies, clinics, and hospitals, we are able to examine the impact on the overall and respective medical expenditures at pharmacies and all levels of healthcare facilities.Footnote 1 We identify a much stronger effect on the expenses at pharmacies compared to in healthcare facilities, highlighting the importance of incorporating this former segment of medical expenses in future analysis, and indicating some plausible behavior channels through which air pollution may impact overall health spending. To the best of our knowledge, Barwick et al. (2021) is the only paper that investigates the impact on expenditures at both pharmacies and hospitals using bank cards. However, they use total expenditures that combine inpatient and outpatient care, while inpatient care is often scheduled in advance and thus may largely be immune to transitory air pollution. In addition, vulnerable population groups, such as older adults and low-income residents who are less likely to use debit or credit cards, tend not to be in their sample obtained from bank transaction records.
Second, existing studies either focus on working-age and older populations or make no distinction by patient age. However, evidence on the healthcare costs of air pollution for young children is limited. As our sample covers all age cohorts of urban residents with information on patient age, our examinations of possible heterogeneities in the sensitivity to air pollution across age groups, as well as for respective age groups, attempt to fill this gap in the literature.
Third, we use individual-level data to identify medical spending in response to air pollution. Previous studies tend to rely on aggregated health spending data that is subject to ecological fallacy. As such, the findings may be biased, depending on the level of aggregation, due to the omitted variables that often threaten identification in research linking air pollution to behavioral outcomes. Employing comprehensive individual-level data also enables us to test the heterogeneous effects across groups to understand which segments of the population are more affected by air pollution. To the best of our knowledge, only two economic studies have examined the effects of air pollution on medical expenditures at the disaggregated level: Liao et al. (2021) and Williams and Phaneuf (2019). However, they both obtained healthcare spending and utilization data from social surveys, which can suffer from recall error or other potential biases.
Fourth, some time–invariant unobserved factors—such as individuals’ health stock and preference to live in a clean environment—are correlated with both health spending and exposure to air pollution, thereby biasing the estimations. By exploiting the longitudinal nature of our health spending data at the individual level, we are among the first to control for individual fixed effects in our estimation of the morbidity costs of air pollution, thereby mitigating concerns over individual heterogeneity in preferences or some other unobservables (Deschênes et al. 2017).
Moreover, our paper contributes to the strand of literature that estimates individuals’ WTP for improved air quality.Footnote 2 Following the health production framework established in the seminal work by Grossman (1972), Deschênes et al. (2017) and Williams and Phaneuf (2019) propose a theoretical model of WTP and show that the benefits that could be accrued by reduced health spending is merely one component of people’s WTP for improved air quality. Therefore, our estimated WTP using medical expenditures may offer a lower bound of the WTP for cleaner air.Footnote 3
Finally, we are among the first to estimate the morbidity costs of air pollution in a developing country using health spending records for all ages in the study cohort. Air pollution is generally worse in developing countries, such as Nepal, Bangladesh, India, China, and Pakistan.Footnote 4 In fact, 98.6% of the population in China have been exposed to PM2.5 at unsafe levels according to the World Health Organization (WHO) guideline (Long et al. 2018). We obtain the health spending data from Wuhan, the capital city of Hubei province, China. As a major manufacturing city in central China, Wuhan tends to be exposed to high levels of air pollution with large daily variations. Therefore, the dose–response relationship between air pollution and medical expenses estimated in this study, using a wide spectrum of pollution exposures, may have implications for other developing countries with similar situations.
The remainder of this paper is organized as follows. Section 2 describes the data sources. Section 3 discusses the empirical model and the identification strategy using thermal inversion as an instrument. Section 4 reports the main findings, including the baseline results, robustness checks, and heterogeneous effects. Section 5 compares our calculated WTP to others in the related literature. Section 6 concludes and proposes some future research directions.
2 Data
2.1 Health spending
Health spending data are obtained from the universal basic medical insurance system, developed by the Chinese central government and covering 95% of China’s population as of 2011 (Yu 2015). The system includes two government programs in urban areas—namely, Urban Employee Basic Insurance (UEBMI) and Urban Resident Basic Medical Insurance (URBMI).Footnote 5 We use a representative sample from the basic medical insurance program in urban areas of Wuhan, the capital city of Hubei province, China. Our dataset includes all the health expenditure records for 1% randomly sampled beneficiaries (approximately 40,000 individuals) from 130 hospitals, 643 clinics, and 2642 pharmacies between 2013 and 2015.Footnote 6 For each record, we observe the patient unique ID, gender, age, location, date, and total value of expenses. Total health spending includes expenditures at pharmacies as well as outpatient and inpatient expenses at all levels of healthcare facilities (i.e., clinics and hospitals). Most inpatient health transactions are likely related to surgeries, with appointments usually made in advance, and thus these are insensitive to transitory air pollution. Therefore, we utilize only the expenses at pharmacies and outpatient health spending at healthcare facilities in our analysis. Medical expenses are further classified into three main categories: medication, examination, and treatment.Footnote 7 Figure A1 plots the monthly values of health spending and the number of transactions from 2013 to 2015. Medical spending and the number of transactions tend to decline during holidays, especially during the Spring Festivals.
For our purposes, there are four advantages in employing data from the basic medical insurance program in Wuhan. First, the program provides wide coverage in Wuhan, and the beneficiaries in our sample cover all age groups of urban residents, enabling us to examine heterogeneous effects across age cohorts and to understand which subpopulations are most affected by air pollution. Second, the health spending records in our sample include all pharmacy and health facility transactions, enabling us to estimate the morbidity costs of air pollution in a more comprehensive way than in studies that consider only medical expenses incurred in hospitals. Third, information on the geographic locations of pharmacies and healthcare facilities, as well as dates of service, enable us to precisely match individual-level healthcare expenditures with external air quality data. Fourth, the daily mean concentration of PM2.5 in Wuhan in 2013–2015 was 80 μg/m3, a much higher figure than that in most developed countries. This useful setting provides us with an opportunity to not only examine the non-linear effect of PM2.5 on health spending, but also to estimate a wide range of dose–response relationships.
2.2 Pollution and weather
Air pollution measures are provided by the daily air quality report of the Ministry of Ecology and Environment (MEE) of China, which started to publish the concentrations of six air pollutants and an air quality index (AQI) in 2013.Footnote 8 The report covers 10 monitoring stations in Wuhan City, with the longitudes and latitudes of each station provided. Given that PM2.5 is more toxic and can penetrate deeper into lungs than PM10, we mainly focus on PM2.5 (Pope and Dockery 2006).Footnote 9 Figure A2 shows the daily mean PM2.5 concentration in Wuhan during the period from 2013 to 2015. From Figure A2, on most days, the concentrations of PM2.5 are higher than the daily air quality guideline values of the WHO (25 μg/m3).
The weather data originates from the China National Meteorological Data Service Center (CMDC), part of the National Meteorological Information Center of China. The dataset reports consecutive daily records of a wide range of weather conditions, including temperature, precipitation, wind speed, sunshine duration, and relative humidity. We calculate the mean values for each weather variable from two monitoring stations in Wuhan.
2.3 Thermal inversion
The data on thermal inversion is drawn from the product M2I6NPANA, version 5.12.4, released by the U.S. National Aeronautics and Space Administration (NASA). The data reports air temperatures every 6 h for each 0.5°\(\times\) 0.625° (around 50 km \(\times\) 60 km) grid, for 42 layers, ranging from 110 to 36,000 m. We interpolate the data at a finer grid level and extract the mean values for each county in Wuhan. For every 6-h period, we further derive the temperature difference between the second layer (320 m) and the first layer (110 m). Under normal conditions, the difference would be negative, since temperature generally decreases as the latitude increases. However, thermal inversion occurs when the temperature difference is positive. If the difference is positive, the magnitude measures the thermal inversion strength. If the difference is negative, we truncate it to zero. We average the thermal inversion strength across the four 6-h periods and calculate the total number of thermal inversion occurrences for each day. Then, we calculate the mean value for the thermal inversion strength and the total number of occurrences within each month based on the daily data.
In order to match air pollution and thermal inversion with health spending data, we infer the residential address for each person from the location of the pharmacy that the person most often visited.Footnote 10 We match air pollution concentrations from the nearest monitoring station and thermal inversion measures at the county level.Footnote 11 Figure 1 plots the distribution of the monitoring stations and healthcare facilities in Wuhan. For the weather data, we match their monthly mean values from the two monitoring stations to each individual.

Distribution of monitoring stations and healthcare facilities in Wuhan, China. Note: The figure is plotted using ArcMap 10.8.2
Our dataset contains around 1.38 million transactions in pharmacies and all levels of healthcare facilities by 40,000 individuals. We calculate the total value of health spending as well as the number of transactions in pharmacies and healthcare facilities by each person in each month. If no health expenditure records exist for one specific month, we assign a value of zero. In this way, we are able to construct a data panel at the individual-month level. The final dataset for analysis includes over 1.44 million person-month observations.Footnote 12
Table 1 displays the key variables and their summary statistics. The beneficiaries, on average, spend 154.86 yuan and make 0.939 transactions per month in pharmacies and healthcare facilities. The monthly average PM2.5 concentration is 81.914 μg/m3 and the monthly average thermal inversion strength is 0.245 °C.
3 Empirical strategy
Our baseline econometric specification is as follows:
The dependent variable Healthijt is the value of health spending, or the number of transactions in pharmacies and healthcare facilities for individual i living in county j during month t. Since our data contain many zero-valued observations, we apply the inverse hyperbolic sine (arcsinh) transformation to the dependent variable.Footnote 13 The advantage of the arcsinh transformation is that it approximates the natural logarithm transformation and allows retaining zero-valued observations (Bellemare and Wichman 2020).Footnote 14 The key variable Pijt represents the monthly mean concentration of PM2.5. We include a set of demographic controls Xijt, including age and its squared term. We also control for a vector of rich weather conditions Wt, involving number of days falling in each temperature bin (< 12 °C, 12–16 °C, 16–20 °C, 20–24 °C, 24–28 °C, > 28 °C), precipitation, wind speed, sunshine duration, and relative humidity in square polynomial forms to mitigate the concern that they are correlated with both health spending and air quality. λi represents individual fixed effects. Finally, we control for county-specific time trend by including county-by-year fixed effects (δjt) and seasonality by including month fixed effects (ηt). εijt is the error term. Standard errors are clustered at the county level. Since there are 13 counties, we estimate wild bootstrapped standard errors to address the possibility of small sample bias (Cameron et al. 2008; Roodman et al. 2019).
OLS estimates of Eq. (1) are prone to bias resulting from potential sources of endogeneity, such as time-varying unobserved factors, avoidance behaviors, and measurement error in air pollution due to the aggregation of pollution data from sporadic monitoring stations at the city level. We address endogeneity by employing an IV strategy, using thermal inversion as an instrument for air pollution. Thermal inversion is a common phenomenon that occurs when a layer of hot air covers a layer of cooler air near the ground. It prevents air flow by trapping air pollutants in the lower atmosphere and has no adverse effects on human health (Arceo et al. 2016). We take advantage of this exogenous shock in order to identify the effects of air pollution on health spending.
The specification for our first stage is as follows:
Following Chen et al. (2022), we use the monthly average thermal inversion strength (TIjt) as the excluded instrument. Thermal inversion strength is defined as the air temperature at the second layer (320 m) minus the temperature near the ground (110 m). We keep the positive differences and truncate the negative differences to zero. Standard errors are clustered at the county level. Other control variables are as defined in Eq. (1). After flexibly controlling for a large number of fixed effects and covariates, our identification assumption is that changes in a city’s thermal inversion are unrelated to changes in health spending, except through air pollution.
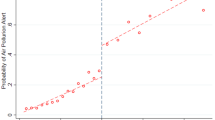
Figure 2 illustrates the relationship between PM2.5 and thermal inversion strength at the monthly level during the sample period. As shown by the figures, thermal inversion strength is highly correlated with PM2.5 concentrations, indicating that thermal inversion is a strong predictor of air pollution levels.

Monthly trend of value of health spending, PM2.5, and thermal inversion strength in Wuhan, 2013–2015. Note: The figure plots the monthly mean value of health spending (million yuan), PM2.5 concentration level (μg/m.3), and thermal inversion strength (°C) in Wuhan during 2013–2015
Before undertaking quantitative analyses, we plot the relationship between PM2.5 and health spending outcomes. As shown in Fig. 3, the value of health spending, as well as the number of transactions in pharmacies and healthcare facilities, is slightly positively correlated with PM2.5 levels. Of course, these bivariate plots provide suggestive evidence only. More rigorous analyses are needed to control for other confounding factors.

Relationship between health spending outcomes and PM2.5 concentrations. Note: Each dot denotes the in-group average of the health spending outcomes. Groups are binned by percentiles of the x-axis variable, PM2.5
4 Results
4.1 Baseline results
Table 2 presents the first-stage estimates of the effect of thermal inversions on PM2.5 concentrations. The regression controls for individual fixed effects, demographic controls, and weather controls, as well as county-by-year and month fixed effects. As the magnitude of the coefficient is difficult to interpret, we convert the point estimate to elasticity. The point estimate indicates that a 1% increase in thermal inversion is associated with a 0.20% (67.729 \(\times\) 0.245/81.914) increase in PM2.5 concentrations. Overall, we find a strong first-stage relationship. The Kleibergen–Paap (KP) F-statistics is well above the Stock–Yogo critical value.
Table 3 shows our baseline results for the effects of air pollution on the value of health spending in panel A and on the number of transactions in panel B. Columns 1 and 3 report the OLS estimates of Eq. (1), while columns 2 and 4 report the IV estimates. The OLS estimate in column 1 suggests a significant positive correlation between the PM2.5 concentration and the value of health spending after controlling for individual fixed effects, demographic controls, weather controls, and county-by-year and month fixed effects. The point estimate indicates that a 1 μg/m3 reduction in monthly average PM2.5 leads to a decrease in medical expenditures by 0.664‰.Footnote 15 As the marginal effect of exposure to air pollution on health spending provides a lower bound of people’s WTP for better air quality, the coefficient on PM2.5 indicates that people are, on average, willing to allocate 0.664% of their medical expenditure for a 10 μg/m3 monthly reduction in PM2.5. To put this into context, note that the mean monthly health spending is CNY 154.86. The WTP amounts to CNY 12.34 per year (= 0.664% \(\times\) 154.86 \(\times\) 12) for a 10 μg/m3 reduction in PM2.5. These two numbers are reported in the last two rows of Table 3.
Column 2 presents the corresponding IV estimate of the causal effect of PM2.5 on the value of health spending. The IV estimate is approximately 3–4 times larger than the corresponding OLS estimate, suggesting that the OLS estimation suffers from significant bias. Furthermore, the IV estimate implies that people are, on average, willing to pay CNY 43.87 per year (= 2.361% \(\times\) 154.86 \(\times\) 12) for a 10 μg/m3 reduction in PM2.5.
A large difference between the OLS and IV results on the effects of air pollution on health spending is common in the literature (Barwick et al. 2021; Deryugina et al. 2019; Williams and Phaneuf 2019).Footnote 16 Two possible reasons exist for this downward bias. First, some time-varying omitted variables, such as economic prosperity and avoidance behavior, are positively correlated with air pollution. As these factors are likely to reduce health spending, the omitted variable bias tends to be negative. Second, measurement errors in PM2.5 could lead to attenuation bias.
Panel B of Table 3 shows the effect of the exposure to PM2.5 on the number of transactions at the monthly level. Similarly, it can be seen that the IV estimates are larger than the corresponding OLS estimates, indicating that OLS estimation still suffers from downward bias. As presented in column 4, the IV estimate suggests that a 10 μg/m3 reduction in monthly average PM2.5 would lead to a 0.791% decrease in the number of transactions in pharmacies and healthcare facilities.
4.2 Robustness checks
In this section, we conduct a set of regressions to check the robustness of our main results. The first issue is that the concentrations of various air pollutants are highly correlated, and thus the estimation of the WTP for PM2.5 reduction may involve payments for other co-pollutants.Footnote 17 In order to address this concern, we add co-pollutants, including PM2.5–10, CO, O3, SO2, and NO2, in each column of Table 4, respectively. As PM10 includes PM2.5, we add PM2.5–10, which represents particulate matter with a diameter between 2.5 to 10 μm, as a co-pollutant. We instrument for PM2.5 utilizing the thermal inversion strength.Footnote 18 As revealed in Table 4, the coefficients on PM2.5 remain significant and the magnitudes barely change. The WTP values for a 10 μg/m3 reduction in PM2.5 are within a reasonable range, between CNY 39.51 and CNY 47.61 per year.
Table 5 presents alternative specifications. Column 1 of Table 5 replicates the baseline results in column 2 of Table 3 for ease of comparison. In column 2, we perform placebo tests by examining whether “PM2.5 in the same month next year” affects health spending. “PM2.5 in the same month next year” is instrumented by “thermal inversion in the same month next year.” As expected, this variable is not statistically significant.
We estimate a non-linear relationship between PM2.5 and health spending in column 3 of Table 5. We classify PM2.5 concentrations into three categories, i.e., PM2.5 ≤ 70 μg/m3, 70 < PM2.5 ≤ 100 μg/m3, and PM2.5 > 100 μg/m3, and assign each category a dummy variable, with PM2.5 ≤ 70 μg/m3 designated as the reference group. We estimate this model utilizing two IVs: thermal inversion strength and the number of occurrences.Footnote 19 Exposure to heavy air pollution, relative to the reference group, is found to be associated with a significant increase in medical expenditures.
In the previous analysis, we inferred the home address for each person from the location of the pharmacy that the person most often visited, and matched the air pollution from the nearest monitoring station. In column 4 of Table 5, we conduct a robustness check by calculating the weighted average of pollution of all the pharmacies/healthcare facilities a person visited, where the weight equals the number of visits. Our estimates are qualitatively unchanged after using the weighted average PM2.5.
In order to address the concern around using linear models for our dependent variable with a large share of zeros, we check the robustness of our main results by presenting estimates from the Correlated Random Effects Tobit (CRE Tobit) model with a lower limit zero. We implement a two-stage control function approach with bootstrapped standard errors using thermal inversion as an exclusion restriction to account for potential endogeneities.Footnote 20 We report the average partial effects in column 5 of Table 5. The CRE Tobit model produces positive and significant results and their magnitude implies an estimated WTP up to CNY61.90, which is similar to our 2SLS estimates. Therefore, the CRE Tobit model results suggest that our findings are generally robust to accounting for the limited dependent variable nature of our data.
In addition, in column 6 of Table 5, we replace the arcsinh transformation by a logarithmic transformation (i.e., ln(x + 1)), considering that the latter has been widely adopted in the literature. The IV estimate indicates that logarithmic transformation of the dependent variables would lead to a relatively smaller effect than the arcsinh case (as shown in column 1 of Table 5). Nevertheless, the similar magnitude of the estimated WTP suggests the robustness of using arcsinh transformation.
Furthermore, we conduct a robustness check by controlling for holiday-month-by-year fixed effects in order to better account for fluctuations in health spending brought about by holidays.Footnote 21 As revealed in column 7 of Table 5, our baseline result is robust to this change.
Finally, since we match individuals to their most-visited pharmacies and interpolate air pollution from the nearest monitoring station, the pollution variation comes at the healthcare facility level. We therefore further supplement our empirical analysis by aggregating the health expenditure data at the healthcare facility level. The results are displayed in Tables A3 through A5. Our main findings still hold and the patterns revealed by the heterogeneous analysis are similar.
4.3 Heterogeneous effects
In this section, we examine the heterogeneous effect of air pollution on health spending and estimate the associated WTP across subpopulations. First, we divide the whole sample into seven age cohorts of patients (0–10, 11–20, 21–30, 31–40, 41–50, 51–60, and 61 + years old) and then test the impact of PM2.5 for the seven age groups, separately by gender. Table 6 reports the results. Panel A refers to the estimates for males, while panel B is for females. As revealed in Table 6, males are generally more vulnerable to air pollution than their female counterparts. This finding is consistent with the literature, which shows that men’s hedonic happiness and cognitive performance are more affected than women’s (Zhang et al. 2018; Zhang et al. 2017a). Moreover, the young (aged 10 years and lower) and the old (aged 51 years and above) are more sensitive to air pollution than the middle-aged (11–50 years old). The more salient effects for young children and older adults are consistent with the findings in the literature on air pollution and health (He et al. 2016; Schlenker and Reed Walker 2016). Old people (61 years old and above) are on average more willing to pay the most for a 10 μg/m3 reduction in PM2.5: CNY 268.17 and CNY 138.47 per year for males and females, respectively.
In Table 7, we divide health spending into three categories: medication (including expenses in pharmacies and healthcare facilities), examination (including laboratory examination fees and imaging examination fees), and treatment (including non-surgical treatment fees, surgical treatment fees, and anesthesia fees). As shown in Table 7, healthcare expenditures in both medication and laboratory examination increase significantly with increasing PM2.5 concentration.
One unique feature of our dataset is that the records of health spending include expenditures in both pharmacies and all levels of healthcare facilities. In the first two columns of Table 7, we estimate the effect of PM2.5 on medication expenses by spending location. We find that the expenses at pharmacies are much more affected by air pollution. It is possible that people visit pharmacies instead of healthcare facilities for treatment for nonessential diseases during polluted days. Therefore, some of the impact of pollution on outpatient expenses can be absorbed in the rising drug expenses at pharmacies. This finding of stronger responses to air pollution in terms of more expenses at pharmacies is particularly important, which suggests that a narrow focus on medical expenditures in healthcare facilities may result in biased estimates.
5 Discussion
Our preferred specification shows that a 10 μg/m3 reduction in monthly average PM2.5 would lead to a 2.36% decrease in the value of health spending and a 0.79% decrease in the number of transactions in pharmacies and healthcare facilities. As the marginal effect of air pollution exposure on total health spending provides a lower bound WTP for improved air quality, our results indicate that people are willing to pay at least CNY 43.87 (or USD 7.09) per capita per year for a 10 μg/m3 reduction in PM2.5.Footnote 22
To better understand the size of our estimates, in Table A6, we compare our calculated WTP to others in the related literature. Generally, our WTP result is lower than the values estimated using other methods, since our approach provides only a lower bound related to the effect on healthcare spending. For example, Zhang et al. (2017b) find that people, on average, are willing to pay CNY 539 (USD 87.74, or 3.8% of annual household per capita income) per year per person for a 1 μg/m3 reduction in PM2.5.
Valuing air quality based on health spending data, Deryugina et al. (2019) find that a 10 μg/m3 increase in PM2.5 results in an increase in ER inpatient spending of USD 59.86 per capita per year among the population aged 65 years old or older. Williams and Phaneuf (2019) show that a 10 μg/m3 increase in PM2.5 results in a 33.1% increase in spending on asthma and chronic obstructive pulmonary disease (COPD). However, all of these studies utilize data from developed countries. Barwick et al. (2021) conduct the first study to examine the morbidity costs of air pollution in China using debit and credit card transactions aggregated at the city level. Their results suggest that a 10 μg/m3 reduction in PM2.5 over the past 90 days leads to a 1.5% decrease in the value of transactions, which is smaller than our estimates. Two issues may contribute to the difference. First, our individual-level longitudinal data allow us to remove individual heterogeneity in our estimations, thereby addressing preferences over the living environment. Second, older persons and low-income residents are more vulnerable to air pollution but less likely to use debit and credit cards; therefore, they tend to be excluded from the analysis in Barwick et al. (2021), resulting in a potential underestimation.
6 Conclusion
Previous studies in economics have mainly focused on examining the effects of exposure to air pollution on health factors, such as mortality and hospitalization. Far less is known about the ways in which air pollution affects medical expenditures, especially in developing countries. Our paper is among the first to estimate the morbidity costs of PM2.5 levels by using individual-level health spending data from both pharmacies and healthcare facilities for all age cohorts in China. We employ an IV strategy using thermal inversion as the instrument for the PM2.5 concentration in order to address the potential endogeneity in air pollution measures.
Our analysis shows that PM2.5 has a significant impact on medical expenditures. The estimates suggest that a 10 μg/m3 reduction in monthly average PM2.5 leads to a 2.36% decline in the value of health spending, in addition to a 0.79% decline in the number of transactions in pharmacies and healthcare facilities. This effect is more salient for males, children (10 years old or younger) and middle-aged and older adults (aged 51 or older). Valuing air quality by utilizing health spending data at the individual-monthly level, our estimates suggest that people are willing to pay CNY 43.87 (equivalent to 0.13% of disposal incomeFootnote 23) per capita per year for a 10 μg/m3 reduction in PM2.5.Footnote 24 The optimal environmental regulations depend on the tradeoffs between their costs and benefits. Our valuations of air quality provide useful insights into the benefits of tightening environment regulations.
Our study also has some limitations that call for further research. First, healthcare data are only available for one metropolitan, Wuhan, in China. As reimbursement schemes for outpatient care in other cities were not implemented during the sample period (2013–2015), which created a disincentive to seek care elsewhere for economic concerns, we cannot rule out the possibility that some medical spending may be mistakenly recorded as zero but may actually have been incurred in cities outside Wuhan. It also remains unknown to what extent we may generalize our findings to China or even developing countries in general. Future work examining the impact of air pollution on health spending will benefit from evidence from various areas. Second, we do not have data on ICD codes and therefore could not distinguish the impact of air pollution on various disease categories. Future research is warranted to collect and incorporate this information. Third, people who are more vulnerable to air pollution may even migrate to avoid more polluted areas in the long term (Chen et al. 2022). However, our IV estimates cannot fully address this concern on residential sorting. Finally, air pollution exposure is likely measured with errors, due to the aggregation of air pollution data from sporadic outdoor monitoring stations at the individual level.
Data availability
The data that support the findings of this study are available from the first author, Xin Zhang, upon reasonable request.
Notes
Medical expenses at pharmacies and healthcare facilities respectively account for 29.3% and 70.7% of the total spending in our data.
There are three main methods for valuing air quality. Each approach has its particular advantages and disadvantages. The hedonic approach infers the value of air quality from property values across regions with differing levels of air pollution exposure (Bayer, Keohane, and Timmins 2009; Chay and Greenstone 2005; Ito and Zhang 2020; Smith and Huang 1995). This approach generally suffers from omitted variable problems, which make the value of air quality endogenous. On the other hand, the contingent valuation method (CVM) directly asks about people’s WTP for better air quality (Sun, Yuan, and Yao 2016; Wang et al. 2015). However, this method is subject to the initial hypothetical monetary value adopted in the survey options and the manner in which the questions are framed. The happiness approach calculates the marginal rate of substitution between a reduction in air pollution and household per capita income by holding happiness constant to assess the monetary value of air pollution (Levinson 2012; Welsch 2006; Zhang et al. 2017b). This approach treats self-reported happiness as a proxy of utility and assumes that utility is comparable among respondents.
Refer to Appendix B for the theoretical model. The model illustrates that people’s WTP for clean air can be estimated by adding up different components of the impact of air pollution on the population’s health and behavior. The marginal effect of air pollution on health spending is just one of the components, other components include mortality impact, reduction in quality of life, and the sub-optimal level of consumption distortion by the exposure to pollution.
According to the 2018 Environmental Performance Index published by Yale University, the five countries with the most polluted air in the world are Nepal, Bangladesh, India, China, and Pakistan.
The UEBMI was launched in 1998 as an employment-based insurance program in urban areas, and its coverage reached 92% in 2010. The URBMI was launched in 2007 to target the unemployed, children, students, and the disabled in urban areas. It covered 93% of the target population as of 2010 (Yu 2015).
As medical expenses covered by the Chinese public health insurance programs are directly billed on medical payment cards, all the payments for people enrolled in public insurance programs—UEBMI and URBMI—are included in the official database by design. Any money saved in the insurance account can be conveyed to the next year. Using others’ insurance accounts to purchase any health services was not allowed during the sample period.
The medication expenses include Western medicine fees, Chinese patent medicine fees, and Chinese herb medicine fees. The examination expenses include laboratory examination fees and imaging examination (B ultrasound, CT and MRI) fees. The treatment expenses include non-surgical treatment fees, surgical treatment fees, and anesthesia fees.
The six air pollutant measures are particulate matter with a diameter smaller than 2.5 µm (PM2.5, fine particulates); particulate matter with a diameter smaller than 10 µm (PM10, coarse particulates); carbon monoxide (CO); nitrogen dioxide (NO2); ozone (O3); and sulfur dioxide (SO2).
Zhang et al. (2017b) suggest that people have a much greater WTP for a reduction in PM2.5 than they do for PM10.
For each individual, we calculate the number of visits to each pharmacy during the sample period and sort the number of visits in descending order. We pick the location of the pharmacy that a person visited most as their home address. If the person did not visit any pharmacy during the sample period, we choose the health facility that the person most often visited. The average number of pharmacies a person visited is 5.27.
The average matching distance between the residential address and the nearest monitoring station is 3.85 km.
We also conduct empirical analysis using data at the individual-daily level without assigning zeros, controlling for demographic variables, daily weather covariates, individual, pharmacy, county-by-year, month and day-of-week fixed effects. The results are displayed in Table A1. The pattern of the estimates is similar to those based on the individual-monthly level data. As we estimate the results only using the subsample for those whose healthcare expenses are positive, indicating that they may either tend to be less healthy or could afford more healthcare expenses, the estimated WTP becomes much larger.
58.7% of the value of health spending/number of transactions are zeros.
The arcsinh transformation is \(\mathrm{arcsinh}\left(\mathrm{y}\right)=\mathrm{ln}(\mathrm{y}+\sqrt{{y}^{2}+1})\).
In the estimable equation of the form \(\mathrm{arcsinh}\left(\mathrm{y}\right)=\mathrm{\alpha }+\mathrm{\beta x}+\upvarepsilon\), the semi-elasticity is \(\frac{\partial y}{\partial x}\cdot \frac{1}{y}=\widehat{\beta }\frac{\sqrt{{y}^{2}+1}}{y}\). As \(\underset{y\to \infty }{\mathrm{lim}}\frac{\sqrt{{y}^{2}+1}}{y}=1\), for large values of y, \(\frac{\partial y}{\partial x}\cdot \frac{1}{y}=\widehat{\beta }\). Therefore, \(\widehat{\beta }\) indicates a semi-elasticity in the arcsinh transformation of y of no less than 10, as suggested by Bellemare and Wichman (2020). Please refer to Bellemare and Wichman (2020) for details.
For example, the IV estimates are substantially (6–17 times) larger than the OLS estimates in (Deryugina et al. 2019).
Table A2 presents the correlations between air pollutants.
We tried to instrument for PM2.5 and another co-pollutant using the thermal inversion strength and the number of occurrences in columns (2)–(6) of Table 4. However, we could not pass the weak identification test.
See columns (2) through (3) of Table 2 for the first-stage estimates.
A similar practice can be found in Williams and Phaneuf (2019), who also study medical expenditure data with a large number of zeros.
The holiday month refers to the month that contains holidays.
Using the average 2013–15 exchange rate of USD 1 = CNY 6.1880 from the Wind Economic Database.
The average disposal income per capita per year of Wuhan urban residents during 2013–2015 was 33,175.87 yuan (Wuhan Statistical Yearbook 2016).
Considering that our current WTP measure only accounts for willingness to pay to mitigate pollution-related morbidity costs (excluding other health aspects of social costs, such as mortality costs and avoidance costs, like facemasks and air filters), and that our individual-monthly level sample has a large share of zero healthcare expenses (i.e., people in a healthy status or who could not afford medical treatment), our measured WTP as a share of disposal income should be a lower-bound estimate. When we instead measure using individual-daily data with positive healthcare expenses only, i.e., among those who were sick and who could afford medical treatment, our estimates suggest that these people are willing to pay much more (CNY 699.29; around 2.11% of average disposal income) per capita per year for the same 10 μg/m3 reduction in PM2.5.
References
Anderson ML (2020) As the wind blows: the effects of long-term exposure to air pollution on mortality. J Eur Econ Assoc 18(4):1886–1927. https://doi.org/10.1093/jeea/jvz051
Arceo E, Hanna R, Oliva P (2016) Does the effect of pollution on infant mortality differ between developing and developed countries? Evidence from Mexico City. Econ J 126(591):257–280. https://doi.org/10.1111/ecoj.12273
Barwick PJ, Li S, Rao D, Zahur NB (2021) The healthcare cost of air pollution: evidence from the world’s largest payment network. NBER Working Paper No. 24688. https://doi.org/10.3386/w24688
Bayer P, Keohane N, Timmins C (2009) Migration and hedonic valuation: the case of air quality. J Environ Econ Manag 58(1):1–14. https://doi.org/10.1016/j.jeem.2008.08.004
Bellemare MF, Wichman CJ (2020) Elasticities and the inverse hyperbolic sine transformation. Oxford Bull Econ Stat 82(1):50–61. https://doi.org/10.1111/obes.12325
Cameron CA, Gelbach JB, Miller DL (2008) Bootstrap-based improvements for inference with clustered errors. Rev Econ Stat 90(3):414–427. https://doi.org/10.1162/rest.90.3.414
Chay KY, Greenstone M (2003) The impact of air pollution on infant mortality: evidence from geographic variation in pollution shocks induced by a recession. Quart J Econ 118(3):1121–1167. https://doi.org/10.1162/00335530360698513
Chay KY, Greenstone M (2005) Does air quality matter? Evidence from the Housing Market. J Polit Econ 113(2):376–424. https://doi.org/10.1086/427462
Chen Y, Ebenstein A, Greenstone M, Li H (2013) Evidence on the impact of sustained exposure to air pollution on life expectancy from China’s Huai River policy. Proc Natl Acad Sci USA 110(32):12936–12941. https://doi.org/10.1073/pnas.1300018110
Chen S, Guo C, Huang X (2018) Air pollution, student health, and school absences: evidence from China. J Environ Econ Manag 92:465–497. https://doi.org/10.1016/j.jeem.2018.10.002
Chen Y, Jin GZ, Kumar N, Shi G (2012) Gaming in air pollution data lessons from China. B.E. J Econ Analys Policy 12(3). https://doi.org/10.1515/1935-1682.3227
Chen S, Oliva P, Zhang P (2022) The effect of air pollution on migration: evidence from China. J Dev Econ 156. https://doi.org/10.1016/j.jdeveco.2022.102833
Currie J, Neidell M (2005) Air pollution and infant health: what can we learn from California’s recent experience? Q J Econ 120(3):1003–1030. https://doi.org/10.1093/qje/120.3.1003
Currie J, Neidell M, Schmieder JF (2009) Air pollution and infant health: lessons from New Jersey. J Health Econ 28(3):688–703. https://doi.org/10.1016/j.jhealeco.2009.02.001
Deryugina T, Heutel G, Miller NH, Molitor D, Reif J (2019) The mortality and medical costs of air pollution: evidence from changes in wind direction. Am Econ Rev 109(12):4178–4219. https://doi.org/10.1257/aer.20180279
Deschênes O, Greenstone M, Shapiro JS (2017) Defensive investments and the demand for air quality: evidence from the NOx budget program. Ame Econ Rev 107(10):2958–2989. https://doi.org/10.1257/aer.20131002
Ebenstein A, Fan M, Greenstone M, He G, Zhou M (2017) New evidence on the impact of sustained exposure to air pollution on life expectancy from China’s Huai River policy. Proc Natl Acad Sci USA 114(39):10384–10389. https://doi.org/10.1073/pnas.1616784114
Ghanem D, Zhang J (2014) Effortless Perfection: do Chinese cities manipulate air pollution data? J Environ Econ Manag 68(2):203–225. https://doi.org/10.1016/j.jeem.2014.05.003
Greenstone M, Hanna R (2014) Environmental regulations, air and water pollution, and infant mortality in India. Am Econ Rev 104(10):3038–3072. https://doi.org/10.1257/aer.104.10.3038
Grossman M (1972) On the concept of health capital and the demand for health. J Polit Econ 80(2):223–255
He G, Fan M, Zhou M (2016) The effect of air pollution on mortality in China: evidence from the 2008 Beijing Olympic Games. J Environ Econ Manag 79:18–39. https://doi.org/10.1016/j.jeem.2016.04.004
Ito K, Zhang S (2020) Willingness to pay for clean air: evidence from air purifier markets in China. J Polit Econ 128(5):1627–1672. https://doi.org/10.1086/705554
Levinson A (2012) Valuing public goods using happiness data: the case of air quality. J Public Econ 96(9–10):869–880. https://doi.org/10.1016/j.jpubeco.2012.06.007
Liao L, Du M, Chen Z (2021) Air pollution, health care use and medical costs: evidence from China. Energy Econ 95. https://doi.org/10.1016/j.eneco.2021.105132
Liu YM, Ao CK (2021) Effect of air pollution on health care expenditure: evidence from respiratory diseases. Health Econ 30(4):858–875. https://doi.org/10.1002/hec.4221
Long Y, Wang J, Wu K, Zhang J (2018) Population exposure to ambient PM2.5 at the subdistrict level in China. Int J Environ Res Public Health 15(12). https://doi.org/10.3390/ijerph15122683
Moretti E, Neidell M (2011) Pollution, health, and avoidance behavior: evidence from the ports of Los Angeles. J Hum Res 46(1):154–175. https://doi.org/10.3368/jhr.46.1.154
Neidell M (2009) Information, avoidance behavior, and health: the effect of ozone on asthma hospitalizations. J Hum Resour 44(2):450–478. https://doi.org/10.1353/jhr.2009.0018
Pope CA, Dockery DW (2006) Health effects of fine particulate air pollution: lines that connect. J Air Waste Manag Assoc 56(6):709–742. https://doi.org/10.1080/10473289.2006.10464485
Roodman D, MacKinnon JG, Nielsen MØ, Webb MD (2019) Fast and wild: bootstrap inference in stata using boottest. Stata J 19(1):4–60. https://doi.org/10.1177/1536867X19830877
Schlenker W, Reed Walker W (2016) Airports, air pollution, and contemporaneous health. Rev Econ Stud 83(2):768–809. https://doi.org/10.1093/restud/rdv043
Smith VK, Huang J-C (1995) Can markets value air quality? A meta-analysis of hedonic property value models. J Polit Econ 103(1):209–227. https://doi.org/10.1086/261981
Sun C, Yuan X, Yao X (2016) Social acceptance towards the air pollution in China: evidence from public’s willingness to pay for smog mitigation. Energy Policy 92:313–324. https://doi.org/10.1016/j.enpol.2016.02.025
Sun C, Kahn ME, Zheng S (2017) Self-protection investment exacerbates air pollution exposure inequality in urban China. Ecol Econ 131:468–474. https://doi.org/10.1016/j.ecolecon.2016.06.030
Wang K, Jinyi Wu, Wang R, Yang Y, Chen R, Maddock JE, Yuanan Lu (2015) Analysis of Residents’ willingness to pay to reduce air pollution to improve children’s health in community and hospital settings in Shanghai, China. Sci Total Environ 533:283–289. https://doi.org/10.1016/j.scitotenv.2015.06.140
Welsch H (2006) Environment and happiness: valuation of air pollution using life satisfaction data. Ecol Econ 58(4):801–813. https://doi.org/10.1016/j.ecolecon.2005.09.006
Williams AM, Phaneuf DJ (2019) The morbidity costs of air pollution: evidence from spending on chronic respiratory conditions. Environ Resource Econ 74(2):571–603. https://doi.org/10.1007/s10640-019-00336-9
Xia F, Xing J, Jintao Xu, Pan X (2022) The short-term impact of air pollution on medical expenditures: evidence from Beijing. J Environ Econ Manag. https://doi.org/10.1016/j.jeem.2022.102680
Yu H (2015) Universal health insurance coverage for 1.3 billion people: what accounts for China’s success? Health Policy 119(9):1145–1152
Zhang J, Mu Q (2018) Air pollution and defensive expenditures: evidence from particulate-filtering facemasks. J Environ Econ Manag 92:517–536. https://doi.org/10.1016/j.jeem.2017.07.006
Zhang X, Zhang X, Chen Xi (2017) Happiness in the air: how does a dirty sky affect mental health and subjective well-being? J Environ Econ Manag 85:81–94. https://doi.org/10.1016/j.jeem.2017.04.001
Zhang X, Zhang X, Chen Xi (2017) Valuing air quality using happiness data: the case of China. Ecol Econ 137:29–36. https://doi.org/10.1016/j.ecolecon.2017.02.020
Zhang X, Chen Xi, Zhang X (2018) The impact of exposure to air pollution on cognitive performance. Proc Natl Acad Sci USA 115(37):9193–9197. https://doi.org/10.1073/pnas.1809474115
Acknowledgements
Xin Zhang acknowledges financial support from the National Natural Science Foundation of China (72003014). Xun Zhang thanks the National Natural Science Foundation of China (71973014) for financial support. Xi Chen is grateful for financial support from the James Tobin Research Fund at Yale Economics Department, Yale Macmillan Center Faculty Research Award (2017–2019), the U.S. PEPPER Center Scholar Award (P30AG021342, 2016–2018), NIH/NIA Career Development Award (K01AG053408, 2017–2022), and a NIH/NIA Research Award (R01AG077529, 2022-2027). The authors acknowledge helpful comments by participants and discussants at the various conferences, seminars and workshops, as well as from editor Kompal Sinha and three anonymous reviewers.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Responsible editor: Kompal Sinha
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhang, X., Zhang, X., Liu, Y. et al. The morbidity costs of air pollution through the Lens of Health Spending in China. J Popul Econ 36, 1269–1292 (2023). https://doi.org/10.1007/s00148-023-00948-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00148-023-00948-y