
Abstract
Purpose
Ultrasound measurements of diaphragm thickness (T di) and thickening (TFdi) may be useful to monitor diaphragm activity and detect diaphragm atrophy in mechanically ventilated patients. We aimed to establish the reproducibility of measurements in ventilated patients and determine whether passive inflation by the ventilator might cause thickening apart from inspiratory effort.
Methods
Five observers measured T di and TFdi in 96 mechanically ventilated patients. The probe site was marked in 66 of the 96 patients. TFdi was measured at peak and end-inspiration (airway occluded and diaphragm relaxed) in nine healthy volunteers inhaling to varying lung volumes. The association with diaphragm electrical activity was quantified.
Results
Right hemidiaphragm thickness was obtained on 95 % of attempts; left hemidiaphragm measurements could not be obtained consistently. Right hemidiaphragm thickness measurements were highly reproducible (mean ± SD 2.4 ± 0.8 mm, repeatability coefficient 0.2 mm, reproducibility coefficient 0.4 mm), particularly after marking the location of the probe. TFdi measurements were only moderately reproducible (median 11 %, IQR 3–17 %, repeatability coefficient 17 %, reproducibility coefficient 16 %). TFdi and diaphragm electrical activity were positively correlated, r 2 = 0.32, p < 0.01). At inspiratory volumes below 50 % of inspiratory capacity, passive inflation did not cause diaphragm thickening. TFdi was considerably lower in patients on either partially assisted or controlled ventilation compared to healthy subjects (median 11 vs. 35 %, p < 0.001).
Conclusions
Ultrasound measurements of right hemidiaphragm thickness are feasible and highly reproducible in ventilated patients. At clinically relevant inspiratory volumes, diaphragm thickening reflects muscular contraction and not passive inflation. This technique can be reliably employed to monitor diaphragm thickness, activity, and function during mechanical ventilation.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Respiratory muscle dysfunction is now recognized as an important complication of critical illness [1, 2]. In patients receiving invasive mechanical ventilation for acute respiratory failure, diaphragm dysfunction has been linked to increased mortality [3] and difficulty weaning from mechanical ventilation [4, 5]. Mechanically ventilated patients may develop diaphragm dysfunction from a range of factors [1, 6] including disuse atrophy from mechanical ventilation [7–10]. Assessing and monitoring diaphragm contractile activity, strength and structural dimensions during mechanical ventilation is therefore an increasingly important clinical and research priority.
Bedside assessment of diaphragm activity and function is challenging during mechanical ventilation. Monitoring diaphragm activity ordinarily requires measurement of esophageal and gastric pressures or crural electromyographic (EMG) signals (as in Neurally Adjusted Ventilatory Assist––NAVA) [11]. Diaphragm function is traditionally measured as the transdiaphragmatic pressure generated in response to volitional stimuli or from magnetic twitch stimulation of the phrenic nerve [11–14]. These techniques require nasogastric catheterization, considerable technical and physiological expertise, and a degree of patient cooperation often not possible in the critically ill [12]. Moreover, these measurements are not designed to detect changes in diaphragmatic structure (such as atrophy) that may be triggered by mechanical ventilation [9, 10, 15, 16].
Transthoracic diaphragm ultrasound imaging represents an important potential advance in diaphragm monitoring during mechanical ventilation [17]. This technique provides a non-invasive, feasible measure of diaphragm thickness and inspiratory thickening previously validated in healthy subjects [18–23]. Increases in diaphragm thickness with inspiration—quantifiable by ultrasound—are correlated with inspiratory effort [21, 24]. Accordingly, transthoracic ultrasound represents a potential modality for evaluating diaphragm activity, function and dimensions during mechanical ventilation.
The feasibility and precision of diaphragm thickness measurements have not yet been established in mechanically ventilated patients. Moreover, it is unknown whether inspiratory thickening of the diaphragm primarily reflects diaphragm contractile activity or expansion of the chest wall per se (which could critically confound the validity of diaphragm inspiratory thickening as a measure of inspiratory effort as these two factors are uncoupled during mechanical ventilation). Accordingly, we aimed to test the feasibility and reproducibility of these measurements in ventilated subjects and to quantify for the first time the independent contributions of muscle contraction and thoracic volume expansion to inspiratory diaphragm thickening on ultrasound. Some of the findings reported in this study have been previously presented in abstract form [25, 26].
Methods
This study consisted of two parts: (1) a clinical study to evaluate the feasibility and reproducibility of diaphragm thickness measurements in mechanically ventilated patients (conducted in the two medical-surgical intensive care units at University Health Network, Toronto, ON, Canada) and (2) a physiological study to evaluate the validity of measuring diaphragm thickening to assess inspiratory effort (conducted in the outpatient Pulmonary Research Laboratory of Edward Hines Jr. VAH, Hines, IL, USA). All subjects (or, in the case of mechanically ventilated patients, their substitute decision makers) provided written informed consent. The study was approved by the Institutional Review Boards at both participating institutions and has therefore been performed in accordance with the ethical standards laid down in the 2008 Declaration of Helsinki.
Experimental subjects
In the reproducibility study, we enrolled adult critically ill patients receiving invasive mechanical ventilation. Patients were excluded from the study if they had a previously diagnosed neuromuscular disorder, had active hemodynamic or respiratory instability at the time of assessment, or exhibited behavioural agitation. In the validation study, we enrolled healthy adult subjects without prior history of cardiopulmonary or neuromuscular disease.
Experimental measurements
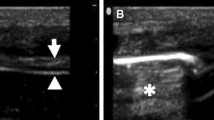
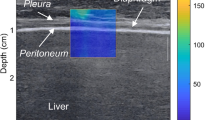
Diaphragm thickness was measured by ultrasound as previously described [17, 21, 24]. Briefly, a 13-MHz linear array transducer (HFL-38xe; FUJIFILM Sonosite, Bothell, WA, USA) was placed in the ninth or tenth intercostal space near the midaxillary line and angled perpendicular to the chest wall [17]. In this location, the diaphragm is identified as a three-layered structure just superficial to the liver, consisting of a relatively non-echogenic muscular layer bounded by the echogenic membranes of the diaphragmatic pleura and peritoneum [23] (Figure E1). Diaphragmatic thickness was measured at end-expiration (T di,ee) and peak inspiration (T di,pi; i.e. peak thickness value during inspiration) as the distance between the diaphragmatic pleura and the peritoneum using M-mode (see Figure E1 in Online Supplement) [27, 28]. Measurements of T di,ee and T di,pi were always made on two breaths visualized in a single M-mode image. Diaphragm thickening during inspiration (ΔT di) was taken as the difference between T di,pi and T di,ee. Diaphragm thickening fraction (TFdi) was defined as the percentage change in diaphragm thickness during inspiration (computed from the quotient of ΔT di and T di,ee).
In the validation substudy, subjects underwent nasogastric catheterization for esophageal and gastric manometry and diaphragmatic electromyography (see online supplement for details) [29]. Inspiratory volumes were measured using a Wright spirometer (experimental setup shown in Figure E2). T di,ee and T di,pi were measured as described above.
Experimental protocol
In the reproducibility study, three observers (in random order) measured T di,ee and T di,pi in mechanically ventilated patients in a single study session. Observers were blinded to each other’s findings. The three observers included an intensivist experienced in the performance of diaphragm ultrasound (E.G.), an intensivist with experience in general critical care ultrasound but no prior experience with diaphragm ultrasound (M.D.) and a research coordinator with no prior experience in diaphragm ultrasound (P.F.). Observers were required to demonstrate competence with the technique on six patients before commencing the study. To assess intra-observer repeatability, one of the observers (E.G.) repeated the measurement 5 min after the initial measurement. During the study, it proved difficult to consistently visualize the left hemidiaphragm, so measurements of left hemidiaphragm thickness were discontinued.
Upon reviewing the preliminary results of the reproducibility study, it was felt that some excess measurement variability may arise from inadequate observer training and from variation in the precise location of the ultrasound probe as the thickness of the diaphragm is heterogeneous across its surface [30]. Therefore, we repeated the reproducibility study with the following modifications: (1) observers had to demonstrate competency on 15 ultrasound examinations before beginning study data collection and (2) the probe placement site was marked by the first observer. Two other observers (A.M. and D.B.––both previously untrained research assistants) were then trained after these modifications. One of the observers (A.M.) obtained two repeated measurements in a larger convenience sample of patients to assess measurement repeatability; in a subset of these patients, two observers (A.M. and D.B.) independently obtained two repeated measurements to assess measurement reproducibility.
In the validation study (healthy subjects), right hemidiaphragm thickness was continuously recorded using M-mode ultrasound while each subject inhaled from functional residual capacity to a series of target inspiratory volumes: 25, 50, 75 and 100 % of inspiratory capacity (IC). Upon reaching the target volume, subjects were instructed to close the glottis (so as to maintain the end-inspiratory lung volume) and relax the respiratory muscles (so as to remove the effect of diaphragmatic contraction on diaphragm thickness). T di was recorded at end-expiration, peak inspiration (maximal effort condition determined from peak thickness), and end-inspiration (relaxed condition) (Figure E3). At least two such maneuvers were conducted at each target inspiratory volume. End-inspiratory (relaxed condition) EMG signals were examined to ensure relaxation of the diaphragm.
Statistical analysis
Descriptive statistics were expressed as means and standard deviations where appropriate. The relationships between physiological variables and TFdi were evaluated using linear mixed effects models to account for repeated measures.
Interobserver repeatability and intra-observer reproducibility of ultrasound measurements were assessed by computing repeatability and reproducibility coefficients [31–33] from the variance components of random effects models of repeated measurements of diaphragm thickness [31]. These coefficients indicate the 95th percentile for the range of variation in repeated measurements either within observers (repeatability) or between observers (reproducibility).
The sample size of the initial reproducibility study was calculated to achieve 95 % confidence intervals of ±0.1 mm for the reproducibility limits assuming a standard deviation of repeated measurements between observers of 0.2 mm, which yielded a required sample of 30 patients [33]. The sample size of the second reproducibility study was calculated assuming a standard deviation of repeated measurements between observers of 0.1 mm (based on the observed standard deviation within observers in the initial study), which yielded a required sample size of 15 patients to achieve confidence intervals of ±0.1 mm for the reproducibility limits. In order to enhance clinical generalizability of the repeatability estimate and avoid spectrum bias, we enrolled a convenience sample of an additional 51 subjects to assess measurement repeatability. The sample size of the validation study was initially estimated based on physiological judgment regarding the number of subjects required for a generalizable inference.
Results
Feasibility and reproducibility of diaphragm thickness measurements in ventilated subjects
Thirty mechanically ventilated patients were enrolled in the initial reproducibility study. After modifying the measurement protocol (see “Methods”), we enrolled an additional 66 ventilated patients; of these, 51 underwent ultrasound examination by a single observer and 15 underwent separate ultrasound examinations by two independent observers (Table E1). Clinical characteristics of the ventilated patients are shown in Table 1.
Right hemidiaphragm T di,ee and T di,pi measurements were obtained on 96 and 95 % of a total of 542 attempts in ventilated patients, respectively. Right hemidiaphragm measurements were generally only missing for one observer and there were no missing measurements in the second reproducibility study. Left hemidiaphragm T di,ee and T di,pi measurements were obtained on 85 and 79 % of a total of 104 attempts in ventilated patients, respectively.
The distributions of T di,ee, T di,pi, ΔT di and TFdi and the coefficients of repeatability and reproducibility for these measurements are reported in Table 2. There was no difference between the right hemidiaphragm and the left hemidiaphragm for both T di,ee (mean difference 0.0 mm, 95 % CI −0.2–0.2 mm) and T di,pi (mean difference 0.0 mm, 95 % CI −0.2–0.2 mm). Reproducibility of right hemidiaphragm measurements improved considerably when the site of probe placement was routinely marked. Using this technique, repeatability and reproducibility of T di,ee and T di,pi measurements were excellent given the observed distributions of those measurements. However, the repeatability and reproducibility of ΔT di and TFdi were only moderately acceptable given their observed distributions. T di,ee and TFdi measurement variability did not vary with body mass index or duration of mechanical ventilation (Figure E4) and T di,ee was not significantly correlated with height, weight or body mass index (Figure E5).
Validity of inspiratory diaphragm thickening fraction to monitor inspiratory activity
Compared to the healthy subjects, TFdi was considerably lower in ventilated patients and nearly absent in patients subjected to neuromuscular blockade (in the reproducibility study cohort) (Fig. 1; p < 0.0001 for difference across groups). TFdi was not significantly different between patients in controlled and partially assisted modes of ventilation (mean difference 3, 95 % CI −2–9 %), and patients in both groups exhibited a wide range of TFdi values.

Inspiratory thickening fraction of the right hemidiaphragm in healthy subjects at rest and ventilated subjects under varying conditions. Inspiratory thickening is observed at very low levels in patients subjected to neuromuscular blockade, suggesting that thickening mainly reflects diaphragm contractile activation rather than increases in thoracic volume per se
Nine healthy subjects participated in the validation study. Transdiaphragmatic pressure and diaphragm electrical activity measurements were obtained in five of the participants. In the series of inspiratory maneuvers to varying inspiratory volumes, TFdi was correlated with inspiratory volume (Figure E5; r 2 = 0.32, p < 0.0001), and with both diaphragm electrical activity (EAdi) and transdiaphragmatic pressure (P di) (Fig. 2; r 2 = 0.32 and 0.28, respectively, p < 0.01).

Diaphragm thickening fraction is correlated with diaphragm electrical activity and transdiaphragmatic pressure during inspiratory maneuvers. EA di diaphragm electrical activity, P di transdiaphragmatic pressure
When subjects inhaled from functional residual capacity (FRC) to volumes below 50 % of inspiratory capacity, inspiratory increases in diaphragm thickness were almost entirely related to muscular contraction as end-inspiratory diaphragm thickness (passive condition) was very similar to end-expiratory thickness (Fig. 3). By contrast, when subjects inhaled from FRC to inspiratory volumes above 50 % of inspiratory capacity, inspiratory increases in diaphragm thickness resulted both from muscle contraction and increased thoracic volume as end-inspiratory thickness (passive condition) was considerably higher than end-expiratory thickness (Fig. 3). The contribution of increased thoracic volume to diaphragm thickening fraction was not statistically significant when inspiratory volumes were approximately less than 1,500 ml (Figure E6).

The relative contributions of inspiratory effort vs. chest wall expansion to inspiratory diaphragm thickening fraction depend on the inspiratory volume. At lower inspiratory volumes (i.e. below 50 % IC), inspiratory changes in diaphragm thickness are almost entirely attributable to inspiratory effort (i.e. diaphragm thickness returns nearly to end-expiratory levels during the end-inspiratory hold––Hold). At higher inspiratory volumes, inspiratory changes in thickness are due to both inspiratory effort and increased thoracic volume (diaphragm thickness observed during the end-inspiratory hold remains considerably higher than end-expiratory levels). IC inspiratory capacity
Discussion
This is the first report on the feasibility and reproducibility of sonographic measurements of diaphragm thickness and inspiratory thickening in a sizable cohort of mechanically ventilated patients. Our findings suggest that sonographic measurements of diaphragm thickness provide a useful non-invasive tool to assess and monitor for diaphragm atrophy and inactivity during mechanical ventilation.
A number of recent studies have employed ultrasound to measure diaphragm thickness and inspiratory thickening in ventilated patients. Grosu and colleagues [34] found evidence of a progressive decrease in diaphragm thickness in a small series of ventilated patients. TFdi has been employed to estimate of inspiratory effort during partially assisted ventilation [24] and to predict the probability of successful liberation from ventilation [35, 36]. While Vivier et al. [24] reported intra-analyzer reproducibility in a small number of ventilated subjects prior to the present study, the precision of these measurements was not well established in a broad population of critically patients, limiting the inferences that may be drawn using this technique.
Our study demonstrates that measurement of right hemidiaphragm thickness is feasible and highly reproducible in a representative cohort of mechanically ventilated patients. By contrast, we found it challenging to consistently visualize and measure the thickness of the left hemidiaphragm. In the 13 patients with bilateral measurements, right and left hemidiaphragm T di,ee and TFdi were similar. Left hemidiaphragm measurements may therefore be unnecessary unless there is some specific clinical reason to suspect unilateral muscle injury or dysfunction (i.e. phrenic nerve injury).
Anatomical studies have shown that the thickness of the diaphragm is heterogeneous across its surface [30]; accordingly, placement of the probe must be standardized to minimize to measurement variability. We initially sought to standardize probe placement using anatomical landmarks; however, we found that marking the site significantly improves measurement reproducibility, particularly between observers. This limits comparisons of diaphragm thickness between patients, but changes in diaphragm thickness as small as 0.2 mm over time can be reliably detected within patients by this technique.
The reproducibility of the inspiratory thickening fraction (TFdi) was less satisfactory: measurements may vary between or within observers by as much as 16–17 %, obscuring important differences in inspiratory muscle activity (given that, during resting, tidal breathing diaphragm thickening fraction in healthy subjects is 30–40 %). In fact, the repeatability coefficient for absolute value of the change in diaphragm thickness during inspiration (ΔT di) was very similar to the repeatability coefficient for end-expiratory diaphragm thickness (0.3 vs. 0.2 mm). Because TFdi incorporates the measurement error of both ΔT di and T di,ee it is unlikely that further improvements in the reproducibility of TFdi can be obtained. Of interest, our repeatability and reproducibility coefficients correspond closely with those previously reported in healthy volunteers [20] and in ventilated subjects [24].
While inspiratory volume and muscle pressure generation are entirely collinear in spontaneously breathing subjects, they are variably dissociated during mechanical ventilation. If passive inflation of the chest could cause apparent tidal diaphragm thickening, TFdi would not be a valid measure of diaphragm contractile activity in these patients. Based on our findings, we conclude that, at relatively low inspiratory volumes (<50 % of inspiratory capacity), thickening of the diaphragm during inspiration arises from muscular contraction rather than increasing thoracic volume per se (Fig. 3). Significant thickening of the diaphragm under passive conditions occurred only at high inspiratory volumes (>50 % of inspiratory capacity). Supporting this conclusion, we found that subjects under neuromuscular blockade exhibited only minimal levels of diaphragm thickening.
The degree of diaphragm thickening for a given level of inspiratory effort varied considerably between subjects (Fig. 3). Accordingly, a given inspiratory TFdi value does not imply the same transdiaphragmatic pressure swing across different subjects, limiting the utility of this measurement for precise interpatient comparison. TFdi is therefore best suited to qualitative comparisons of inspiratory muscle activity between subjects and to quantitative comparisons of changes in inspiratory muscle activity within subjects.
Our study is subject to a number of limitations. First, it is not entirely clear whether improvements in measurement reproducibility observed in the second study phase are attributable to marking the probe location or more rigorous training. We reason that the first explanation is most likely because, after marking the site, the between-observer reproducibility improved considerably more than the within-observer reproducibility. Second, the need to mark the location of the probe to ensure adequate measurement reproducibility greatly limits the utility of this technique for comparisons between subjects. Third, we assessed the validity of TFdi measurements in healthy subjects but did not measure diaphragm electrical activity in mechanically ventilated patients. However, our conclusion that diaphragm thickening fraction is a valid marker of inspiratory effort is corroborated by the low levels of thickening observed in ventilated patients subjected to neuromuscular blockade, and by a recent description of the relationship between the diaphragm thickening fraction and ther inspiratory effort during mechanical ventilation [24].
In summary, we conclude that ultrasound of the diaphragm can reproducibly measure variation in right hemidiaphragm thickness within mechanically ventilated patients over time. We also conclude that inspiratory thickening of the diaphragm reflects the degree of contractile activation of the muscle during partially assisted mechanical ventilatory support. This technique may therefore be employed in ventilated patients to reliably detect diaphragmatic atrophy over time and to assess diaphragm contractile activity. Future research is required to confirm the utility of this technique to assess muscle function in response to a maximal volitional inspiratory effort and to diagnose patient–ventilator dyssynchrony.
References
Tobin MJ, Laghi F, Jubran A (2010) Narrative review: ventilator-induced respiratory muscle weakness. Ann Intern Med 153:240–245. doi:10.7326/0003-4819-153-4-201008170-00006
De Jonghe B, Bastuji-Garin S, Durand M-C et al (2007) Respiratory weakness is associated with limb weakness and delayed weaning in critical illness. Crit Care Med 35:2007–2015. doi:10.1097/01.ccm.0000281450.01881.d8
Demoule A, Jung B, Prodanovic H et al (2013) Diaphragm dysfunction on admission to the intensive care unit. Prevalence, risk factors, and prognostic impact-a prospective study. Am J Respir Crit Care Med 188:213–219. doi:10.1164/rccm.201209-1668OC
Meade MO, Cook DJ, Guyatt GH et al (2008) Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA 299:637–645. doi:10.1001/jama.299.6.637
Kim WY, Suh HJ, Hong S-B et al (2011) Diaphragm dysfunction assessed by ultrasonography: influence on weaning from mechanical ventilation. Crit Care Med. doi:10.1097/CCM.0b013e3182266408
Laghi F, Tobin MJ (2003) Disorders of the respiratory muscles. Am J Respir Crit Care Med 168:10–48. doi:10.1164/rccm.2206020
Powers SK, Shanely RA, Coombes JS et al (2002) Mechanical ventilation results in progressive contractile dysfunction in the diaphragm. J Appl Physiol 92:1851–1858. doi:10.1152/japplphysiol.00881.2001
Sassoon CSH, Caiozzo VJ, Manka A, Sieck GC (2002) Altered diaphragm contractile properties with controlled mechanical ventilation. J Appl Physiol 92:2585–2595. doi:10.1152/japplphysiol.01213.2001
Levine S, Nguyen T, Taylor N et al (2008) Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med 358:1327–1335. doi:10.1056/NEJMoa070447
Jaber S, Petrof BJ, Jung B et al (2011) Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am J Respir Crit Care Med 183:364–371. doi:10.1164/rccm.201004-0670OC
Doorduin J, van Hees HW, van der Hoeven JG, Heunks LM (2013) Monitoring of the respiratory muscles in the critically ill. Am J Respir Crit Care Med 187:20–27. doi:10.1164/rccm.201206-1117CP
Cattapan SE, Laghi F, Tobin MJ (2003) Can diaphragmatic contractility be assessed by airway twitch pressure in mechanically ventilated patients? Thorax 58:58–62
Man WD-C, Moxham J, Polkey MI (2004) Magnetic stimulation for the measurement of respiratory and skeletal muscle function. Eur Respir J 24:846–860. doi:10.1183/09031936.04.00029004
ATS/ERS statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166:518–624. doi: 10.1164/rccm.166.4.518
Anzueto A, Peters JI, Tobin MJ et al (1997) Effects of prolonged controlled mechanical ventilation on diaphragmatic function in healthy adult baboons. Crit Care Med 25:1187–1190
Hooijman PE, Beishuizen A, de Waard MC et al (2014) Diaphragm fiber strength is reduced in critically ill patients and restored by a troponin activator. Am J Respir Crit Care Med 189:863–865. doi:10.1164/rccm.201312-2260LE
Matamis D, Soilemezi E, Tsagourias M et al (2013) Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med 39:801–810. doi:10.1007/s00134-013-2823-1
McCool FD, Tzelepis GE (2012) Dysfunction of the diaphragm. N Engl J Med 366:932–942. doi:10.1056/NEJMra1007236
McCool FD, Benditt JO, Conomos P et al (1997) Variability of diaphragm structure among healthy individuals. Am J Respir Crit Care Med 155:1323–1328. doi:10.1164/ajrccm.155.4.9105074
Baldwin CE, Paratz JD, Bersten AD (2011) Diaphragm and peripheral muscle thickness on ultrasound: intra-rater reliability and variability of a methodology using non-standard recumbent positions. Respirology 16:1136–1143. doi:10.1111/j.1440-1843.2011.02005.x
Cohn D, Benditt JO, Eveloff S, McCool FD (1997) Diaphragm thickening during inspiration. J Appl Physiol 83:291–296
Ueki J, de Bruin PF, Pride NB (1995) In vivo assessment of diaphragm contraction by ultrasound in normal subjects. Thorax 50:1157–1161
McCool FD, Conomos P, Benditt JO et al (1997) Maximal inspiratory pressures and dimensions of the diaphragm. Am J Respir Crit Care Med 155:1329–1334. doi:10.1164/ajrccm.155.4.9105075
Vivier E, Mekontso Dessap A, Dimassi S et al (2012) Diaphragm ultrasonography to estimate the work of breathing during non-invasive ventilation. Intensive Care Med 38:796–803. doi:10.1007/s00134-012-2547-7
Goligher EC, Detsky ME, Farias P, Murray A et al (2010) Validity and reproducibility of sonographic evaluation of diaphragm structure and activity in mechanically ventilated patients. Am J Respir Crit Care Med 181:A6346
Goligher EC, Laghi F, Morales D, Kavanagh BP et al (2013) A Window into the work of breathing: feasibility, precision, and physiological meaning of ultrasound measurements of diaphragm thickness. Crit Care 17(Suppl 2):P145
Gottesman E, McCool FD (1997) Ultrasound evaluation of the paralyzed diaphragm. Am J Respir Crit Care Med 155:1570–1574. doi:10.1164/ajrccm.155.5.9154859
de Bruin PF, Ueki J, Watson A, Pride NB (1997) Size and strength of the respiratory and quadriceps muscles in patients with chronic asthma. Eur Respir J 10:59–64
Laghi F, Shaikh HS, Morales D et al (2014) Diaphragmatic neuromechanical coupling and mechanisms of hypercapnia during inspiratory loading. Respir Physiol Neurobiol 198:32–41. doi:10.1016/j.resp.2014.03.004
Poole DC, Sexton WL, Farkas GA et al (1997) Diaphragm structure and function in health and disease. Med Sci Sports Exerc 29:738–754
Bland JM, Altman DG (1999) Measuring agreement in method comparison studies. Stat Methods Med Res 8:135–160
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310
McAlinden C, Khadka J, Pesudovs K (2011) Statistical methods for conducting agreement (comparison of clinical tests) and precision (repeatability or reproducibility) studies in optometry and ophthalmology. Ophthalmic Physiol Opt 31:330–338. doi:10.1111/j.1475-1313.2011.00851.x
Grosu HB, Lee YI, Lee J et al (2012) Diaphragm muscle thinning in patients who are mechanically ventilated. Chest 142:1455–1460. doi:10.1378/chest.11-1638
Ferrari G, De Filippi G, Elia F et al (2014) Diaphragm ultrasound as a new index of discontinuation from mechanical ventilation. Crit Ultrasound J 6:8. doi:10.1186/2036-7902-6-8
DiNino E, Gartman EJ, Sethi JM, McCool FD (2014) Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. Thorax 69:423–427. doi:10.1136/thoraxjnl-2013-204111
Acknowledgments
This study was funded by an operating grant from the Physician Services Incorporated Foundation (Toronto, Canada). E.G. is supported by a Post-Doctoral Fellowship from the Canadian Institutes of Health Research.
Conflicts of interest
On behalf of all the authors, the corresponding author states that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Take-home message:
Diaphragm ultrasound measurements are feasible and highly reproducible in mechanically ventilated patients and provide a valid measure of diaphragm activity during mechanical ventilation. Many ventilated patients exhibit much lower diaphragm activity levels compared to resting tidal breathing in healthy subjects.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Goligher, E.C., Laghi, F., Detsky, M.E. et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity. Intensive Care Med 41, 642–649 (2015). https://doi.org/10.1007/s00134-015-3687-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-015-3687-3