
Abstract
Introduction
While prone positioning (PP) has been shown to improve patient survival in moderate to severe acute respiratory distress syndrome (ARDS) patients, the rate of application of PP in clinical practice still appears low.
Aim
This study aimed to determine the prevalence of use of PP in ARDS patients (primary endpoint), the physiological effects of PP, and the reasons for not using it (secondary endpoints).
Methods
The APRONET study was a prospective international 1-day prevalence study performed four times in April, July, and October 2016 and January 2017. On each study day, investigators in each ICU had to screen every patient. For patients with ARDS, use of PP, gas exchange, ventilator settings and plateau pressure (Pplat) were recorded before and at the end of the PP session. Complications of PP and reasons for not using PP were also documented. Values are presented as median (1st–3rd quartiles).
Results
Over the study period, 6723 patients were screened in 141 ICUs from 20 countries (77% of the ICUs were European), of whom 735 had ARDS and were analyzed. Overall 101 ARDS patients had at least one session of PP (13.7%), with no differences among the 4 study days. The rate of PP use was 5.9% (11/187), 10.3% (41/399) and 32.9% (49/149) in mild, moderate and severe ARDS, respectively (P = 0.0001). The duration of the first PP session was 18 (16–23) hours. Measured with the patient in the supine position before and at the end of the first PP session, PaO2/FIO2 increased from 101 (76–136) to 171 (118–220) mmHg (P = 0.0001) driving pressure decreased from 14 [11–17] to 13 [10–16] cmH2O (P = 0.001), and Pplat decreased from 26 [23–29] to 25 [23–28] cmH2O (P = 0.04). The most prevalent reason for not using PP (64.3%) was that hypoxemia was not considered sufficiently severe. Complications were reported in 12 patients (11.9%) in whom PP was used (pressure sores in five, hypoxemia in two, endotracheal tube-related in two ocular in two, and a transient increase in intracranial pressure in one).
Conclusions
In conclusion, this prospective international prevalence study found that PP was used in 32.9% of patients with severe ARDS, and was associated with low complication rates, significant increase in oxygenation and a significant decrease in driving pressure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute respiratory distress syndrome (ARDS) is still associated with significant mortality [1]. To date, only three interventions have been proven efficient in improving patient survival [2], namely lower tidal volume (V T) [3] targeting 6 ml/kg predicted body weight (pbw), continuous intravenous infusion of the neuromuscular blocking agent (NMBA) cisatracurium for 48 h [4] and prolonged sessions of prone positioning [5]. These two latter interventions were, however, performed in selected ARDS patients, i.e. those with PaO2/FIO2 < 150 mmHg. The LUNG SAFE study [1], an international prospective epidemiological study conducted in 459 ICUs across the world in 2014, analyzed the treatment of 2377 ARDS patients and found that the above-mentioned interventions had not been widely adopted by clinicians. Specifically, the median V T was 7.7 ml/kg pbw and irrespective of the severity of hypoxemia, NMBA and PP were used in 37.8 and 16.3% of severe ARDS, respectively. The rate of prone position use was low despite the results of an individual meta-analysis [6] and a randomized controlled trial [5] that consistently showed benefits in selected patients. It was hypothesized that this low rate of prone positioning in ARDS patients in the LUNG SAFE study might be due in part to selection bias or a clinicians’ perception that the evidence level was weak. It is important to assess the prevalence of proning in ARDS patients to quantify the gap between the reality of daily practice and the use of an efficient intervention, and to identify any barriers that could be overcome. As the LUNG SAFE study was not focused specifically on ARDS but on acute hypoxemic respiratory failure, and was also not dedicated entirely to prone positioning, its results may have been biased. For this reason, we undertook a prospective observational international study with the primary aim of measuring the prevalence of use of the prone position in ARDS. Our hypothesis was that it was higher than found in the LUNG SAFE study. We based this assumption on the above considerations and on the fact that the publication of the Proseva trial [5] should be beginning to have an impact on routine clinical practice. Our secondary aims were to identify the reasons for not applying PP, the principal differences between proned and not proned ARDS patients, the physiologic response to and complications of spending extended periods of time in the prone position, and the concurrent treatments. This work was presented at the 2017 LIVES ESICM meeting [7].
Methods
Study design
A 1-day prevalence study was carried out four times: in April 2016, July 2016, October 2016 and January 2017. Each center participated as many times as it could and chose one of four predetermined calendar days (the 5th or 12th or 19th or 26th day of the month) for the study. Because it was a prevalence study, no patient follow-up was mandated. The protocol was drawn up by a steering committee and improved during regular meetings of the Acute Respiratory Failure Section of the European Society of Intensive Care Medicine (ESICM). It had been endorsed by the ESICM clinical trials group. The study was registered at the clinicaltrials.gov website (clinicalTrials.gov identifier: NCT02842788).
Selection of intensive care units
Intensive care units (ICUs) were recruited through the Réseau Européen de Recherche en Ventilation Artificielle (REVA) network and the Réseau recherche de la Société Française d’Anesthésie-Réanimation (SFAR-recherche) both in France and via the ESICM platform once the APRONET had been was endorsed by the ESICM clinical trials group. The ICUs participated on a voluntary basis in any of the four study times. The list of all registered ICUs on the ESICM platform was sent to the University Hospital of Angers France, where study staff were responsible for the electronic case record form (eCRF) and performed data extraction and management. Each center received a protected account and gained access to the system through an individual password to complete the eCRF. At each participating ICU, one physician was designated as investigator.
Inclusion criteria
-
ARDS criteria according to the Berlin definition [8] fulfilled on the day of the study. The onset of ARDS could have been established at any time between ICU admission and the study day, but ARDS criteria had to be met on the study day.
-
Age ≥ 18 years.
-
Intubated or tracheotomized and mechanically ventilated.
Exclusion criteria
-
Not intubated on the day of the study.
-
No ARDS on the day of the study even if ARDS criteria had been fulfilled between ICU admission and the study day.
Data collection
On each study day the investigator screened every patient who was present in the ICU for the whole day, and checked for ARDS criteria as defined on the first page of the eCRF (Fig. 1 ESM). If ARDS criteria were present, the investigator had to complete the following six sections of the eCRF: (1) general characteristics at the time of ICU admission (gender, age, origin, comorbidities, SAPSII score and anthropometric data), (2) ARDS characteristics at the time of study day (date of ARDS diagnosis, ARDS risk factors, V T, FIO2, PEEP and plateau pressure at the time of worst PaO2/FIO2 ratio in the supine position), (3) proning or not, with the reasons for not proning, (4) concurrent treatments for ARDS, (5) V T, FIO2, positive end-expiratory pressure (PEEP), PaO2, PaCO2, pH and plateau pressure before and after prone positioning, together with the duration of the session (6) complications during the prone position session. The data pertaining to the onset or to the end of the proning session could be recorded on the day before and/or the day after the scheduled study day (Fig. 1 ESM). If more than one proning session was delivered during the whole study period, items 5 and 6 were documented for each session.
Ethical issues
The protocol was approved by the ethics committee of Lyon, France (IRB identification number 9118) on July 9th, 2015. Informed consent was waived according the French law. This approval was valid for all participating centers in France. Centers in other countries obtained authorization to perform the study according to their national regulations. The database was approved by the CNIL in France. No patient personal data was recorded. The patient identification included ICU number, serial inclusion number and, according to local regulations, the first letter of the last name and first name.
Funding
The study was funded by a research grant from the Hospices Civils de Lyon and a research grant from the ESICM clinical trials group.
Data analysis
The variables are presented as median (1st–3rd quartiles) and absolute numbers (with percentages). The main endpoint, the prevalence of use of PP in ARDS patients, was computed for each center as the number of ARDS patients who were proned divided by the total number of ARDS patients in the ICU on the day of the study. The corresponding proportion was expressed together with its 95% confidence interval. The chi-square test was used to look for any trend across the four study days. If no significant differences were found across the four study days, the data were merged for analysis of the secondary endpoints, namely the reasons for not proning, the characteristics of ARDS patients at the time of ICU admission and study inclusion, the physiological effects of the first proning session, the complications during the first proning session and the concurrent treatments.
Among the reasons for not proning, we placed special emphasis on oxygenation. Based on the previously reported low rate of PP use in severe ARDS, we were expecting that clinicians would not choose to put patients in the prone position because they would judge the hypoxemia as not severe enough. We assessed the reasons for not proning due to insufficiently severe hypoxemia in different ways. First, the rate of use of prone positioning was measured between ARDS stages [8]. Second, we defined patients retrospectively by whether or not they fulfilled the criteria of inclusion in the Proseva trial [5]: PaO2/FIO2 < 150 mmHg, PEEP ≥ 5 cm H2O, FIO2 ≥ 0.60, V T = 6 ml/kg pbw on the day of the study. Third, we split the values of PaO2/FIO2 measured on the study days into quintiles and for each of them, we measured the odds ratio (with 95% confidence intervals, 95% CI) of the PP. In each quintile, the odds ratio was analyzed using the Z test.
Proned and nonproned patients were further compared between European and non-European countries. Driving pressure was computed as plateau pressure minus PEEP. Groups were compared by using parametric or nonparametric tests as appropriate. Variables before and after the proning sessions were compared by using nonparametric or parametric tests for paired values. Binary multivariate logistic regression analysis was performed on the risk factors for not proning ARDS patients, which was the dependent variable, and adjusted for the ICU. The covariates were those which differed at the threshold of 0.20 in the univariate comparison between proned and nonproned ARDS patients during the four periods.
Only the pertaining to the first proning session were analyzed because we expected a very low number of patients with more than one proning session during the study period. The patients with additional proning sessions were, however, counted and are reported in the results section. The database was cleared after two sets of queries were sent to the centers and frozen on June 30 2017. The missing data for each variable can be found in Table 1 in the electronic supplementary material (ESM). They were checked for missing data at random, which was confirmed. The data were analyzed by one person (LA) using SPSS and EpiINFO softwares. P < 0.05 was considered as the threshold of statistical significance.
Results
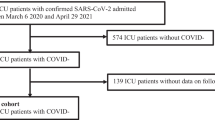
A total of 6,723 patients were screened over the four study days. Of these, 735 patients in 141 ICUs of 20 countries (ESM Table 2) fulfilled the criteria of ARDS (Fig. 1). ARDS had been diagnosed 4.5 (1-11) days before the study day. The prevalence of ARDS on each study day was 13.3% (11.7–14.9; 240/1808) in April 2016, 8.9% (7.5–10.3; 143/1611) in July 2016, 9.9% (8.4–11.4; 157/1593) in October 2016 and 11.4% (9.9–12.9; 195/1711) in January 2017 (P = 0.134).

Flow chart for the four study days. IMV invasive mechanical ventilation
Prevalence of prone position use
Over the four study days, 101 ARDS patients underwent at least one session of prone positioning (13.7%). Nine patients had a second proning session on the same study day, the data of which were not analyzed. The prevalence of PP in ARDS patients did not differ significantly across study days: it was 13.8% (9.4–18.2; 32/240) in April 2016, 12.6% (7.2–18.0; 18/143) in July 2016, 15.3% (9.7–20.9; 24/157) in October 2016 and 13.8% (9.0–18.6; 27/195) in January 2017 (P = 0.83; Fig. 2 ESM). With the four study days merged, the rate of proning use was 5.9% (2.5–9.3; 11/187), 10.3% (7.3–13.3; 41/399) and 32.9% (25.4–40.4; 49/149) in mild, moderate and severe ARDS, respectively (P = 0.0001; Fig. 2 ESM). In ARDS patients who met the Proseva criteria as defined for the present study (11.2% of the whole cohort), the rate of proning was 40.2% (29.6–50.8; 33/82) versus 10.4% (8.1–12.7; 68/653) in those who did not meet the Proseva criteria (P = 0.0001).
Reasons for not proning
The reasons for not proning are listed in Table 1. The primary reason, which accounted for 64.3% of cases, was clinicians’ assessment of hypoxemia as not severe enough to justify proning. Its frequency was significantly lower in severe ARDS than in mild or moderate ARDS. The distribution of patients across the five quintiles of PaO2/FIO2 showed that 50.8% of patients with PaO2/FIO2 < 138 mmHg received proning (Fig. 2). The quintile with PaO2/FIO2 < 100 mmHg was associated with a significant (fivefold) likelihood of proning whilst above a threshold of 139 mmHg, there was a significant probability of not proning (Fig. 2). The second most commonly occurring reason for not proning was having mean arterial pressure lower than 65 mmHg (5.7%) followed by end-of-life decision (4.2%), both of which were significantly more frequent in severe ARDS than in mild or moderate ARDS. The other reasons accounted for less than 4% of the total number of reasons and did not differ among the three stages of ARDS, with the exception of abdominal problems which were cited more often in severe ARDS. In patients meeting the Proseva criteria, the reasons for not proning were insufficiently severe hypoxemia, chest trauma and end-of-life decision (Table 3 ESM).

Odds ratio for the rate of use of prone positioning across PaO2/FIO2 quintiles. *P < 0.0001 for total prone group (χ 2 test), † P < 0.05, ‡ P < 0.001 (Z test). Squares are odds ratio and horizontal bars joining low to high 95% confidence intervals
The patients who were proned differed from those who were not proned in higher frequency of ARDS originating from pneumonia, more severe hypoxemia, higher PEEP and higher plateau pressure at the time of inclusion (Table 2). The multivariate logistic regression analysis found that PaO2/FIO2 < 150 mmHg, V T < 6 ml/kg pbw and PEEP > 10 cm H2O at the time of inclusion were significantly associated with a lower probability of prone positioning not being used, i.e. with a greater likelihood of proning. Conversely, the higher the SAPS II and the higher the plateau pressure, the greater the probability of proning not being used (Table 3).
Physiological response to the session in prone position
The duration of the first prone positioning session over the four study days was 18 (16–23) hours without interruption.
Measured with the patient in the supine position before and after the first PP session, PaO2/FIO2 increased from 101 (76–136) to 171 (118–220) mmHg (P = 0.0001) and driving pressure and Pplat decreased from 14 (11–17) to 13 (10–16) cmH2O (P = 0.001) and from 26 (23–29) to 25 (23–28) cmH2O (P = 0.04), respectively (Table 4 ESM). PaCO2 and V T did not change and PEEP was essentially the same in the supine and prone positions (Table 4 ESM).
Complications of the prone position session
Complications related to sessions of prone positioning were reported in 12 of the 101 proned patients (11.9%) (ESM Table 5): endotracheal tube-related complications in 2 patients, hypoxemia in 2, ocular complications in 2, pressure sores in 5 and a transient increase in intracranial pressure in 1. One death was notified, which was not due to the procedure.
Concurrent treatments
Proned ARDS patients more frequently received vasopressors, inhaled nitric oxide, sedation and neuromuscular blockade than those who were not proned (Table 6 ESM).
Discussion
The main findings of this study are that: (1) the rate of use of PP was higher than previously reported for severe ARDS in the Lung Safe study, (2) the major reason for not proning was related to the severity of hypoxemia and (3) the rate of complications was much lower than previously reported in trials comparing prone and supine positioning in patients with ARDS or hypoxemic respiratory failure.
This is the first prospective multicenter international study dedicated specifically to the use of PP in ARDS patients. Previous large observational studies on the practice of mechanical ventilation in the ICU provided some information on the rate of use of proning in ARDS patients (Table 7 ESM). The decline in the use of proning observed between the first [9] and the second [10] international survey led by Esteban et al. followed the early negative trials [11, 12]. However, in spite of the positive signals from individual data meta-analysis [6] and three most recent trials [5, 13, 14], PP was still infrequently used in the subsequent international observational studies [1, 15]. The LUNG SAFE study extended these results by showing that actually the use of proning depended on the severity of hypoxemia, from 1% in mild to 5.5% in moderate and to 16.3% in severe ARDS [1]. In the present study, a twofold increase in the rate of use of proning since the LUNG SAFE study was observed, with similar increases across the ARDS stages culminating in 32.9% in severe ARDS category and 24% in ARDS patients with PaO2/FIO2 < 150 mmHg + PEEP ≥ 10 cmH2O and FIO2 ≥ 60%. The rate of use of PP was consistent; it did not vary significantly across the four study days. The difference in the use of the prone position between LUNG SAFE and the present study may reflect a selection bias of centers, as most of the ICUs were located in France, Spain and Italy, where PP has been used for many years in ARDS patients and where most of the large clinical trials on PP have been conducted so far. This is very different from the LUNG SAFE study in which about half of the patients were enrolled in non-European countries. Indeed, a secondary analysis of the LUNG SAFE database [16] has shown that the use of PP in high-income countries is eight times greater in Europe than in the rest of the world. However, we found that the rate of proning use was higher in non-European than in European countries: (28.6 vs. 13%; P = 0.019). This is surprising, but should be interpreted with caution, as the proportion of ARDS patients from non-European countries in the present study was small (4.8%) and much lower than in the LUNG SAFE study (46%). One possible explanation for this finding is that the non-European ICUs in our study are strong believers in prone positioning.
It is possible that our results regarding the rate of use of proning (from data collected 2 years after LUNG SAFE) reflect a change in practice. If clinicians are indeed less reluctant to use PP, the reason may be wider better dissemination and a positive perception of the results of the last trial [5]. The Proseva trial showed a significantly improved benefit-to-risk ratio of using PP, a finding that should make clinicians keener to implement this strategy in their ICU. However, this does not explain why the proportion of patients with severe ARDS in whom prone positioning was used was not higher in the present study. The best PaO2-to-FIO2 ratio to use as threshold in determining the indication fore prone positioning is still being debated. The meta-analysis based on individual data found benefit for ARDS patients with PaO2/FIO2 < 100 mmHg [6], in line with a meta-analysis based on grouped data [17], whilst for the Proseva trial, the benefit was obtained below 150 mmHg [5]. The mean PaO2-to-FIO2 ratio at the time of randomization in this trial was 100 mmHg for both groups in the Proseva trial [5]. However, survival was better in the prone group than in the supine group over the whole 49–150-mmHg range of PaO2/FIO2 at the time of randomization [5]. Further grouped-data meta-analyses confirmed the benefit of proning in patients with moderate to severe ARDS [18, 19]. The multivariate analysis of the present data showed that a PaO2-to-FIO2 ratio < 150 mmHg had the lowest odds ratio for prediction of the risk of not being proned. In the present study, 40.2% of the patients meeting the Proseva criteria were proned. This means that 49 patients who fulfilled those criteria were not placed in the prone position. It should be mentioned that our study design obviously did not replicate the Proseva trial. Of note, neither the exclusion criteria of the Proseva trial nor the 12–24-h stabilization period were satisfied by our study design.
The primary reason for not proning ARDS patients in the present study was related to clinicians’ judgment of hypoxemia as not being severe enough to justify PP for that specific patient. As would be expected, this reason was observed significantly less frequently in patients with severe ARDS than in those with mild or moderate ARDS. The fact that, even in severe ARDS, many clinicians rated the hypoxemia not severe enough to justify proning suggests that PP is still viewed as a rescue maneuver. However, PP is a method to prevent/attenuate ventilator-induced lung injury [20] and to improve/stabilize hemodynamics [21] and therefore should be applied irrespective of the level of hypoxemia, at least in the subgroup of patients with a PaO2-to-FIO2 ratio < 150 mmHg, in whom benefit was shown. Furthermore, defining ARDS as severe only on the basis of the level of hypoxemia may not be enough. Even if it is true that, on average, the amount of lung tissue increased with the severity of hypoxemia [22], for a given patient the relationship between excess in lung tissue volume and hypoxemia may be less strong. Therefore, and from the specific perspective of PP, other markers for ARDS severity could be used, such as lung morphology as assessed on the CT scan. Further studies are needed to better define ARDS severity and investigate specific interventions such as PP [23]. The second most important reason for not proning patients with severe ARDS was hemodynamic instability. This finding suggests that the possible hemodynamic benefits of proning [24] are still widely unknown among ICU physicians. The other reasons for not using prone positioning were rare, less than 5%. However, the fact that ECMO was the reason for not proning in 1.9% of the cases be related to the rate of use of ECMO in our study, which was half that in the LUNG SAFE study. Obesity was a reason for not using prone positioning in five patients in the present study. However, it has been shown that obese patients can not only be turned prone safely but also benefit from proning more than the non-obese in terms of oxygenation [25]. An increase in the use of proning to treat patients with ARDS may result from evidence showing that using criteria other than oxygenation in deciding whether to prone patients, such as the focal morphological kind of ARDS [26], may be beneficial to the patients. Given that hemodynamic problems are also cited as a reason for not placing patients in the prone position, further data should be provided to confirm the hemodynamic benefit of proning. Findings showing that proning can be done safely after abdominal surgery [27] should be confirmed by trials in specific settings such as trauma, abdominal or cardiac surgery.
Surprisingly, the rate of complications attributed to PP in the present study was very low. For instance, only two complications related to artificial airways were reported. This differs from the results of previous trials on PP. Mancebo et al. found that 7.9% of proned patients had unplanned extubation [13], Taccone et al. reported a 10.7% rate of endotracheal tube displacement [14] and Guérin et al. described a 13.3% rate of non-scheduled extubation with 2.5% main-stem bronchus intubation and 4.9% endotracheal tube obstruction [5]. The low rate of airways-related complications in the present study may reflect improvement in practice, ICU selection bias or underestimation. The rate of pressure sores found in the present study is also very much lower than previously reported. However, we did not assess the rate of complications in patients who were not proned. It should be mentioned that the one death reported was not related to the procedure.
The physiological response to the first session of prone positionning confirms the well-known finding of significant improvement in oxygenation. In our sample, the reduction in driving pressures at similar V T presumably reflects improvement in respiratory system compliance. The effect of PP on respiratory mechanics is complex and not consistent across trials. Respiratory system compliance was found to be increased in the prone versus the supine position in one trial [13] but unchanged in another [5]. We found a significant decrease in respiratory driving pressure in the prone position. This is an important finding as driving pressure has recently been suggested to be the strongest predictor of death in ARDS patients [28]. It is worth mentioning that in the present study, plateau pressure was measured in 90.7% of patients (667/735 ARDS patients), a much higher proportion than in the LUNG SAFE study where Pplat was determined in 40% of patients overall and 48.5% of those undergoing controlled ventilation. This result may reflect ICU selection bias or improvement in practice since the publication of the LUNG SAFE study.
Our study has limitations. Centers were informed in advance about the study days and, hence, may have adapted their practice accordingly. There may well be a selection bias in the participating ICUs, whose staff are likely to be proponents of and trained in proning. Furthermore, the data were not recorded during a long prospective period but only on four (separate) days. However, the fact that the rate of proning was not different across the four study days is an argument against any real bias in the present study. Our study was underpowered. We computed a posterior that, at α and β risks of 5 and 20%, respectively, 884 patients with ARDS would have needed to be enrolled for the overall prevalence of PP of 13.7% in this and 7.9% in the Lung SAFE study to be shown to be significantly different.
In conclusion, this prospective international prevalence study found that PP was used in 32.9% of severe ARDS and was associated with a low rate of complications, a significant increase in oxygenation, and a significant decrease in driving pressure.
References
Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A (2016) Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 315:788–800
Tonelli AR, Zein J, Adams J, Ioannidis JP (2014) Effects of interventions on survival in acute respiratory distress syndrome: an umbrella review of 159 published randomized trials and 29 meta-analyses. Intensive Care Med 40:769–787
ARDSnet (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 342:1301–1308
Papazian L, Forel JM, Gacouin A, Penot-Ragon C, Perrin G, Loundou A, Jaber S, Arnal JM, Perez D, Seghboyan JM, Constantin JM, Courant P, Lefrant JY, Guerin C, Prat G, Morange S, Roch A (2010) Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med 363:1107–1116
Guerin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, Mercier E, Badet M, Mercat A, Baudin O, Clavel M, Chatellier D, Jaber S, Rosselli S, Mancebo J, Sirodot M, Hilbert G, Bengler C, Richecoeur J, Gainnier M, Bayle F, Bourdin G, Leray V, Girard R, Baboi L, Ayzac L, Group PS (2013) Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 368:2159–2168
Gattinoni L, Carlesso E, Taccone P, Polli F, Guerin C, Mancebo J (2010) Prone positioning improves survival in severe ARDS: a pathophysiologic review and individual patient meta-analysis. Minerva Anestesiol 76:448–454
Guérin C, Beuret P, Constantin JM, Bellani G, Baboi L, Mercat A, Chrétien JM, François G (2017) A prospective international observational one-day prevalence study on prone positioning in ARDS. The APRONET study. Intensive Care Med Exp 5:44
Ranieri VM, Rubenfeld GD, Thompson BT, Fergsuon ND, Cladwell E, Fan E, Camporota L, Slutsky AS (2012) Acute Respiratory Distress Syndrome. The Berlin definition. JAMA 307:E1–E8
Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart TE, Benito S, Epstein SK, Apezteguia C, Nightingale P, Arroliga AC, Tobin MJ (2002) Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA 287:345–355
Esteban A, Ferguson ND, Meade MO, Frutos-Vivar F, Apezteguia C, Brochard L, Raymondos K, Nin N, Hurtado J, Tomicic V, Gonzalez M, Elizalde J, Nightingale P, Abroug F, Pelosi P, Arabi Y, Moreno R, Jibaja M, D’Empaire G, Sandi F, Matamis D, Montanez AM, Anzueto A (2008) Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med 177:170–177
Gattinoni L, Tognoni G, Pesenti A, Taccone P, Mascheroni D, Labarta V, Malacrida R, Di Giulio P, Fumagalli R, Pelosi P, Brazzi L, Latini R (2001) Effect of prone positioning on the survival of patients with acute respiratory failure. N Engl J Med 345:568–573
Guerin C, Gaillard S, Lemasson S, Ayzac L, Girard R, Beuret P, Palmier B, Le QV, Sirodot M, Rosselli S, Cadiergue V, Sainty J-M, Barbe P, Combourieu E, Debatty D, Rouffineau J, Ezingeard E, Millet O, Guelon D, Rodriguez L, Martin O, Renault A, Sibille J-P, Kaidomar M (2004) Effects of systematic prone positioning in hypoxemic acute respiratory failure: a randomized controlled trial. JAMA 292:2379–2387
Mancebo J, Fernandez R, Blanch L, Rialp G, Gordo F, Ferrer M, Rodriguez F, Garro P, Ricart P, Vallverdu I, Gich I, Castano J, Saura P, Dominguez G, Bonet A, Albert RK (2006) A multicenter trial of prolonged prone ventilation in severe acute respiratory distress syndrome. Am J Respir Crit Care Med 173:1233–1239
Taccone P, Pesenti A, Latini R, Polli F, Vagginelli F, Mietto C, Caspani L, Raimondi F, Bordone G, Iapichino G, Mancebo J, Guerin C, Ayzac L, Blanch L, Fumagalli R, Tognoni G, Gattinoni L (2009) Prone positioning in patients with moderate and severe acute respiratory distress syndrome: a randomized controlled trial. JAMA 302:1977–1984
Esteban A, Frutos-Vivar F, Muriel A, Ferguson ND, Penuelas O, Abraira V, Raymondos K, Rios F, Nin N, Apezteguia C, Violi DA, Thille AW, Brochard L, Gonzalez M, Villagomez AJ, Hurtado J, Davies AR, Du B, Maggiore SM, Pelosi P, Soto L, Tomicic V, D’Empaire G, Matamis D, Abroug F, Moreno RP, Soares MA, Arabi Y, Sandi F, Jibaja M, Amin P, Koh Y, Kuiper MA, Bulow HH, Zeggwagh AA, Anzueto A (2013) Evolution of mortality over time in patients receiving mechanical ventilation. Am J Respir Crit Care Med 188:220–230
Laffey JG, Kavanagh BP (2017) Fifty years of research in ARDS. Insight into Acute Respiratory Distress Syndrome. From models to patients. Am J Respir Crit Care Med 196:18–28
Sud S, Friedrich JO, Taccone P, Polli F, Adhikari NK, Latini R, Pesenti A, Guerin C, Mancebo J, Curley MA, Fernandez R, Chan MC, Beuret P, Voggenreiter G, Sud M, Tognoni G, Gattinoni L (2010) Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: systematic review and meta-analysis. Intensive Care Med 36:585–599
Sud S, Friedrich JO, Adhikari NK, Taccone P, Mancebo J, Polli F, Latini R, Pesenti A, Curley MA, Fernandez R, Chan MC, Beuret P, Voggenreiter G, Sud M, Tognoni G, Gattinoni L, Guerin C (2014) Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: a systematic review and meta-analysis. CMAJ 186:E381–E390
Lee JM, Bae W, Lee YJ, Cho YJ (2014) The efficacy and safety of prone positional ventilation in acute respiratory distress syndrome: updated study-level meta-analysis of 11 randomized controlled trials. Crit Care Med 42:1252–1262
Broccard A, Shapiro RS, Schmitz LL, Adams AB, Nahum A, Marini JJ (2000) Prone positioning attenuates and redistributes ventilator-induced lung injury in dogs. Crit Care Med 28:295–303
Jozwiak M, Teboul JL, Monnet X (2014) Reply: prone positioning actually exerts benefits on hemodynamics! Am J Respir Crit Care Med 189:1567–1568
Cressoni M, Cadringher P, Chiurazzi C, Amini M, Gallazzi E, Marino A, Brioni M, Carlesso E, Chiumello D, Quintel M, Bugedo G, Gattinoni L (2014) Lung inhomogeneity in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med 189:149–158
Jaber S, Bellani G, Blanch L, Demoule A, Esteban A, Gattinoni L, Guerin C, Hill N, Laffey JG, Maggiore SM, Mancebo J, Mayo PH, Mosier JM, Navalesi P, Quintel M, Vincent JL, Marini JJ (2017) The intensive care medicine research agenda for airways, invasive and noninvasive mechanical ventilation. Intensive Care Med. https://doi.org/10.1007/s00134-017-4896-8
Jozwiak M, Teboul JL, Anguel N, Persichini R, Silva S, Chemla D, Richard C, Monnet X (2013) Beneficial hemodynamic effects of prone positioning in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med 188:1428–1433
De Jong A, Molinari N, Sebbane M, Prades A, Futier E, Jung B, Chanques G, Jaber S (2013) Feasibility and effectiveness of prone position in morbidly obese patients with ARDS: a case-control clinical study. Chest 143:1554–1561
Puybasset L, Cluzel P, Gusman P, Grenier P, Preteux F, Rouby JJ (2000) Regional distribution of gas and tissue in acute respiratory distress syndrome. I. Consequences for lung morphology. CT Scan ARDS Study Group. Intensive Care Med 26:857–869
Gaudry S, Tuffet S, Lukaszewicz AC, Laplace C, Zucman N, Pocard M, Costaglioli B, Msika S, Duranteau J, Payen D, Dreyfuss D, Hajage D, Ricard JD (2017) Prone positioning in acute respiratory distress syndrome after abdominal surgery: a multicenter retrospective study: SAPRONADONF (Study of Ards and PRONe position After abDOmiNal surgery in France). Ann Intensive Care 7:21
Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, Stewart TE, Briel M, Talmor D, Mercat A, Richard JC, Carvalho CR, Brower RG (2015) Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med 372:747–755
Acknowledgments
The investigators of the APRONET Study Group (listed in the accompanying table of investigators), the REVA Network, the Réseau recherche de la Société Française d’Anesthésie-Réanimation (SFAR-recherche) and the ESICM Trials Group.
Table of investigators
Country | City | Name of the ICU | Name of the hospital | Collaborator #1 | Collaborator #2 | Head of the ICU or department |
|---|---|---|---|---|---|---|
Tunisia | Tunis | Critical Care Medicine and Anesthesiology | Military hospital for instruction of Tunis | HAJJEJ Zied | SELLAMI Walid | FERJANI M |
India | Lucknow | Critical Care Medicine | Sanjay Gandhi Postgraduate Institute of Medical Sciences | GURJAR Mohan | ||
Saudi Arabia | Abha | Intensive care unit | Asher Central Hospital | ASSIRI Amer | AL BSHABSHE Ali | |
Saudi Arabia | Riyadh | Intensive care unit | Prince Sultan Military Medical City | ALMEKHLAFI Ghaleb | MANDOURAH Yasser | |
Malaysia | Kuala Lumpur | Intensive Care Unit | University Malaya Medical Centre | HASAN Mohd Shahnaz | RAI Vineya | MARZIDA M |
Spain | Albacete | Servicio Medicina intensiva | Hospital General de Albacete | CORCOLES GONZALEZ Virgilio | SANCHEZ INIESTA Rafael | |
Spain | Madrid | Intensive Care Unit | H.G.U Gregorio Marañon | GARCIA Pablo | ||
Spain | Pamplona | Intensive Care Unit | Complejo Hospitalario De Navarra | GARCIA-MONTESINOS DE LA PEÑA Manuel | GARCIA HERRERA Adriana | |
Spain | Barcelone | Vall d’Hebron—Critical Care Department | Hospital Universitari Vall d’Hebron | ROCA Oriol | GARCIA-de-ACILU Marina | |
Spain | Barcelone | Del Mar—Anestesiología y Reanimación | Hospital del Mar | MASCLANS ENVIZ Joan Ramon | ||
Spain | Barcelone | San Pau—Anestesiología y Reanimación | Hospital Sant Pau | MANCEBO Jordi | ||
Spain | Madrid | Unidad de Cuidados Intermedios Respiratorios | Hospital Fundación Jiménez Díaz-Quirón Salud | CALVO NATIVIDAD Arias Cesar Peset | HEILI Sarah Frades | |
Spain | Sabadell | Intensive Medicine Service | Hospital Parc Tauli | ARTIGAS RAVENTOS Antonio | BLANCH TORRA Lluís | |
Spain | Tortosa | Medicina intensiva | Hospital Verge de la Cinta | ROCHE-CAMPO Ferran | ||
Spain | Palma de Mallorca | Intensive Care Department | Hospital Son Llàtzer | RIALP Gemma | FORTEZA Catalina | |
Spain | Burgos | Intensive Care Unit | Hospital Universitario de Burgos | BERRAZUETA Ana | MARTINEZ Esther | |
Spain | Getafe | Intensive Care Unit | Hospital Universitario de Getafe | PENUELAS Oscar | ||
Spain | Murcia | Servicio de Medicina Intensiva | Hospital Clínico Universitario Virgen de la Arrixaca | JARA-RUBIO Ruben | ||
France | Lens | Réanimation Polyvalente | Centre Hospitalier de Lens | MALLAT Jihad | THEVENIN D | |
France | Amiens | Réanimation Chirurgicale | Centre Hospitalier universitaire d’Amiens | ZOGHEIB Elie | ||
France | Angers | Réanimation Médicale | Centre Hospitalier universitaire d’Angers | MERCAT Alain | ||
France | Annecy | Réanimation Polyvalente | Centre Hospitalier Annecy Genevois | LEVRAT Albrice | ||
France | Annonay | Réanimation Polyvalente | Centre Hospitalier Annonay | POROT Veronique | BEDOCK B | |
France | Antibes | Réanimation Polyvalente | Centre Hospitalier Antibes | GRECH Ludovic | ||
France | Argenteuil | Réanimation Polyvalente | Hopital Victor Dupouy | PLANTEFEVE Gaetan | ||
France | Belfort | Réanimation Polyvalente | Hopital Nord Franche Comtè | BADIE Julio | ||
France | Besançon | Réanimation Chirurgicale | Centre Hospitalier Universitaire Jean Minjoz | BESCH Guillaume | PILI-FLOURY Sébastien | |
France | Bordeaux | Réanimation Médicale | Hopital Saint André | GUISSET Olivier | ||
France | Bourg en Bresse | Réanimation Médicale | Centre hospitalier Bourg en Bresse | ROBINE Adrien | ||
France | Brest | Réanimation Medicale | CHRU Cavale Blanche | PRAT Gwenael | ||
France | Chalon sur Saone | Réanimation Médicale | Centre Hospitalier de Chalon sur Saone | DOISE Jean-Marc | ||
France | Chambéry | Réanimation Polyvalente | Centre Hospitalier Metropole Savoie | BADET Michel | THOURET JM | |
France | Charleville-Mézières | Réanimation Polyvalente | Centre Hospitalier de Charleville-Mézières | JUST Bernard | ||
France | Clermond -Ferrand | Réanimation Médico-Chirurgicale | Centre Hospitalier Universitaire Clermond -Ferrand | PERBET Sébastien | ||
France | Clermond -Ferrand | Réanimation Médicale Polyvalente | Centre Hospitalier Universitaire Clermond -Ferrand | LAUTRETTE Alexandre | SOUWEINE B | |
France | Clermond -Ferrand | Neuro Réanimation | Centre Hospitalier Universitaire Clermond -Ferrand | CHABANNE Russell | ||
France | Brest | Réanimation Polyvalente | Hôpital d’Instruction des Armées Clermont Tonnerre | DANGUY DES DÉSERTS Marc | ||
France | Dieppe | Réanimation Polyvalente | Centre Hospitalier de Dieppe | RIGAUD Jean-Philippe | MARCHALOT Antoine | RIGAUD JP |
France | Draguignan | Réanimation Polyvalente | Centre Hospitalier de Draguignan | BELE Nicolas | ||
France | Dunkerque | Réanimation Chirurgicale | Centre Hospitalier de Dunkerque | BEAGUE Sébastien | ||
France | Corbeil-Essones Cedex | Réanimation Polyvalente | Centre Hospitalier Sud Francilien | HOURS Sandrine | MARQUE Sophie | |
France | Grenoble | Réanimation Cardiovasculaire et Thoracique | Hopital Michallon | DURAND Michel | PAYEN JF | |
France | Villejuif | Réanimation USCM | Institut Gustave Roussy Cancer Campus | STOCLIN Annabelle | GAFFINEL Alain | |
France | La Réunion | Réanimation Polyvalente | Centre Hospitalier Universitaire de la Réunion | WINER Arnaud | ||
France | LeMans | Réanimation Medico—Chirurgicale | Centre Hospitalier de LeMans | CHUDEAU Nicolas | TIROT Patrice | |
France | Longjumeau | Réanimation Polyvalente | Centre Hospitalier des Deux Vallées | THYRAULT Martial | PAULET Rémi | THYRAULT M |
France | Lyon | Reanimation chirurgicale | Hospices Civils de Lyon, Hôpital Croix Rousse | AUBRUN Frederic | ||
France | Lyon | Réanimation Médicale | Hospices Civils de Lyon, Hôpital Croix Rousse | GUERIN Claude | ||
France | Lyon | Réanimation HEH Gréa | Hospices Civils de Lyon, Hôpital Edouard Herriot | FLOCCARD Bernard | RIMMELE T | |
France | Lyon | Réanimation HEH Nréa | Hospices Civils de Lyon, Hôpital Edouard Herriot | ARGAUD Laurent | HERNU Romain | |
France | Lyon | Réanimation HEH Préa | Hospices Civils de Lyon, Hôpital Edouard Herriot | CROZON CLAUZEL Jullien | ||
France | Lyon | Réanimation Desgenettes | Hôpital d’instruction des armées Desgenettes | WEY Pierre-François | ||
France | Lyon | Réanimation Polyvalente Saint Joseph | Centre Hospitalier Saint Joseph—Saint Luc | BOURDIN Gael | POMMIER C | |
France | Mâcon | Réanimation Médicale | Centre Hospitalier des Chanaux | CUEUILLE Nadège | DE VARAX | |
France | Marseille | Réanimation DRIS | Hopital Nord | MARCHI Elisa | PAPAZIAN L | |
France | Melun | Médecine Intensive | Centre Hospitalier de Melun | JOCHMANS Sebastien | MONCHI M | |
France | Montpellier | Réanimation Chirurgicale | Centre Hospitalier de Montpellier | JABER Samir | DE JONG Audrey | |
France | Montpellier | Réanimation Médicale | Centre Hospitalier de Montpellier | MOULAIRE Valerie | ||
France | Moulins | Réanimation Polyvalente | Centre Hospitalier Moulins Yzeure | CAPRON Matthieu | JARRIGE L | |
France | Mulhouse | Réanimation Médicale | Centre Hospitalier de Mulhouse | BARBERET Guillaume | IOIDEYIN Autoine | |
France | Nantes | Réanimation chirurgicale polyvalente HGRL | de Nantes | LAKHAL Karim | ROZEC B | |
France | Nice | Réanimation Médicale | Centre Hospitalier Universitaire l’ARCHET 1 | DELLAMONICA Jean | ROBERT Alexandre | BERNARDIN G |
France | Nice | Réanimation Médico-Chirurgicale | Centre Hospitalier Universitaire l’ARCHET 2 | DANIN Pierre-Eric | RAUCOULES M | |
France | Orleans | Réanimation Médicale | Centre Hospitalier Régional d’Orleans | RUNGE Isabelle | ||
France | Paris | Réanimation Chirurgicale Polyvalente | Hôpital Beaujon (Clichy) APHP | FOUCRIER Arnaud | ||
France | Paris | Réanimation Chirurgicale | Hôpital Bicêtre APHP | HAMADA Sophie | ||
France | Paris | Réanimation Chirurgicale Digestive | Hôpital Cochin APHP | TESNIERE Antoine | FROMENTIN Mélanie | SAMAMA CM |
France | Paris | Réanimation Médicale | Hôpital Cochin APHP | MIRA Jean-Paul | ||
France | Paris | Réanimation | Hôpital George Pompidou APHP | DIEHL Jean-Luc | ||
France | Créteil | Réanimation Médicale—Créteil | Hôpital Henri-Mondor APHP | MEKONTSO DESSAP Armand | ||
France | Paris | Réanimation Chirurgicale | Hôpital Pitié-Salpêtrière APHP | ARBELOT Charlotte | ||
France | Paris | Réanimation médicale Montyon | Hôpital Pitié-Salpêtrière APHP | DEMOULE Alexandre | ROCHE Anne | SIMILOWSKI T |
France | Colombes | Réanimation Médico Chirurgicale—Louis mourier | Hopitaux Universitaires Paris Nord Val de Seine APHP | RICARD Jean-Damien | GAUDRY Stéphane | DREYFUSS D |
France | Saint Denis | Réanimation Médicale—Saint Denis | Centre Hospitalier Saint Denis | de MONTMOLIN Etienne | Da SILVA Daniel | VERDIERE B |
France | Paris | Réanimation Médicale—Saint Louis | Hôpital Saint Louis APHP | ARDISSON Fanny | LEMIALE Virginie | AZOULAY Elie |
France | Paris | Réanimation Médicale—St joseph | Hôpital Paris Saint Joseph | BRUEL Cédric | TIERCELET Kelly | |
France | Paris | Réanimation Médico-Chirurgicale | Hôpital Tenon APHP | FARTOUKH Muriel | VOIRIOT Guillaume | |
France | Clamart | Centre de Traitement des Brûlés | Percy Military Teaching Hospital | HOFFMANN Clement | LECLERC T | |
France | Poitiers | Réanimation Médicale | Centre Hospitalier Universitaire Poitiers | THILLE Arnaud | ROBERT Réné | |
France | Roanne | Réanimation Médicale | Centre Hospitalier de Roanne | BEURET Pascal | ||
France | Rouen | Réanimation Médicale | Centre Hospitalier Universitaire de Rouen | BEDUNEAU Gaëtan | BEUZELIN Marion | TAMION F |
France | Saint-Priest en Jarez | Réanimation Polyvalente | Centre Hospitalier Universitaire de Saint Etienne | MOREL Jérôme | TREMBLAY Aymeric | MOLLIEX S |
France | Toulon | Réanimation Polyvalente | Centre Hospitalier de Toulon | AMAL Jean-Michel | ||
France | Toulon | Réanimation HIA | HIA SAINTE-ANNE | MEAUDRE Eric | GOUTORBE Philippe | |
France | Tours | Anesthésie Réanimation | Centre Hospitalier Régional Universitaire de Tours | LAFFON Marc | ||
France | Le Chesnay (Versailles) | Réanimation Médico-Chirurgicale | Centre Hospitalier de Versailles | GROS Antoine | ||
France | Compiegne | Réanimation | Centre Hospitalier de Compiegne Noyon | NICA Alexandru | BARJON Genevieve | |
France | Poitiers | Réanimation Chirurgicale | Centre Hospitalier Universitaire Poitiers | DAHYOT-FIZELIER Claire | IMZI Nadia | |
France | Mulhouse | Réanimation Chirurgicale | Groupe hospitalier de la région Mulhouse et sud Alsace | GALLY Josette | REAL | |
France | Cherbourg en Cotentin | Réanimation Polyvalente | Centre Hospitalier Public du Cotentin | SAUNEUF Bertrand | SOULOY Xavier | |
The Netherlands | Amsterdam | Department of Intensive Care | University Hospital VU medical centre | GIRBES Armand | TUINMAN Pieter Roel | |
The Netherlands | Amsterdam | Intensive Care Unit | Academic medical Center | SCHULTZ Marcus | WINTERS Tineke | |
The Netherlands | Roermond | Intensive Care Unit | Laurentius Ziekenhuis Roermond | MIJZEN Lisa | ROEKAERTS | |
The Netherlands | Enschede | Intensive Care Centrum | Medisch Spectrum Twente | VERMEIJDEN Wytze | BEISHUIZEN Albertus | TROF R. |
The Netherlands | Nijmegen | Intensive Care afdeling | Canisius Wilhelmina Ziekenhuis | CORSTEN Stijn | ||
The Netherlands | Utrecht | Department of Intensive Care Medicine | University Medical Center Utrecht | KESECIOGLU Jozef | ||
The Netherlands | Groningen | Critical Care | University Medical Center Groningen | MEERTENS John | DIEPERINK Wim | |
The Netherlands | Nijmegen | Intensive Care Unit | Radboudumc | PICKERS Peter | ROOVERS Noortje | |
Portugal | Porto | Cuidados intensivos | Hospital Santo António | MAIA Paulo | DUQUE Melanie | FERNANDO RUA |
Portugal | Cascais | Intensive Care | Hospital de Cascais | PEREIRA DE FIGUEIRED António Manuel | RAMOS Armindo | |
Portugal | Lisboa | Unidade de Cuidados Intensivos Respiratórios (UCIR)—Serviço de Pneumologia | Hospital de Santa Maria—Centro Hospitalar de Lisboa Norte | FRAGOSO Elsa | AZEVEDO Pilar | AZEVEDO P |
Portugal | Lisboa | Serviço de Medicina Intensiva—UCIP | Hospital Santa Maria | GOUVEIA Joao | Zélia Costa e Silva | |
Portugal | Funchal | Serviço de Medicina Intensiva | Hospital Central do Funchal | SILVA Goncalo | CHAVES Susana | NOBREGA JJ |
Portugal | Porto | Unidade de Cuidados Intensivos Polivalente da Urgência (UCIPU), Unidade de Cuidados Intensivos Polivalente Geral (UCIPG) | Hospital São João | LOPES Luís | NUNO Iriucipe | |
Portugal | Lisboa | Hospital de São Francisco Xavier | VALERIO Bernardino | |||
Portugal | Amadora | Hospital Amadora-Sintra | ARAUJO Ana Carolina | Dr. Paulo Telles de Freitas | ||
Portugal | Lisboa | IPO Lisboa | BOUW Maria Jose | |||
Portugal | Faro | UCIP Unidade de Cuidados Intensivos Polivalente | Centro Hospitalar do Algarve | MELAO Maria | GRANJA C | |
Portugal | Gaia | CHVNG Centro Hospitalar Vila Nova de Gaia | MARCAL Paulo | |||
Portugal | Almada | Hospital Almada | Hospital Almada | FERNANDES Antero | ||
Portugal | Vila Franca Xira | Hospital Vila Franca Xira | Hospital Vila Franca Xira | JOAO Gonçalves Pereira | ||
Portugal | Ponta Delgada—Açores Islands | Hospital Ponta Delgada | Hospital Ponta Delgada | FARIA MAIA Dionísio | ||
Italy | Ferrara | Intensive care unit | Arcispedale Sant’Anna | SPADARO Savino | VOLTA Carlo Alberto | |
Italy | Monza | General ICU | Hospital San Gerardo | BELLANI Giacomo | CITERIO G | |
Italy | Milano | Terapia Intensiva Postoperatoria | Fondazione IRCCS Ospedale Maggiore Policlinico | MAURI Tommaso | ALBAN Laura | PESENTI A |
Italy | Milano | U.O.C. Anestesia e Rianimazione | Ospedale San Paolo—Polo Universitario | MISTRALETTI Giovanni | FORMENTI Paolo | TOMMASINO C |
Italy | Milano | Terapia Intensiva Generale 1 | ASST Grande Ospedale Metropolitano Niguarda | TARDINI Francesca | FUMAGALLI R | |
Italy | Milano | Terapia Intensiva | Ospedale Luigi Sacco | COLOMBO Riccardo | FOSSALI Tommaso | CATENA E |
Italy | Chiari | Unità di terapia intensiva | ASST FRANCIACORTA Chiari Hospital | TODESCHINI Manuel | GNESIN Paolo | |
Italy | Palermo | Terapia Intensiva Polivalente 2 | ARNAS Ospedale Civico Di Cristina BENFRATELLI | CRACCHIOLO Andrea Neville | PALMA Daniela | TETAMO R |
Italy | Rozzano | Terapia Intensiva Generale | Humanitas Research Hospital | ALBIERO Daniela | COSTANTINI Elena | RAIMONDI F |
Italy | Lecco | Rianimazione Generale | A. Manzoni Hospital | COPPADORO Andrea | VASCOTTO Ettore | LUSENTI F |
Germany | Kiel | Anesthesiology and Intensive Care Medicine | Universitätsklinik Schleswig-Holstein, Campus Kiel | BECHER Tobias | SCHÄDLER Dirk | WEILER N |
Germany | Cologne | ARDS and ECMO centre Cologne | ARDS and ECMO centre Cologne-Merheim/University Witten/Herdecke | KARAGIANNIDIS Christian | ||
Sweden | Stockholm | Karolinska Universitetssjukhuset, Solna | Karolinska University Hospital Solna | PETERSSON Johan | KONRAD D | |
Sweden | Uppsala | Central intensive care | Akademiska sjukhuset | KAWATI Rafael | WESSBERGH Joanna | VALTYSSON J |
Sweden | Kalmar | ICU | Länssjukhuset i Kalmar | ROCKSTROH Matthias | BORGSTROM Sten | |
Sweden | Umeå | Centrum för intensiv och postoperativ vård | Umeå University Hospital | LARSSON Niklas | THUNBERG J | |
UK | Poole | Critical Care Unit | Poole Hospital | CAMSOOKSAI Julie | BRIGGS | |
UK | London | Critical care complex | The North Middlesex University Hospital Trust | KOVARI Ferenc | CUESTA J | |
UK | London | Barts Heart Centre | Barts Heart Centre- St. Bartholomew’s Hospital | ANWAR Sibs | O’ BRIEN B | |
UK | Carlisle | Intensive Care | Cumberland Infirmary | BARBERIS Luigi | STURMAN J | |
Greece | Athens | Intensive Care Unit | Hippokrateion General Hospital of Athens | MAINAS Efstratios | KARATZAS S | |
Czech Republic | Prague | Intensive Care Unit | IKEM Institute of Clinical and Experimental Medicine | PIZA Petr | ||
Belgium | Gosselies | Intensive Care Unit | Clinique Notre-Dame de Grâce | SOTTIAUX Thierry | ADAM JF | |
Poland | Opole | Department of Anesthesiology and Critical Care | PS ZOZ Wojewodzkie Centrum Medyczne w Opolu | GAWDA Ryszard | GAWOR M | |
Canada | Moncton | Respirology Critical Care | The Moncton Hospital | ALQDAH Maen | ALQDAH M and COHEN D | |
Canada | Toronto | Intensive Care Unit | St. Michael’s Hospital | BROCHARD Laurent | BAKER A | |
Mexico | Mexico City | Department of Critical Care Unit | Instituto Nacional de Cancerología | ÑAMENDYS-SILVA Silvio Antonio | GARCIA-GUILLEN Francisco Javier | |
Ecuador | Quito | Unidad de Terapia Intensiva | Hospital de Especialidades Eugenio Espejo | MOROCHO TUTILLO Diego Rolando | JIBAJA VEGA Manuel | JIBAJA VEGA MANUEL |
Argentina | Mendoza | Terapia intensiva | Hospital Luis Carlos Lagomaggiore | ZAKALIK Graciela | PAGELLA Gonzalo | MARENGO J |
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
The complete list of investigators and centers can be found in the Acknowledgments and in ESM file 10.
Electronic supplementary material
Below is the link to the electronic supplementary material.
134_2017_4996_MOESM1_ESM.pdf
Supplementary material 1 (PDF 195 kb) Electronic case record form used in the APRONET study. Fig. 2 Prevalence of prone position use in each study period (upper panel) and across ARDS categories over all study periods (lower panel)
Rights and permissions
About this article

Cite this article
Guérin, C., Beuret, P., Constantin, J.M. et al. A prospective international observational prevalence study on prone positioning of ARDS patients: the APRONET (ARDS Prone Position Network) study. Intensive Care Med 44, 22–37 (2018). https://doi.org/10.1007/s00134-017-4996-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-017-4996-5