
Abstract
Objectives
Study objectives were to: (1) provide an estimate of the prevalence of repeat emergency department (ED) use for mental health reasons among individuals enrolled in intensive case management programs; and (2) to identify socio-demographic, diagnostic, and service need characteristics associated with repeat ED visits among this service population.
Methods
The study utilized administrative health data from community mental health organizations in Toronto, Canada on a sample of 2274 individuals enrolled in intensive case management programs. Patients with 2+ ED visits for mental health reasons within the prior 6 months were compared with individuals who had no ED visits or one visit on the basis of demographic, diagnostic and service need characteristics.
Results
Approximately 6 % of intensive case management clients had two or more ED visits over a 6-month period. Membership in the repeat ED user group was associated with younger age (OR 0.98), a mood disorder (OR 1.58), being in service less than 1 year (OR 1.94) and unmet needs related to psychotic symptoms (OR 2.19), substance use (OR 2.27), and safety to self/others (OR 3.42).
Conclusions
The repeat ED user group within case management may have distinct need profiles that require different treatment responses. Moreover, clinical needs rather than psychosocial needs have the greatest relationship with repeat psychiatric ED utilization. These unmet needs suggest areas for future interventions aimed at reducing the use of ED services for mental health reasons and improving care for patients who repeatedly present at the ED.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Overcrowding in emergency departments (EDs) has become an issue of increasing concern in many jurisdictions [1, 2], with repeated visits to the ED contributing to this phenomenon [1, 3, 4]. Many studies have shown that a relatively small group of patients account for a disproportionate number of ED visits [5–9]. Moreover, several studies have noted that mental health concerns are prevalent among these service users [10–15].
Interest in this subgroup of ED presenters with mental health concerns has spurred a burgeoning literature. This literature has identified predictors of repeated ED visits for mental health reasons including several socio-demographic, diagnostic and service use characteristics including: male gender [16, 17], younger age [3, 12, 17, 18], black or Hispanic race [12], unemployment [19, 20], low income [3, 17, 18, 21], homelessness [21, 22], living alone [23], lacking social support [22], schizophrenia [3, 12, 18, 20], psychosis [17, 20], personality disorder [19, 22, 25], substance abuse [12, 17, 20, 25], developmental delay [22], prior hospitalizations [21, 22, 24], history of detoxification [22], recent and increased use of outpatient treatment [21], current psychiatric treatment [25], and a history of incarceration [21].
In addition to socio-demographic, diagnostic and service use characteristics linked to use of the ED, a limited number of studies have examined patient needs related to ED use or the reason for referral to the ED. One study found anxiety, homicidal ideation, self-injurious behavior, intoxication and an absent or vacationing psychotherapist were associated with frequent ED use [25]. Another study found that the need for medication was predictive of frequent ED use [21]. Identification of patient service needs in additional to socio-demographic and diagnostic predictors may serve to inform the development of clinical and system-based interventions that engage frequent presenters in community-based care and alleviate pressure on ED services.
An often cited intervention to minimize ED use is intensive case management [3, 4, 12, 20]. This intervention has been found to reduce ED visits among the general population of frequent ED presenters [26]. However, the efficacy of this intervention for populations with psychiatric conditions has mixed results. Some studies found that intensive case management (ICM) for frequent ED presenters with psychiatric conditions was correlated with fewer hospital admissions or ED visits [20], while others found no reduction [27, 28], or found that intensive case management resulted in increased ED utilization [29]. Consequently, the complexity of needs of this service population warrants a more detailed enquiry.
While studies evaluating the effectiveness of ICM in reducing ED use among patients with psychiatric conditions have mixed results, they show that high ED use continues to be a challenge for some ICM clients, despite the service aim of keeping clients out of hospital. Increasing our understanding of the needs of repeat ED presenters receiving intensive case management may inform programming and interventions targeted at needs associated with repeated ED use.
The present study examines patients enrolled in intensive case management services with and without repeated visits to the ED for mental health concerns. The current literature on repeat use of ED services for mental health reasons has investigated repeat presenters among community samples but not yet among treatment samples such as those receiving case management services. However, the profile of repeat presenters enrolled in community-based mental health services, such as intensive case management, may differ from the broader population of repeat ED presenters with psychiatric conditions. Moreover, a multivariate approach examining socio-demographic, diagnostic, and clinical and psychosocial need factors associated with repeated ED use is lacking. The objectives of the present study are: (1) to estimate the prevalence of repeat ED use for mental health concerns among individuals enrolled in community-based intensive case management services, and (2) to identify socio-demographic, diagnostic, and clinical and psychosocial need characteristics associated with repeated ED use for mental health concerns among individuals receiving case management services.
Methods
Setting and sample
The study utilized anonymized routinely collected clinical health data from seven community mental health organizations that provide intensive case management in the Greater Toronto Area in Ontario, Canada. This urban center includes a population of just over 6 million and is Canada’s largest metropolitan area. The study examined a convenience sample of individuals aged 16 years or older enrolled within intensive case management programs on March 31, 2013. These programs are expected to offer a moderate level of support (1–2 contacts per week) with staff caseloads of 15–20 clients. Services include care coordination, crisis intervention, supportive counseling, as well as assistance in obtaining stable housing and income entitlements, linkage to medical care providers and ongoing assertive community outreach and monitoring. While provincial program standards exist which specify the structure and components of case management programs [30], implementation data are not routinely collected and compliance with these standards is not monitored. These programs operate within a public health care system in which such services as well inpatient and emergency care are provided without any charge to patients.
Design
To identify risk factors of repeat mental health ED use, we used a cross-sectional study, comparing case management service recipients with repeat ED visits for mental health reasons to those with a single visit or no visits to the ED. The study protocol was reviewed and approved by the Community Research Ethics Office of the Centre for Community-Based Research.
Variables
All study data were obtained from two common assessment tools routinely used by community mental health service providers in Ontario, Canada: the Community Mental Health Common Data Set (CDS-MH) [31] and the Ontario Common Assessment of Need (OCAN) [32]. Each of the participating organizations used the same client management database. De-identified patient data were exported from the administrative databases of participating organizations, collated into a master dataset and imported into SPSS Version 22 for analyses [33]. Study data were based on the most recently completed client needs assessment as of March 31, 2013.
Predictor variables were grouped into demographic, health condition, and need variables. Demographic variables included age, gender, and primary income source. Health condition variables included primary mental health diagnosis (psychotic disorder, mood disorder, other disorder) and the presence of a concurrent disorder (i.e., mental illness and substance abuse disorder). Case managers recorded mental health diagnoses based on available medical reports or, in the absence of such documentation, based on patient self-report, pending a diagnostic assessment by a physician or psychologist.
Need variables were obtained from the OCAN and were based on current needs identified at the time of assessment. Embedded within the OCAN is the Camberwell assessment of need, which is the most widely used measure of health and social needs for patients with severe mental illness [34]. The Camberwell assessment tool is used to inform and coordinate the care planning process of individual patients and serve as a measure in outcome assessments at the system level. The OCAN includes 24 need domains (e.g., accommodation, food, daytime activities, psychotic symptoms) [35]. There are two components of the measure—a client-completed version and a staff-completed version. The staff-completed version was used within the study as the number of cases with a staff-completed OCAN was nearly double that of cases with a client-completed OCAN. Needs are rated using four response options: 0 no problem, 1 met need due to help given, 2 unmet need, 9 not known. Need variables were dichotomized into unmet need and no unmet need (i.e., met/no need categories). Responses of “Not Known” were excluded. Some need variables were also combined into higher order variables to maximize subsample size for analyses (e.g., needs related to alcohol and drug use were combined into unmet alcohol or drug needs, safety to self and safety to others were combined into safety to self or others). The a priori selection of OCAN need items for inclusion within the analyses was informed by the existing empirical research. In total, nine OCAN need items were included and grouped into four conceptual domains: basic needs (accommodations, food, money/benefits), health needs (alcohol/drug use, psychological distress, psychotic symptoms, safety to self/others), functional needs (looking after the home/self-care), and social needs (company).
Self-reported data on the number of ED visits for mental health reasons in the prior 6 months were also obtained from the OCAN which included the following response options: none, one visit, two to five visits, and six or more visits. Subjects with two or more visits were categorized into the repeat user group and those with one or no ED visits were categorized into the single user/non-user group.
Analyses
Descriptive statistics and univariate logistic regression was used to identify demographic, clinical, and service need factors associated with membership in the repeat ED use group. Cases with missing data or response options of “Not Known” were excluded. Factors identified as significant (p < 0.05) in the bivariate analysis were then entered into a multivariate logistic regression model to identify the factors independently associated with repeat ED use.
Results
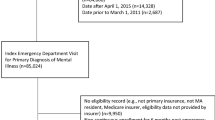
In total, 2611 patients were enrolled in case management programs. Emergency department utilization data were available for 2435 (93.3 %) patients. A further 161 cases (6.6 %) were excluded due to missing predictor variable data or response options of “Not Known”. Of the remaining 2274 individuals, the mean age was 47.11 years, more than half were female (n = 1162, 51.1 %) and nearly three quarters (n = 1649, 72.5 %) had a primary income source of public disability assistance, social assistance or no income source (Table 1). Most had a primary diagnosis of a mood disorder (n = 1016, 44.7 %) and over a quarter had a co-occurring substance use disorder present (n = 611, 26.9 %). The most prevalent unmet needs were psychological distress (n = 477, 21.0 %), followed by company (n = 461, 20.3 %), and money/benefits (n = 420, 18.5 %). The mean length of time in service was 3.73 years.
Of the sample, 1914 (84.2 %) had no ED visits for mental health reasons in the 6 months prior to their last OCAN, 214 (9.4 %) had one ED visit, 126 (5.5 %) had two to five ED visits and 20 (0.9 %) had six or more ED visits. In total, 146 (6.4 %) case management clients met criteria for repeat ED use, reporting two or more ED visits in the 6-month period prior to their last OCAN assessment. The median number of unmet needs for case management clients with two or more ED visits for mental health reasons was three with a range from 0 to 19 while the median number of unmet needs for clients with less than two ED visits was one with a range from 0 to 14. The distributions in the two groups differed significantly (Mann–Whitney U = 111,473, p < 0.001) (not shown in tables).
Table 2 displays the univariate logistic regression analyses between repeat ED visits and demographic, diagnostic and need factors. Compared to individuals with no ED visits or one ED visit within a 6-month span, those with two or more visits were more likely to be younger (16–24 years of age), receiving disability or social assistance or without an income source, have a primary diagnosis of a mood disorder, and have a co-occurring substance use disorder. In addition, they were more likely to be in service for a shorter duration. Individuals in service less than 1 year had the greatest odds of multiple visits as compared to individuals in service four or more years. A broad range of needs were also associated with repeat ED use. Needs related to psychiatric symptoms or conditions had the strongest association with repeat ED visits (i.e., safety to self/others, psychotic symptoms, substance use, psychological distress), followed by basic needs (i.e., accommodation, food, money/benefits) and social needs (i.e., company). Functional needs (i.e., taking care of home/self-care) were not associated with repeat ED use.
Multivariate logistic regression analyses examined factors independently associated with membership in the repeat ED visits group (Table 3). Length of stay in service was dichotomized to meet the assumption of linearity of the logit for logistic regression. Decreasing age (OR 0.98, 95 % CI 0.97–1.00), a primary diagnosis of a mood disorder (OR 1.58, 95 % CI 1.03–2.42), being in service less than 1 year (OR 1.94, 95 % CI 1.32–2.85) and unmet needs related to psychotic symptoms (OR 2.19, 95 % CI 1.36–3.54), substance use (OR 2.27, 95 % CI 1.37–3.76), and safety to self/others (OR 3.42, 95 % CI 1.99–5.88) were associated with membership in the population with repeat ED visits for mental health reasons. Conversely, primary income source, presence of a substance use disorder and unmet needs for accommodation, food, money/benefits, psychological distress and company were not correlated with repeat ED use.
Discussion
Prevalence of repeat ED use
Overall, there was a relatively low prevalence rate of repeat ED use within the sample with a little over 6 % of individuals enrolled in case management having 2 or more ED visits for mental health reasons in a 6-month period. This was lower than the rate found in other studies that applied a similar threshold for repeat ED use. Perez and colleagues [24] found 15.6 % of ED patients in a Canadian sample had two or more ED visits in the 6 months preceding their index emergency room consultation, while Dhossche and Ghani [20] found 18.1 % of ED patients in a US sample had two or more ED visits over a 7-month period. However, unlike the present study, these studies used community samples, not treatment samples such as those enrolled in mental health case management programming. Moreover, these studies did not rely on patient-reported ED utilization data.
Characteristics of individuals enrolled in case management with multiple ED visits
Repeat ED presenters enrolled in case management programs were more likely to be younger, to carry a primary diagnosis of a mood disorder, to be in case management for a shorter duration and have uncontrolled health issues (i.e., to be coping with the sequelae of psychosis or substance use and to be at risk for self-harm or harm to others). Individuals between the ages of 16 and 34 were at higher odds of repeat ED use. The association between younger age and ED use may relate to the age of onset for some psychiatric illnesses. For many in this age group, repeat ED use may be episodic rather than chronic. In addition, individuals with a primary diagnosis of an affective disorder were more likely than those with a psychotic disorder to have multiple ED visits; however, individuals with unmet needs related to managing psychotic symptoms were also more likely to be repeat ED presenters.
These results underscore the importance of distinguishing among subgroups of repeat ED presenters. Repeat ED users likely represent a number of distinct groups with differing need profiles that may be better elucidated by examining condition-specific clinical populations (e.g., individuals with psychotic disorders versus individuals with affective disorders) or demographic segments of the population (e.g., transitional aged youth versus adults). For example, the reasons for repeat use of the ED among patients with a psychotic disorder may be very different from those with a mood disorder or with a concurrent mental illness and substance use disorder. Pooling disparate populations may flatten sub-population (e.g., condition specific) effects that would assist with designing interventions tailored to population subgroups [4, 24, 36].
Length of time in case management was also important to consider. Shorter time in case management was associated with repeat ED use. Longer durations in case management may reduce repeat ED use, although examining this causal relationship would require longitudinal analyses.
The strongest correlates of repeat ED use were needs related to psychiatric symptoms or conditions (psychotic symptoms, alcohol and/or drug use, safety to self/others). Basic needs (e.g., food, accommodations), functional needs (self-care, looking after home), and social needs (e.g., company) were not independently associated with repeat ED utilization. These findings suggest that clinical rather than psychosocial needs have the strongest relationship with ED utilization among individuals receiving case management services. This is a departure from prior studies examining ED use among a general population of individuals with a psychiatric condition which have found psychosocial factors such as homelessness [21, 22], poverty [3, 17, 18, 21], and isolation [22] to be robust predictors of repeat ED use.
It is also noteworthy that proximal factors such as unmet needs related to psychiatric conditions had a greater relationship with multiple ED visit than more distal factors, such as diagnosis. By considering unmet service needs related to repeat ED use, case management providers may leverage the Camberwell assessment tools to identify individuals at greater risk of high utilization of emergency departments. Moreover, consideration of such needs may also assist with the design and implementation of case management programs that decrease ED use by targeting interventions at proximal factors predictive of repeat ED utilization: psychotic symptoms, alcohol/drug use, and risk of harm to self or others.
The relationship between unmet needs related to psychotic symptoms and repeat ED use may warrant the incorporation of evidence-based interventions for psychosis into the case management service delivery framework or their provision as adjunctive interventions. For example, cognitive behavioural therapy is a recommended intervention for psychosis that has been found to reduce hospital admissions, [37, 38] positive symptoms and associated depressive symptoms, and improve adherence to treatment [39]. Moreover, preliminary research has found that cognitive behaviour techniques for psychosis delivered by case managers under clinical supervision had a moderate to strong effect on the reduction of positive psychotic symptoms [40]. There is also evidence that family interventions using education and negotiated problem solving or crisis management work to reduce risk of relapse, hospital readmission and improve medication adherence [37, 41].
Consideration may also be given to modifying the case management service model to incorporate elements of the assertive community treatment (ACT) service model. ACT utilizes a multidisciplinary approach in which a team of social workers, nurses, psychiatrists and other health professions conduct assertive outreach with individuals who are reluctant to engage with service and support the patient at home. A systematic review and meta-regression study found that case management teams organized more similarly to ACT teams were better at reducing time in hospital [42]. Specifically, inpatient stays were shorter in cases where case managers operated as a team rather than as independent practitioners. The authors concluded that case management teams could optimize hospital use reductions through shared caseloads and by focusing on patients with a history of high hospital use. Future research is required to determine whether similar effects occur for ED visits.
A variant of ACT which may also hold promise for addressing the needs of individuals with unmet psychotic symptoms is flexible assertive community treatment (FACT). FACT represents a combination of ACT and ICM community care models within one multidisciplinary team. It includes individual case management for patients whose condition is currently stable and shared caseloads with an intensive full ACT approach for patients with current acute care needs, affording step-up and step-down service intensity as needed. Drukker and colleagues [43] found that for patients with unmet needs related to psychotic symptoms, symptom remission was higher in FACT than standard care (inpatient treatment, sheltered residential treatment and community treatment with broker-type case management). Future research, however, is required to replicate these findings.
Interventions to address unmet need related to substance use may also be advantageous. Both the relationship between unmet needs related to alcohol and drug use and multiple ED visits and the prevalence of concurrent disorders among repeat presenters (38.4 %) highlight a need for increasing capacity to integrate substance abuse interventions within the current delivery of case management services. An evidence-based integrated approach to treatment may include the provision of addiction services and mental health supports by the same team of providers, adoption of motivation-based treatment interventions to meet clients’ motivation for change (or stage of change) and/or multiple psychotherapeutic models including motivational interviewing, cognitive behavioral therapy, and group modalities within an overarching harm reduction framework [44]. Moreover, with such an approach, motivational interviewing should be considered a core clinical skill that is part of the basic training curriculum for all case management staff.
Unmet needs related to safety to self and others had the strongest relationship with repeat ED visits. Higher ED use and costs among patients with these unmet needs may relate to repeated episodes of deliberate self-harm (DSH) [45]. Extant research suggests that one of the strongest predictors of repeat episodes of DSH among patients presenting with self–harm to EDs is the presence of a personality disorder [46]. Linkage to dialectical behavior therapy (DBT) services may be undertaken to support individuals with personality disorders engaging in DSH. DBT is a comprehensive multicomponent intervention designed to treat individuals engaging in DSH who meet criteria for borderline personality disorder. DBT draws on strategies from cognitive and behavioural interventions, dialectics and mindfulness, and has four components: individual therapy, group skills training, therapist consultation and as-needed telephone coaching to patients. There is an accumulating evidence supporting the efficacy of standard DBT for reducing suicide attempts, self-injurious behaviours and utilization of emergency and inpatient services among individuals with borderline personality disorder [47, 48]. There is also evidence to support the incorporation of components of DBT into the delivery of case management services. In a randomized clinical trial, Linehan and colleagues evaluated the importance of the skills training component of DBT by comparing skills training plus case management with DBT individual therapy and standard DBT which includes skills training and individual therapy [49]. In the case management plus skills group intervention, case managers ran groups focusing on distress tolerance, emotion regulation, interpersonal effectiveness and mindfulness in addition to providing case management services. Case managers also received specialized training in the assessment and management of suicidal behavior. All three treatment conditions (i.e., individual therapy without skills groups, skills groups plus case management and standard DBT) resulted in similar improvements in the frequency and severity of suicide attempts, suicidal ideation, and use of crisis services due to suicidality. However, interventions that included skills training resulted in greater improvements reducing the frequency of non-suicidal self-injurious acts and depression.
Research examining the diagnostic profile of individuals with unmet needs in this domain and their specific presenting issues would further inform the selection of evidence-based interventions that address needs in this area.
Limitations
Some limitations for the present study must be considered. First, the data are cross-sectional. Consequently, we identified correlates of multiple ED visits but were not able to establish temporal and causal relationships in the absence of longitudinal data. Second, as the analyses relied on available administrative data, measurement of constructs which could be related to repeated ED use (e.g., adherence with treatment and prior medical history) could not be included. Third, though all programs within the study were funded as intensive case management programs, information about program composition, caseloads, staff training, clinical oversight, use of evidence-based interventions and fidelity to provincial program standards were not available. Consequently, the degree of heterogeneity in the approaches, resources and staff skills sets across programs is not known, limiting inferences about the effectiveness of specific interventions employed within programs. Fourth, data on ED utilization were obtained through patient self-report and as such were subject to the vagaries of recall, and may not accurately capture true usage rates. The low prevalence of ED utilization among this sample as compared to community samples may suggest under-reporting of ED visits. However, the relatively short reference period used to capture ED use (e.g., prior 6 months) and the operationalization of repeat ED visits as two or more visits within this period may mitigate the potential impact of recall bias. Fifth, the presence of correlated observations likely led to an underestimation or an overestimation of p values. Correlated data may arise when clusters of observations are related and thus are more similar to each other than to other observations in the dataset. Observations may be related because they derive from the same subject or because they derive from the same case manager caseload, program or service provider organization. Because data were anonymized by case management organizations prior to collation into a master dataset, there is a possibility that some portion of clients were enrolled in two or more case management programs at the same time. However, as data collection was limited to individuals enrolled in service on a specific day, the risk of duplicate cases existing across organizations is minimized. Moreover, multivariate logistic regression was used instead of generalized linear mixed models despite the nesting of data within organizations since in random intercept and mixed models, the effect of organization was not significant. Nevertheless, it was not possible to discern which cases were correlated because they were part of a common caseload or program as data were obtained at the organizational level.
Directions for future research
The above findings offer insight about some of the factors associated with repeat ED use among patients with psychiatric conditions receiving ICM and also give rise to lines of inquiry for future research. Foremost among these is characterizing discrete subgroups who are frequent ED presenters. There may be sharp differences among frequent ED presenters on the basis of psychiatric condition or demographic segment [4]. Moreover, need profiles may vary among frequent ED presenters who are episodic users of ED services and those who are chronic users. Understanding these distinctions will be key to tailoring generic program-based approaches like case management to the needs of distinct subgroups of patients with high ED utilization. A parallel line of inquiry might examine what specific case management program facets affect reductions in repeat ED use. Though research has started to examine the efficacy of case management as an intervention to reduce ED utilization, this research has been limited by a lack of data on program structures, processes and interventions. Indeed, differences in these program facets may, in part, account for mixed results across studies evaluating the effectiveness of case management to reduce repeated ED use. More work is needed to characterize these program facets and identify how they may affect reductions in ED use and for which clinical subgroups.
Conclusions
In sum, our findings showed a small subgroup within mental health case management who experience repeated ED use. This group may be composed of distinct subgroups with unique need profiles which may be better discerned by examining correlates of ED utilization among diagnostic subgroups and/or demographic population segments. In addition, they highlight the relative importance of dynamic risk factors related to unmet need over distal and static factors such as diagnosis. Moreover, these findings suggest that clinical rather than psychosocial needs have a stronger relationship with ED utilization among individuals receiving case management services. Specifically, needs related to psychotic symptomatology, substance use and safety risks were more strongly linked to repeated ED use. These may be important areas for intervention to engage repeat presenters in community-based care to alleviate pressure from costly hospital-based emergency services and better meet the needs of this service population.
References
Sun BC, Burstin HR, Brennan TA (2003) Predictors and outcomes of frequent emergency department users. Acad Emerg Med 10(4):320–328. doi:10.1111/j.1553-2712.2003.tb01344.x
Wooden MD, Air TM, Schrader GD, Wieland B, Goldney RD (2009) Frequent attenders with mental disorders at a general hospital emergency department. Emerg Med Aust 21(3):191–195. doi:10.1111/j.1742-6723.2009.01181.x
Chaput YV, Lebel MJ (2007) Demographic and clinical profiles of patients who make multiple visits to psychiatric emergency services. Psychiatr Serv 58(3):335–341. doi:10.1176/ps.2007.58.3.335
LaCalle E, Rabin E (2010) Frequent users of emergency departments: the myths, the data and the policy implications. Ann Emerg Med 56(1):42–48. doi:10.1016/j.annemergmed.2010.01.032
Blanks FS, Li H, Hennenman PL, Smithline HA, Santoro JS, Provost D, Maynard AM (2005) A descriptive study of heavy emergency department users at an academic emergency department reveals heavy ED users have better access to care than average users. J Emerg Nurs 31(2):139–144. doi:10.1016/j.jen.2005.02.008
Riggs JE, Davis SM, Hobbs GR, Paulson DJ, Chinnis AS, Heilman PL (2003) Association between early returns and frequent ED visits at a rural academic medical center. Am J Emerg Med 21(1):30–31. doi:10.1053/ajem.2003.50017
Cook LJ, Knight S, Junkins EP Jr, Mann NC, Dean JM, Olson LM (2004) Repeat patients to the emergency department in a statewide database. Acad Emerg Med 11(3):256–263. doi:10.1111/j.1553-2712.2004.tb02206.x
Hunt KA, Weber EJ, Showstack JA, Colby DC, Callaham ML (2006) Characteristics of frequent users of emergency departments. Ann Emerg Med 48(1):1–8. doi:10.1016/j.annemergmed.2005.12.030
Vandyk AD, Harrison MB, VanDenLerkhof EG, Graham ID, Ross-White A (2013) Frequent emergency department use by individuals seeking mental healthcare: a systematic search and review. Arch Psychiatr Nurs 27(4):171–178. doi:10.1016/j.apnu.2013.03.001
Mehl-Madrona LE (2008) Prevalence of psychiatric diagnoses among frequent users of rural emergency medical services. Can J Rural Med 13(4):22–30
Williams ER, Guthrie E, Mackway-Jones K, James M, Tomenson B, Eastham J, McNally D (2001) Psychiatric status, somatisation, and health care utilization of frequent attenders at the emergency department: a comparison with routine attenders. J Psychosom Res 50(3):161–167. doi:10.1016/S0022-3999(00)00228-2
Curran GM, Sullivan G, Williams K, Hans X, Collins K, Key J, Kotria KJ (2003) Emergency department use of persons with comorbid psychiatric and substance abuse disorders. Ann Emerg Med 41(5):659–667. doi:10.1067/mem.2003.154
Oven HJ, Chan BT (2001) Heavy users of emergency services: a population-based review. Can Med Assoc J 165(8):1049–1050
Markham D, Graudin A (2011) Characteristics of frequent emergency department presenters to an Australian emergency medicine network. BMC Emerg Med 11:21–26. doi:10.1186/1471-227X-11-21
Mandelberg JH, Kuhn RE, Kohn MA (2000) Epidemiologic analysis of an urban, public emergency department’s frequent users. Acad Emerg Med 7(6):637–646. doi:10.1111/j.1553-2712.2000.tb02037.x
Aagaard J, Aagaard A, Buus N (2014) Predictors of frequent visits to a psychiatric emergency room: a large-scale register study combined with a small-scale interview study. Int J Nurs Stud 51(7):1003–1013. doi:10.1016/j.ijnurstu.2013.11.002
Ledoux Y, Minner P (2006) Occasional and frequent repeaters in a psychiatric emergency room. Soc Psychiatry Psychiatric Epidemiol 41(2):115–121. doi:10.1007/s00127-005-0010-6
Chaput YJ, Lebel MJ (2007) An examination of the temporal and geographical patterns of psychiatric emergency service use by multiple visit patients as a means for their early detection. BMC Psychiatry 7:60. doi:10.1186/1471-244X-7-60
Bruffaerts R, Sabbe M, Demyttenaere K (2006) Who visits the psychiatric emergency room for the first time? Soc Psychiatry Psychiatr Epidemiol 41(7):580–586. doi:10.1007/s00127-006-0062-2
Dhossche DM, Ghani SO (1998) A study on recidivism in the psychiatric emergency room. Ann Clin Psychiatry 10(2):59–67. doi:10.3109/10401239809147744
Arfken CL, Zeman LL, Yeager L, White A, Mischel E, Amirsadri A (2004) Case-control study of frequent visitors to an urban psychiatric emergency service. Psychiatr Serv 55(3):295–301. doi:10.1176/appi.ps.55.3.295
Pasic J, Russo J, Roy-Byrne P (2005) High utilizers of psychiatric emergency services. Psychiatr Serv 56(6):678–684. doi:10.1176/appi.ps.56.6.678
Saarento O, Hakko H, Joukamaa M (1998) Repeated use of psychiatric emergency out-patient services among new patients: a 3-year follow-up study. Acta Psychiatr Scand 98(4):276–282. doi:10.1111/j.1600-0447.1998.tb10084.x
Perez E, Minoletti A, Blouin J, Blouin A (1986) Repeated users of a psychiatric emergency service in a Canadian general hospital. Psychiatr Q 58(3):189–201. doi:10.1007/BF01064733
Ellison JM, Blum N, Barsky AJ (1989) Frequent repeaters in a psychiatric emergency service. Hosp Comm Psychiatry 44(4):372–375. doi:10.1176/ps.40.9.958
Althaus F, Paroz S, Hugll O, Ghall WA, Daeppen JB, Peytremann-Bridevaux I, Bodenmann P (2011) Effectiveness of interventions targeting frequent users of emergency departments: a systematic review. Ann Emerg Med 58(1):41–52. doi:10.1016/j.annemergmed.2011.03.007
Curtis J, Millman E, Struening E, D’Ercore A (1992) Effects of case management on rehospitalization and utilization of ambulatory care services. Hosp Community Psychiatr 43(9):895–908
Craig TJ, Bracken J (1995) A case-control study of rapid readmission in a state hospital population. Ann Clin Psychiatry 7(2):79–85. doi:10.3109/10401239509149031
Phillips GA, Brphy DS, Weiland TJ, Chenhall AJ, Dent AW (2006) The effect of multidisciplinary case management on selected outcomes for frequent attenders at an emergency department. Med J Aust 184(12):602–606
Ontario Ministry of Health and Long-Term Care (2005) Intensive case management services standards for mental health services and supports. Queen’s Printer for Ontario. http://health.gov.on.ca/en/common/ministry/publications/reports/mentalhealth/intens_cm.pdf. Accessed 25 May 2015
Ontario Ministry of Health and Long-Term Care (2004) Community Mental Health—Common Data Set—Mental Health (CDS-MH) Version 2. Toronto: Information Management Unit, Finance and Information Management Branch, Ministry of Health and Long-Term Care
Community Care Information Management (2010) Ontario common assessment of need (OCAN): OCAN user guide 2.0. https://www.ccim.on.ca/CMHA/OCAN/Private/Document/Education%20and%20Training%20v2.0/OCAN%202%20Day%20Training%20Materials/OCAN%202%20Day%20Training%20-%20User%20Binder/Tab%201%20-%20OCAN%20User%20Guide.pdf. Accessed 25 May 2015
IBM Corp. (2013) IBM SPSS Statistics for Windows, Version 22.0. IBM Corp, Armonk
Wennström E, Wiesel FA (2006) The Camberwell assessment of need as an outcome measure in routine mental health care. Soc Psychiatry Psychiatr Epidemiol 41(9):728–733. doi:10.1007/s00127-006-0084-9
Community Care Information Management and Ontario Common Assessment of Need (OCAN): Community mental health common assessment project: Full OCAN 2.0 Revision 2.0.5. https://www.ccim.on.ca/CMHA/OCAN/Private/Document/Assessment%20Tool%20v2.0/OCAN_2.0/OCAN_2.0_FULL_v2.0.5i.pdf. Accessed 25 May 2015
Doupe MB, Palatnick W, Day S, Chateau D, Soodeen RA, Burchill C, Derksen S (2012) Frequent users of emergency departments: developing standard definitions and defining prominent risk factors. Ann Emerg Med 60(1):24–32. doi:10.1016/j.annemergmed.2011.11.036
National Collaborating Centre for Mental Health (2014) Psychosis and schizophrenia in adults: treatment and management. National Institute for Health and Care Excellence, London. http://www.guideline.gov/content.aspx?id=47863. Accessed 25 May 2015
Malik N, Kingdon D, Pelton J, Mehta R, Turkington D (2009) Effectiveness of brief cognitive-behavioral therapy for schizophrenia delivered by mental health nurses: relapse and recovery at 24 months. J Clin Psychiatry 70(2):201–207. doi:10.4088/JCP.07m03990
Rathod S, Turkington D (2005) Cognitive-behaviour therapy for schizophrenia: a review. Curr Opin Psychiatry 18(2):159–163. doi:10.1097/00001504-200503000-00009
Turkington D, Munetz M, Pelton J, Monesano V, Sivec HJ, Nausheen B, Kingdon D (2014) High-yield cognitive behavioral techniques for psychosis delivered by case managers to their clients with persistent psychotic symptoms: an exploratory trial. J Nerv Ment Dis 202(1):30–34. doi:10.1097/NMD.0000000000000070
Jung XT, Newton R (2009) Cochrane reviews of non-medication-based psychotherapeutic and other interventions for schizophrenia, psychosis, and bipolar disorder: a systematic literature review. Int J Ment Health Nurs 18(4):239–249. doi:10.1111/j.1447-0349.2009.00613.x
Burns T, Catty J, Dash M, Roberts C, Lockwood A, Marshall M (2007) Use of intensive case management to reduce time in hospital in people with severe mental illness: systematic review and meta-regression. BMJ 335(7615):336–340. doi:10.1136/bmj.39251.599259.55
Drukker M, Maarschalkerweerd M, Bak M, Driessen G, a Campo J, de Bie A, Poddighe G, van Os J, Delespaul P (2008) A real-life observational study of the effectiveness of FACT in a Dutch mental health region. BMC Psychiatry 8:93. doi:10.1186/1471-244X-8-93
Horsfall J, Cleary M, Hunt GE, Walter G (2009) Psychosocial treatments for people with co-occuring severe mental illnesses and substance user disorders (dual diagnosis): a review of empirical evidence. Harv Rev Psychiatry 17(1):24–34. doi:10.1080/10673220902724599
Sinclair JH, Gray A, Rivero-Arias O, Saunders KE, Hoawton K (2011) Healthcare and social services resource use and costs of self-harm patients. Soc Psychiatry Psychiatr Epidemiol 46(4):263–271. doi:10.1007/s00127-010-0183-5
Larkin C, Blasi Z, Arensman E (2014) Risk factors for repetition of self-harm: a systematic review of prospective hospital-based studies. PLoS One 9(1):e84282. doi:10.1371/journal.pone.0084282
Kliem S, Kröger C, Kosfelder J (2010) Dialectical behavior therapy for borderline personality disorder: a meta-analysis using mixed effects modelling. J Consult Clin Psychol 78(6):936–951. doi:10.1037/a0021015
Stoffers JM, Vollm BA, Rucker G, Timmer A, Husband N, Lieb K (2012) Psychological therapies for people with borderline personality disorder. Cochrane Database Syst Rev 8:CD005652
Linehan MM, Korslund KE, Harned MS, Gallop RJ, Lungu A, Neacsiu AD, McDavid J, Comtois KA, Murray-Gregory AM (2015) Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: a randomized clinical trial and component analysis. JAMA Psychiatry 72(5):475–482. doi:10.1001/jamapsychiatry.2014.3039
Acknowledgments
The authors would like to thank the managers and data support staff of the organizations participating in this study for their time and assistance in pulling data for this study. This research was made possible by funding from the Toronto Central Local Health Integration Network (TC LHIN) which is gratefully acknowledged. The views expressed in this report do not necessarily reflect those of the TC LHIN or the Ontario Ministry of Health and Long-Term Care.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Sirotich, F., Durbin, A. & Durbin, J. Examining the need profiles of patients with multiple emergency department visits for mental health reasons: a cross-sectional study. Soc Psychiatry Psychiatr Epidemiol 51, 777–786 (2016). https://doi.org/10.1007/s00127-016-1188-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-016-1188-5