
Abstract
Aims/hypothesis
Both short and long sleep durations have been linked to higher diabetes risk. However, sleep duration may vary over time, and there has been limited research focusing on individual sleep trajectories and diabetes risk. There are substantial racial disparities in both sleep health and diabetes risk in the USA. Thus, it is important to understand the role of suboptimal sleep patterns in diabetes risk in different racial groups.
Methods
We assessed long-term trajectories of sleep duration and incident diabetes in 22,285 Black adults (mean age ± SD, 51.1 ± 8.2 years; 64.8% women) and 13,737 White adults (mean age ± SD, 54.4 ± 9.0 years; 63.8% women) enrolled in the Southern Community Cohort Study. Nine sleep trajectories were derived based on self-reported sleep duration at baseline and after a mean of 5 years of follow-up: normal–normal (reference), short–normal, normal–short, short–short, long–normal, normal–long, long–long, long–short and short–long. Diabetes was reported using a validated questionnaire. Multivariable-adjusted logistic regression was used to determine relationships between sleep trajectories and incident diabetes.
Results
When compared with the normal–normal trajectory, suboptimal sleep trajectories were associated with higher likelihoods of developing diabetes (OR; 95% CI: short–normal 1.19; 1.09, 1.31; normal–short 1.14; 1.02, 1.27; short–short 1.17; 1.07, 1.28; long–normal 1.13; 0.98, 1.30; normal–long 1.16; 1.00, 1.34; long–long 1.23; 1.02, 1.48; long–short 1.45; 1.19, 1.77; short–long 1.51; 1.28, 1.77). Stratified analyses by race and socioeconomic status (i.e. education and household income) showed that most suboptimal sleep trajectories were consistently associated with incident diabetes in all sociodemographic subgroups. We also noted potential interaction with race and education for several sleep trajectories (i.e. short–long and normal–short with race; long–long and short–short with education).
Conclusions/interpretation
Adults with suboptimal sleep duration trajectories are more likely to develop incident diabetes. Future research is needed to study how sociodemographic factors modulate this relationship.
Graphical Abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.

Introduction
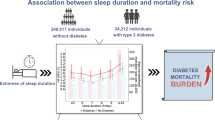
In 2019, 37.3 million American people (or 11.3% of the US population) had diabetes, with over 90% having type 2 diabetes [1]. Along with numerous well-established genetic, lifestyle and environmental risk factors, suboptimal sleep duration, including both short and long sleep, has been suggested as a modifiable risk factor for diabetes, with the lowest risk observed among individuals reporting 7–8 h of sleep [2, 3].
Sleep duration is dynamic and may change over time, reflecting both short-term variability and long-term shifts due to various internal and external factors [4]. Several recent studies have found that persistent short sleep durations [5,6,7], as well as increasing [5,6,7,8] or decreasing [6] sleep durations, were associated with a higher risk of diabetes, suggesting that abnormal sleep trajectories over time are predictors of type 2 diabetes. However, these studies were performed in racially and ethnically homogenous samples of predominantly White [5,6,7] or exclusively Chinese [8] populations, and their study participants were generally of middle-to-high socioeconomic status (SES). Therefore, it is difficult to generalise these findings to other populations, such as individuals of lower SES and Black Americans.
Black Americans suffer a disproportionately high burden of diabetes. It is estimated that 17.4% of non-Hispanic Black adults have diabetes, compared with 13.6% of non-Hispanic White adults [1]. Moreover, the prevalence of both short and long sleep durations was higher among Black individuals than White individuals [9, 10]. A recent analysis showed that, compared with White adults, Black adults were more likely to experience unhealthy long-term sleep patterns [11]. Low-SES populations are also more likely to experience both poor sleep and to develop diabetes [12]. Given the high burden of both suboptimal sleep patterns and diabetes among Black Americans and individuals of lower SES, it is a public health priority to understand how long-term trajectories of sleep duration are associated with diabetes risk in these populations.
We studied long-term sleep duration trajectories in relation to incident diabetes in a large cohort of primarily low-income middle-to-older-aged Black and White adults in the southeastern USA. We hypothesised that suboptimal sleep trajectories that deviate from a consistent sleep duration of the recommended 7–9 h [13] would be associated with higher odds of developing diabetes in both Black and White participants. Given the well-documented racial and socioeconomic disparities in both sleep and diabetes, we also explored differences in this association by race, education and income.
Methods
Study population
We used data from the Southern Community Cohort Study (SCCS), which enrolled middle-to-older-aged adults in the southeastern USA (Alabama, Arkansas, Florida, Georgia, Kentucky, Louisiana, Mississippi, North Carolina, South Carolina, Tennessee, Virginia and West Virginia) from 2002–2009 [14]. Approximately 85% of the study participants were recruited from community health centres, which primarily serve uninsured and underinsured populations, and the rest were recruited from the general population using stratified random sampling. Eligible participants were 40–79 years old, spoke English, and had not received cancer treatment within the past year. When compared to the general population in these states, the study sample had a higher percentage of individuals that were Black and/or of lower SES. The SCCS baseline questionnaire collected information on sociodemographic characteristics, lifestyle factors including sleep duration, and health and disease history including diabetes diagnosis. In 2008–2013, a follow-up questionnaire was mailed to SCCS participants to collect updated information on lifestyle and health status, including sleep duration and diabetes. The mean time gap between baseline and the follow-up was 5 years (range 1–10 years). All SCCS study procedures were approved by institutional review boards at the Vanderbilt University Medical Center and Meharry Medical College. Data and study documentation including questionnaires can be found on the study website (https://www.southerncommunitystudy.org/).
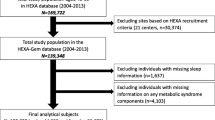
Of the 84,508 individuals enrolled at baseline, 53,342 participated in the follow-up survey. We excluded those who were missing information on sleep duration (n=4009) or diabetes (n=898) at baseline or follow-up, or reported having diabetes at baseline (n=10,597). We further removed participants who reported as neither Black or White (n=1816). The final analytic sample consisted of 36,022 participants, including 22,285 Black and 13,737 White adults (see electronic supplementary material [ESM] Fig. 1).
Sleep trajectories
The baseline questionnaire asked ‘How many hours do you typically sleep in a 24-hour period?’ and participants answered for weekdays and weekends separately. Baseline sleep duration was then determined as (weekday duration × 5 + weekend duration × 2)/7. The follow-up survey asked ‘In a 24-hour period, how many hours do you typically spend sleeping?’, without making a distinction between weekday and weekends. We defined short, normal/healthy and long sleep durations as <7 h, 7–9 h and >9 h, according to the recommendations by the American Academy of Sleep Medicine [13]. Based on the sleep duration at baseline and follow-up, we first defined a nine-category sleep trajectory variable (i.e. normal–normal [reference], short–short, long–long, normal–short, normal–long, short–normal, long–normal, short–long and long–short), which served as the main exposure variable. To aid interpretation and visualisation of results, we further combined categories with similar distributions of key study characteristics, creating a secondary, six-category variable: the optimal stable healthy trajectory (normal–normal, reference), and five suboptimal trajectories, stable short (short–short), stable long (long–long), healthy-to-short (normal–short and short–normal), healthy-to-long (normal–long and long–normal) and unstable unhealthy (long–short and short–long). Finally, we evaluated to what degree the results are affected by the categorisation of sleep duration, by using 7–8 h as the definition of normal sleep duration in sensitivity analysis.
Diabetes
At baseline, participants were asked whether they had ‘been diagnosed with diabetes or high blood sugar (not during pregnancy)’. The follow-up survey asked participants ‘After joining this study, have you been diagnosed with diabetes/high blood sugar?’ Incident diabetes was defined as answering ‘yes’ to the follow-up survey question after answering ‘no’ to the baseline question.
Covariates
The following covariates were included in the analysis: sociodemographic characteristics (age, race, sex, education, household income, marital status, employment status), lifestyle factors (smoking status, alcohol intake, healthy eating index [HEI]-2015 [15], total physical activity, total sitting time) and BMI. All covariates were derived based on self-reported information collected in the baseline questionnaire. We additionally included household income, marital status and employment status at follow-up as covariates in the sensitivity analyses.
Statistical analysis
Descriptive statistics are presented as percentages for categorical variables and means ± SD for continuous variables. Multivariable-adjusted logistic regression models were used to calculate OR and 95% CIs for incident diabetes in each suboptimal sleep trajectory compared with the reference (normal–normal/stable healthy). The results were derived from four models. Model 1 was the minimal model adjusted for age (continuous) and sex (male, female). Model 2 was the main model additionally adjusted for race (Black, White; not in race-stratified analysis), education (less than high school, high school graduate, vocational training or some college, college graduate or higher; not in education-stratified analysis), marital status (married, separated or divorced or widowed, never been married), annual household income (<US$15,000, $15,000 to <25,0000, $25,000 to <50,000, ≥$50,000), employment status (employed, unemployed), smoking status (current, former, never), alcohol use (non-drinker, <1 drink per day, ≥1 drinks per day), healthy eating index (quartiles), total physical activity (metabolic equivalent hour [MET-h], quartiles), total sitting hours (quartiles) and follow-up duration (continuous). We performed sensitivity analyses using two separate models. Model 3 was additionally adjusted for BMI (<18.5, 18.5–24.9, 25–29.9, ≥30 kg/m2), which can act both as a confounder and a mediator of the relationship between sleep trajectories and diabetes, and model 4 was additionally adjusted for household income, marital status and employment status at follow-up to assess to what degree the results are confounded by changes in these sociodemographic attributes. Missing values for all covariates (<5% for all variables) were coded as a separate category. We performed stratified analyses by race (Black, White), education (high school or lower, more than high school) and household income (<US$15,000, ≥$15,000). The cutoff points for education and income were chosen to create roughly equal sample sizes in the subgroups to preserve statistical power. Statistical significance for interactions was evaluated by including a product term between two variables and tested using a likelihood ratio test. All analyses were performed using SAS 9.4 (SAS Institute, USA).
Results
In the overall study sample, approximately one third (34.5%) were in the normal–normal or stable healthy group, followed by the short–short (20.4%), short–normal (16.8%) and normal–short (10.4%) groups. Each of the remaining trajectory groups contained 2.0–5.3% of the study sample (Table 1). Compared with White participants, Black participants were less likely to be in the normal–normal group and more likely to be in a suboptimal sleep trajectory group. The likelihood of developing incident diabetes between baseline and follow-up was almost twice as high in the Black participants (16.43%, n=3661) than in White participants (8.93%, n=1227).
Substantial group differences were observed in the distribution of baseline characteristics by sleep trajectory groups and by race (Table 1, ESM Table 1). In the total sample, the normal–normal group generally showed a sociodemographic and lifestyle profile that would favour a lower risk for diabetes when compared with other sleep trajectory groups. Specifically, participants in the normal–normal group had the highest SES (i.e. education and household income), were the most likely to be married and employed and the least likely to be current smokers, and reported the least amount of sedentary time and the highest dietary quality. In contrast, the long–short, short–long and the long–long group showed the least favourable profile for diabetes risk, as characterised by lower SES and unhealthy lifestyle. These patterns were largely similar in both Black and White participants. However, Black participants also showed a few distinct patterns. Most notably, among Black participants, the short–short group showed a comparable, even slightly higher, SES compared with the normal–normal group.
In the total population, all eight suboptimal sleep trajectories were associated with higher odds of developing diabetes when compared with the normal–normal group (Table 2, model 1). Adjusting for confounders in the main model attenuated the associations; however, all results remained statistically significant (Table 2, model 2). Compared with the normal–normal group, the short–long and long–short trajectories were associated with the highest odds of incident diabetes, showing an approximately 50% greater risk (OR 1.51; 95% CI 1.28, 1.77 for the short–long trajectory and OR 1.45; 95% CI 1.19, 1.77 for the long–short trajectory), while the other suboptimal sleep trajectories showed a more modest increase in risk (OR range: 1.13 to 1.23). Additionally adjusting for BMI or follow-up covariates had a limited impact on the results (Table 2, models 3 and 4). Using 7–8 h as the definition of normal sleep duration had only a limited impact on the study findings (changes in effect estimates <5% for most associations, data not shown).
Greater odds of incident diabetes for suboptimal sleep trajectories were similarly observed in all subgroups, but the results also showed notable between-group differences by race and education as shown in Table 2 (nine-category sleep trajectory results) and Fig. 1 and ESM Table 2 (six-category sleep trajectory results). Specifically, race-stratified analyses showed that the greater odds of diabetes observed among the long–short and short–long trajectories were more prominent in White participants (long–short OR 1.74; 95% CI 1.02, 2.94; short–long OR 1.92; 95% CI 1.41, 2.62) than in Black participants (long–short OR 1.39; 95% CI 1.12, 1.72; short–long OR 1.36; 95% CI 1.13, 1.64), although the p values for interaction suggested significant effect modification for only the short–long trajectory (pinteraction=0.03) but not the long–short trajectory (pinteraction=0.28). Moreover, the associations for the normal–short trajectory were also stronger in White participants (OR 1.45; 95% CI 1.17, 1.79) than in Black participants (OR 1.05; 95% CI 0.92, 1.19) (pinteraction=0.005). Stratified analysis by education level showed significant interaction with the long–long (pinteraction=0.003) and short–short trajectories (pinteraction=0.03), and for both trajectories, the association was stronger in those with higher than high school education (OR 1.76; 95% CI 1.31, 2.36 and OR 1.33; 95% CI 1.15, 1.53 for the long–long and short–short trajectories, respectively) than in those with a lower education level (OR 0.99; 95% CI 0.78, 1.26 and OR 1.07; 95% CI 0.95, 1.20, respectively). We did not observe any interaction between sleep trajectories and household income (ESM Table 3). Finally, because we detected statistically significant effect modification by race and education, we performed additional analyses in the four race and education subgroups (ESM Table 4). We found that being in the unstable unhealthy group (i.e. the long–short and short–long trajectories) was consistently associated with higher incident diabetes across all race and education groups, with the largest effect size found in the White participants with more than high school education (OR 1.93; 95% CI 1.17, 3.16) and the lowest in the Black participants with high school or lower education (OR 1.29; 95% CI 1.08, 1.54), although the p value for interaction was only borderline significant (pinteraction=0.06). A similarly borderline significant interaction (pinteraction=0.07) was also observed for the healthy-to-short group, and no other sleep group showed evidence for interaction.

Associations between long-term sleep patterns and incident diabetes in the SCCS in the total sample and by race (a) and education (b). The results were derived from multiple logistic regression models adjusted for age, sex, race (not in race-stratified analysis), education (not in education-stratified analysis), marital status, annual household income, employment status, smoking status, alcohol use, healthy eating index, total physical activity, total sitting hours and follow-up duration. Bars represent ORs and error bars represent 95% CI. The p values for interaction between race and the sleep trajectory variables are 0.03 for healthy-to-short, 0.49 for stable short, 0.86 for healthy-to-long, 0.63 for stable long and 0.01 for unstable unhealthy. The p values for interaction between education and the sleep trajectory variables are 0.24 for healthy-to-short, 0.03 for stable short, 0.12 for healthy-to-long, 0.002 for stable long and 0.15 for unstable unhealthy. Ref., reference
Discussion
In a unique cohort of middle-to-older-aged adults who were predominantly Black and of low SES in the southeastern USA, we found that suboptimal sleep duration trajectories were associated with higher odds of incident diabetes. In stratified analyses, we observed potential effect modification by race and education, which may suggest that certain sleep trajectories are stronger predictors of diabetes in specific sociodemographic groups than in others.
Several prior longitudinal studies have examined sleep duration trajectories in relation to diabetes risk. In the Nurses’ Health Study, the authors used methods similar to ours to assign nine categories of 14-year sleep trajectories. They found that women in the short–normal and short–short groups had significantly higher incidence of diabetes, and both increases and decreases in sleep duration predicted higher diabetes risk [7]. In the Nurses’ Health Study II, latent class growth modelling was used to derive six sleep trajectories (persistent sleep duration of 5, 6, 7 and 8 h, decreased and increased sleep duration) based on retrospectively reported data. The findings suggested that women in the consistent 5 and 6 h groups, as well as women in the decreasing and increasing groups, had a higher risk of type 2 diabetes [6]. In the Whitehall II Study, Ferrie et al examined sleep patterns over four consecutive study cycles in relation to incident type 2 diabetes [5]. Compared with those reporting 7 h of sleep at both the beginning and end of a study cycle, participants with an increase in sleep duration of 2 h or more and those who had consistently short sleep (mean ≤ 5.5 h) had a 65% and 35% greater risk of diabetes during that cycle, respectively. Finally, a Chinese study of workers in the coal industry found that, when compared with participants who persistently reported 7 h of sleep, those with persistently long sleep (7.5–8 h and ≥8.5 h) and an increasing sleep duration of ≥2 h over a two-year period had higher risk of diabetes [8]. Overall, our findings are consistent with these previous findings, and suggest that multiple suboptimal sleep trajectories may be associated with higher risk of incident diabetes.
Of all the sleep trajectories assessed in our study, the unstable unhealthy group (i.e. short–long and long–short trajectories) showed the strongest association with diabetes in the total sample and all subgroups. These two sleep trajectories are characterised by more extreme changes in sleep duration between baseline and follow-up, which may suggest higher variability in sleep duration. High variability in sleep duration has been linked to poorer glycaemic control, obesity and diabetes. For example, in the PREDIMED-Plus trial, a greater night-to-night sleep duration variability was associated with a 14% increase in prevalent diabetes even after controlling for average sleep duration [16]. A larger variation in sleep duration was associated with significantly higher HbA1c in the Observation of Cardiovascular Risk Factors in Luxembourg (ORISCAV-LUX-2) study [17]. In addition, an analysis of participants in the Multi-Ethnic Study of Atherosclerosis showed that greater sleep duration variability was associated with a higher incidence of multiple metabolic abnormalities [18]. A recent systematic review concluded that greater variation in sleep duration may be associated with higher weight gain, although the associations for diabetes and glucose levels were mixed [19]. In our sample, Black participants were nearly twice as likely to have a short–long or long–short trajectory than White participants. Moreover, our previous analysis of participants in the SCCS reported a strong association between lower SES and both the long–short and short–long trajectories [11]. The substantially high prevalence of these trajectories in Black and low-SES populations, combined with convincing evidence supporting a link between sleep duration variability and metabolic dysfunction, suggest that a highly variable sleep duration in disadvantaged populations may be an important contributing factor to racial and socioeconomic disparities in cardiometabolic health, which is an important research topic that warrants further investigation.
The healthy-to-short (i.e. short–normal and normal–short) and stable short (i.e. short–short) trajectories were associated with a moderate increase in the odds of incident diabetes in our study. This finding is consistent with previous studies suggesting that short sleep is a risk factor for type 2 diabetes. A meta-analysis of prospective studies found that, when compared with 7 h of sleep, every 1 h decrease in sleep duration was associated with a 9% increase in diabetes risk (95% CI 1.04, 1.15) [2]. The aforementioned studies focusing on sleep trajectories also generally suggested that persistent short sleep was associated with diabetes risk [5,6,7]. There is growing evidence demonstrating that the prevalence of short sleep is higher in Black than White Americans [9, 10]. Moreover, emerging evidence suggests a more complex pattern of sleep disparities at the intersection of race and SES: although higher SES is associated with a lower prevalence of short sleep in White populations, multiple studies have reported a weaker, or even opposite, relationship between SES and short sleep in Black Americans [11, 20, 21]. These findings suggest that the protective effect of higher SES against short sleep is not universal, and Black Americans, even those with relatively higher SES, are disproportionately affected by short sleep, likely due to psychological stress and housing disparities related to persistent racism [21].
Participants in the healthy-to-long (i.e. long–normal and normal–long) and stable long (i.e. long–long) trajectory groups showed higher odds of incident diabetes when compared with the optimal or normal–normal sleep trajectory. Long sleep has been consistently linked to a higher risk of diabetes, with a meta-analysis reporting that every 1 h increase in sleep duration was associated with 14% (95% CI 1.03, 1.26) increase in diabetes risk [2]. There has been some debate about the mechanisms underlying the relationship between long sleep and diabetes [22], with suggestions that it may be spuriously caused by confounding by other diabetes risk factors, including comorbidity, and/or reflect reverse causation due to fatigue from undiagnosed diabetes. These hypotheses are supported by a recent Mendelian randomisation study that did not find a causal relationship between long sleep duration and type 2 diabetes [23]. However, even without a causal relationship, long sleep is still an important behavioural predictor of diabetes risk that may be used for risk prediction and disease screening. Our previous study [11] reported that lower education and income, unemployment status and lower neighbourhood SES were all associated with long–long, long–normal and normal–long sleep trajectories, and, interestingly, lower neighbourhood SES appeared to show a stronger relationship with these trajectories among Black populations compared with White people. Collectively, the evidence suggested that Black adults with lower SES and living in disadvantaged neighbourhoods may have a particularly high prevalence of long sleep, and thus resources are needed for diabetes screening and treatment in this population.
In stratified analyses, we found that almost every suboptimal sleep trajectory was consistently associated with higher incident diabetes in all subgroups, suggesting that unhealthy sleep may be a predictor of metabolic diseases across diverse populations. However, we also noted several statistically significant interactions for certain sleep trajectories. For example, the unstable unhealthy (i.e. long–short and short–long) and healthy-to-short (i.e. normal–short and short–normal) trajectories appeared to have a stronger association with diabetes among White participants than Black participants, while the short–short and long–long trajectories were associated with diabetes risk only among those with more than high school education. Although such subgroup differences may be chance findings, several previous studies also reported that the associations between sleep duration and health may differ by race. For example, a cross-sectional analysis reported that short and long sleep duration were more strongly associated with diabetes in White than in Black adults, although such racial differences became non-significant after adjusting for SES [24]. In our previous analysis of participants in the SCCS, we also found that the U-shaped relationship between sleep duration and mortality rate was stronger among White people [25]. However, we are not aware of other studies that investigated the sleep–health relationship by education status, and our findings in the current analysis are thus novel and warrant further investigations.
Although it is unclear what may have caused the observed subgroup differences in the sleep–diabetes association, we speculate that there may be several explanations. First, the validity of self-reported sleep duration has been shown to vary across demographic groups [26], which may have contributed to the varied strength in the sleep–health associations. Second, sleep duration may be correlated with various socioeconomic, work-related, cultural and lifestyle factors. The distribution of these factors and their influence on diabetes may differ by race, education and income, leading to varying degrees of confounding by these factors in different subgroups. Because it is almost impossible to eliminate residual confounding in observational studies, this may also contribute to the different strengths of the relationships in subgroup results. Finally, diabetes is a complex disease, and sleep is only one potential causal factor among numerous causes in the ‘causal pie’ [27], and its effect on diabetes may be influenced by other causal factors that have different distributions and relative importance across different populations. Nonetheless, these subgroup-specific findings, if confirmed in other populations, may inform the development and refinement of algorithms and nuanced clinical practices for predicting, monitoring and managing disease risk in diverse populations.
There are two main strengths to our study. First, longitudinal and repeated surveys of sleep duration and diabetes in the SCCS have allowed us to examine the association between sleep trajectories and incident diabetes. Second, the unique study population allowed us to examine this association in Black and White Americans separately and in a low-SES sample, which have not been investigated in previous studies. Our study also has several limitations. First, the measurement of sleep duration was based on self-report, which is more prone to error and possible bias compared with objectively-measured sleep duration [26]. Second, the importance of multidimensional sleep assessment has been increasingly recognised [28], but we only had data on sleep duration, and were not able to examine other important aspects of sleep, including efficiency, timing and sleep disorders such as sleep apnoea. We also were not able to distinguish between night-time sleep and daytime napping, which may be independently associated with diabetes. Third, diabetes status was assessed by self-report, although validation studies within the SCCS showed high specificity for self-reported diabetes, with 96% of diagnoses confirmed using medical records or HbA1c testing [29]. In addition, although adult-onset type 1 diabetes is generally rare, we did not have information on types of diabetes and thus were not able to restrict our analysis to type 2 diabetes. Fourth, we did not have information on time of diabetes diagnosis, and were not able to calculate hazard ratios, which would be a more accurate measure of relative risk. Importantly, underdiagnosis and delayed diagnosis of diabetes are common, especially in low-income populations. These issues may lead to misclassification of the study outcome and failure to exclude participants who had undiagnosed diabetes at baseline. As undiagnosed diabetes may disrupt sleep as a result of neuropathic pain and nocturia, this could cause temporal ambiguity in the relationship between exposure and outcome and contribute to reverse causation. Fifth, the statistical power is limited for detecting significant interactions in subgroup analyses, particularly the analysis by subgroups defined by both race and education. Sixth, although our large and diverse study sample was a unique strength, it only included participants living in the southeastern USA, who may not be representative of the national population. Seventh, all covariates included in our analyses were based on self-reported data, which may lead to measurement error and incomplete control for confounding. Eighth, the follow-up period was the same for the measurement of sleep trajectories and incident diabetes. Therefore, we were not able to clarify the temporal relationship between the two, and a bidirectional relationship is possible. Finally, the SCCS is an observational cohort, and is not designed to allow causal inferences based on its findings, due to residual confounding.
In conclusion, our findings contribute to the existing literature by further establishing associations between long-term sleep duration trajectories and diabetes. Our study also expanded the knowledge base by focusing on an understudied population that includes large numbers of low-income and Black Americans, and by performing analyses in specific race and socioeconomic subgroups. Future studies should assess to what degree long-term patterns of sleep contribute to racial and socioeconomic disparities in health outcomes, and identify what social and environmental factors shape long-term sleep trajectories in the population. Intervention studies are also needed to evaluate whether improving sleep health may reduce health disparities in the USA.
Abbreviations
- SCCS:
-
Southern Community Cohort Study
- SES:
-
Socioeconomic status
References
Centers for Disease Control and Prevention. National Diabetes Statistics Report. Available from https://www.cdc.gov/diabetes/php/data-research/index.html. Accessed 24 March 2023
Shan Z, Ma H, Xie M et al (2015) Sleep duration and risk of type 2 diabetes: a meta-analysis of prospective studies. Diabetes Care 38(3):529–537. https://doi.org/10.2337/dc14-2073
Lu H, Yang Q, Tian F et al (2021) A meta-analysis of a cohort study on the association between sleep duration and type 2 diabetes mellitus. J Diabetes Res 2021:8861038. https://doi.org/10.1155/2021/8861038
Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV (2004) Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep 27(7):1255–1273. https://doi.org/10.1093/sleep/27.7.1255
Ferrie JE, Kivimaki M, Akbaraly TN et al (2015) Change in sleep duration and type 2 diabetes: the Whitehall II study. Diabetes Care 38(8):1467–1472. https://doi.org/10.2337/dc15-0186
Baden MY, Hu FB, Vetter C, Schernhammer E, Redline S, Huang T (2020) Sleep duration patterns in early to middle adulthood and subsequent risk of type 2 diabetes in women. Diabetes Care 43(6):1219–1226. https://doi.org/10.2337/dc19-2371
Cespedes EM, Bhupathiraju SN, Li Y, Rosner B, Redline S, Hu FB (2016) Long-term changes in sleep duration, energy balance and risk of type 2 diabetes. Diabetologia 59(1):101–109. https://doi.org/10.1007/s00125-015-3775-5
Song Q, Liu X, Zhou W, Wang X, Wu S (2016) Short-term changes in sleep duration and risk of type 2 diabetes: Kailuan prospective study. Medicine (Baltimore) 95(45):e5363. https://doi.org/10.1097/MD.0000000000005363
Whinnery J, Jackson N, Rattanaumpawan P, Grandner MA (2014) Short and long sleep duration associated with race/ethnicity, sociodemographics, and socioeconomic position. Sleep 37(3):601–611. https://doi.org/10.5665/sleep.3508
Caraballo C, Mahajan S, Valero-Elizondo J et al (2022) Evaluation of temporal trends in racial and ethnic disparities in sleep duration among US adults, 2004–2018. JAMA Netw Open 5(4):e226385. https://doi.org/10.1001/jamanetworkopen.2022.6385
Nyarko SH, Luo L, Schlundt DG, Xiao Q (2023) Individual and neighborhood socioeconomic status and long-term individual trajectories of sleep duration among Black and White adults: the Southern Community Cohort Study. Sleep 46(1):zsac225. https://doi.org/10.1093/sleep/zsac225
Papadopoulos D, EtindeleSosso FA (2023) Socioeconomic status and sleep health: a narrative synthesis of 3 decades of empirical research. J Clin Sleep Med 19(3):605–620. https://doi.org/10.5664/jcsm.10336
Consensus Conference Panel, Watson NF, Badr MS et al (2015) Joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society on the recommended amount of sleep for a healthy adult: methodology and discussion. Sleep 38(8):1161–1183. https://doi.org/10.5665/sleep.4886
Signorello LB, Hargreaves MK, Steinwandel MD et al (2005) Southern Community Cohort Study: establishing a cohort to investigate health disparities. J Natl Med Assoc 97(7):972–979
Krebs-Smith SM, Pannucci TE, Subar AF et al (2018) Update of the healthy eating index: HEI-2015. J Acad Nutr Diet 118(9):1591–1602. https://doi.org/10.1016/j.jand.2018.05.021
Rosique-Esteban N, Papandreou C, Romaguera D et al (2018) Cross-sectional associations of objectively-measured sleep characteristics with obesity and type 2 diabetes in the PREDIMED-Plus trial. Sleep 41(12):zsy190. https://doi.org/10.1093/sleep/zsy190
Aguayo GA, Pastore J, Backes A et al (2022) Objective and subjective sleep measures are associated with HbA1c and insulin sensitivity in the general population: findings from the ORISCAV-LUX-2 study. Diabetes Metab 48(1):101263. https://doi.org/10.1016/j.diabet.2021.101263
Huang T, Redline S (2019) Cross-sectional and prospective associations of actigraphy-assessed sleep regularity with metabolic abnormalities: the Multi-Ethnic Study of Atherosclerosis. Diabetes Care 42(8):1422–1429. https://doi.org/10.2337/dc19-0596
Zhu B, Wang Y, Yuan J et al (2022) Associations between sleep variability and cardiometabolic health: a systematic review. Sleep Med Rev 66:101688. https://doi.org/10.1016/j.smrv.2022.101688
Sheehan CM, Walsemann KM, Ailshire JA (2020) Race/ethnic differences in educational gradients in sleep duration and quality among U.S. adults. SSM Popul Health 12:100685. https://doi.org/10.1016/j.ssmph.2020.100685
Luo L, Buxton OM, Gamaldo AA, Almeida DM, Xiao Q (2021) Opposite educational gradients in sleep duration between Black and White adults, 2004–2018. Sleep Health 7(1):3–9. https://doi.org/10.1016/j.sleh.2020.10.003
Tan X, Chapman CD, Cedernaes J, Benedict C (2018) Association between long sleep duration and increased risk of obesity and type 2 diabetes: a review of possible mechanisms. Sleep Med Rev 40:127–134. https://doi.org/10.1016/j.smrv.2017.11.001
Gao X, Sun H, Zhang Y, Liu L, Wang J, Wang T (2020) Investigating causal relations between sleep-related traits and risk of type 2 diabetes mellitus: a Mendelian randomization study. Front Genet 11:607865. https://doi.org/10.3389/fgene.2020.607865
Jackson CL, Redline S, Kawachi I, Hu FB (2013) Association between sleep duration and diabetes in black and white adults. Diabetes Care 36(11):3557–3565. https://doi.org/10.2337/dc13-0777
Xiao Q, Blot WJ, Matthews CE (2019) Weekday and weekend sleep duration and mortality among middle-to-older aged White and Black adults in a low-income southern US cohort. Sleep Health 5(5):521–527. https://doi.org/10.1016/j.sleh.2019.04.008
Lauderdale DS, Knutson KL, Yan LL, Liu K, Rathouz PJ (2008) Self-reported and measured sleep duration: how similar are they? Epidemiology 19(6):838–845. https://doi.org/10.1097/EDE.0b013e318187a7b0
Rothman KJ (1976) Causes. Am J Epidemiol 104(6):587–592. https://doi.org/10.1093/oxfordjournals.aje.a112335
Buysse DJ (2014) Sleep health: can we define it? Does it matter? Sleep 37(1):9–17. https://doi.org/10.5665/sleep.3298
Signorello LB, Hargreaves MK, Blot WJ (2010) The Southern Community Cohort Study: investigating health disparities. J Health Care Poor Underserved 21(1 Suppl):26–37. https://doi.org/10.1353/hpu.0.0245
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Data availability
All data in the SCCS study are available upon request, following an established proposal procedure. Relevant information, documents and the proposal submission link may be found at https://www.southerncommunitystudy.org/
Funding
The research reported in this publication was supported by the National Cancer Institute of the NIH under award number U01CA202979. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. SCCS data collection was performed by the Survey and Biospecimen Shared Resource, which is supported in part by the Vanderbilt–Ingram Cancer Center (P30 CA68485). This work is also supported by the National Heart, Lung and Blood Institute (grant number R21HL165369 to QX), the National Institute on Aging (grant number R01AG063946 to QX) and the NIHR Manchester Biomedical Research Centre (MKR).
Authors’ relationships and activities
The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Contribution statement
QX was responsible for study design, statistical analysis, and preparation of the initial draft of the manuscript. All other authors were responsible for interpretation of the results and critical review of the manuscript for important intellectual content. All authors approved the version to be published. QX is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Xiao, Q., Full, K.M., Rutter, M.K. et al. Long-term trajectories of sleep duration are associated with incident diabetes in middle-to-older-aged Black and White Americans. Diabetologia 67, 1853–1864 (2024). https://doi.org/10.1007/s00125-024-06202-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-024-06202-8