
Abstract
Background
Literature describing stigmatizing attitudes towards people with mental illness by children in the developing world is lacking. Children’s mental health issues in the Kenyan context are especially pertinent due to the increased likelihood of exposure to risk factors and the high prevalence of mental disorders. The objective of the current study was to examine socio-demographic factors associated with the endorsement of stigmatizing attitudes towards people with mental illness among Kenyan school children.
Methods
We analyzed cross-sectional survey data from 4585 primary school-aged children in standards one through seven in the Eastern Province of Kenya. We examined relationships between the endorsement of stigmatizing attitudes and age, gender, district, religion, being in the standard appropriate for one’s age, and parental employment status.
Results
Stigma scores decreased with increasing age (β = −0.83; 95 % CI = −0.99 to −0.67). Boys had higher stigma scores compared to girls (β = 1.55; 95 % CI = 0.86–2.24). Students from the rural district had higher average stigma scores as compared to those from the peri-urban district (β = 1.14; 95 % CI = 0.44–1.84). Students who were not in the standard appropriate for their age had lower stigma scores than those who were in the standard typical for their age (β = −1.60; 95 % CI = −2.43 to −0.77).
Conclusions
Stigmatizing attitudes toward the mentally ill exist among primary school children in Kenya; thus, anti-stigma interventions are needed, and our findings highlight particular subgroups that could be targeted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Stigmatizing attitudes towards people with mental illness is a pervasive issue with far-reaching consequences. Defined as the unwarranted social devaluing of a person or group based on an actual or inferred attribute [1, 2], stigma is comprised of the stereotypes, prejudices, and discriminatory behaviors that prevent individuals or groups from participating fully in society [3, 4]. Mental health stigma may result in perceptions of affected people as being less intelligent, less trustworthy, less employable, and less favorable as romantic partners [5]. Mental health stigma may have detrimental effects on people due to hesitation to disclose psychiatric diagnoses [6], as well as decreased help-seeking behaviors and treatment compliance [7], potentially worsening prognosis.
The endorsement of stigmatizing attitudes is strongly linked to the social and cultural context; therefore, differences in the construct of stigma and its consequences are seen around the globe [2, 8]. The definition and experience of mental illness, beliefs about its etiology, and the treatment deemed acceptable vary widely between countries [9–11]. A study of stigma in 16 countries found that there was more stigma surrounding mental illness in developing countries compared to developed countries [12]. Furthermore, a study comparing stigmatizing attitudes between people from Canada and Cameroon (Africa) found that the levels of stigma were higher in the African context [8]. Similarly, Barke and colleagues [5] found higher levels of stigma and socially restrictive views in Ghana, including the belief that people with mental illness are inferior and should be socially isolated. This group also found that people with mental illness coped with stigmatizing beliefs by being more secretive about their mental illness, and this unwillingness to disclose was a barrier to seeking treatment [5]. Additional work in Nigeria [13, 14] and South Africa [15, 16] also demonstrated that mental illness stigma was a barrier to care.
Although the vast majority of research on mental illness stigma has been conducted in adult populations, stigma can play a unique role in child and youth populations, where social acceptance and belonging are highly desired [1]. Previous work has demonstrated that children do hold stigmatizing beliefs and that they may keep a greater social distance from their mentally ill peers [10]. Furthermore, children with emotional and behavioral problems who experience rejection are at risk of poor developmental outcomes and problem behavior [17, 18].
There is currently a paucity of research on mental health stigma in Kenya. Although neuropsychiatric disorders account for 5.7 % of the global burden of disease in Kenya [19], Kenyans lack knowledge about mental illness [20, 21]. There is a particular need to explore stigmatizing attitudes towards mental illness among children in Kenya. Children’s mental health issues in the Kenyan context are especially pertinent due to the increased likelihood of exposure to risk factors such as child labour, physical punishment, HIV/AIDS-related orphanhood, and exposure to post-election violence. Moreover, previous work in Kenya has demonstrated that among school-aged children, there is a high prevalence of anxiety disorders [22], post-traumatic stress disorder [23], major depressive disorder [22], suicidality [22], and substance use [24]. Mental health issues in children have consequences that extend far beyond childhood; thus, to prevent the persistence of mental illness into adulthood, it is essential that child mental health issues are investigated and addressed [25], and this includes addressing factors that may contribute to the high burden of illness and barriers to seeking care, such as stigma towards people with mental illness. Understanding stigma and its correlates is the first step in combating stigma towards mental illness and mitigating the consequent poor outcomes.
The objective of this study was to examine socio-demographic factors that are associated with the endorsement of stigmatizing beliefs towards people with mental illness among school children in the Eastern Province of Kenya in an effort to identify subgroups that could be targeted for anti-stigma initiatives.
Materials and methods
Study sites
This study was conducted in two separate districts of the Eastern Province of Kenya. The rural Makindu District has a total population of 70,302, including 21,680 children enrolled in 66 primary schools. The peri-urban Machakos District has a total population of 442,930, with 44,603 children enrolled in 129 primary schools. The schools in Makindu District are divided into three clusters, and the schools in Machakos District are divided into six clusters. Both districts have similar school enrollment by gender.
Kenya rolled out free primary school education in 2003 and witnessed a surge in enrolment, from 77 % in 2002 to 94 % in 2009, meaning that the majority of eligible children would be enrolled in school [26]. Reports have indicated that children who are eligible for school may not be enrolled due to non-tuition-based education costs (eg., uniform, books, transportation), a lack of physical access to a school, and other non-monetary factors, such as poor nutrition and health [27]. The findings from this study are therefore representative of the majority of eligible children in the two districts.
Study sample
Primary school in Kenya runs from standard one (age 6 years) to standard eight (age 13 years). At the time of data collection, students in standard eight were completing exams and were not available to participate. Students from standards one through seven in both Makindu and Machakos Districts were included in the sample. One cluster from each district was randomly selected. Within each cluster, 23 schools were selected using simple random sampling (Makindu District = 11; Machakos District = 12).
Students in standards one through seven are typically between the ages of 6 and 12 years. However, some pupils in these classes were older than this age bracket due to failure to excel academically or late primary school entry, with the latter due to the introduction of free primary education in 2003. We observed that a large proportion of students (≈40 %) were not in the standard appropriate for their age, defined as being more than 1 year older than the typical age for a particular standard. To prevent losing a large proportion of students, we opted to include all students in the analysis irrespective of age, although we adjusted for this factor in the multivariate analyses.
The principal of each school granted permission for study investigators to enter the schools. The parents of students in standards one to seven in the selected schools were informed of the project goals, benefits, risks, and confidentiality measures, and they provided written informed consent for their child to participate. In addition, all children received a detailed verbal explanation of the study, including the voluntary nature of participation, and gave written assent before participating in the study. Ethics approval was obtained from the Research Ethics Board at the Centre for Addiction and Mental Health and from the Kenya Medical Research Institute.
Data collection
The data were collected as part of the baseline data collection for the Kenyan Integrated Intervention Model for Dialogue and Screening to Promote Children’s Mental Well-being (KIDS) project—a primary school-based program aimed at promoting mental well-being, preventing mental illness, and reducing the treatment gap for children.
We assessed the endorsement of stigmatizing attitudes towards people with mental illness using the stereotype agreement subscale from the Self-Stigma of Mental Illness Scale. The stereotype agreement subscale is a 10-item self-report measure using statements that describe stereotypes commonly believed to be associated with people with mental illness (Appendix). Responses fell along a nine point agreement scale (1 = strongly disagree; 9 = strongly agree). The stereotype agreement subscale has been previously found to have acceptable levels of internal consistency (Cronbach’s α = 0.72) and test–retest reliability (r = 0.68), and good content validity [28]. It has previously been used in different cultural groups [29, 30]; however, it has not been validated for the Kenyan context or for use in children. A total score on the stereotype agreement scale between 10 and 90 is reported, with a higher score indicating the endorsement of more stigmatizing beliefs.
The data collection instrument was translated into the local languages (Kiswahili and Kamba), and then back translated by an independent linguist. Inconsistencies were discussed amongst a group of bilingual speakers from a variety of backgrounds (linguist, psychiatrist, clinical psychologist, nurse, teacher, and lay persons). Forward and backward translations were performed until there was consensus. Students in standards one to four completed the instruments in Kamba or English in an interview format due to the limited literacy of this age group. Students in standards five to seven self-completed the instruments in Kiswahili or English.
All data collection was administered by research assistants who had completed high school and had previous research experience or had taken a related course. The instruments used for the current analysis were completed as part of a battery of tools used for baseline data collection for the KIDS project. A total of 45 min was needed to complete all of the instruments. The completed assessments were reviewed for inconsistencies or missing information, and incorrectly completed forms were returned to the participant for correction. The forms were then sent to a central office for cleaning and data entry.
Data analysis
The data were coded and double-entered into Stata SE Version 12.1 [31]. For responses that fell outside of the range of the stereotype agreement subscale (i.e., 0 or 10), the response was replaced with the minimum or maximum scale value (i.e., 1 or 9, respectively) (n = 24). The analyses include all participants with complete data on the stereotype agreement subscale and the covariates of interest.
Descriptive information on study participants is presented as proportions for count data and as means with standard deviations (SD) for continuous data. Simple linear regression analyses were performed to examine unadjusted relationships between scores on the stereotype agreement subscale and the following covariates: age, gender, district, religion, father’s employment status, mother’s employment status, and whether the child was age-appropriate for standard. The classification of the remaining variables can be found in Table 1. Finally, multivariate linear regression models including the aforementioned covariates were used to examine independent predictors of scores on the stereotype agreement subscale. All results from the regression models are presented as β-coefficients with corresponding 95 % confidence intervals (CI), and confidence intervals that do not include zero are considered statistically significant.
Results
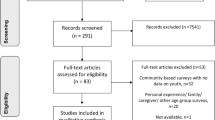
A total of 5469 students participated in the study, and there were no refusals by parents or children. Of those, 884 were missing a response in at least one variable of interest, resulting in a final sample size of 4585 (84 % of total). Demographic information for participants with complete and incomplete survey data is provided in Table 1. There were differences between the groups such that a greater proportion of students with incomplete data were from Machakos District and were not in the age-appropriate grade; however, the scores on the stereotype agreement subscale and all remaining covariates were similar between students with complete and incomplete data.
The mean age of participants was 10.4 years (SD 2.6), ranging from 5 to 21 years (99 % of the sample were ≤16 years). There was an even split by gender and district. For religion, the largest proportion of students identified as Protestant, followed by Catholic, and only a negligible proportion identified as an African Traditional Religion, Muslim, other religion, or as not having any religion. More than 70 % of students had fathers who were employed, while 37 % reported that their mother was employed. Approximately 60 % of students were in the age-appropriate grade (Table 1).
The mean score on the stereotype agreement subscale for the total sample was 55.4 (SD 11.9, interquartile range 48–64), which is slightly higher than the midpoint of the range of possible scores (10–90). We found statistically significant associations between scores and the covariates age, gender, and district in both the unadjusted and adjusted analyses (Table 2). When adjusted for all other covariates, there was an inverse relationship between age and the endorsement of stigmatizing attitudes, such that as age increased, stigma scores decreased (β = −0.83; 95 % CI = −0.99 to −0.67). Boys had higher scores compared to girls (β = 1.55; 95 % CI = 0.86–2.24). Similarly, students from Makindu District had higher average scores as compared to those from Machakos District (β = 1.14; 95 % CI = 0.44–1.84) (Table 2).
In the unadjusted analyses, students who identified as African Traditional Religion had lower scores on the stereotype agreement subscale than students who identified as Catholic (β = −4.69; 95 % CI = −9.31 to −0.06). Adjustment for effects of the other covariates attenuated the parameter estimates and the association was no longer statistically significant (β = −2.61; 95 % CI = −7.18 to 1.96) (Table 2).
The association between age-appropriate grade and endorsement of stigmatizing attitudes was not statistically significant in the unadjusted analysis, but became significant in the adjusted analysis when the effects of the other covariates were accounted for (Table 2). In the adjusted analysis, students who were not in the age-appropriate grade had lower scores on the stereotype agreement subscale than those who were in the age-appropriate grade (β = −1.60; 95 % CI = −2.43 to −0.77).
We did not find evidence of a statistically significant relationship between the endorsement of stigmatizing attitudes and the employment status of either parent (Table 2).
Discussion
This study describes the factors that are correlated with the endorsement of stigmatizing attitudes among primary school children in the Eastern Province of Kenya. The findings suggest that stigma towards mental illness is prevalent in this population, and that particular socio-demographic factors may be related to the likelihood of endorsing stigmatizing attitudes.
Gender differences
According to the present findings, boys have more stigmatizing attitudes towards mental illness than girls. This is in line with previous research suggesting that male children and adolescents [32–34], as well as adults [35, 36], tend to hold more stigmatizing beliefs than females. Dogra and colleagues [10] demonstrated that girls and boys in Nigeria have differing knowledge and beliefs about mental illness. One explanation for this gender difference may be that males have less familiarity with mental illness, as some illnesses, such as depression, are more prevalent among females [36]. However, it is unknown whether this explanation holds for school children in the Kenyan context, as these factors were not assessed in the current study.
Age differences
This study found that the endorsement of stigmatizing attitudes decreases with increasing age of primary school children. Previous literature is inconclusive, with some work demonstrating an increase in stigma as children get older [32, 37, 38], whereas other research suggests the opposite [38–40]. More specifically, Whalen and colleagues [40] studied 654 students between fourth and tenth grade, and found that older students avoided mental illness labels and held fewer stigmatizing beliefs. Perhaps this is due to a clearer understanding of mental illness and its etiology as children mature [38]. Another explanation is offered by Corrigan and Watson [39], who found that prejudice regarding mental illness tends to decrease between the ages of 5 and 7 years. They explain that although children at this age have knowledge of the stereotypes associated with groups to which they do not belong, they may learn that it is important to constrain their prejudicial beliefs according to the norms of social desirability.
Geographic differences
Our study found that children in rural environments (i.e., Makindu District) are more likely to endorse stigmatizing attitudes than children in urban environments (i.e., Machakos District). Although the nature of our data prevents us from ascertaining the reason behind this observed difference, findings from previous studies provide some potential explanations. For example, other investigators have suggested that the difference in knowledge and beliefs regarding the causation of mental illness [10, 13], as well as the emphasis on self-reliance [4, 41], that are present in rural communities all contribute to higher levels of stigmatizing beliefs. Previous work with adults in Nigeria has found that people in rural areas believe that associating with a person with mental illness may be risky, and also tend to endorse beliefs in supernatural causation [13]. A belief in supernatural causation has been linked to social distance, which is used as a proxy for stigma, such that people who believe that mental illness is caused by supernatural forces tend to have higher levels of stigma toward the mentally ill [42]. It has also been suggested that one reason stigmatizing attitudes are so highly prevalent in rural contexts is because these attitudes allow community members to limit their obligation to the mentally ill—a significant challenge in areas where access to formal mental health services are limited [4]. Future research should examine the role that explanatory models of illness and availability of formal health services play in mediating the urban/rural differences that we observed in the endorsement of stigmatizing attitudes towards people with mental illness.
Religious differences
According to the results of our multivariate model, the endorsement of stigmatizing attitudes was not associated with religious affiliation. This is interesting to note as religious-based differences in mental health beliefs are well established in the literature, including differences in community stigma towards mental illness [43, 44] as well as health beliefs and mental health treatment seeking [43, 45]. Of particular importance, previous research has demonstrated that traditional religions tend to maintain stronger beliefs in supernatural causation of mental illness and may be more socially restrictive in their views [13]; thus, it is noteworthy that students of the African Traditional Religion demonstrated the same level of stigmatizing attitudes as students of other religions. However, the proportion of students who self-identify as African Traditional Religion was negligible, which may have limited our ability to observe a difference.
Differences by age-appropriate standard
Almost half of the students in this study were not in the standard appropriate for their age. The results of our multivariate model suggest that students who are not in the age-appropriate standard had lower stigma levels than those who were in the standard typical for age. Other work from this project suggests that children who are not in the age-appropriate standard also have a higher prevalence of mental disorders [46]. It is possible that these students are less likely to endorse stigmatizing attitudes towards mental illness due to their own experiences with a mental disorder. The reason why students are not in the age-appropriate standard (i.e., falling behind vs. late entry) and how this is connected to the endorsement of stigmatizing attitudes warrants further exploration.
Differences in parental employment status
Our results suggest that the employment status of parents did not have an impact on stigmatizing attitudes among the school children. Although only a very crude indicator of socio-economic status, this finding is in line with other research looking at children and adolescents in Ireland, which found that parental education levels did not have an effect on stigma levels [37]. On the other hand, the work of Jackson and Heatherington [47] in Jamaica suggests that students of lower socio-economic position were less socially restrictive and were less likely to attribute the cause of mental illness to a lack of willpower or to laziness. These authors suggested that their findings could be explained by the fact that people from lower socio-economic position may be better able to understand that stressors may impact mental health. They may also have more familiarity with mental illness, as they would be more likely to encounter homeless or mentally ill people in their neighbourhoods [47]. Further work using more robust measures of socio-economic status is needed to clarify its link with attitudes towards mental illness in the Kenyan context.
Policy and practice implications
Although this paper clearly identifies significant levels of mental illness stigma in schools, further research on intervention strategies is needed to address this challenge. Prior literature points towards education on mental illness as a potential avenue for reducing stigma, and our findings highlight particular areas where this could be targeted. Specifically, the finding that stigmatizing attitudes reduced with increasing age, which may be attributable to a better understanding of and empathetic attitude to mental illness, suggests that educational initiatives aimed at improving knowledge of mental illness may reduce stigmatizing attitudes. Further, the finding that the peri-urban Machakos District had less endorsement of stigmatizing attitudes, possibly due to better exposure to services and the medical model of disease than the mainly rural Makindu District, suggests that education about the causes of mental illness may help to reduce stigmatizing attitudes. Community education programs on mental illness could be delivered in schools as a feasible intervention to reduce stigma. Future studies should be directed towards supporting the development of strategies that reduce stigma towards mental illness among children in developing countries and ameliorate understanding of these programs for potential scale-up.
Limitations
This study has a number of limitations. The sample was taken from one Kenyan province; therefore, generalizing the findings to other cultural contexts must be done with caution. Additionally, approximately 6 % of Kenyan children are not enrolled in school due to financial barriers or poor health and nutrition status [27]; therefore, the attitudes endorsed by the children in our sample cannot be generalized to these vulnerable subgroups. The stereotype agreement scale was used as a data collection tool, yet it has not been formally validated for use in the Kenyan context nor with children. Despite efforts to ensure accurate translation, participants’ interpretation of questions may be dissimilar from the English meaning or mistakenly nuanced based on the cultural setting. Parent employment status was used as a proxy for socio-economic status; however, socio-economic status is comprised of multiple factors, and the use of a single variable may not provide a complete or accurate picture of socio-economic status [48].
Conclusions
This study has provided a clearer picture of the mental illness stigma that exists among primary school children in the Eastern Province of Kenya. We found evidence to suggest that stigmatizing attitudes toward mental illness exist in Kenya, and we identified several socio-demographic factors that may be predictive of stigmatizing attitudes and a potential target for anti-stigma efforts.
References
Mukolo A, Heflinger CA, Wallston KA (2010) The stigma of childhood mental disorders: a conceptual framework. J Am Acad Child Adolesc Psychiatry 49:92–103
Weiss MG, Ramakrishna J, Somma D (2006) Health-related stigma: rethinking concepts and interventions. Psychol Health Med 11:277–287
Hinshaw SP, Stier A (2008) Stigma as related to mental disorders. Ann Rev Clin Psychol 4:367–393
Boyd CP, Hayes L, Sewell J, Caldwell K, Kemp E, Harvie L et al (2008) Mental health problems in rural contexts: a broader perspective: response to Jackson et al. (2007) Mental health problems in rural contexts: what are the barriers to seeking help from professional providers? Aust Psychol 43:2–6
Barke A, Nyarko S, Klecha D (2011) The stigma of mental illness in Southern Ghana: attitudes of the urban population and patients’ views. Soc Psychiatry Psychiatr Epidemiol 46:1191–1202
Lasalvia A, Zoppei S, Van Bortel T, Bonetto C, Cristofalo D, Wahlbeck K et al (2013) Global pattern of experienced and anticipated discrimination reported by people with major depressive disorder: a cross-sectional survey. Lancet 381:55–62
Sirey JA, Bruce ML, Alexopoulos GS, Perlick DA, Friedman SJ, Meyers BS (2001) Stigma as a barrier to recovery: perceived stigma and patient-rated severity of illness as predictors of antidepressant drug adherence. Psychiatr Serv 52:1615–1620
St. Louis KO, Roberts PM (2013) Public attitudes toward mental illness in Africa and North America. Afr J Psychiatr 16:123–133
Robles-Garcia R, Fresan A, Berlanga C, Martinez N (2013) Mental illness recognition and beliefs about adequate treatment of a patient with schizophrenia: association with gender and perception of aggressiveness-dangerousness in a community sample of Mexico City. Int J Soc Psychiatry 59:811–818
Dogra N, Omigbodun O, Adedokun T, Bella T, Ronzoni P, Adesokan A (2012) Nigerian secondary school children’s knowledge of and attitudes to mental health and illness. Clin Child Psychol Psychiatry 17:336–353
Peluso EDTP, Blay SL (2004) Community perception of mental disorders: a systematic review of Latin American and Caribbean studies. Soc Psychiatry Psychiatr Epidemiol 39:955–961
Alonso J, Buron A, Bruffaerts R, He Y, PosadaVilla J, Lepine JP et al (2008) Association of perceived stigma and mood and anxiety disorders: results from the World Mental Health Surveys. Acta Psychiatr Scand 118:305–314
Adewuya AO, Makanjuola ROA (2008) Social distance towards people with mental illness in southwestern Nigeria. Aust N Z J Psychiatry 42:389–395
Gureje O, Lasebikan VO (2006) Use of mental health services in a developing country: results from the Nigerian survey of mental health and well-being. Soc Psychiatry Psychiatr Epidemiol 41:44–49
Andersson LMC, Schierenbeck I, Strumpher J, Krantz G, Topper K, Backman G et al (2013) Help-seeking behaviour, barriers to care and experiences of care among persons with depression in Eastern Cape, South Africa. J Affect Disord 151:439–448
Hugo CJ, Boshoff DEL, Traut A, ZunguDirwayi N, Stein DJ (2003) Community attitudes toward and knowledge of mental illness in South Africa. Soc Psychiatry Psychiatr Epidemiol 38:715–719
Woodward LJ, Fergusson DM (2000) Childhood peer relationship problems and later risks of educational under-achievement and unemployment. J Child Psychol Psychiatry 41:191–201
Ladd GW, Burgess KB (2001) Do relational risks and protective factors moderate the linkages between childhood aggression and early psychological and school adjustment? Child Dev 72:1579–1601
Department of Mental Health and Substance Abuse (2011) Kenya: mental health atlas-2011. World Health Organization, http://www.who.int/mental_health/evidence/atlas/profiles/ken_mh_profile.pdf?ua=1/. Accessed 15 May 2014
Muga FA, Jenkins R (2008) Public perceptions, explanatory models and service utilisation regarding mental illness and mental health care in Kenya. Soc Psychiatry Psychiatr Epidemiol 43:469–476
Kiima DM, Njenga FG, Okonji MMO, Kigamwa PA (2004) Kenya mental health country profile. Int Rev Psychiatry 16:48–53
Ndetei DM, Khasakhala L, Nyabola L, Ongecha-Owuor F, Seedat S, Mutiso V et al (2008) The prevalence of anxiety and depression symptoms and syndromes in Kenyan adolescents. J Child Adolesc Ment Health 20:33–51
Harder VS, Mutiso VN, Khasakhala LI, Burke HM, Ndetei DM (2011) Postelection violence, posttraumatic stress, and comorbidity of behavioural and emotional problems among Kenyan youth. Compr Psychiatry 52:e7
Ndetei DM, Mutiso V, Ongecha-Owuor FA, Kokonya DA, Khasakhala LI (2009) Psychosocial and health aspects of drug use by students in public secondary schools in Nairobi, Kenya. Subst Abuse 30:61–66
Kieling C, Baker-Henningham H, Belfer M, Conti G, Ertem I, Omigbodum O et al (2011) Children and adolescent mental health worldwide: evidence for action. Lancet 378:1515–1525
Kenya National Bureau of Statistics and ICF Macro (2010) Kenya demographic and health survey 2008–09. Calverton, ICF Macro
Ministry of State for Planning, National Development and Vision 2030 (2010) Millennium Development Goals Status Report for Kenya, 2009. Nairobi: Ministry of State for Planning, National Development and Vision 2030
Corrigan PW, Watson AC, Barr L (2006) The self-stigma of mental illness: implications for self-esteem and self-efficacy. J Soc Clin Psychol 25:875–884
Xiong NC (2011) Stigma of mental illness and depression in Hmong women. Dissertation, Alliant International University
Fung KMT, Tsang HWH, Corrigan PW, Lam C, Cheng W (2007) Measuring self-stigma of mental illness in China and its implications for recovery. Int J Soc Psychiatry 53:408–418
StataCorp (2011) Stata Statistical Software: Release 12. StataCorp LP, College Station
O’Driscoll C, Heary C, Hennessy E, McKeague L (2012) Explicit and implicit stigma towards peers with mental health problems in childhood and adolescence. J Child Psychol Psychiatry 53:1054–1062
Arbanas G (2008) Adolescents’ attitudes toward schizophrenia, depression, and PTSD. J Psychosoc Nurs Ment Health Serv 46:45–51
Watson AC, Miller FE, Lyons JS (2005) Adolescent attitudes toward serious mental illness. J Nerv Ment Dis 193:769–772
Aromaa E, Tolvanen A, Tuulari J, Wahlbeck K (2011) Predictors of stigmatizing attitudes towards people with mental disorders in a general population in Finland. Nordic J Psychiatry 65:125–132
Wang J, Fick G, Adair C, Lai D (2007) Gender specific correlates of stigma toward depression in a Canadian general population sample. J Affect Disord 103:91–97
Swords L, Heary C, Hennessy E (2011) Factors associated with acceptance of peers with mental health problems in childhood and adolescence. J Child Psychol Psychiatry 52:933–941
Wahl OF (2002) Children’s views of mental illness: a review of the literature. Am J Psychiatr Rehabil 6(2):134–158
Corrigan PW, Watson AC (2007) How children stigmatize people with mental illness. Int J Soc Psychiatry 53:526–546
Whalen CK, Henker B, Dotemoto S, Hinshaw SP (1983) Child and adolescent perceptions of normal and atypical peers. Child Dev 54:1588–1598
Jackson H, Judd F, Komiti A, Fraser C, Murray G, Robins G et al (2007) Mental health problems in rural contexts: what are the barriers to seeking help from professional providers? Aust Psychol 42:147–160
Kermode M, Bowen K, Arole S, Pathare S, Jorm AF (2009) Attitudes to people with mental disorders: a mental health literacy survey in a rural area of Maharashtra, India. Soc Psychiatry Psychiatr Epidemiol 44:1087–1096
Cinnirella M, Loewenthal KM (1999) Religious and ethnic group influences on beliefs about mental illness: a qualitative interview study. Br J Med Psychol 72:505–524
Lefley HP (1990) Culture and chronic mental illness. Hosp Community Psychiatry 41:277–286
Ng TP, Nyunt MSZ, Chiam PC, Kua EH (2011) Religion, health beliefs and the use of mental health services by the elderly. Aging Ment Health 15:143–149
Ndetei DM, Mutiso V, Musyimi C, Anderson KK, McKenzie K, Musau A. The prevalence of mental disorders among upper primary school children in Kenya (Forthcoming)
Jackson D, Heatherington L (2006) Young Jamaicans’ attitudes toward mental illness: experimental and demographic factors associated with social distance and stigmatizing opinions. J Community Psychol 34:563–576
Duncan CJ, Daly MC, McDonough P, Williams DR (2002) Optimal indicators of socioeconomic status for health research. Am J Public Health 92:1151–1157
Acknowledgments
This study was funded by a grant from Grand Challenges Canada (#0083-04) and was supported by the Africa Mental Health Foundation. Kelly Anderson is supported by a Postdoctoral Fellowship Award from Canadian Institutes of Health Research (#274885). The authors have no conflicts of interest with respect to the publication of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Ten items from the stereotype agreement subscale, taken from the Self-Stigma of Mental Illness Scale developed by Corrigan et al. [28].
-
1.
Most persons with mental illness are to blame for their problems.
-
2.
Most persons with mental illness are unpredictable (you cannot tell what they will do next).
-
3.
Most persons with mental illness will not recover or get better.
-
4.
Most persons with mental illness are unable to get or keep a regular job.
-
5.
Most persons with mental illness are dirty and unkept (untidy).
-
6.
Most persons with mental illness are dangerous/harmful to self and others.
-
7.
Most persons with mental illness cannot be trusted.
-
8.
Most persons with mental illness are below average in intelligence.
-
9.
Most persons with mental illness are unable to take care of themselves.
-
10.
Most persons with mental illness are disgusting.
Rights and permissions
About this article

Cite this article
Ndetei, D.M., Mutiso, V., Maraj, A. et al. Stigmatizing attitudes toward mental illness among primary school children in Kenya. Soc Psychiatry Psychiatr Epidemiol 51, 73–80 (2016). https://doi.org/10.1007/s00127-015-1090-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-015-1090-6